
Abstract
Background
Antiphospholipid syndrome and systemic lupus erythematosus are autoimmune inflammatory conditions involving multiple organs and sharing various clinical aspects. Owing to the scarcity of data about the surgical outcomes of these autoimmune disorders, we conducted a systematic review to assess the outcomes for patients with these diagnoses undergoing heart surgery and contextualize the findings regarding high-risk cardiac surgeries.
Methods
A thorough search of PubMed, Embase and Scopus used Preferred Reporting Items for Systematic Reviews and Meta-Analyses standards to find articles that involved patients who underwent heart surgery and had antiphospholipid syndrome and systemic lupus erythematosus. Inclusion criteria concentrated on a definitive diagnosis, while case reports and studies lacking data on surgical outcomes were excluded. Using the Joanna Briggs Institute's methodologies, quality evaluation categorized studies according to their risk of bias.
Results
Fourteen studies with 277 patients and a prevalence of middle-aged females met the inclusion criteria out of 6381 papers. The major preoperative comorbidity in the cohort was a history of thromboembolic events (43%). Thromboembolic complications (6%) and catastrophic antiphospholipid syndrome (2%), even with appropriate anticoagulation, were notable early post-operative outcomes. Six percent of people died within 30 days. Data from follow-up studies showed a 14% death rate and a 23% frequency of thromboembolic events.
Conclusions
With the striking exception of a high frequency of thromboembolic complications and catastrophic antiphospholipid syndrome, surgical results in patients with antiphospholipid syndrome and systemic lupus erythematosus are analogous to those in high-risk cardiac procedures. Improving surgical care for this susceptible population requires an understanding of these hazards.
Keywords
Introduction
Antiphospholipid syndrome (APS) is a multisystem autoimmune disease distinguished by a group of antibodies, including anticardiolipin antibodies, anti-beta2-glycoprotein 1 antibodies and lupus anticoagulant, broadly known as antiphospholipid antibodies (aPL). 1 The condition is characterized by antibody-mediated inflammation and hypercoagulability, which manifest as recurrent vascular thrombosis and difficulties during pregnancy. 1 Antiphospholipid syndrome may occur as primary APS or as secondary APS, often in association with other systemic autoimmune diseases, the most common being systemic lupus erythematosus (SLE). 1 Various studies have reported an incidence of APS between 1 and 2 cases per 100,000 and a prevalence of 40–50 cases per 100,000. The mortality in APS patients is 50–80% greater than in the general population. 2
Systemic lupus erythematosus is a systemic autoimmune disease affecting multiple organs and shares several clinical similarities with APS. 3 Relatively 36% of APS patients may develop SLE, and 20–40% of SLE patients may have aPL. 3 Despite their differences, APS and SLE are often considered allied disorders, and the development of APS in SLE or vice versa contributes to increased organ damage and mortality.3–5 Usual cardiac manifestations of APS include cardiac valvular thickening and vegetation, which can lead to valvular dysfunction, coronary artery disease, intracardiac thrombus, pulmonary hypertension and left ventricular diastolic dysfunction.5,6 The prevalence of heart valve disease (HVD) in APS ranges from 10% to 60%, with 4–6% of patients eventually requiring surgery. 5 In addition to HVD, patients with other cardiac manifestations may require surgeries such as coronary artery bypass grafting (CABG), intracardiac thrombectomy, left ventricular assist device implantation and heart transplantation. 5 Data on surgical outcomes in these patients are scarce because APS is uncommon, and most of the literature consists of case reports.7–9 To the best of our knowledge, there is no review available on the outcomes in APS patients undergoing heart surgery, except for a meta-analysis published by Gorki et al. in 2008 that included 39 case reports. 10 Furthermore, the longer life expectancy of these individuals because of the improvements in medical care could raise the need for heart surgery. 11 Considering this, we evaluated the outcomes of patients with APS and SLE undergoing heart surgery through a systematic review with the objective of determining the thromboembolic complications in such patients.
Material and methods
Search technique
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 12 and the Meta-analysis of Observational Studies in Epidemiology criteria 13 were adhered to for this review (Supplementary file S1 and S2). We searched the articles in PubMed, Embase and Scopus using the following terms:
Coronary artery bypass grafting OR coronary artery surgery OR cardiac surgery OR heart valve surgery OR heart valve prosthesis implantation OR valvular heart disease AND antiphospholipid syndrome OR Hughes syndrome OR antiphospholipid antibody syndrome OR lupus anticoagulant syndrome OR systemic lupus erythematosus OR SLE. The additional references in sub-references and similar articles were also searched. The last search of the databases was done in July 2024.
Selection criteria
The following were the inclusion criteria for the studies included in this review:
Articles reporting cardiac surgery on patients with a definite diagnosis of APS or SLE. Articles in the English language. Case reports, reviews and editorials. Associated with other diseases such as Q fever, basal cell carcinoma and hepatitis C. Consisting of pregnant patients. Studies with no description of surgical outcomes. Studies in patients with aPl only and not definitive APS.
The articles were excluded as follows:
Definitions
Primary APS
The APS occurs in isolation.
Secondary APS
Antiphospholipid syndrome is secondary to other autoimmune disease mainly SLE.
Extraction of data
The following information was gathered independently by two authors from each included study: authors’ names, study duration, type of study, sample size, autoimmune disease, type of cardiac surgery and outcomes. Disagreements were settled by dialogue or by the involvement of a third investigator. Zotero, the reference management software, was used for citation and management of included studies.
Quality and risk of bias assessment of included studies
Studies that were included were evaluated for quality and risk of bias by two independent reviewers. Discussion was used to settle disagreements between the reviewers at various stages of the review. The Joanna Briggs Institute (JBI) Critical Appraisal tools for case series and cohort study which are made up of 10 and 11 yes/no/unclear or not applicable questions, respectively, were used to assess the standard of the included studies. 14
For a succinct assessment of the general quality of the included studies, these were categorized as follows: 1. Low risk of bias (studies that met at least 75% of the standards for quality). 2. Studies with a moderate risk of bias (compliant with 50%–74% of the quality standards). 3. Studies with a high risk of bias (those that only complied with less than 49% of the standards for quality). 15
Data analysis
The demographics and clinical variables were reported using descriptive statistics. For continuous variables, we used mean and standard deviation, and for dichotomous variables, we used frequencies and percentages. The included studies were evaluated by two independent researchers for the methodological quality and risk of bias using the JBI risk of bias checklist.
Results
Study selection
A total of 6381 articles were identified through the electronic search. After removing duplicates, 5264 articles were screened by two independent reviewers. Following a review of titles and abstracts, 5247 articles were excluded. Full texts of the remaining 17 studies were retrieved, and 16 were assessed for eligibility. Two publications were eliminated following an independent review, leaving 14 research studies to be included in this analysis (Table 1).
Characteristics of included studies.
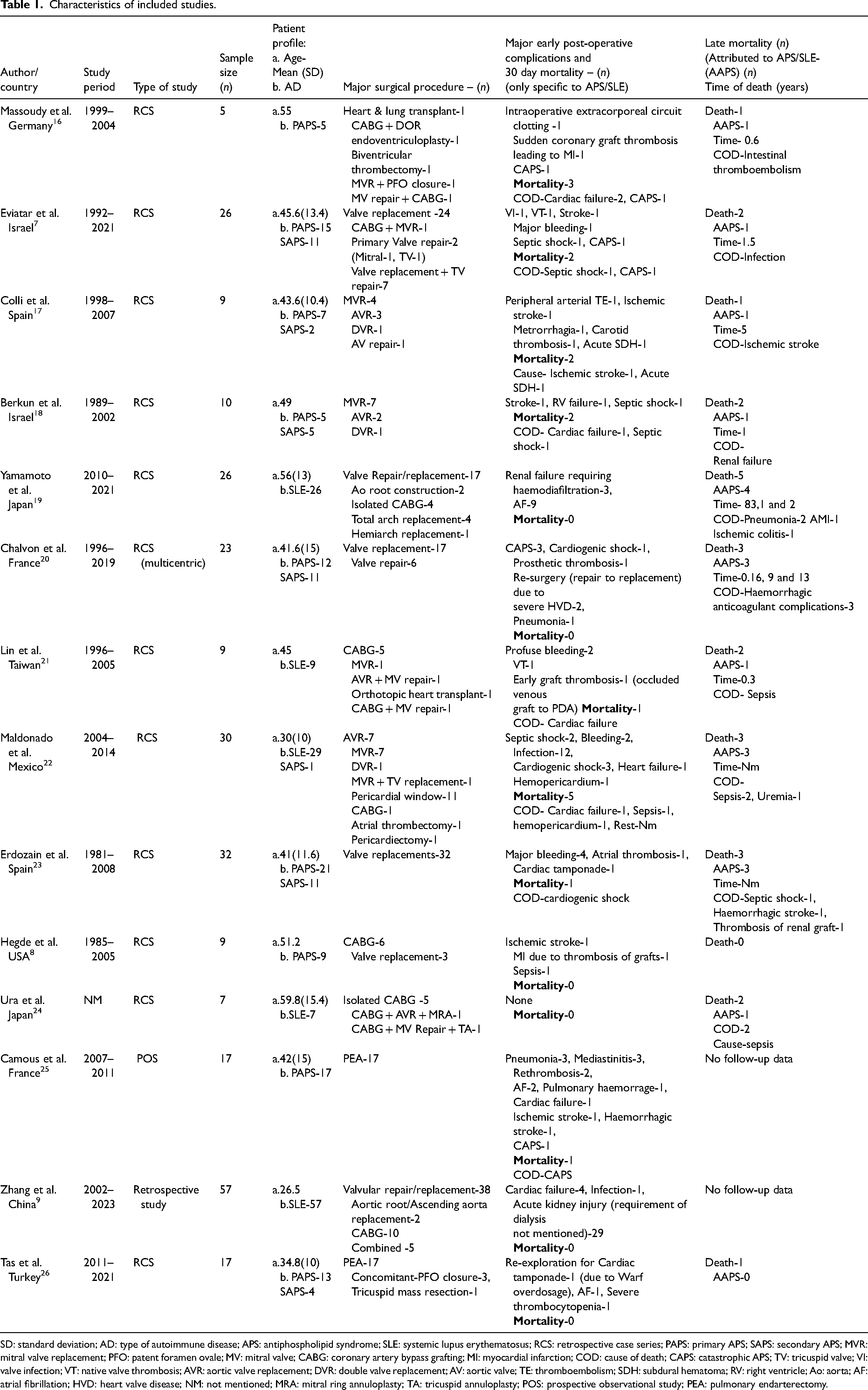
SD: standard deviation; AD: type of autoimmune disease; APS: antiphospholipid syndrome; SLE: systemic lupus erythematosus; RCS: retrospective case series; PAPS: primary APS; SAPS: secondary APS; MVR: mitral valve replacement; PFO: patent foramen ovale; MV: mitral valve; CABG: coronary artery bypass grafting; MI: myocardial infarction; COD: cause of death; CAPS: catastrophic APS; TV: tricuspid valve; VI: valve infection; VT: native valve thrombosis; AVR: aortic valve replacement; DVR: double valve replacement; AV: aortic valve; TE: thromboembolism; SDH: subdural hematoma; RV: right ventricle; Ao: aorta; AF: atrial fibrillation; HVD: heart valve disease; NM: not mentioned; MRA: mitral ring annuloplasty; TA: tricuspid annuloplasty; POS: prospective observational study; PEA: pulmonary endarterectomy.
The PRISMA flow diagram (Figure 1) illustrates the study selection process.
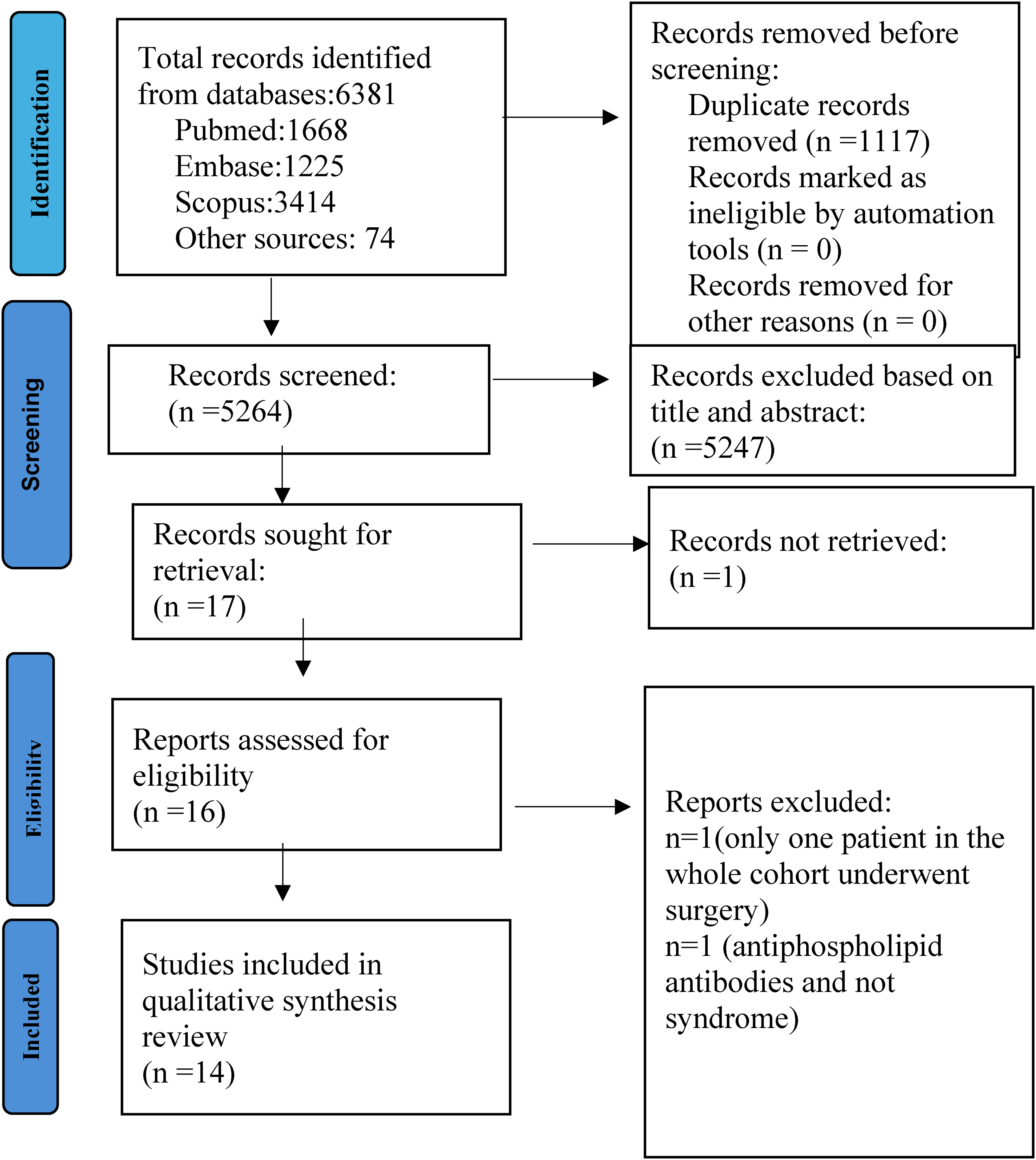
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart for study selection.
The demographic characteristics of 277 patients with APS/SLE revealed a predominantly female cohort (82%) with an average age of 44.3 years. The APS was present in 54% (primary: 38% and secondary: 16%) and SLE (46%), with a mean disease duration of 13.3 years. Preoperative comorbidities included thromboembolic events (43%), renal dysfunction (35%), neurological symptoms (27%) and obstetric problems (20%). There was extensive use of medications, such as immunosuppressants (27%), aspirin (33%), vitamin K antagonists (39%), corticosteroids (65%) and aspirin (33%).
Valve replacements or repairs accounted for 63% of intraoperative procedures. A lower percentage underwent isolated CABG (11%), aortic arch replacement (2%), aortic root reconstruction (1%) and heart transplant (1%) treatments. Mechanical prosthetic valves were used in 53% of patients. The baseline characteristics and intraoperative data are outlined in Table 2.
Preoperative characteristic and intraoperative data of APS/SLE patients (n = 277).
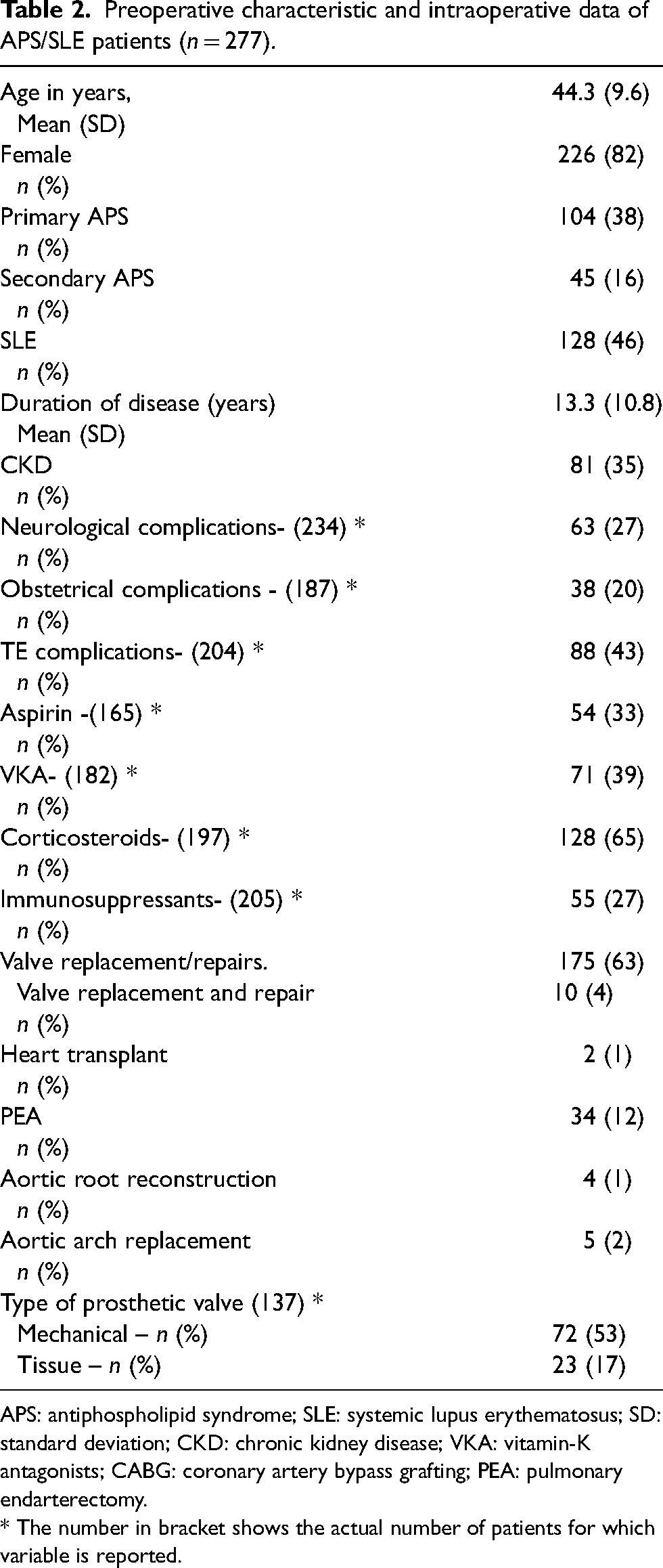
APS: antiphospholipid syndrome; SLE: systemic lupus erythematosus; SD: standard deviation; CKD: chronic kidney disease; VKA: vitamin-K antagonists; CABG: coronary artery bypass grafting; PEA: pulmonary endarterectomy.
* The number in bracket shows the actual number of patients for which variable is reported.
The post-operative outcomes and follow-up data are presented in Table 3.
Post-operative outcomes.

MI: myocardial infarction; PVT: prosthetic valve thrombosis; TE: thromboembolism; APS: antiphospholipid syndrome; SLE: systemic lupus erythematosus; LSE: Libman–Sach endocarditis; NVE: native valve endocarditis; PVE: prosthetic valve endocarditis; BVD: biological valve deterioration; ECC: extracorporeal circuit; RE: re-exploration; CAPS: catastrophic antiphospholipid syndrome; ARDS: acute respiratory distress syndrome; AF: atrial fibrillation; FU: follow up.
The incidence of thromboembolic and haemorrhagic complications was 6%. Ischemic stroke (24%), coronary graft (18%) and native valve thrombosis (12%) were the most common thromboembolic complications. Sepsis was observed in 9%, renal failure in 12%, atrial fibrillation in 4%, cardiogenic shock in 3% and catastrophic APS (CAPS) in 2%. Thirty-day mortality was listed at 6%, due to cardiogenic shock (35%), CAPS (18%), septic shock (18%) and haemorrhagic events (12%).
Follow-up data for 184 patients over a median duration of 37 months disclosed thromboembolic complications in 23%, redo surgery in 5% and a mortality rate of 14%. Sepsis, thromboembolic and haemorrhagic events were the most common causes of late death.
Risk of bias
The mean of the two reviewers’ scores was calculated and the risk of bias was determined as per pre-defined criteria. The JBI checklist with mean reviewer's scores and risk of bias is available as supplementary material (Supplemental Table 3). There is no significant bias risk in any of the studies. Most of the studies7–9,16–23,26 fell into the low-risk bias group and 2 studies24,25 had moderate-risk bias.
Discussion
This systematic review highlights the clinical outcomes of patients with APS/SLE who underwent cardiac surgery. This systematic review mainly includes case series on cardiac surgery outcomes in APS/SLE patients. Furthermore, we examined the findings considering high-risk cardiac procedures, which are currently a major spectrum for cardiac surgeons around the globe. 27 The key findings of the review are outlined below:
This cohort mainly consisted of middle-aged females, in tune with the known epidemiology of APS and SLE.2,3 The female preponderance is due to certain genes expressed on the X chromosome, sex hormones and pregnancy-induced immunological variations. 28 The most frequent cause of secondary APS was SLE, as known in existing data. 1 On average, patients underwent surgery 13.3 years after the diagnosis of APS/SLE, reflecting the gradual progression of valvular damage in these diseases.3,8 Significant preoperative comorbidities such as renal dysfunction and thromboembolic events accompanied by widespread use of medications such as anticoagulants, corticosteroids and immunosuppressants may make the surgeons apprehensive.3,17,18,29,30
The cohort underwent a full spectrum of cardiac surgeries, with two-thirds undergoing valve replacements or repairs. The prevalence of valvular involvement, ranging from thickening to sterile vegetation known as Libman–Sacks endocarditis, varies from 10% to 80%, with approximately 4–6% eventually requiring valve replacement surgery.5,17,23,30 Repeated episodes of thrombosis and inflammation may lead to fibrosis and calcification, contributing to valve damage.5,30 The mechanical valve was the prosthetic valve of choice in more than 50% of patients. The optimal choice of valve type for these patients remains undetermined.10,23 Considering that the APS patients are younger, and patients require long-term anticoagulation, mechanical valves seem to be a preferable choice. Besides, aPL may cause immunologic damage to tissue valves.5,17,20,31 However, further long-term studies are justified to draw a definitive verdict.
The incidence of post-operative outcomes: renal failure, sepsis, haemorrhagic complications and cardiogenic shock was compared to outcomes reported by the Society of Thoracic Surgeons database 32 and high-risk cardiac surgeries.33–35 The distinctive outcomes revealed by the review were thromboembolic complications and CAPS.
The thromboembolic complications included ischemic stroke (24%), coronary graft thrombosis (18%), native valve, arterial thrombosis of the limbs and pulmonary artery thrombosis, each occurring in 12%. These findings underline the prothrombotic state innate of APS/SLE, exacerbated by the withdrawal of vitamin K antagonists before surgery. 17 The pathogenetic mechanisms contributing to the hypercoagulability associated with APS include stimulation of the extrinsic coagulation system, formation of immune complexes mediated by autoantibodies, complement activation, inhibition of proteins C and S and oxidative stress. 1 Notably, the incidence of stroke in our study exceeded that reported in the literature of 1.4–14%. 36 In addition to conventional risk factors such as age over 51 years, duration of cardiopulmonary bypass and a previous history of stroke, the presence of arteriopathy is a significant variable for stroke. 35 The prothrombotic state in APS, combined with autoantibody-mediated thrombosis and atherogenesis, contributes to cerebrovascular disease, particularly in younger patients.2,5,30 The combination of APS-related arteriopathy and cardiopulmonary bypass explains the high incidence of stroke in these patients. 37 In our review, 3 out of 37 patients who underwent CABG developed early graft thrombosis, with 2 of them experiencing post-operative myocardial infarction (MI).8,16,21 The above three patients had occlusion of venous grafts, and one patient succumbed to death due to myocardial failure. 16 The incidence of perioperative MI in post-cardiac surgical patients varies from 1% to 10%, attributed to multiple grafts and non-graft-related etiologies. 38 While the overall incidence of early graft failure after CABG is 12%, only 3% are clinically evident. A prior history of stroke, duration of surgery and number of grafts are independent predictors of early graft failure. 39 Graft thrombosis is the most common cause of early graft failure. 40 Arampatiz et al. reported in-hospital asymptomatic graft occlusion rates of 6.8% and suggested that the inflammatory and prothrombotic state following recent MI may contribute to graft failure. 40 The high occurrence of early graft thrombosis and perioperative MI in our review may be connected to the pro-inflammatory and procoagulant activities associated with APS. 1 Additionally, the presence of multiple comorbidities, such as SLE nephritis, diabetes mellitus and dyslipidemia in SLE patients, may explain early graft occlusion. 21 The absence of collateral flow in cases of graft failure due to existing myocardial microvascular thrombosis may also contribute to the high incidence of post-operative MI.5,40
Native valve thrombosis occurred in two patients7,16 in our review, one of whom developed an aortic valve thrombus 6 days after surgery and ultimately died. 16 Interestingly, all patients were on anticoagulants. A recent systematic review identified 74 cases of native aortic valve thrombosis, most associated with APS. 41 The authors concluded that the presence of aortic valve thrombosis is linked to unfavourable outcomes and increased hospital mortality. Aside from the studies,7,16 we found no additional data in the literature regarding native valve thrombosis as a post-operative complication of cardiac surgery.
Less than 1% of patients experience the severe form of APS known as CAPS, which has a death rate more than 50%.16,25 It is triggered by an extensive thrombotic storm that typically comes on by surgery and preoperative anticoagulant withdrawal. This results in widespread ischemia and multiorgan failure.10,16 In our review, a total of six patients developed CAPS7,16,20,25 of whom three died.7,16,25 One patient died due to exaggerated thromboembolic events, 16 another from limb, mesenteric, renal and splenic ischemia, 7 and the last succumbed to cerebral complications. 25 Despite receiving standard treatment for CAPS – including aggressive anticoagulation, intravenous immunoglobulins, corticosteroids and plasma exchange – these patients could not be saved. Strategies for optimal perioperative anticoagulation in APS patients include minimizing the duration of anticoagulation cessation, doubling the activated coagulation time to monitor heparin concentration during cardiopulmonary bypass and reducing the use of protamine.10,23 The optimal INR (International Normalized Ratio) is usually maintained between 2 and 3, as a high INR (3–4) has not proved beneficial in such patients. 42
The overall mortality rate in our review was 6%, with the leading causes of death comprising cardiogenic shock (35%),16,18,21,22,23 CAPS (18%),7,16,25 septic shock (18%),7,18,22 haemorrhagic events (12%)17,22 and ischemic stroke (6%). 17 Chan et al. found that in 11,190 STS-indexed cardiac operations, which comprised both isolated and combination procedures, the total operational mortality was 2.4%. 43 The operative mortality rate for patients undergoing high-risk cardiac surgery was 4.6% in research by Huckaby et al., 44 though it was 7.5% for patients suffering from severe left ventricular dysfunction. 33 In a study by Metkus et al., the rate of mortality among critically ill patients undergoing heart surgery was 9.4%, and cardiogenic shock was the most common cause of death [R-6]. 45 Thus, the mortality in this subset is comparable to other high-risk patients. However, thromboembolic events associated with CAPS as causes of death are unique to this cohort of patients.
The follow-up details over a median duration of 37 months disclosed a mortality rate of 14% with only 18 patients (10.7%) dying due to fundamental autoimmune disease.7,16–24 This is lower than as delineated in the literature 46 and may be due to the small sample size in our review. Thromboembolic events account for a large percentage of deaths (24%) in follow-up, highlighting the continued danger these patients face even with prescribed anticoagulation.
The above insights had valuable ramifications for the surgeons. Firstly, this cohort of patients is younger, with multiple comorbidities, and may require perioperative management by multidisciplinary healthcare professionals. Secondly, the post-operative outcomes and death rates are similar to those of other high-risk cardiac procedures, apart from thromboembolic events and CAPS, which are specific to these patients. Finally, the same problems continued during the follow-up, emphasizing the necessity of customized anticoagulation plans and continuous monitoring to successfully manage late complications.
Limitations
Most of the studies included in this review were conducted in single centers and lacked multiple data points. As most of these studies were retrospective case series with small sample sizes, statistical analysis was not feasible, and the results could not be extrapolated to the broader population. The differences in the severity of the autoimmune disease and surgical procedures in the included studies may have influenced the outcomes. Moreover, the studies were lacking in the definitions of surgical outcomes, which may have affected our analysis. The small sample size limited our ability to provide separate results for APS and SLE patients and to compare their outcomes. Despite these limitations, the information gathered from these articles is valuable, particularly given the rarity of the disease and the limited available literature.
Conclusion
The surgical outcomes of patients with APS/SLE undergoing cardiac surgeries are comparable to other high-risk cardiac surgeries with thromboembolic complications and CAPS detected as unique post-operative problems. Further studies are warranted to develop tailored strategies that can effectively mitigate these risks and improve surgical outcomes for patients with APS/SLE undergoing cardiac procedures.
Supplemental Material
sj-docx-1-aan-10.1177_02184923251321066 - Supplemental material for Surgical outcomes of cardiac surgery in patients with antiphospholipid syndrome and systemic lupus erythematosus: A systematic review
Supplemental material, sj-docx-1-aan-10.1177_02184923251321066 for Surgical outcomes of cardiac surgery in patients with antiphospholipid syndrome and systemic lupus erythematosus: A systematic review by Rajat Agarwal, Shiv Mudgal, Smarakranjan Rout and Amiy Arnav in Asian Cardiovascular and Thoracic Annals
Supplemental Material
sj-docx-2-aan-10.1177_02184923251321066 - Supplemental material for Surgical outcomes of cardiac surgery in patients with antiphospholipid syndrome and systemic lupus erythematosus: A systematic review
Supplemental material, sj-docx-2-aan-10.1177_02184923251321066 for Surgical outcomes of cardiac surgery in patients with antiphospholipid syndrome and systemic lupus erythematosus: A systematic review by Rajat Agarwal, Shiv Mudgal, Smarakranjan Rout and Amiy Arnav in Asian Cardiovascular and Thoracic Annals
Supplemental Material
sj-docx-3-aan-10.1177_02184923251321066 - Supplemental material for Surgical outcomes of cardiac surgery in patients with antiphospholipid syndrome and systemic lupus erythematosus: A systematic review
Supplemental material, sj-docx-3-aan-10.1177_02184923251321066 for Surgical outcomes of cardiac surgery in patients with antiphospholipid syndrome and systemic lupus erythematosus: A systematic review by Rajat Agarwal, Shiv Mudgal, Smarakranjan Rout and Amiy Arnav in Asian Cardiovascular and Thoracic Annals
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.