
Abstract
Background
The Nuss procedure is the primary treatment for pectus excavatum (PE), but patient expectations are not always met. In our unit, our standard approach in the last few years has been the routine application of two bars instead of one. We aimed to retrospectively assess the impact of this approach on patient satisfaction, quality of life (QoL) and safety.
Methods
A retrospective study included 182 patients over 16 years old who underwent the Nuss procedure for PE between January 2007 and September 2021. Patients were categorized into one-bar or two-bar correction groups. Propensity score matching (PSM) was used, resulting in 30 patients in each group. Primary endpoints were QoL and cosmetic satisfaction, while secondary endpoints included complications and recurrence.
Results
After PSM, both groups showed similar general characteristics. Patients treated with two bars reported fewer psychological complaints post-surgery (93.3% vs. 73.3%, p = 0.031). There were no significant differences in QoL improvement (96.7% in both groups, p = 0.197), perioperative complications (p = 0.771) or recurrence (one patient in the one-bar group, p = 1.000).
Conclusions
Our study reveals that patients undergoing the Nuss Procedure for PE with two bars exhibit comparable clinical outcomes and QoL to those with one bar. However, patients with two bars may have higher levels of psychological well-being and satisfaction, indicating potential benefits associated with this approach. These findings suggest potential advantages of the two-bar approach, but further research with larger sample sizes is warranted to confirm these observations.
Introduction
Pectus excavatum (PE) is the most common congenital chest wall deformity, occurring in approximately 1 in 1000 children, with male prevalence. 1 Usually, children with PE complain of physiologic and psychologic limitations that may improve after surgery. 2 Despite the challenge of objectively quantifying and demonstrating cardiopulmonary limitations, there is indicative evidence suggesting that surgical intervention could result in improvement. 3 Nonetheless, it is worth noting that cosmetic enhancement remains an important factor in the correction of PE. 4
The Nuss procedure gained prominence following Donald Nuss's ground-breaking report in 1998, 5 although its initial application dates back to 1987, with the first publication of results at the American Political Science Annual meeting in 1997, prompted by Robert Kelly. In the classical Nuss procedure, a single bar is placed to lift the sternum. Nevertheless, the correction may be incomplete especially in adult patients.6,7 The use of multiple bars may have some advantages (cosmesis and postoperative pain) but may be associated with increased postoperative complications and hospital readmissions.6,8
In our unit, due to personal experience, our standard approach, regardless of the type of PE, has been modified with the routine placement of two bars instead of one. The aim of our study was to retrospectively investigate the usefulness of this strategy in terms of patient's satisfaction, quality of life (QoL) and safety. Here, satisfaction is defined as the fulfillment of patients’ preoperative desires and expectations with cosmetic outcomes; QoL encompasses physical, psychological and social well-being; and safety refers to the minimization of potential adverse effects or complications.
Patients and methods
This is a retrospective study of consecutive patients older than 16 years who underwent the Nuss procedure for PE by one senior surgeon who had already surpassed the learning curve threshold of 59 procedures, 9 between January 2007 and September 2021. They were divided in two groups: correction with one bar or with two bars. The selection criteria for the one-bar versus two-bar procedure were based on our unit's evolving clinical practice and personal experience dating back to 2009. Over the years, it became apparent through clinical observation and patient feedback that the insertion of two bars yielded improved cosmetic outcomes and reduced postoperative pain compared to the traditional single-bar approach.6,8 Consequently, our unit adopted a standard protocol of routinely applying two bars in eligible patients undergoing the Nuss procedure for PE. This decision was not based on formalized criteria or randomized allocation but rather on anecdotal evidence and continuous refinement of surgical techniques to optimize patient outcomes. In our institution, it is common practice to obtain written informed consent from all patients as well as consent for the anonymous use of patient data for all research purposes, prior to surgery. In this case, each patient present in the study followed this protocol. Moreover, written informed consent was obtained from all patients and the institutional review board of the principal investigator hospital approved the study (N° 2528-CESC). The study was performed in line with the principles of the Declaration of Helsinki. The paper was written according to the STROCSS criteria (Strengthening the reporting of cohort studies in surgery), the checklist is provided as Supplementary File 1. 10
Primary endpoints of the study were QoL and satisfaction with the cosmetic results. The secondary endpoints were complications and recurrence.
Exclusion criteria were patients younger than 16-year-old (pediatric patients) and hybrid procedures (defined as bar insertion plus open repair of the chest deformity).
Patients’ baseline condition, technical details of surgical procedures together with short- and long-term outcomes were collected.
In both groups, the surgical procedure was carried out in the same manner with the exception of the number of bars inserted, as previously described 11 and described in more brief as Supplementary File 2.
Pain management was individualized for each patient, with the attending anesthesiologist making decisions regarding specific procedure details. In selected cases, the anesthesia team inserted a thoracic epidural catheter just prior to surgery, typically at the T5–6 or T6–7 interspaces. Subsequent to catheter placement, an epidural infusion was initiated using a solution containing 0.2% ropivacaine and 2 μg/cc of fentanyl and continued for 48 h at 5–6 ml/h. Alternatively, continuous peripheral morphine infusion at a rate of 0.25 mg/kg/day for 48 h was administered. On postoperative day 1, patients began taking oral analgesics, including paracetamol (acetaminophen) combined with codeine at the standard dose of 500/30 mg three times daily and ibuprofen 600 mg three times daily. A rescue dose of acetaminophen 1000 mg or morphine (0.1 mg/kg/day) was administered if VAS scale was >5.
Safety was evaluated by comparing the rates of complications between the two groups. The Clavien–Dindo–Seely classification was used to grade perioperative complications. 12 Poorly controlled or persistent postoperative pain (e.g., requiring rescue doses of opioids or daily medication beyond the 30th postoperative day) was counted as a Grade 1 complication. Before the repair, all patients were informed that the implants would be usually removed after three years and that pectus recurrence might occur in 1–3% of cases.
After the repair, follow-up visits and chest radiographs were scheduled at 1, 6 and 12 months and yearly thereafter, up to one year after bar removal. Bar removal was performed at the 3-year mark for patients experiencing discomfort or those opting for the procedure. When patients inquired about prolonging the presence of bars beyond this time frame to mitigate recurrence risks, discussions on available evidence ensued. Shared decisions, considering normal chest X-ray results and absence of clinical issues, were made on a case-by-case basis regarding whether to proceed with removal or delay. If the latter was chosen, bar removal would be scheduled during subsequent follow-up appointments. 11 Long-term complications were defined as occurring or lasting for more than 1 year.
We contacted patients who had undergone the Nuss procedure and met the inclusion criteria for a structured interview, either in person, over the phone, or via email. The survey for this study was designed to examine the patients’ baseline condition and assess the effects of the repair in terms of QoL and satisfaction with cosmetic results. Quality of life and general well-being were assessed on a 5-tier scale from ‘very much improved’ to ‘worse than before surgery’. The interviewers were also instructed to systematically collect information about any adverse event that required medical intervention during the follow-up period and assess whether it was potentially attributable to the presence of pectus bars. The questionnaire was administered to the patients a minimum of one month subsequent to their surgical procedure. No Italian version of the sole validated questionnaire is available, 13 thus a readjusted version was used, as previously published. 11
Statistical analysis
Analyses were conducted with IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp. Continuous variables are expressed as median and range, categorical variables are expressed as numbers and percentages.
In order to minimize the bias caused by non-randomized patients, a propensity score matched (PSM) analysis was used to mitigate the confounding factors. We employed a nearest neighbour matching algorithm without replacement, using a caliper of 0.04 to select the most appropriately matched pairs. Matching variables included sex, age, type of PE, Haller Index, preoperative psychological complaints and previous correction attempt. All covariates were chosen based on clinical expertise. Standardized mean difference was defined as the difference in the means of the two groups divided by the standard deviation. Standardized mean difference < 0.2 was considered to demonstrate acceptable balance.
The significance level was set to 5% (p = 0.05). Normality of the variables was calculated using the Shapiro–Wilk test. The two groups were compared using the Fisher's exact test, applied to dichotomous or categorical data, and the Mann–Whitney U test, applied to continuous or discrete data.
Results
Between January 2007 and December 2021, 182 patients, including 33 patients in the one-bar Group and 149 patients in the two-bar Group, met the study criteria (Figure 1). After PSM, a total of 60 patients were included, 30 patients in each group. Patients’ general characteristics and perioperative results before and after PSM are shown in Table 1. After 1:1 PSM, no differences were observed between the two groups regarding the variables used for the PSM: age, gender, type of PE, Haller Index, preoperative psychological complaints and previous correction attempts. Additionally, there were no disparities noted in the duration of surgery, length of hospital stay (LOS), rates and types of perioperative complications, pain management, acute pain and Clavien–Dindo classification scores. In particular, despite the need to insert an additional bar the surgery was not longer (63.8 ± 10.47 vs. 65.0 ± 7.42, p = 0.444) and LOS was similar (3.50 ± 0.63 vs. 3.53 ± 0.629, p = 0.814).
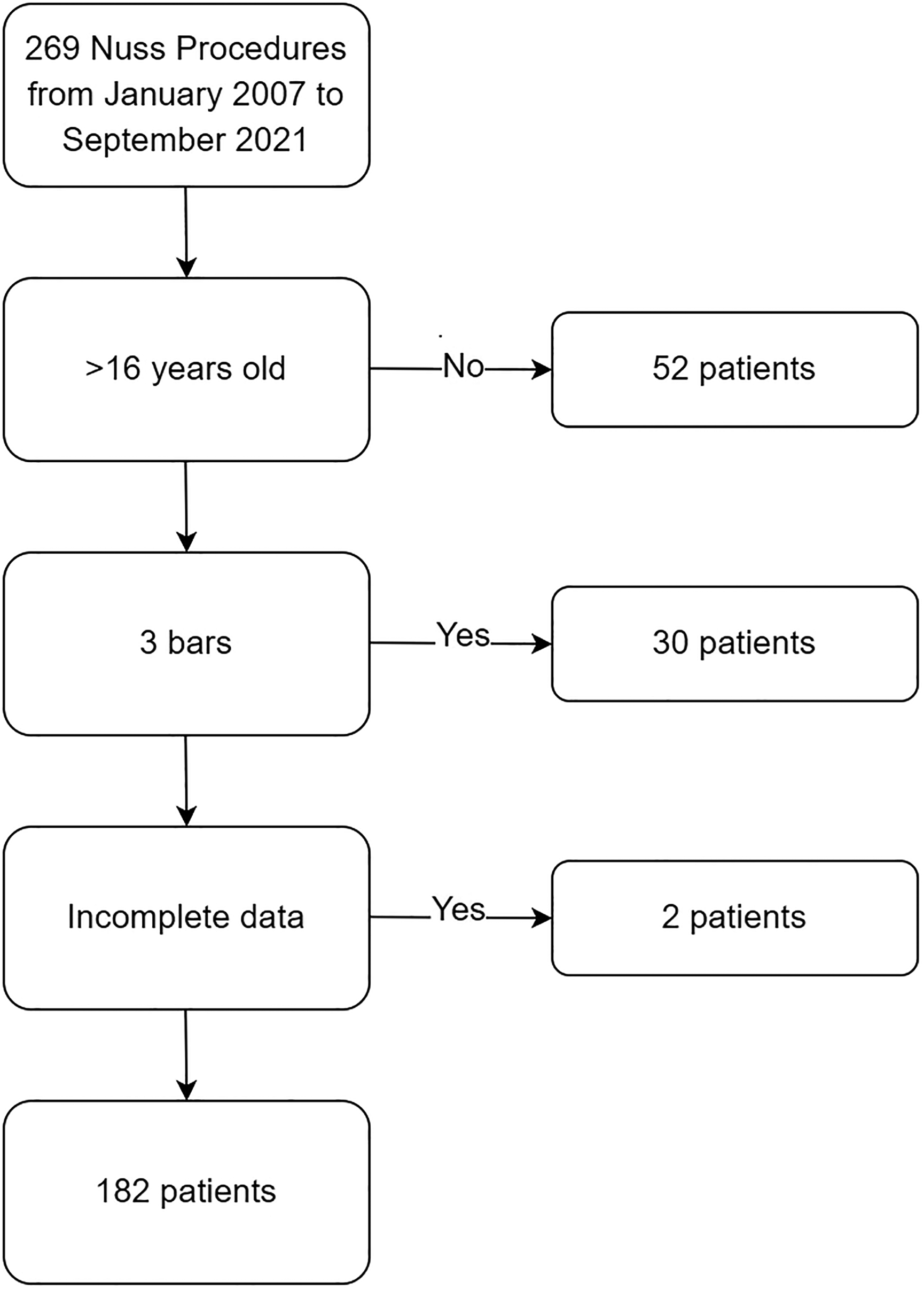
Flow chart describing patient cohort and patient selection.
General and perioperative characteristics of the patients.
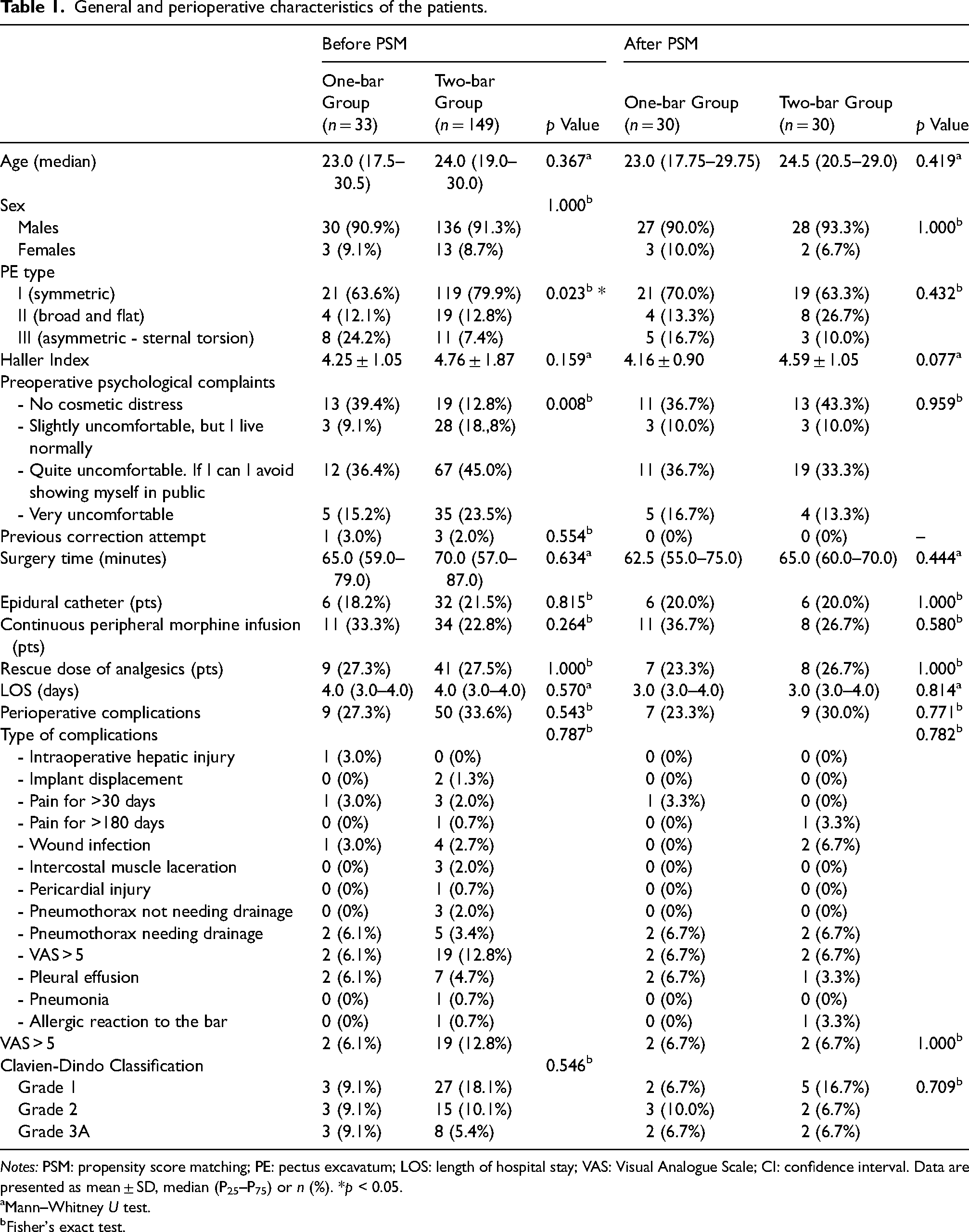
Notes: PSM: propensity score matching; PE: pectus excavatum; LOS: length of hospital stay; VAS: Visual Analogue Scale; CI: confidence interval. Data are presented as mean ± SD, median (P25–P75) or n (%). *p < 0.05.
Mann–Whitney U test.
Fisher's exact test.
Long-term results of the Nuss procedure are shown in Table 2. No patients had long-term complications nor bar displacement (needing removal or surgery). No patient was readmitted to the hospital or reoperate. One patient of the one-bar Group had recurrence (p = 1.000). No Bars in 25 patients of the one-bar Group (83.3%) and 24 of the two-bar Group (80.0%) had already been removed at the time of publishing (p = 1.000). Patient-reported QoL was improved or very much improved in 96.7% of patients in both groups. There was a difference between the two groups in the psychological effect of surgery (p = 0.031). In fact, more frequently, patients treated with two bars have no psychological complaints after surgery (93.3% vs. 73.3%).
Long-term results of Nuss procedure.
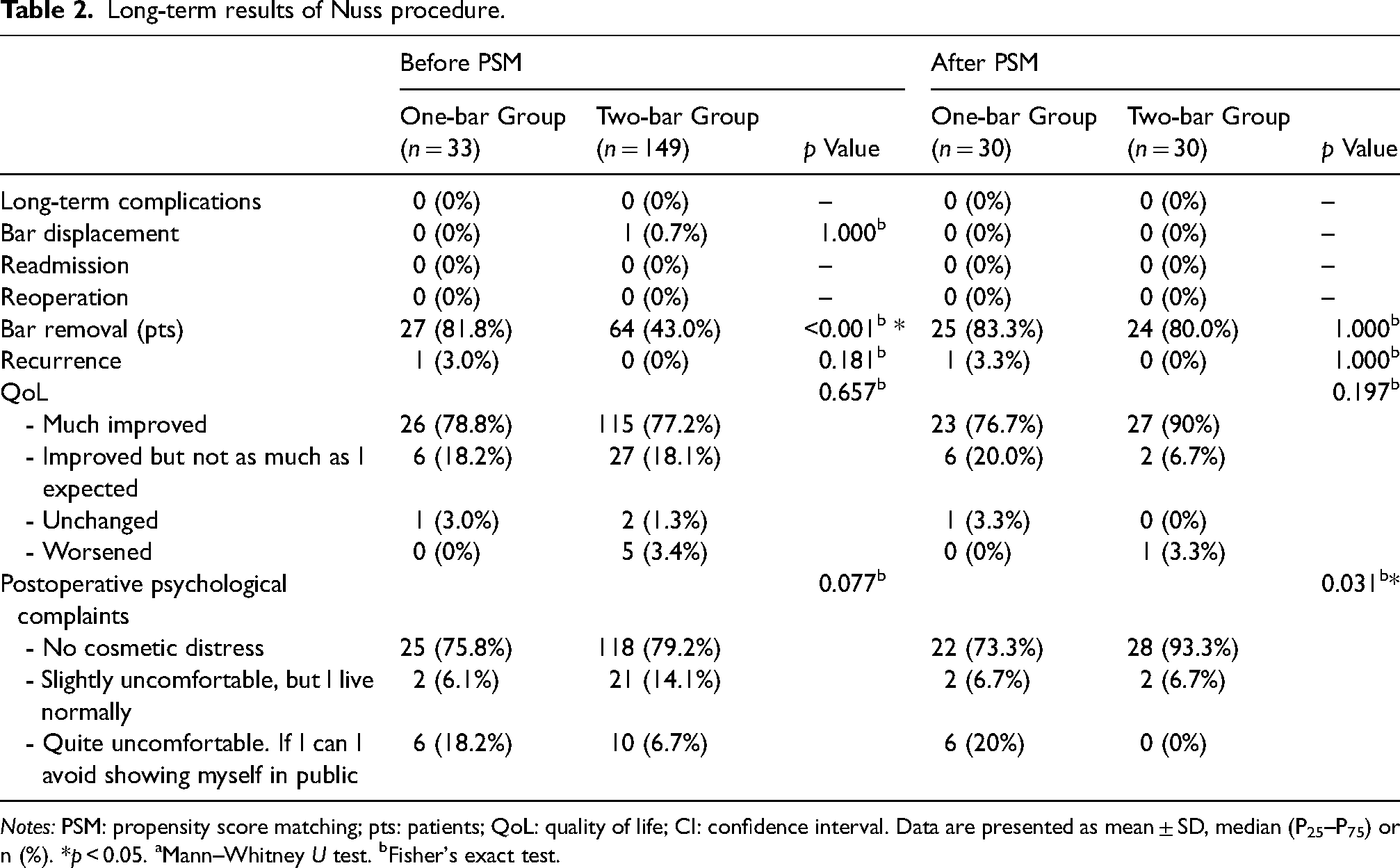
Notes: PSM: propensity score matching; pts: patients; QoL: quality of life; CI: confidence interval. Data are presented as mean ± SD, median (P25–P75) or n (%). *p < 0.05. aMann–Whitney U test. bFisher's exact test.
Discussion
The Nuss procedure has gained popularity in the past decades and nowadays is considered the gold standard treatment technique to correct PE, thanks to less invasiveness, shorter operative time, minimal blood loss and comparable postoperative morbidity to Ravitch procedure.14,15 Nevertheless, the cosmetic result is often not perfectly satisfactory when one bar is applied, thus we recently standardized the surgery by routinely applying two bars, regardless of the type of PE. Still, multiple bar insertion may determine more postoperative complications and morbidities.6,8 Thus, our intention was to retrospectively evaluate the difference between patients treated with one or two bars.
While there is evidence suggesting that surgical correction of PE can lead to improvements in immediate cardiac and lung parameters,2,16 it is crucial to recognize that a significant motivation for surgery in most patients is to address cosmesis and enhance self-esteem and body perception. Therefore, evaluating postoperative QoL becomes paramount in assessing the success of PE correction procedures. Our study underscores the importance of QoL assessment by demonstrating that the use of two bars did not result in increased cosmetic distress or significant changes in QoL compared to one bar (p = 0.197). Notably, a substantial proportion of patients in both groups experienced significant improvements in QoL postoperatively, with 90% of the two-bar group and 76.6% of the one-bar group reporting enhanced QoL.
Furthermore, our findings highlight the significant impact of surgery on psychological well-being, with a statistically significant difference observed between the two groups (p = 0.031). Specifically, a higher proportion of patients treated with two bars reported no psychological complaints postoperatively (93.3% vs. 73.3% in the one-bar group), suggesting that the use of two bars may offer psychological benefits regardless of the type of PE. This aligns with existing literature 7 and our clinical experience, which support the notion that two-bar placement enables more effective correction of extensive defects, leading to an enhanced subjective impression of the surgery and improved patient satisfaction. Nevertheless, it is noteworthy to delve deeper into the pre-PSM analysis, where we observed that postoperative psychological complaints exhibited no statistically significant differences between the groups. This finding, while seemingly counterintuitive, underscores the nuanced interplay between sample size and the detection of subtle psychological outcomes. The lack of statistical significance before PSM could be attributed to the relatively small sample size, which may have limited the power to detect differences in psychological well-being accurately.
However, despite the absence of statistically significant differences before PSM, it is essential to recognize the potential implications of these findings. Small sample sizes inherently pose challenges in detecting subtle variations, particularly in outcomes as multifaceted as psychological well-being. Thus, it serves as a reminder of the intricacies involved in interpreting psychological outcomes within the context of surgical interventions for PE.
Among preoperative characteristics of the patients, while no statistically significant difference in the Haller Index between the two groups was observed, it is notable that the Haller Index tended to be slightly higher in the two-bar group. Although this difference did not achieve statistical significance, it suggests a potential variation in the severity of chest wall deformity among the groups. While factors such as sample size or confounding variables may contribute to the lack of statistical significance, the elevated Haller Index in the two-bar group warrants careful consideration in interpreting our findings. A higher Haller Index may indicate that patients perceived their deformity as more severe preoperatively, which could influence their psychological outcomes and satisfaction post-surgery. This perception of a more severe deformity could lead to a greater psychological benefit from the correction, potentially skewing satisfaction results. Furthermore, the higher Haller Index may justify the intraoperative decision to use two bars, as it suggests a more severe anatomical defect that may require additional support for adequate correction. The use of two bars in these cases was more justified and perhaps necessary to achieve the desired surgical outcomes. Additionally, the initial overrepresentation of the asymmetrical type in the one-bar group was addressed through PSM, which included the type of anomaly as a matching criterion. This ensured that the differences in outcomes were not due to preoperative differences in PE type, allowing for a fair comparison between the one-bar and two-bar groups. This approach provides a more robust evaluation of the impact of using one versus two bars in the Nuss procedure. This highlights the importance of considering both objective and subjective measures in assessing the effectiveness of surgical interventions.
Regarding the secondary endpoints of the study, recurrence and complications were assessed as important indicators of the long-term efficacy and safety of the Nuss procedure. Our findings revealed that only one patient in the one-bar group experienced recurrence, although this result did not reach statistical significance (p = 1.000). While the lack of statistical significance may be attributed to the small sample size, it is noteworthy that the incidence of recurrence was low in both groups, suggesting a favourable outcome of the Nuss procedure in terms of recurrence prevention. Additionally, as previously reported, 11 our practice does not advocate for the immediate removal of bars at 3 years postoperatively; indeed, a significant proportion of our patients still have bars in place, which may influence this result. Furthermore, the comprehensive evaluation of complications remains crucial in determining the safety profile of the Nuss procedure. In fact, despite its low invasiveness, Nuss procedure is not free from complications. 17 We found no differences in terms of short- and long-term complications between the two groups, indicating comparable safety profiles. Swee et al. 18 report an increase of postoperative complications when multiple bars are applied, which is in contrast to our results. This is probably due to progressively increased experience and standardization of the procedure and the absence of the use of stabilizers. Among complications, the most common one is pain.19,20 Sacco Casamassima et al. reported that severe pain occurred in 10% of their patients and may influence the long-term patient satisfaction after PE correction. 19 In the study published by De Loos et al., chronic pain lasting over 3 months and relieved by additional analgesia was the most common minor complication and occurred significantly more often among adults. 20 Only two patients in each group experienced perioperative significant pain, requiring infusion of intravenous morphine, without respiratory complications associated. However, the low incidence of complications in both groups should be interpreted in the context of the relatively small sample size and the need for continued surveillance to capture potential rare complications.
As anticipated, our concerns on this topic have been echoed in recent discussions. Notably, Dr Donald Nuss himself has questioned the necessity of universally applying two bars for all patients. 21 He suggested that a single bar may suffice for many cases, advocating for decisions to be individualized based on specific patient characteristics and deformity severity. This underscores the importance of a tailored approach in the Nuss procedure, considering both clinical and cosmetic outcomes on a case-by-case basis. Our data contribute to the ongoing discussion and should be considered to enhance our understanding of this topic, though they should be interpreted with caution.
One of the main concerns of our study is the lack of generalizability which stems from the imbalance in group sizes, primarily driven by the scarcity of comparators in the one-bar group compared to the two-bar group. Specifically, the matched groups are heavily influenced by the small number of patients in the one-bar group, resulting in almost complete inclusion in the matched sample. Conversely, the two-bar group exhibits a different pattern, with a notable portion remaining unmatched. This disparity in group representation raises concerns about the representativeness of our findings, as the overrepresentation of one group may skew the results and limit the applicability of our conclusions to broader populations. It is essential to acknowledge this imbalance and its potential impact on the generalizability of our study's findings, as it underscores the need for caution when interpreting and extrapolating the results to other patient populations or clinical settings. Further discussion and exploration of this imbalance are warranted to provide a comprehensive understanding of the study's limitations and implications.
The study limitations are as follows. This is a retrospective study, despite the PSM analysis may mitigate its inherent bias. Nevertheless, it cannot eliminate the impact of unmeasured confounding variables that may still influence the outcome. Furthermore, it is important to note that the study did not include a comprehensive psychological evaluation, which might encompass assessments of depression, anxiety or other psychological measures. The small sample size of the one-bar group before PSM (33 vs. 149 in the other group) may affect the robustness of our findings and limit the generalizability of the results to broader populations. Moreover, it should be noted that, although a brief unstructured interview was conducted before the surgery, the questionnaires were administered postoperatively, resulting in retrospective data collection; this sequential timing might introduce recall bias and affect the accuracy of participant responses, particularly in terms of preoperative perspectives and experiences. Finally, we included patients over a large time span, during which we gained experience and dexterity.
Conclusions
Our study reveals that patients undergoing the Nuss Procedure for PE with two bars exhibit comparable clinical outcomes and QoL to those with one bar. However, patients with two bars may have higher levels of psychological well-being and satisfaction, indicating potential benefits associated with this approach. It is essential to interpret these findings with caution due to intrinsic limitations of the study, including the small size of the one-bar group and the possibility of unrecognized bias. Further research with larger sample sizes and rigorous study designs is warranted to confirm these observations.
Supplemental Material
sj-docx-1-aan-10.1177_02184923241272887 - Supplemental material for Patient satisfaction after Nuss procedure with one or two bars in young adults: A propensity score–matched cohort study
Supplemental material, sj-docx-1-aan-10.1177_02184923241272887 for Patient satisfaction after Nuss procedure with one or two bars in young adults: A propensity score–matched cohort study by Alessio Campisi, Riccardo Giovannetti, Giovanni Falezza, Emanuele Voulaz, Alessandro Lonardoni and Maurizio Valentino Infante in Asian Cardiovascular and Thoracic Annals
Supplemental Material
sj-docx-2-aan-10.1177_02184923241272887 - Supplemental material for Patient satisfaction after Nuss procedure with one or two bars in young adults: A propensity score–matched cohort study
Supplemental material, sj-docx-2-aan-10.1177_02184923241272887 for Patient satisfaction after Nuss procedure with one or two bars in young adults: A propensity score–matched cohort study by Alessio Campisi, Riccardo Giovannetti, Giovanni Falezza, Emanuele Voulaz, Alessandro Lonardoni and Maurizio Valentino Infante in Asian Cardiovascular and Thoracic Annals
Footnotes
Author contributions
Alessio Campisi: conceptualization, data curation, formal analysis, patient treatment and follow-up, data collection, writing, review, validation and final approval. Riccardo Giovannetti: patient treatment and follow-up, data collection, review, final approval. Giovanni Falezza: patient treatment and follow-up, data collection, review and final approval. Emanuele Voulaz: patient treatment and follow-up, data collection, review and final approval. Alessandro Lonardoni: patient treatment and follow-up, data collection, review and final approval. Maurizio Infante: resources, conceptualization, supervision, writing, review, validation and final approval.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Institutional Research Ethics Boards of University and Hospital Trust, Verona (N° 2528-CESC). All figures and tables are original and have not been published before.
Informed consent
Written informed consent was obtained from all patients.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.