
Abstract
Background
The Fontan operation is the definitive palliation for single-ventricle physiology. In low- and middle-income countries, delayed diagnosis and limited paediatric cardiac services often result in adults presenting for primary Fontan rather than staged completion.
Methods
Adults (≥18 years) undergoing extracardiac or lateral-tunnel Fontan between January 2021 and June 2025 were retrospectively reviewed. Variables included demographics, conduit and fenestration, cardiopulmonary bypass and cross-clamp times, re-exploration, extubation time, intensive care unit (ICU) stay, pulmonary-artery pressure, atrioventricular valve regurgitation, pleural effusion >14 days, arrhythmia and survival.
Results
Twenty-four adults (median age 20.5 years (interquartile range 19–22); 17 males (71%)) underwent primary Fontan: 18 (75%) extracardiac and 6 (25%) lateral tunnel. Fenestration was created in 14 (58%). Mean pulmonary-artery pressure increased from 12.6 ± 3.2 to 13.7 ± 3.5 mmHg (p = .12). Systemic oxygen saturation improved significantly from 79 ± 4% to 92.8 ± 3.1% (p < .001). Atrioventricular-valve regurgitation decreased significantly (p = .03), and New York Heart Association (NYHA) I–II class increased from 25% to 88% (p < .001). Pleural effusion >14 days occurred in nine (38%) and arrhythmia in three (13%) patients. Kaplan–Meier survival was 100% at 2 years and 95.8% at 3 years (95% confidence interval [83–100]).
Conclusions
Primary Fontan beyond childhood can be performed safely in adults with favourable haemodynamics, achieving excellent early survival and functional improvement. Standardised technique and vigilant postoperative care are central to recovery in low- and middle-income country settings.
Keywords
Introduction
Since its initial description in 1971, the Fontan procedure has evolved into the preferred palliation for patients with functionally single ventricle. 1 Since its original description, the Fontan operation has undergone several modifications aimed at improving haemodynamics and reducing atrial complications, including the atriopulmonary connection, lateral tunnel Fontan, extracardiac conduit Fontan and more recently intra-extracardiac modifications, with or without fenestration.2,3
The success of Fontan physiology depends on low pulmonary vascular resistance (PVR), competent atrioventricular (AV) valves and preserved ventricular function. 4 While ideal Fontan completion occurs in early childhood (2–5 years), 5 many patients in low- and middle-income countries (LMICs) present late due to delayed diagnosis or lack of staged palliation.6,7 In such settings, individuals may be considered for primary Fontan operation in adolescent or adult stage.
Adults carry an additional risk of chronic cyanosis and volume overload leading to ventricular dysfunction and endocardial fibrosis, which reduce diastolic compliance and impair preload adaptation. Over time, myocardial fibrosis and hypertrophy impair the ability of the ventricle to fill effectively.8,9 Concurrently, progressive AV valve regurgitation, atrial dilation and elevated central venous pressures further pose a challenge for Fontan physiology.
Despite these challenges, several adult Fontan series report acceptable early survival albeit the higher morbidity.10,11 However, most published series either involve Fontan conversion or staged completion rather than de novo primary Fontan in adults. The aim of this study is to present our institutional experience with adult primary Fontan operations—analysing haemodynamics, conduit selection, surgical details, complications and short-term survival in an LMIC environment.
Materials and methods
Study design and setting
We conducted a retrospective observational review at the Department of Cardiothoracic and Vascular Surgery, PGIMER, Chandigarh, spanning January 2021 to June 2025. Institutional ethics approval was obtained prior to data collection.
Inclusion and exclusion criteria
Inclusion: adult patients (≥18 years) with single-ventricle physiology undergoing primary Fontan operation (extracardiac or lateral tunnel). Exclusion: Fontan completion or conversion, incomplete records, age <18 years.
Patient selection
During the study period, adult patients with single-ventricle physiology were evaluated for operability; only those meeting eligibility criteria underwent primary Fontan. All Patients included in this study were selected for primary Fontan based on late presentation without prior palliation; staged palliation was not considered feasible or appropriate in this adult cohort.
Preoperative evaluation and eligibility criteria for adult primary Fontan
All patients underwent systematic preoperative assessment including echocardiography and cardiac catheterisation to determine operability. Adult candidates were selected using stricter criteria than those applied in childhood due to the physiological effects of long-standing cyanosis and volume overload. Eligibility for primary Fontan in adulthood required preserved ventricular systolic function (normal or mildly reduced), absence of significant AV valve regurgitation, acceptable pulmonary artery pressures and favourable pulmonary artery anatomy (including adequate branch pulmonary artery size), and absence of advanced end-organ dysfunction. Patients were excluded if they had markedly reduced ventricular function, severe AV valve regurgitation not amenable to repair, or clinical/end-organ features suggesting advanced Fontan intolerance. Surgical candidacy was determined through an integrated assessment of haemodynamics, ventricular function, pulmonary artery anatomy and hepatic/renal profile. Fenestration was selectively created in patients with borderline haemodynamics, higher pulmonary artery pressures, mildly reduced ventricular function, or concern for postoperative venous hypertension based on the overall preoperative assessment.
Data collection
Data extracted included demographic variables (age, sex, body surface area), diagnosis, surgical details (approach, conduit or patch type and size, fenestration, cardiopulmonary bypass (CPB) and aortic cross-clamp times, re-exploration, extubation time, intensive care unit (ICU) stay), haemodynamics (pre- and post-operative mean pulmonary artery pressure, oxygen saturation), ventricular function and AV valve regurgitation grades, New York Heart Association (NYHA) class, complications (pleural effusion >14 days, arrhythmia, ascites), and survival.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD) or median (interquartile range (IQR)), and categorical variables as frequencies and percentages. Comparisons between pre- and post-operative continuous variables were performed using the paired t-test or Wilcoxon signed-rank test, as appropriate. Categorical variables were compared using the chi-square or Fisher's exact test. Survival was analysed using the Kaplan–Meier method with 95% confidence intervals (CIs). A p < .05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics Version 26.0 (IBM Corp., Armonk, NY, USA).
Results
Patient demographics and diagnoses
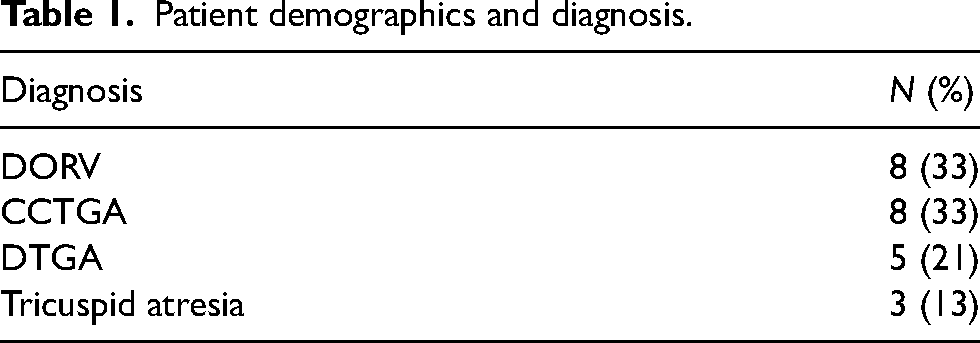
Twenty-four adults (median age of 20.5 years (IQR 19–22); 17 male (71%)) underwent a primary Fontan operation. All patients had anatomy and physiology compatible with single-ventricle palliation, including associated pulmonary outflow obstruction. Diagnoses included double-outlet right ventricle in eight (33%), congenitally corrected transposition of the great arteries in eight (33%), dextro-transposition of the great arteries in five (21%) and tricuspid atresia in three (13%) (Table 1).
Patient demographics and diagnosis.
Preoperative pulmonary artery anatomy and baseline organ function
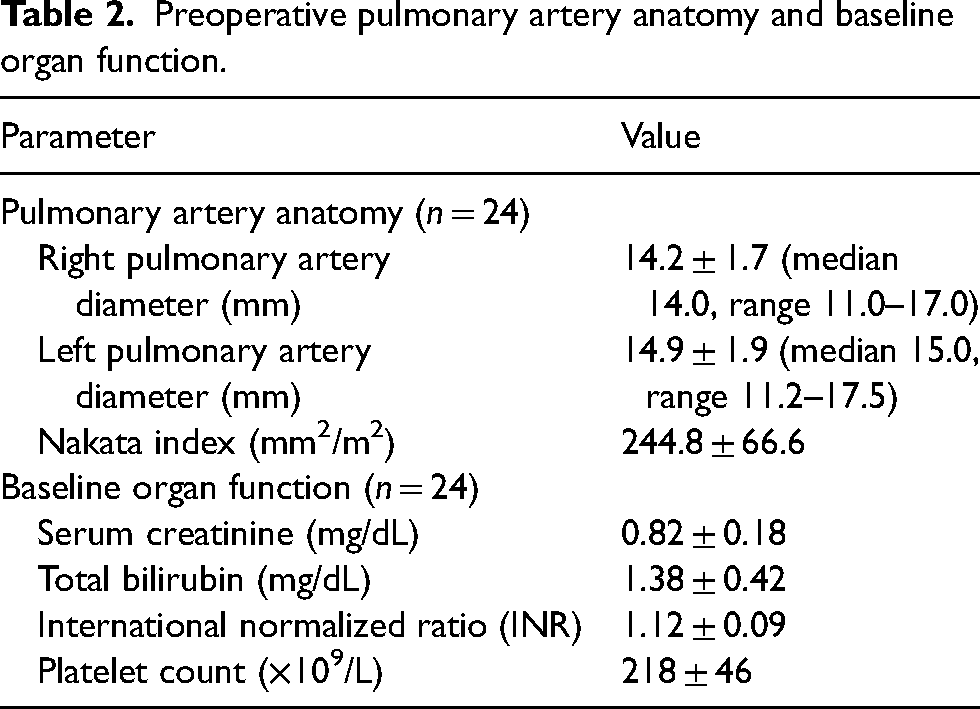
Preoperative branch pulmonary artery diameters and baseline hepatic and renal parameters are summarised in Table 2. Mean right pulmonary artery and left pulmonary artery diameters were adequate, with a mean Nakata index consistent with Fontan operability.
Preoperative pulmonary artery anatomy and baseline organ function.
Surgical details
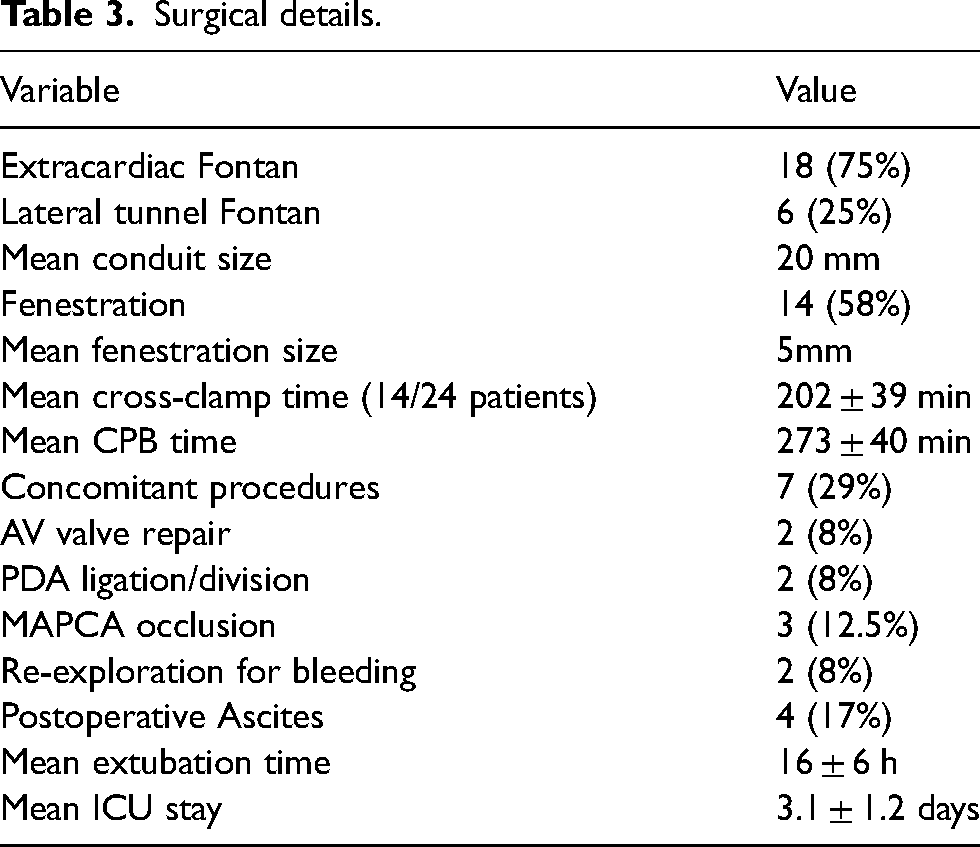
All patients underwent standard median sternotomy and CPB via aorto-bicaval cannulation under general anaesthesia. Eighteen patients (75%) had an extracardiac Fontan with polytetrafluoroethylene (PTFE) tube grafts, and six (25%) had a lateral-tunnel modification using PTFE patches. Fenestration was performed in 14 (58%) patients (mean diameter of 5 mm). Aortic was cross-clamped in 14 (58%) patients, all of whom received Del Nido cardioplegia. Mean CPB time was 273 ± 40 min and mean cross-clamp time was 202 ± 39 min. Concomitant procedures were performed in seven patients (29%), including AV valve repair in two patients (8%), patent ductus arteriosus ligation/division in two patients (8%) and occlusion of major aortopulmonary collateral arteries in three patients (12.5%). A pericardial drain and two pleural drains were placed in all patients. Two patients (8%) required re-exploration for bleeding. Mean extubation time was 16 ± 6 h, and mean ICU stay was 3.1 ± 1.2 days. Four patients (17%) developed transient ascites post-operatively (Table 3).
Surgical details.
Haemodynamics, valve function and functional status
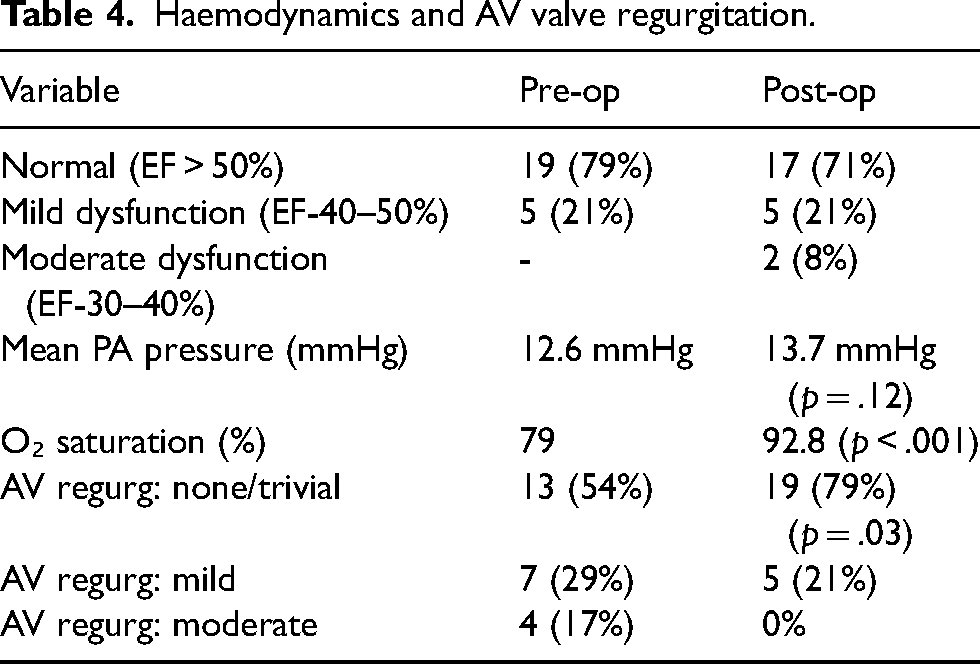
Mean pre-operative pulmonary-artery pressure was 12.6 ± 3.2 mmHg, rising to 13.7 ± 3.5 mmHg post-operatively (p = .12). Systemic oxygen saturation improved significantly from 79 ± 4% pre-operatively to 92.8 ± 3.1% post-operatively (p < .001). AV-valve regurgitation before surgery was none/trivial in 13 (54%), mild in 7 (29%) and moderate in 4 (17%). At post-operative follow-up, none/trivial AV-valve regurgitation was present in 19 (79%), mild in 5 (21%) and moderate in 0 (0%) (p = .03). None of the patients required any repair after primary surgery for AV regurgitation. Pre-operatively, 18 (75%) patients were NYHA Class III–IV; post-operatively 21 (88%) improved to Class I–II with 14 patients (58%) in class I (p < .001) (Table 4).
Haemodynamics and AV valve regurgitation.
Complications and survival
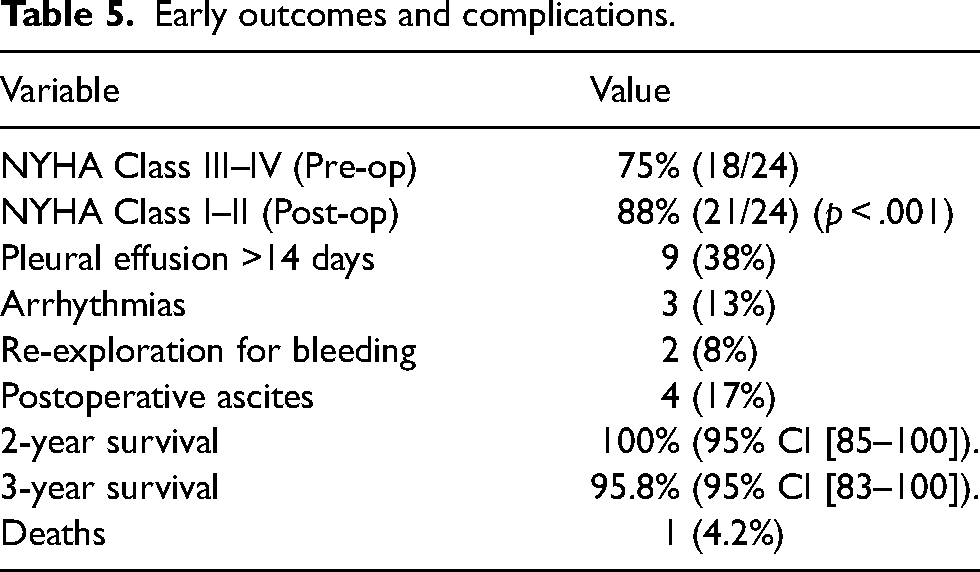
Arrhythmias (atrial fibrillation and junctional ectopic tachycardia) occurred in three (13%) and pleural effusion persisting beyond 14 days occurred in nine patients (38%). Overall morbidity included prolonged pleural effusion, transient ascites and minor rhythm disturbances, which were managed pharmacologically, with no early mortality. At a median follow-up of 18 months (IQR 12–28), Kaplan–Meier survival was 100% at 2 years and 95.8% at 3 years (95% CI [83–100]) (Figure 1). One late death (4.2%) occurred 907 days after surgery due to Fontan failure. The longest individual follow-up was 3.9 years (Table 5).
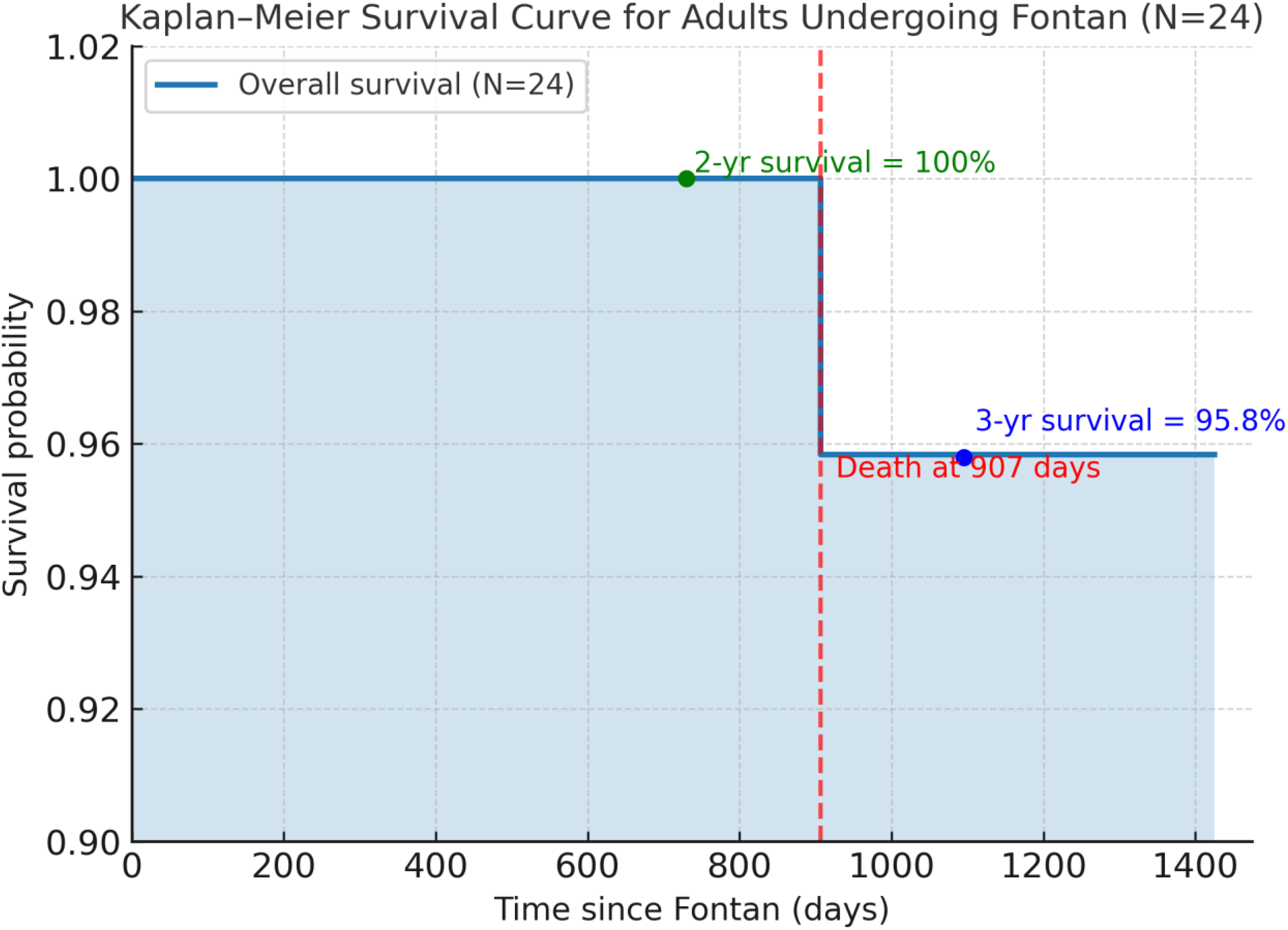
Kaplan–Meier survival curve showing overall survival for adults undergoing primary Fontan completion (N = 24). Two-year survival was 100% (95% CI [85–100]). At 3 years, survival was 95.8% (95% CI [83–100]), with one death at 907 days due to Fontan failure. The longest individual follow-up was 3.9 years and the longest-followed patient was alive at last contact.
Early outcomes and complications.
Discussion
The present series demonstrates that primary Fontan operation in adults can be safely performed in carefully selected adult patients, achieving excellent early survival and meaningful functional improvement. Despite the haemodynamic and structural challenges inherent to delayed presentation, outcomes were favourable, with survival rates of 100% at 2 years and 95.8% at 3 years, accompanied by significant gains in oxygenation and physical capacity. In contrast to completion Fontan performed after staged palliation, this cohort included adults undergoing the Fontan operation de novo. These patients presented with the cumulative consequences of long-standing cyanosis and volume overload, leading to ventricular hypertrophy, diastolic stiffness and endocardial fibrosis that compromise preload accommodation and elevate PVR.7,8 For this reason, adult candidates in this series were selected using stricter operability criteria than those typically applied in younger children. Such physiological alterations make adult Fontan surgery inherently demanding, yet meticulous selection, uniform operative technique, and standardized postoperative care resulted in stable recovery and favourable early outcomes.
A consistent operative strategy was adopted for all cases. Eighteen patients (75%) underwent the extracardiac Fontan with PTFE conduits, whereas six (25%) underwent the lateral tunnel modification. Both configurations provided satisfactory early haemodynamics and survival; however, the extracardiac approach showed a trend toward smoother postoperative recovery, with fewer arrhythmias in 2 of 18 patients (11%) and a shorter duration of pleural effusion compared with 1 of 6 patients (17%) in the lateral tunnel group. Although pleural effusion appeared less frequent in the extracardiac group, this observation must be interpreted cautiously, as fenestration status differed between patients and is a known determinant of postoperative effusions. Although not statistically significant due to small sample size, these findings are consistent with broader experience indicating that the extracardiac conduit reduces atrial manipulation, preserves sinus node function and lowers arrhythmia incidence.10–12 In adult candidates, this configuration also facilitates easier re-entry for potential future procedures and minimizes atrial suturing in dilated chambers, making it the preferred technique in most contemporary centres.5–11 The lateral tunnel approach was selected in a minority of patients based on anatomical considerations, including atrial morphology and pulmonary artery configuration. In adults, CPB was used to allow precise intracardiac reconstruction and to safely address concomitant procedures where required.
Fenestration was created in 14 patients (58%) to allow decompression of the Fontan circuit in borderline haemodynamics. This strategy appeared beneficial, with early recovery characterized by a mean extubation time of 16 ± 6 h and an average ICU stay of 3.1 ± 1.2 days, values comparable with international adult Fontan benchmarks.10,11 Two patients (8%) required re-exploration for bleeding, and four (17%) developed transient ascites, most likely due to temporary hepatic congestion resulting from elevated systemic venous pressure. Pleural effusion persisting beyond 14 days occurred in nine patients (38%), similar to the 30–40% incidence reported in other adult Fontan series, reflecting the tendency of this population toward postoperative lymphatic and serous effusions.9–10 Overall morbidity therefore remained within an acceptable range, and most complications were managed conservatively without affecting early survival.
AV valve competence was an important determinant of postoperative stability, showing a statistically significant improvement (p = .03). Moderate regurgitation, present in 4 patients (17%) pre-operatively, was eliminated at follow-up, with 19 patients (79%) demonstrating no or trivial regurgitation. AV valve repair was required only in patients with structural regurgitation, while functional regurgitation improved following Fontan physiology in the remaining cases. Timely intra-operative valve repair likely contributed to this favourable result and reinforces the established recommendation that addressing AV valve dysfunction at the time of Fontan surgery enhances long-term ventricular function and circuit durability. 13 Haemodynamically, a modest increase in mean pulmonary artery pressure from 12.6 to 13.7 mmHg was observed postoperatively. This finding, widely recognised in adult Fontan literature, reflects the influence of ventricular stiffness and endocardial fibrosis rather than procedural inadequacy.8,9 Despite this, systemic oxygen saturation improved significantly from 79% to approximately 92% (p < .001), confirming efficient cavopulmonary flow and successful elimination of right-to-left shunting. Functionally, improvement was statistically significant and clinically substantial—NYHA Class I–II increased from 6 patients (25%) pre-operatively to 21 (88%) post-operatively (p < .001), mirroring outcomes from larger international series where most survivors remain in Class I–II after surgery.11–14
The relatively longer CPB and aortic cross-clamp times observed in this series reflect the complexity of primary Fontan surgery performed as the first cardiac operation in adulthood. Adult primary Fontan requires extensive dissection, intracardiac assessment, and concomitant procedures in dilated and hypertrophied hearts. Similar CPB durations have been reported in adult primary Fontan series, particularly when AV valve repair or fenestration is required. 5
When compared with global benchmarks, the 3-year survival rate of 95.8% observed in this cohort aligns closely with reported 5-year survival of 92–95% and 10-year survival of 80–90% from large multicentre registries.10–12,15 The incidence of early morbidity, including re-exploration, arrhythmia and pleural effusion were also comparable to published adult Fontan data. 10 These parallels indicate that satisfactory results can be achieved even when surgery is performed beyond the typical paediatric window, provided that ventricular function and PVR remain acceptable. Chronological age alone should therefore not be regarded as a contraindication to Fontan palliation.11–14
Fontan circulation, however, carries an inherent risk of progressive systemic venous hypertension and end-organ effects. Over time, patients may develop hepatic fibrosis, protein-losing enteropathy, arrhythmia, or ventricular dysfunction, conditions that can compromise late survival and quality of life.6,8,15 Continuous multidisciplinary follow-up remains essential, incorporating echocardiography, hepatic elastography, rhythm assessment and exercise testing to detect early manifestations of Fontan-associated disease. Establishing regional and multicentre registries across South Asia would facilitate pooled data analysis and help define the long-term trajectory of adult primary Fontan outcomes, especially in LMIC contexts where delayed presentation is common.14,15
The strengths of this study include a uniform operative technique, comprehensive peri-operative documentation and the exclusive inclusion of de novo primary Fontan cases, excluding conversions and revisions to accurately reflect early outcomes in adult palliation. Limitations include its retrospective nature, modest sample size and relatively short follow-up duration, which preclude definitive statistical comparisons between subgroups. This study represents a carefully selected cohort of adult patients deemed suitable for primary Fontan surgery, and the results may not be generalisable to all adults with single-ventricle physiology, particularly those with advanced ventricular dysfunction, elevated PVR, or significant end-organ involvement. Nevertheless, the consistency of the findings and alignment with international data emphasise that primary Fontan beyond childhood can be performed safely with meaningful improvement in survival and quality of life, even in resource-limited environments. 15 Continued longitudinal surveillance is warranted to evaluate late organ sequelae and Fontan circuit performance as this cohort matures.
Conclusion
Primary Fontan operation beyond childhood can be performed safely in carefully selected adult patients, even in low- and middle-income country settings. When stringent preoperative evaluation, appropriate patient selection and standardized surgical techniques are applied, early survival and functional outcomes are excellent. These findings support primary Fontan as a viable definitive palliation for selected adults presenting late with single-ventricle physiology.
Footnotes
Acknowledgements
The authors gratefully acknowledge Department of Cardiothoracic and Vascular Surgery and Department of Cardiology for their support in patient management and data collection.
Authors’ contribution
Anand Kumar Mishra, Manojkumar K Rohit and Harkant Singh: conceptualization and supervision; Sanketh Edem: methodology and writing–original draft preparation; Sanketh Edem, Lasya Reddy, Vivek Jaswal and Tsering Sangdup: writing–review and editing; Sanketh Edem and Akshay Kheni: visualization; Sanketh Edem and Akshay Kheni: resources and software.
Data availability
Data available on request from the authors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Approval was taken from Institutional Ethics Committee (IEC-INT/2025/Study-2954).
Informed consent
Written informed consent was taken from the patients for participation and publication.