
Abstract
Introduction
Tuberculosis (TB) is a rare cause of chylopericardium. Optimal management remains unclear.
Methods/Results
A 30-year-old Filipino male presented with recurrent massive pericardial effusions, with pericardiostomy revealing chylopericardium. Microbiologic TB studies were negative, and other etiologies were excluded. Pericardial fluid adenosine deaminase was elevated; anti-TB regimen was initiated, leading to resolution.
Discussion
There is no consensus about the optimal management of TB chylopericardium. Adenosine deaminase represents a useful test to diagnose TB in inflammatory, lymphocyte-predominant effusions, especially when other tests are negative. Failed conservative management merits more invasive approaches.
Conclusion
While data remain lacking, this case suggests that TB chylopericardium responds to anti-TB therapy.
Introduction
Chylopericardium is a rare condition in which there is an accumulation of chylous fluid in the pericardial cavity.1,2 Commonly, it is idiopathic, postoperative, or neoplastic. 3 Tuberculosis (TB) as a cause is rare, representing 3% of all cases.3,4 Optimal management remains unclear.
Results
We report a case of a 30-year-old Filipino male, initially asymptomatic, who was initially seen at the outpatient setting with an incidental finding of cardiomegaly on routine chest radiograph. A full transthoracic echocardiogram (TTE) was done subsequently revealing a large pericardial effusion, measuring 2.6 mm in its widest diameter. He had no previous TB infection, trauma, surgeries, radiotherapy, and cancer. He was then sent to the emergency room for appropriate management. Electrocardiogram showed low voltage complexes (Figure 1). A point-of-care cardiac ultrasound was done to confirm the large pericardial effusion and detect any echocardiographic signs of cardiac tamponade. Point-of-care cardiac ultrasound revealed no overt chamber collapse and tamponade, no signs of constriction, and normal chamber sizes (Figure 2). A wide differential of infectious and noninfectious etiology can be considered but given the indolent nature of presentation, a pathologic diagnosis through pericardial sampling is essential.
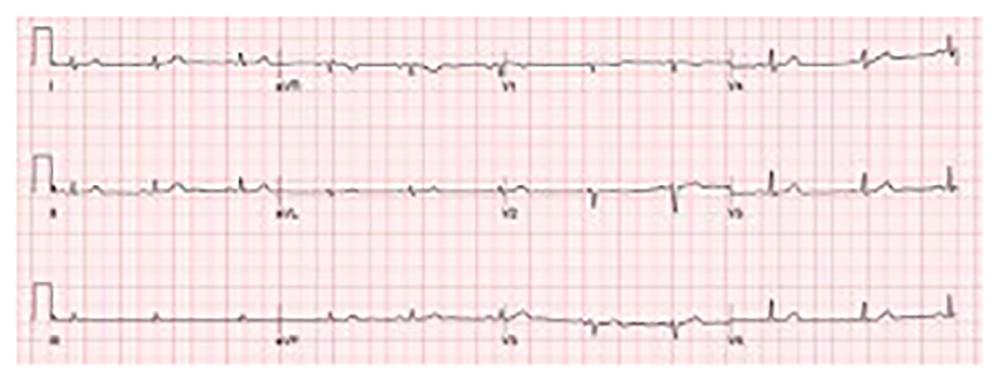
Electrocardiogram (ECG) showing low-voltage complexes.
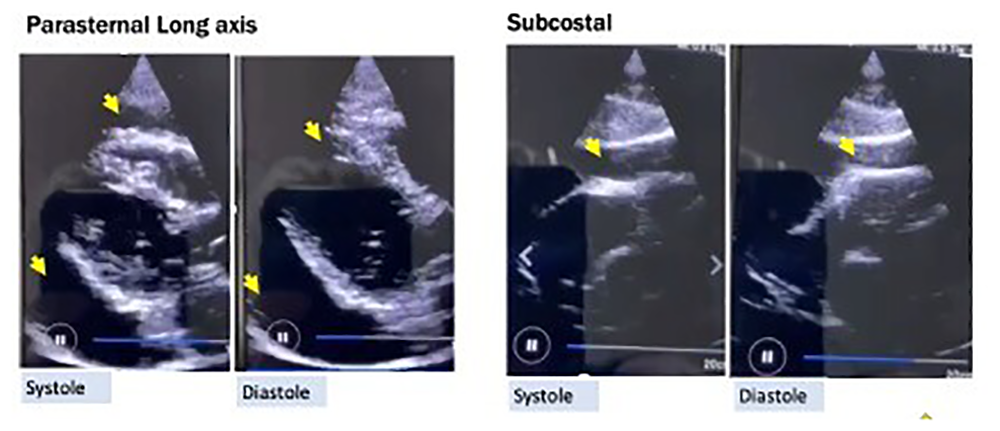
Point of care cardiac ultrasound finding. Yellow arrows point to large pericardial effusion.
The patient was admitted and underwent pericardiostomy, draining 1 liter of milky, creamy white fluid with elevated cholesterol (79 mg/dL) and triglyceride (323 mg/dL) counts, with white blood cell count showing a lymphocytic predominance (87%) (Figure 3). Pericardial fluid/serum total protein and LDH ratios suggested an exudative etiology. These findings were consistent with chylopericardium. Based on clinical grounds, patient's age, and epidemiology, possible differentials for this condition include idiopathic, malignancy, and TB. Pericardial biopsy and pericardial effusion cytology, and microbial testing, which included bacterial and fungal cultures, were negative; thyroid function tests and antinuclear antibody tests were also negative. An initial investigation for a tuberculous cause of the effusion was done with TB culture and Gene-Xpert MTB/RIF assay, which were both negative. A chest computed tomography scan revealed a tiny calcific density in the right upper lung lobe and a small noncalcified nodule in the left lower lobe, which were both likely inflammatory (Figure 4A). Lymphoscintigraphy revealed no lymphatic obstruction or injury (Figure 4B). In the absence of a bacteriologic and histopathologic diagnosis, idiopathic chylopericardium, representing the majority of its causes, was initially the leading consideration.
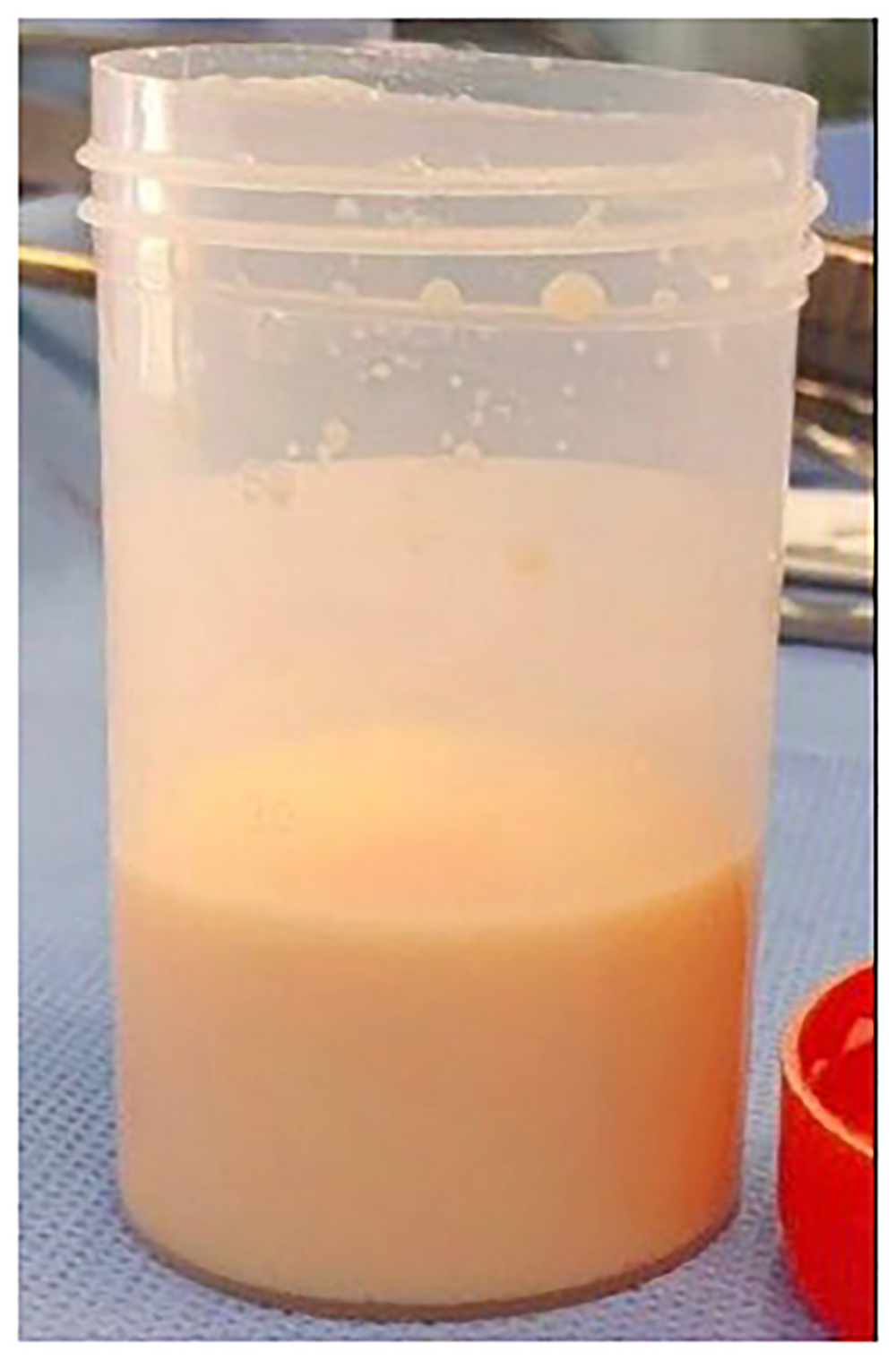
Gross finding from pericardiostomy. Milky/creamy white pericardial fluid typical of chylous pericardial effusion.
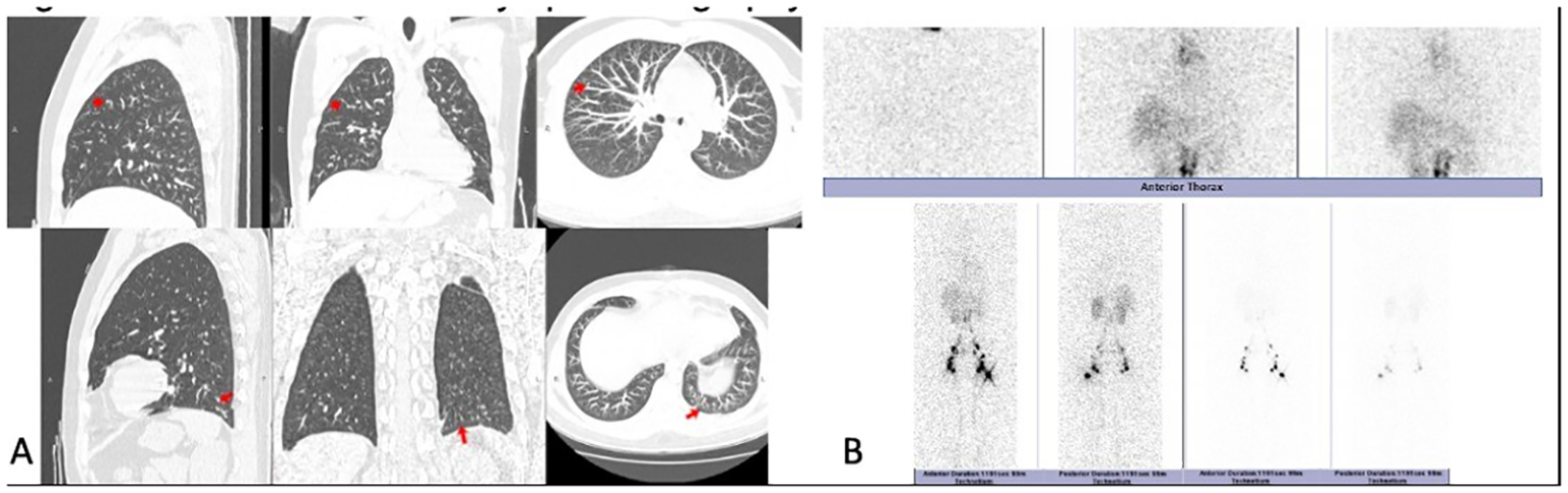
Chest computed tomography (CT) scan and lymphoscintigraphy findings. (a) CT scan with IV contrast. Upper clips: Tiny calcific density at the right upper lobe. Lower clips: Small noncalcified nodule at the left lower lobe. (b) Lymphoscintigraphy. No tracer collection in the thorax on static whole body and SPECT-CT images. Increased tracer activity in the superior mediastinum after 6 h. No tracer accumulation in the pericardial space.
A conservative management approach with pericardiostomy followed by a medium-chain triglyceride diet was initiated. He was initially responsive, with decreasing pericardial drain output (100–200 ml during the first three days then less than 50–100 ml during the succeeding days), hence he was discharged on the 9th hospital day. Three months after discharge, there was new-onset dyspnea on exertion. A repeat TTE revealed a recurrence of the large pericardial effusion. The patient was readmitted and a repeat pericardiostomy was done draining 1200 ml of chylous pericardial effusion. Pericardiectomy with possible thoracic duct ligation was advised; however, the patient did not consent. Adenosine deaminase (ADA) testing of the fluid was done and was elevated (100 U/L). First-line anti-TB therapy consisting of fixed-dose combination tablets of isoniazid/rifampicin/pyrazinamide/ethambutol (75 mg/150 mg/400 mg/275 mg) was initiated at four tablets per day and given for 2 months then isoniazid/rifampicin (75 mg/150 mg) one fixed-dose combination tablet per day for the succeeding 4 months. Surveillance TTE was done at the 3rd and 6th month of treatment and after 1 year. There was no recurrence of the fluid or signs of development of pericardial constriction.
Discussion
Chylous pericardial effusion is a rare condition consisting of excess chyle in the pericardial fluid.1–3 Tuberculosis is a major cause of pericardial effusion in developing countries such as the Philippines but TB as an etiology of chylopericardium is rarely reported.3,5,6 A high incidence of an idiopathic etiology might be in part due to an underdiagnosis of TB, leading to publication and reporting bias. 3
The mechanism by which chyle accumulates is believed to be secondary to damaged lymphatics, elevated pressure (e.g., obstruction), or abnormal communication within the thoracic duct, lymphatic vessels, and/or venous system. 2 Specifically, TB causes pericardial effusion via an immune response to viable bacilli that spread to the pericardium. 7 The pathogenesis of TB causing chyle accumulation is largely unknown.
Most patients are asymptomatic at presentation (40–60%) and discovered as an incidental finding on routine chest radiograph. 1 Conservative therapy is the initial approach and consists of pericardiocentesis, tube pericardiostomy, and a medium-chain triglyceride diet.2,3 Failure to respond should prompt surgical intervention in the form of thoracic duct ligation and/or pericardiectomy. 2 Nevertheless, cardiac tamponade and pericarditis may result when therapy is not instituted early. 3
In the absence of a definitive etiology, management was conservative as per guideline recommendations. Tuberculosis culture, polymerase chain reaction, and biopsy have a diagnostic sensitivity of 53%, 81%, and 10–64%, respectively. 7 Hence, negative findings do not exclude the diagnosis. Pericardial fluid ADA has a sensitivity and specificity approaching 100% in the setting of lymphocyte-predominant pericardial effusion in a patient in an endemic area. Thus, it may be helpful as part of the initial workup not only in chylous pericardial effusion but in patients with pericardial effusion in general. With a high cure rate for tuberculous pericardial effusion, anti-TB therapy was instituted, and the outcome was favorable. 8
Conclusion
Tuberculosis as a cause of chylopericardium, although rarely reported, should always be entertained particularly in endemic areas. Diagnosis of a treatable underlying condition may alter management, potentially avoiding unnecessary risks and complications. While data are lacking, this case suggests that TB chylopericardium is highly responsive to anti-TB therapy.
Footnotes
Acknowledgements
The authors would like to acknowledge James Delas Alas MD, Regina Berba MD, and Danielle Louis Villanueva MD for their significant contribution in the management of this case. The authors would also like to acknowledge Frances Ho MD for her assistance in the review and editing of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent statements
Written informed consent for publication was provided by the patient. This case report was conducted in accordance with the principles of the Philippine National Ethical Guidelines for Health Research and the Philippine Data Privacy Act of 2012 (RA 10173). As case reports and case series involve a small number of human participants, but are not considered research subjects, this study was deemed exempt from institutional board review.