
Abstract
Sutureless aortic valves, such as the Perceval (Corcym) valve, provide important procedural advantages and favorable mid- to long-term outcomes; however, potentially serious aortic complications related to their self-expanding stent structure remain incompletely understood. Thus, we report the case of an 85-year-old woman who developed early-onset localized ascending aortic dissection after aortic valve replacement with a sutureless valve. The entry tear was located at the level of the stent edge, slightly proximal to the aortotomy suture line, and the dissection extended only between these two points, suggesting a localized stent–aortic wall interaction with external mechanical stress as a potential trigger.
Introduction
Sutureless valves have been widely adopted in older adults and high-risk patients because they offer procedural advantages including reduced aortic cross-clamp time and favorable mid- to long-term outcomes.1,2 Despite these advantages, the self-expanding stent structure maintains continuous contact with the aortic wall, and only a few cases of aortic dissection after sutureless valve implantation have been reported.3,4 We report a case of early-onset localized ascending aortic dissection following sutureless aortic valve replacement (AVR) (Perceval, Corcym) with an entry tear at the stent edge after postoperative chest compressions.
Case presentation
An 85-year-old woman with osteoporosis and bronchial asthma was referred to our hospital for evaluation of a systolic ejection murmur. Echocardiography revealed severe aortic stenosis with reduced left ventricular function (35%), and moderate aortic regurgitation. Coronary angiography demonstrated chronic total occlusion of the circumflex artery (#11) with inferior-to-lateral wall asynergy. The maximum diameter of the ascending aorta was 38.9 mm, and that of the sinotubular junction (STJ) was 27.4 mm. The native aortic valve was tricuspid.
A sutureless valve was selected to minimize cardiopulmonary bypass and cross-clamp times in this older patient with reduced left ventricular function. Surgery was performed via a minimally invasive right anterior thoracotomy. A size M Perceval valve was selected based on annular and STJ dimensions. Intraoperative transesophageal echocardiography confirmed optimal coaxial valve deployment, and direct visualization verified sufficient clearance between the nitinol frame and the coronary ostia.
Five hours postoperatively, new-onset atrial fibrillation progressed to ventricular tachycardia, followed by an R-on-T phenomenon causing ventricular fibrillation and hemodynamic collapse refractory to direct-current defibrillation. Chest compressions were initiated, resulting in return of spontaneous circulation.
Contrast-enhanced computed tomography on postoperative day 4 revealed an ascending aortic dissection (Figure 1). The entry tear was located on the posterior lesser curvature of the aortic root at the level of the bare stent edge of the sutureless valve. A patent false lumen extended spirally toward the anterior wall, terminating at the aortotomy suture line. The dissection flap was located above the coronary ostia, with no coronary involvement (Figure 2). The patient was managed conservatively because the dissection was localized, did not involve the coronary ostia, and prosthetic valve function was preserved; surgical intervention was reserved for progression. Follow-up computed tomography and echocardiography 2 months showed no progression. On postoperative day 63, catheter ablation was performed for recurrent ventricular arrhythmias. Although the procedure was successfully, the patient developed hemorrhagic shock shortly after returning to the intensive care unit. Despite resuscitation and percutaneous cardiopulmonary support (PCPS), cardiac arrest recurred. Computed tomography revealed massive bleeding from the right femoral vein puncture site used for ablation access. Hemorrhage was uncontrollable because of systemic anticoagulation for PCPS. The patient died despite emergent surgical hemostasis.
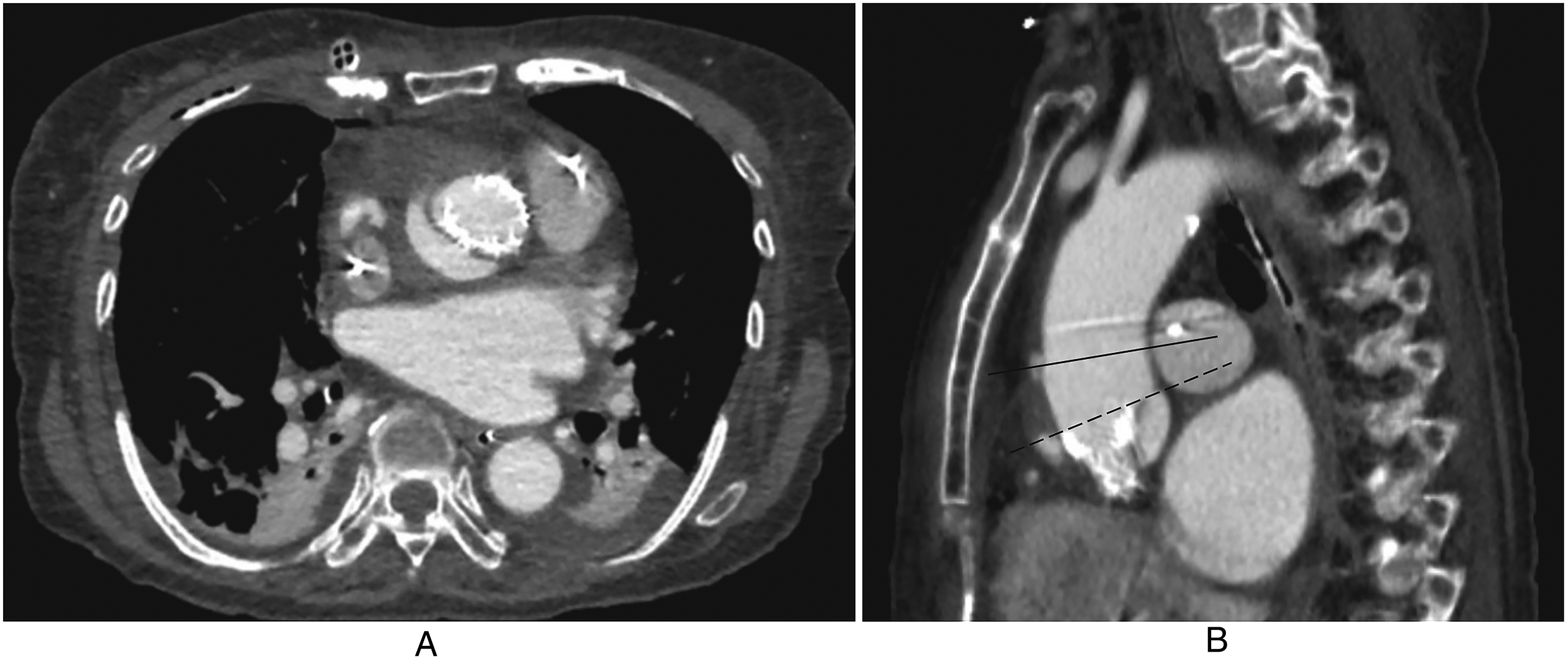
Axial (panel A) and sagittal (panel B) images show a localized dissection on the posterior lesser curvature of the ascending aorta. In panel B, the solid line indicates the aortotomy suture line, and the dotted line indicates the level of the stent edge.
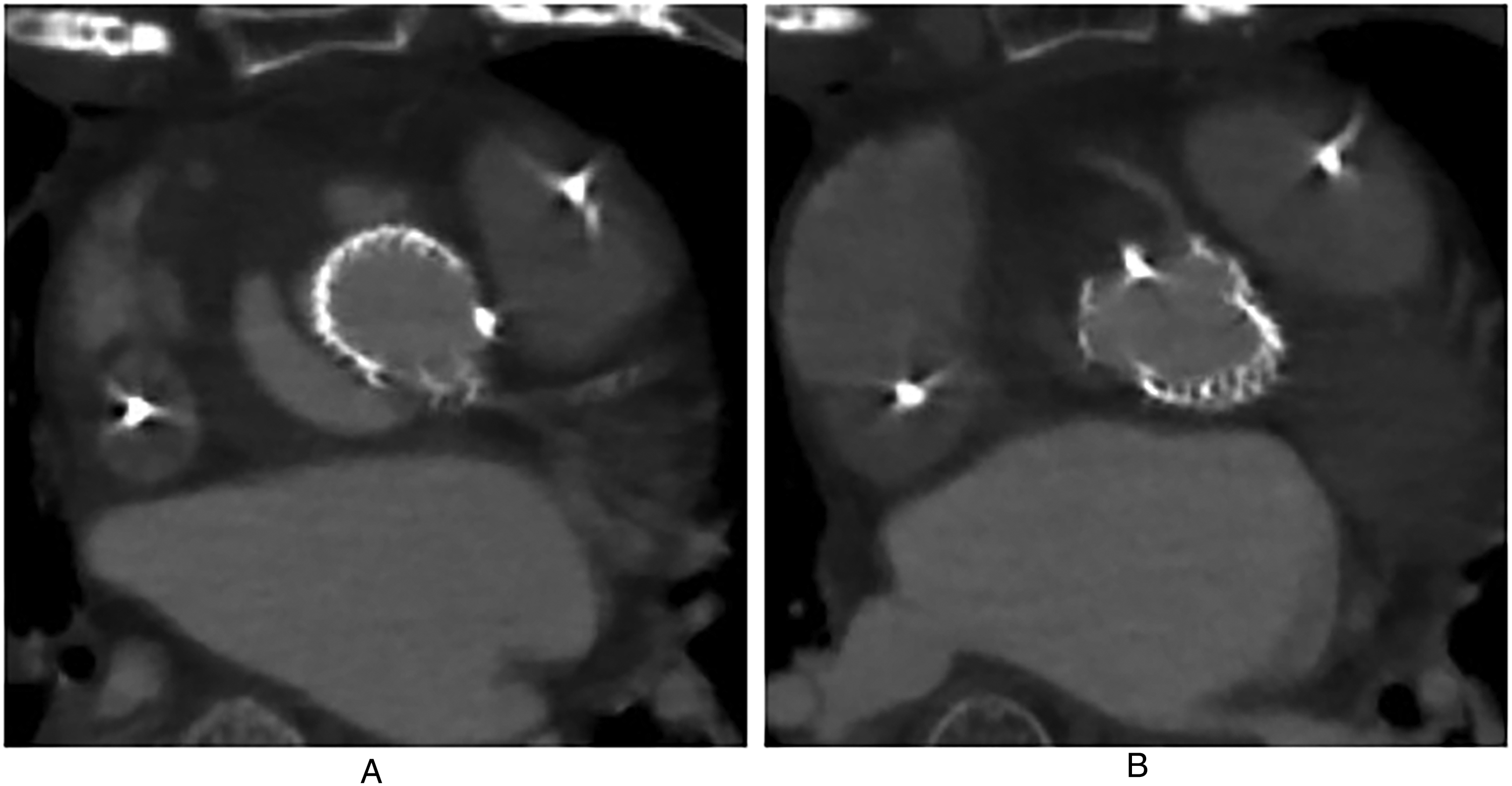
Axial (panel A) and axial (panel B) images show that the aortic root dissection does not extended to the coronary arteries.
Discussion
Sutureless valves consist of a self-expanding nitinol stent anchored to the aortic wall. Only a few cases of aortic dissection after valve implantation have been reported, and although the relationship between the stent frame and the aortic wall has been discussed, a direct causal role of the device remains unproven.3,4 In this case, the entry tear was located on the posterior lesser curvature of the aortic root at the bare stent edge, and the false lumen extended spirally toward the anterior wall, terminating at the aortotomy suture line. This anatomical relationship suggests that localized device–aortic wall interaction may have contributed to the focal origin of the dissection.
In our patient, ventricular tachycardia and fibrillation refractory to direct-current defibrillation required chest compressions. Because surgery was performed via minimally invasive right anterior thoracotomy without sternotomy, compressions were initiated without concern for sternal instability. External mechanical stress from chest compressions has been reported to cause aortic dissection. 5 Similarly, Scherner et al. reported transcatheter aortic valve prosthesis dysfunction attributed to mechanical stress during compressions. 6 These observations suggest that cardiopulmonary resuscitation can impose substantial mechanical stress on the aortic wall and valve frame, providing a plausible mechanism for focal dissection in this case.
To reduce anterior–posterior compression of the prosthetic valve, a modified technique that applies force more laterally toward the left ventricular apex has been proposed. 6 With increasing use of minimally invasive AVR and sutureless valves, resuscitation strategies that account for self-expanding valve frames may warrant particular consideration. In selected situations, modified chest compression techniques may help reduce excessive mechanical stress on prosthetic valve structures.
In conclusion, this case suggests that early-onset localized ascending aortic dissection after sutureless valve implantation may originate at the stent edge and be influenced by mechanical stress during postoperative resuscitation, particularly in minimally invasive surgical approaches.
Footnotes
Ethical approval
Not applicable.
Informed consent
Verbal informed consent was obtained from the patient's next of kin for the publication of this case report, including the accompanying images.
Author contributions
Yoshiki Hori performed investigation, visualization, writing—original draft, writing—review and editing. Kenichiro Sato did Investigation and Resources. Kei Akiyoshi did conceptualization, visualization, writing—original draft, writing—review and editing, supervision, project administration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data used in this case report are not publicly available due to patient privacy and ethical restrictions but are available from the corresponding author upon reasonable request.
Declaration of generative AI and AI-assisted technologies in the manuscript preparation process
During the preparation of this manuscript, the authors used ChatGPT to assist in English language proofreading. After using this tool/service, the authors reviewed and edited the content as required and take full responsibility for the content of the published article.