
Abstract
Background
Arterial cannulation during cardiopulmonary bypass (CPB) significantly alters native aortic hemodynamics by generating a high-velocity jet that interacts with the ascending aorta and aortic arch geometry. These flow disturbances may influence wall shear stress (WSS), turbulence intensity, embolic trajectories, and cerebral perfusion. Cannula depth, orientation, and tip design have emerged as potentially important determinants of intra-aortic flow behavior.
Materials and methods
A structured narrative review of the literature was conducted. PubMed/MEDLINE, Scopus, and Web of Science were searched from January 1990 to April 2025. Keywords included combinations of “aortic cannulation,” “cardiopulmonary bypass,” “computational fluid dynamics,” “wall shear stress,” “turbulence,” “atherosclerotic plaque,” “cerebral perfusion,” “microembolization,” “gaseous emboli,” “NIRS,” and “transcranial Doppler.” Studies were included if they evaluated hemodynamic effects of cannulation strategies using computational, in vitro, or clinical models. Articles not directly related to CPB intra-aortic flow dynamics were excluded.
Results
The available evidence suggests that cannula positioning significantly influences intra-aortic flow behavior. Centrally aligned cannulation directed toward the descending thoracic aorta promotes axial flow and is associated with reduced jet-wall impingement and lower peak WSS. This configuration decreases arch turbulence and limits embolic transport toward supra-aortic vessels.
Conclusion
Arterial cannulation strategy during CPB is a modifiable determinant of flow behavior and potential cerebral embolic exposure. Hemodynamically informed cannulation principles may contribute to intraoperative neuroprotection, although prospective clinical validation is still required.
Keywords
Introduction
Cardiopulmonary bypass (CPB) alters physiological aortic hemodynamics by replacing pulsatile native cardiac output with continuous extracorporeal flow. The arterial inflow cannula introduces a high-velocity jet into the ascending aorta, disrupting organized helical flow structures and modifying pressure gradients, wall shear stress (WSS), turbulence intensity, and embolic transport patterns. Rather than representing a simple technical step, arterial cannulation should be considered an active hemodynamic intervention capable of influencing cerebral perfusion and embolic risk. Computational investigations have demonstrated that cannula depth significantly affects the intra-aortic transport of gaseous emboli. In a computational fluid dynamics (CFD) study, Ho et al. showed that more proximal cannula positioning increases recirculation zones and promotes embolic diversion toward supra-aortic branches, whereas deeper insertion modifies jet interaction with the aortic wall and reduces cerebral embolic transport. 1 In a related analysis, the same group demonstrated that cannula orientation is a critical determinant of embolic trajectories: cranially directed jets increase embolic delivery to carotid vessels, while descending-oriented flow reduces embolic burden to the brain. 2 Recently, patient-specific CFD modeling of carotid perfusion during CPB has confirmed that cannulation strategy significantly alters supra-aortic flow fractions depending on vascular anatomy, arch geometry, and jet direction. 3 Numerical modeling in type A aortic dissection further demonstrated that alternative cannulation approaches produce distinct flow patterns and shear stress distributions within the true and false lumens, reinforcing the importance of inflow configuration. 4 Experimental work in pediatric models has similarly shown that cannula tip orientation affects cerebral perfusion symmetry and magnitude, highlighting the sensitivity of carotid flow distribution to jet geometry. 5 Beyond cannula position, device design may also influence perfusion patterns. Experimental and translational investigations have reported that optimized cannula tip geometry can improve flow uniformity, reduce focal WSS peaks, and promote more stable cerebral perfusion during CPB.5–7 In addition, the selected inflow site may affect arch hemodynamics, since retrograde femoral perfusion can generate less favorable flow interactions in patients with extensive aortic atherosclerosis, whereas central cannulation provides antegrade systemic flow. 8 Although the available evidence derives from heterogeneous computational, experimental, and clinical models, a consistent physiological rationale emerges: arterial inflow configuration influences flow organization within the aorta and may contribute to embolic exposure and cerebral perfusion asymmetry. On this basis, the present review summarizes current evidence on cannula position, orientation, insertion depth, tip design, and inflow site during CPB, with the aim of identifying clinically relevant hemodynamic principles for intraoperative neuroprotection.
Materials and methods
This study was designed as a structured narrative review aimed at synthesizing current evidence regarding arterial cannulation strategies during CPB, with specific focus on intra-aortic hemodynamics, WSS, turbulence generation, atherosclerotic plaque destabilization, embolic transport, and cerebral perfusion monitoring. Given the methodological heterogeneity of the available literature, a qualitative integrative approach was adopted to critically evaluate mechanistic coherence and translational implications. A comprehensive literature search was performed using PubMed/MEDLINE, Scopus, and Web of Science. The search covered the period from January 1990 through April 2025. Both controlled vocabulary terms (MeSH where applicable) and free-text keywords were used. The search strategy combined the following conceptual domains: (1) arterial or aortic cannulation; (2) CPB; (3) CFD, WSS, or turbulence; (4) cerebral perfusion, embolism, microembolization, or gaseous emboli; and (5) monitoring modalities such as near-infrared spectroscopy (NIRS) and transcranial Doppler (TCD). Boolean operators (AND/OR) were used to construct structured search strings. An example of a representative search string was: (“aortic cannulation” OR “arterial cannulation”) AND (“cardiopulmonary bypass”) AND (“computational fluid dynamics” OR “wall shear stress” OR “turbulence”) AND (“cerebral perfusion” OR “microembolization” OR “embolism” OR “gaseous emboli”). The study selection process was conducted in three sequential phases. First, titles and abstracts were screened to identify studies relevant to intra-aortic flow dynamics during CPB. Articles clearly unrelated to arterial inflow hemodynamics were excluded at this stage. Second, full-text versions of potentially eligible studies were reviewed to assess methodological rigor, relevance to the hemodynamic endpoints of interest, and contribution to mechanistic understanding. Third, final inclusion was based on predefined criteria emphasizing direct evaluation of cannulation-related flow patterns, WSS distribution, turbulence characteristics, embolic transport modeling, or cerebral perfusion outcomes. Reference lists of included articles were manually screened (snowballing technique) to identify additional relevant publications not captured by the initial database search. Inclusion criteria comprised peer-reviewed original research articles that met at least one of the following conditions: CFD modeling of arterial cannulation during CPB; experimental in vitro or in vivo studies evaluating cannula geometry, jet dispersion, or WSS; clinical observational studies assessing cerebral perfusion, embolization, or neurological outcomes associated with cannulation strategy; or foundational mechanistic studies on WSS and plaque biomechanics directly applicable to CPB-related hemodynamic perturbations. Exclusion criteria included case reports, non-English publications, editorials without original data, and studies focused exclusively on extracorporeal membrane oxygenation without relevance to ascending aortic inflow dynamics during CPB. For each included study, data were extracted regarding study design (CFD, in vitro, in vivo, clinical), cannulation site and orientation, cannula depth and tip characteristics, hemodynamic parameters (WSS magnitude, turbulence intensity, recirculation zones, flow symmetry), embolic transport outcomes, and cerebral monitoring findings where applicable. Data synthesis was qualitative and focused on identifying consistent mechanistic patterns across computational, experimental, and clinical evidence.
The structured literature search identified 312 records. After duplicate removal (n = 78), 234 abstracts were screened, and 61 full-text articles were assessed. Twenty studies met inclusion criteria and were included in the final synthesis (references 1–20). These comprised 11 CFD studies,1–4,9–14 four experimental or translational investigations,5–7,15 three clinical observational studies incorporating cerebral monitoring,16–18 and two integrative state-of-the-art analyses.8,19,20 Despite heterogeneity in modeling assumptions and clinical designs, strong mechanistic convergence was observed across five principal domains. The PRISMA flow diagram is shown in Figure 1.
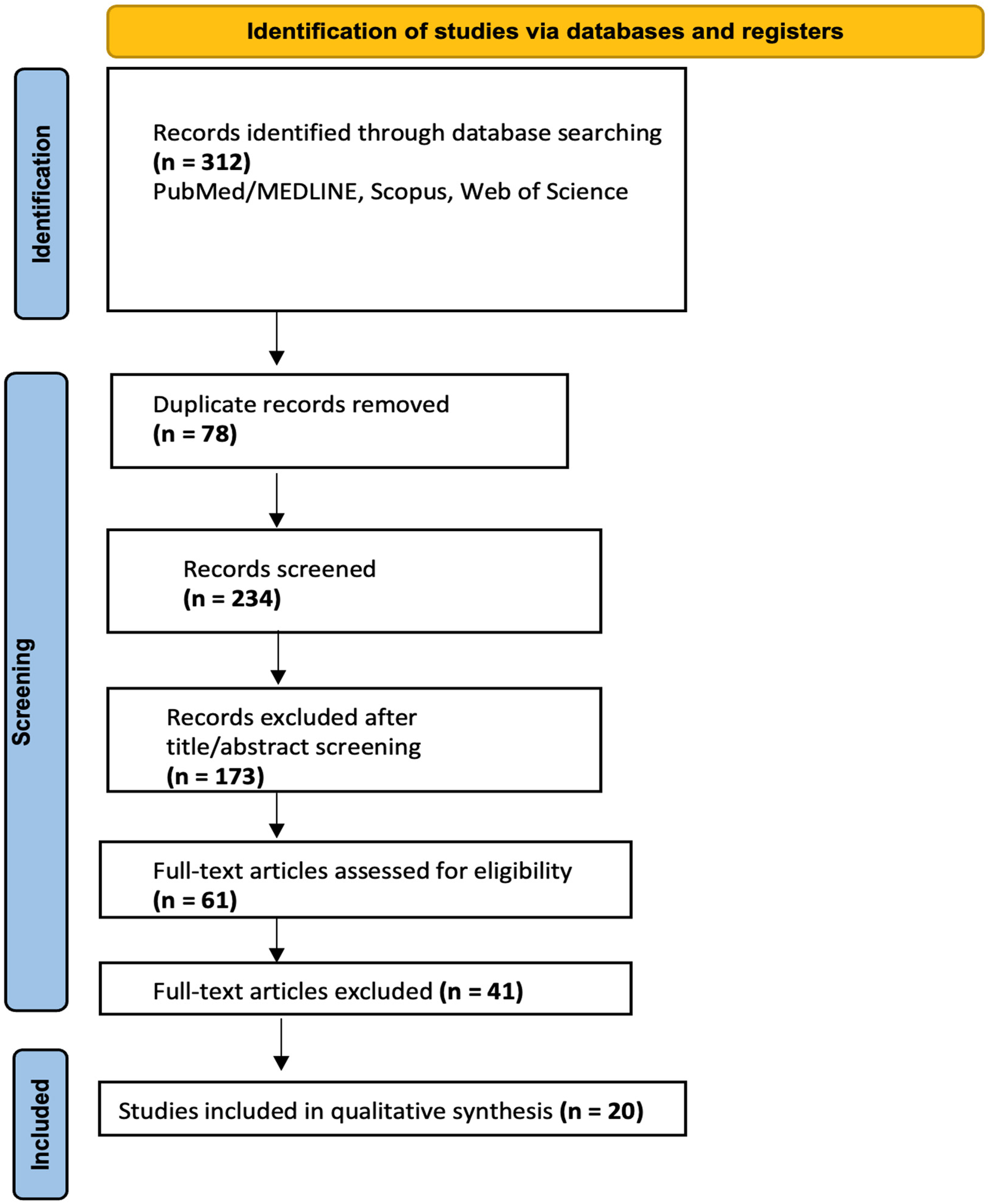
PRISMA flow diagram.
Results
Jet orientation and insertion depth: Determinants of intra-aortic flow architecture
Across CFD investigations,1–4,9–11,13,14 cannula orientation consistently emerged as the dominant determinant of intra-aortic flow behavior during CPB. Cranially directed or eccentrically positioned jets produced focal impingement against the anterior ascending aortic wall, generating high local velocity gradients and promoting boundary layer separation. These effects resulted in the formation of secondary vortical structures within the curvature of the aortic arch. 11 Ho et al. 2 demonstrated that cannula orientation significantly modifies embolic trajectories, with cranially oriented jets increasing embolic diversion toward supra-aortic branches. In a subsequent study, cannulation depth was shown to influence proximal recirculation zones and embolic transport dynamics (Figure 2). 1 Patient-specific CFD models further confirmed that vascular anatomy modulates but does not override the influence of jet direction on arch flow topology.3,13 Numerical simulations in aortic arch surgery settings similarly showed that inflow configuration alters regional flow distribution and shear stress patterns. 9 Earlier CFD analyses comparing ascending and subclavian inflow sites also demonstrated that inflow alignment determines supra-aortic flow fractions and turbulence generation. 14 In contrast, centrally aligned cannulation directed toward the descending thoracic aorta promoted axial flow propagation with reduced direct wall impingement. This configuration consistently attenuated proximal recirculation and limited secondary vortex formation within the arch 10 (Figure 2).
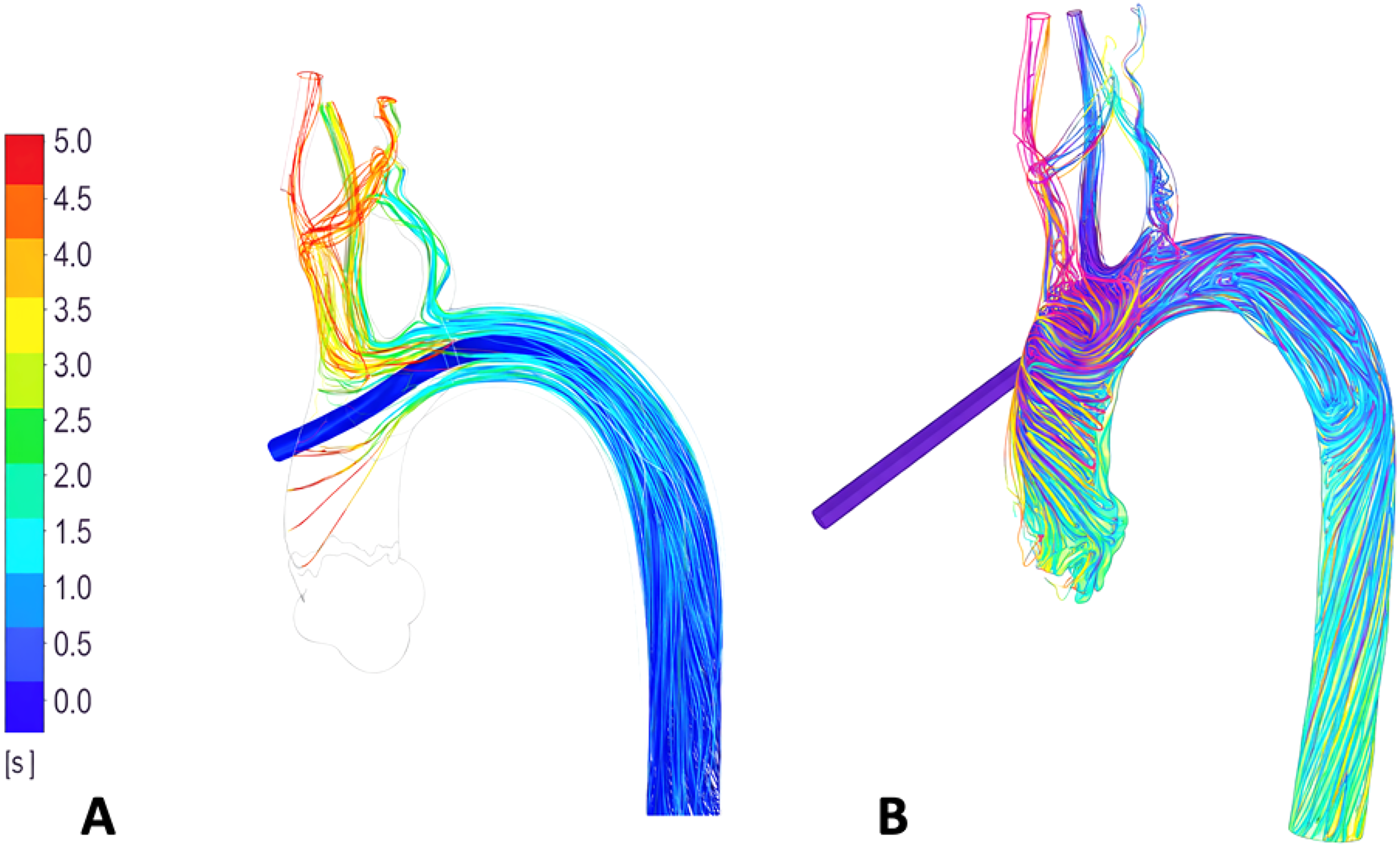
(A-B) Computational fluid dynamics (CFD) visualization of intra-aortic flow patterns under different cannula orientations during cardiopulmonary bypass. (A) Centrally aligned cannulation directed toward the descending thoracic aorta. Axial jet propagation is preserved with reduced wall impingement. Proximal recirculation zones are attenuated, secondary vortex formation is limited, and flow continuity toward the descending aorta is maintained. (B) Cranially directed/eccentrically oriented aortic cannulation. The inflow jet impinges on the anterior ascending aortic wall, generating focal regions of elevated velocity gradients and boundary layer separation. Secondary vortical structures develop within the curvature of the aortic arch, with increased flow diversion toward supra-aortic branches. Original schematic illustration created by the authors based on concepts reported in literary works.1,2,10
Wall shear stress distribution and plaque destabilization
Nine studies addressed WSS distribution under varying cannulation strategies.4,9–12,14,19,20 Peak WSS values were spatially correlated with jet-wall impingement sites. Cranially oriented jets generated localized shear magnitudes exceeding physiological pulsatile levels, particularly along the anterior ascending aorta and arch curvature. Experimental and computational studies have demonstrated that dispersive cannula designs reduce focal WSS peaks compared with conventional jet cannulas.12,15 Assmann et al. 12 showed that dispersive cannulas significantly decrease aortic WSS, potentially reducing the mechanical forces that contribute to plaque destabilization (Figure 3). These findings align with established biomechanical models of shear-mediated plaque vulnerability.19,20 Foundational CFD analyses of aortic arch flow confirm that curvature-induced secondary flows amplify shear stress heterogeneity when high-momentum jets are misaligned. 11 In aortic dissection modeling, altered inflow configuration also modified shear stress distribution across the aortic wall. 4 Autopsy data demonstrating iatrogenic embolization following cardiac intervention further support the clinical relevance of minimizing aortic wall stress during CPB. 18
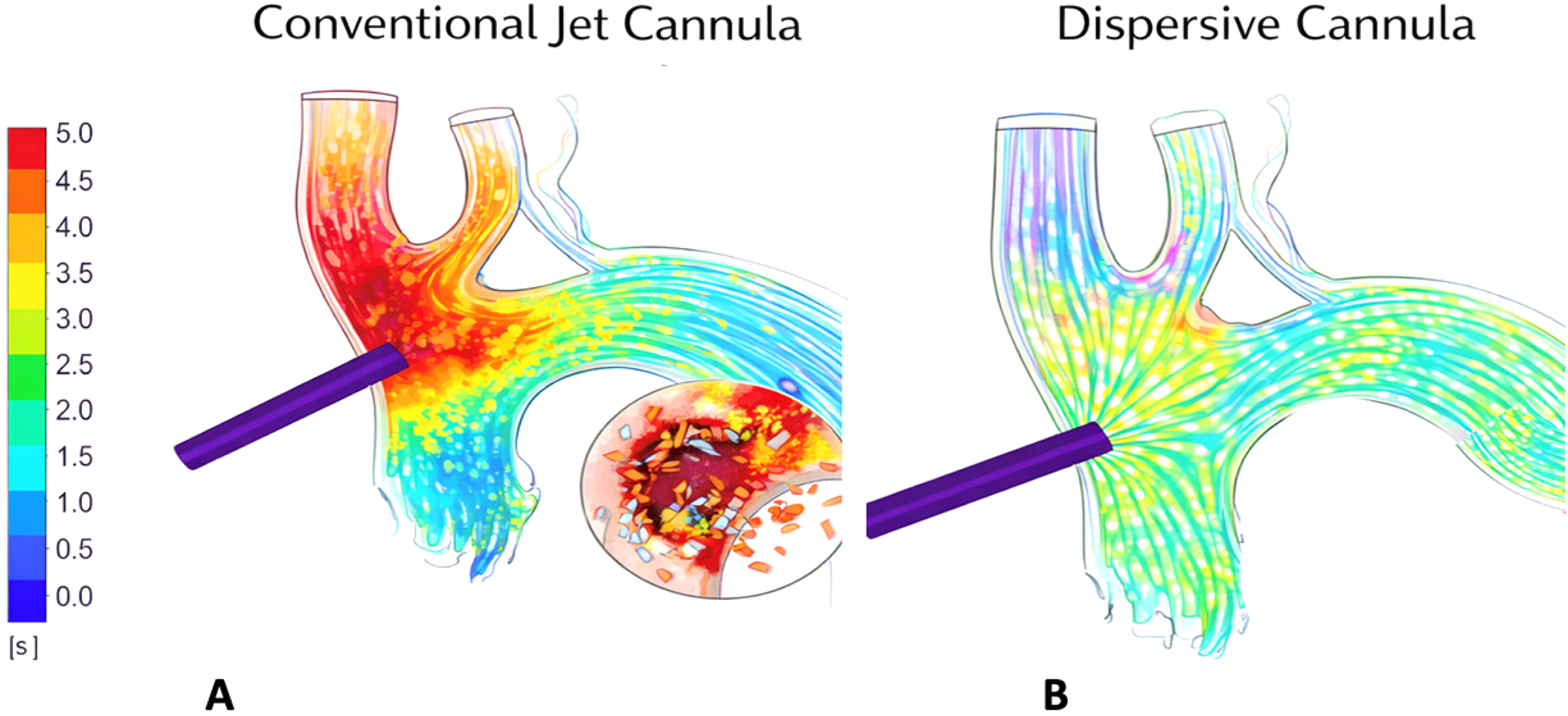
Comparative computational analysis of WSS distribution and plaque response under different arterial cannulation designs during cardiopulmonary bypass. (A) Conventional jet cannula. CFD visualization demonstrates focal high-magnitude wall shear stress localized at the site of jet-wall impingement along the anterior ascending aorta and proximal arch curvature. Elevated WSS and steep spatial gradients promote flow separation and secondary vortex formation. The inset illustrates mechanical disruption and fragmentation of an atherosclerotic plaque subjected to concentrated shear forces, consistent with shear-mediated plaque destabilization. (B) Dispersive cannula. Flow field analysis shows more homogeneous WSS distribution with reduced peak shear stress values and attenuated wall impingement. The dispersive jet pattern promotes smoother axial flow propagation and minimizes localized stress concentration. The inset depicts preserved plaque integrity under lower and more evenly distributed shear stress conditions. Color scale represents wall shear stress magnitude (Pa). Original schematic illustration created by the authors based on data from literary works.12,15 WSS: wall shear stress; CFD: computational fluid dynamics.
Embolic transport dynamics
Eight CFD studies modeled embolic transport during CPB.1,2,4,9,10,13,14 Ho et al.1,2 demonstrated that both cannula orientation and insertion depth significantly influence the distribution of simulated gaseous emboli. Cranially directed jets increased embolic entry into supra-aortic vessels, while descending-oriented jets reduced cerebral embolic fractions. Endoluminal perfusion modeling confirmed that jet direction and turbulence intensity directly affect embolic dispersion within the arch. 10 Patient-specific modeling in extracorporeal support settings similarly demonstrated that inflow geometry determines embolic trajectories toward cerebral vessels. 13 Numerical simulations applied to aortic arch surgery further showed that alternative cannulation configurations redistribute flow toward carotid arteries, altering embolic exposure. 9 Across studies, although absolute embolic percentages varied, the directional consistency was robust: centrally aligned descending orientation reduced simulated cerebral embolic burden (Figure 4).
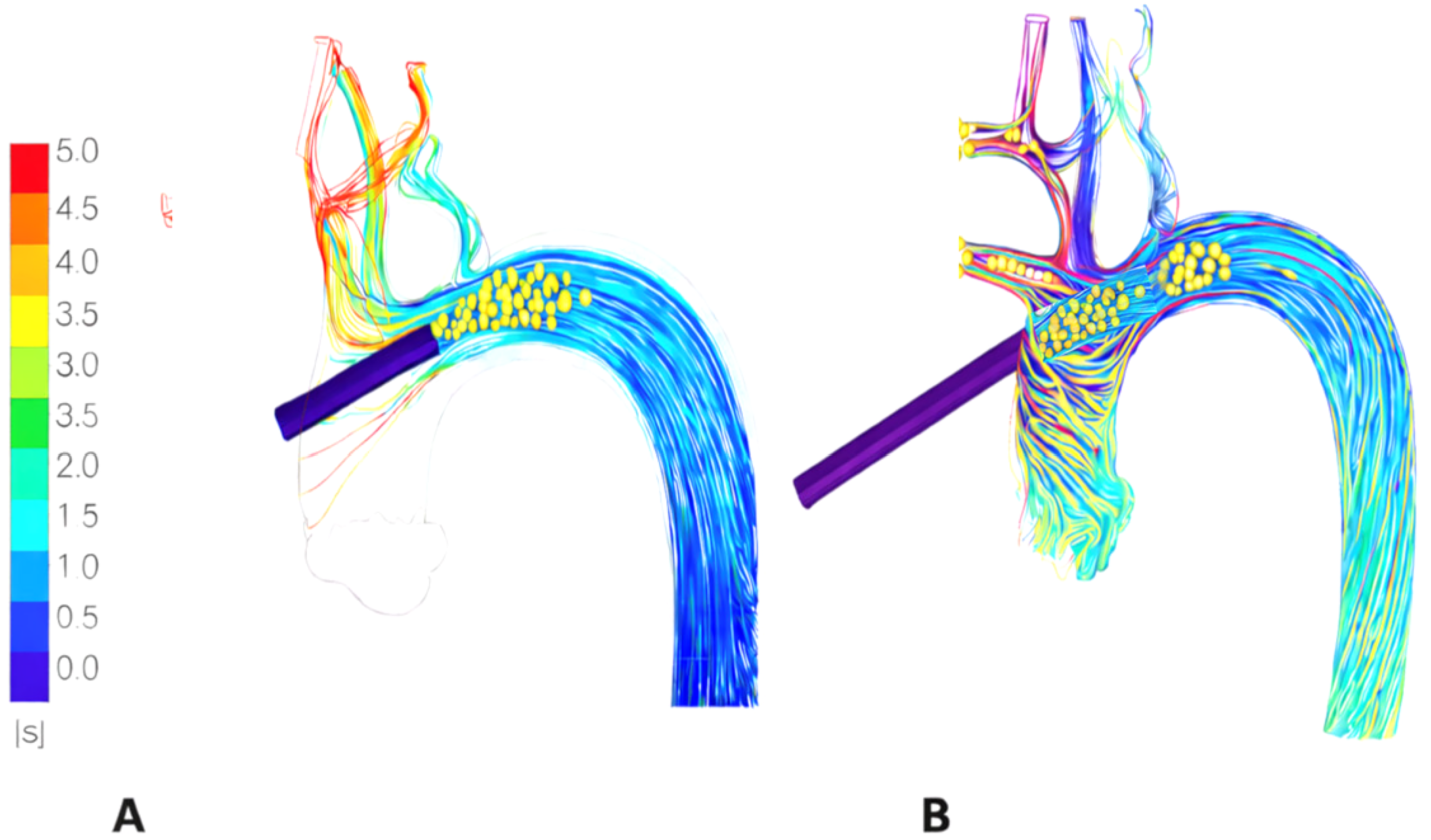
(A-B) Computational simulation of embolic transport dynamics under different arterial cannulation strategies during cardiopulmonary bypass. (A) Cannula centrally aligned and directed toward the descending thoracic aorta.Axial flow propagation is preserved with reduced proximal wall impingement and more organized downstream flow patterns. Simulated microemboli predominantly remain within the central lumen and are preferentially transported toward the descending aorta, with limited embolic entry into supra-aortic vessels. Color-coded streamlines represent instantaneous velocity magnitude. (B) Cannula positioned in the ascending aorta with cranially directed inflow. Computational fluid dynamics (CFD) streamlines demonstrate focal jet impingement against the anterior ascending aortic wall with subsequent redistribution of flow toward supra-aortic branches. Simulated microemboli (yellow spheres) are transported proximally within the aortic arch and preferentially diverted into the supra-aortic trunks, illustrating increased potential cerebral embolic exposure. Flow velocity magnitude is represented by the color scale (m/s). Original schematic illustration created by the authors based on concepts reported in literary works.1,2,9,13
Cerebral perfusion distribution and monitoring correlations
Cerebral perfusion implications were evaluated in CFD studies3,5,7,14 and correlated with clinical monitoring data.16,17 Lu et al. 3 demonstrated that cannulation strategy significantly affects carotid perfusion distribution, with anatomical variability influencing magnitude but not direction of effect. Hugenroth et al. 7 combined in silico, in vitro, and in vivo testing and reported improved cerebral perfusion stability with optimized cannula design. 6 Menon et al. 5 used a pediatric bypass model and demonstrated that cannula tip orientation significantly altered carotid flow symmetry. Clinically, TCD has been validated as a surrogate for cerebral blood flow during cardiac surgery, 17 and prospective data show that alterations in cerebral hemodynamics correlate with postoperative neurological function. 16 Asymmetric flow configurations predicted by CFD were associated with interhemispheric NIRS variability and Doppler flow asymmetry.
Central versus peripheral cannulation
Comparative analyses of femoral versus central cannulation demonstrate distinct hemodynamic behaviors.8,14 Retrograde femoral perfusion increases turbulence within the arch and may enhance mechanical stress on atherosclerotic segments. 8 Central ascending cannulation allows more controlled antegrade flow propagation. CFD comparisons of inflow sites confirm that central cannulation, when properly aligned toward the descending aorta, reduces arch recirculation and pathological shear gradients. 14
Integrated hemodynamic synthesis
Across the included studies, a consistent pattern emerged: unfavorable jet alignment increased wall impingement, shear stress heterogeneity, and embolic diversion, whereas optimized central inflow promoted more organized flow and lower simulated cerebral embolic exposure. Dispersive cannula designs further reduced focal shear concentration. Although outcome trials are lacking, these findings support the physiological relevance of cannulation strategy during CPB.12,19,20
Discussion
The present synthesis supports the concept that arterial cannulation during CPB represents a hemodynamically relevant intervention rather than a purely technical step. Across computational, experimental, and clinical investigations, cannula orientation, insertion depth, and tip geometry consistently emerged as important determinants of intra-aortic flow organization, influencing WSS distribution, embolic transport pathways, and cerebral perfusion stability.1–4,9–11,13,14 One of the most consistent observations across the available literature is the relationship between jet alignment and aortic wall interaction. Malpositioned or cranially directed inflow tends to increase focal wall impingement, recirculation, and shear stress heterogeneity, whereas more favorable alignment promotes a more organized longitudinal flow field with lower simulated embolic diversion toward supra-aortic vessels.1–4,9,10,13,14 Although derived largely from CFD studies, this mechanistic consistency strengthens the physiological relevance of cannulation strategy during CPB. The potential clinical implications of these findings are multifactorial. Peak WSS localizes to sites of jet-wall interaction, suggesting a possible role in plaque destabilization and embolic release in susceptible aortas.12,18–20 In parallel, embolic transport simulations indicate that unfavorable inflow direction may increase cerebral embolic exposure, while optimized alignment favors distal axial transport.1,2,10 In addition, experimental and translational studies suggest that improved cannula geometry may enhance cerebral flow symmetry and hemodynamic stability during bypass.5–7 Importantly, these hemodynamic principles should be interpreted within the constraints of real-world surgery. Precise control of cannula orientation may be limited by calcific aortic disease, ascending aortic diameter, arch angulation, cross-clamp position, restricted operative exposure, and other patient-specific anatomical factors. Therefore, the proposed configuration should be viewed as a hemodynamic target rather than a universally achievable technical standard. Finally, neurological injury during CPB remains multifactorial, and cannulation strategy represents only one modifiable component of a broader protective framework. Nevertheless, integration of patient-specific imaging, intraoperative monitoring, and hemodynamically informed cannulation planning may help refine neuroprotection strategies and deserves prospective clinical evaluation.
Limitations
Several limitations should be acknowledged. These references do not directly investigate CPB-specific jet flow conditions, but provide mechanistic insight into the relationship between abnormal shear stress and plaque vulnerability. CFD simulations rely on assumptions regarding wall compliance, flow pulsatility, and rheological modeling that may not fully replicate intraoperative conditions. Clinical evidence remains largely observational and lacks randomized comparisons specifically addressing cannula orientation geometry. Moreover, neurological injury during CPB is multifactorial, influenced by perfusion pressure, temperature management, hematocrit, inflammatory response, and baseline cerebrovascular reserve. Cannulation strategy represents one modifiable component within this broader physiological framework. Despite these limitations, the mechanistic coherence across fluid dynamic theory, computational modeling, experimental validation, and clinical monitoring is compelling. The integrated evidence suggests a plausible mechanistic sequence: jet misalignment leads to focal wall impingement and elevated WSS, promotes turbulence and vortex formation within the arch, increases embolic diversion toward cerebral vessels, and may destabilize vulnerable atherosclerotic plaques. Conversely, central lumen alignment with descending anterograde orientation preserves axial flow propagation, attenuates shear concentration, limits secondary vortex formation, and reduces simulated cerebral embolic exposure. Future investigations should focus on integrating patient-specific imaging with computational planning tools to guide cannulation strategy, as well as conducting prospective studies comparing cranial versus descending-oriented central cannulation with standardized neurological endpoints and multimodal cerebral monitoring (Table 1).
Summary of hemodynamic effects of arterial cannulation strategies during cardiopulmonary bypass.
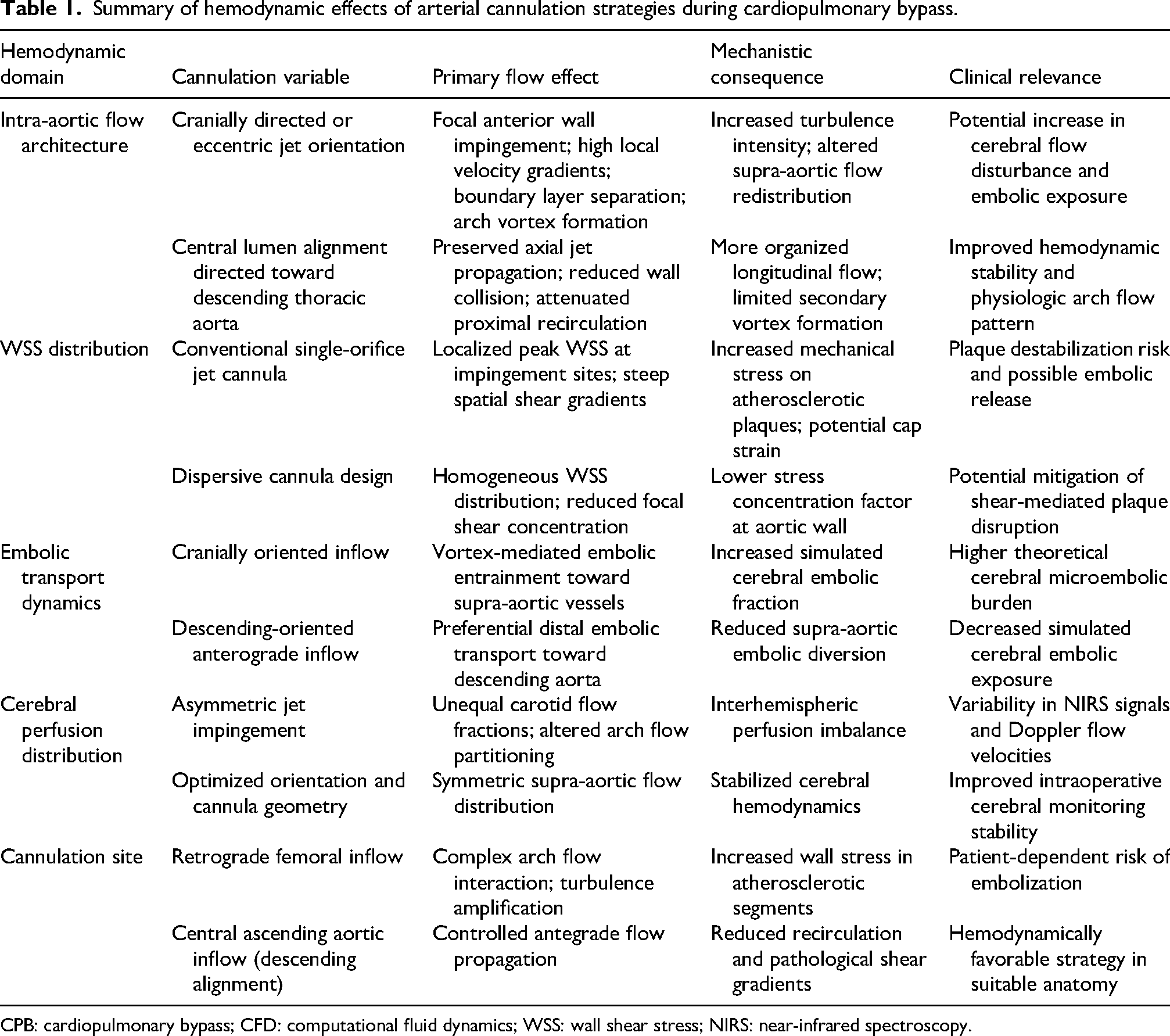
CPB: cardiopulmonary bypass; CFD: computational fluid dynamics; WSS: wall shear stress; NIRS: near-infrared spectroscopy.
Conclusion
Arterial cannulation during CPB should be regarded as a hemodynamically relevant component of extracorporeal support rather than a purely technical maneuver. Available computational, experimental, and clinical evidence indicates that cannula orientation, insertion depth, and tip design may influence WSS, embolic transport, and supra-aortic perfusion. Although prospective outcome studies are still needed, incorporation of hemodynamically informed cannulation principles may help refine neuroprotection strategies during cardiac surgery.
Footnotes
Ethical approval
Not applicable.
Informed consent
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.