
Abstract
Background
Acute type B aortic dissection (TBAD) has traditionally been classified as either complicated or uncomplicated, guiding management toward urgent intervention or optimal medical therapy with surveillance. However, growing evidence suggests that this binary framework inadequately captures the biological and haemodynamic heterogeneity of the disease. A subset of patients initially classified as uncomplicated demonstrates clinical or radiological features associated with adverse outcomes, commonly described as “high-risk” uncomplicated TBAD.
Methods
A structured narrative review was conducted to synthesise contemporary evidence relating to clinical predictors, imaging markers, and outcome data in TBAD. Major observational studies, meta-analyses, guideline statements, and recent registry data were evaluated to examine the pathophysiological basis and prognostic significance of high-risk features and their implications for disease classification and management.
Results
Accumulating data indicate that TBAD represents a dynamic continuum of haemodynamic and morphological instability rather than discrete clinical categories. Clinical markers such as refractory pain and persistent hypertension provide early indicators of potential instability but demonstrate limited specificity. In contrast, imaging findings, including false lumen diameter, entry tear geometry, true lumen compression, and aortic diameter, more reliably reflect underlying biomechanical stress and risk of progression. Contemporary outcome studies and meta-analyses suggest that thoracic endovascular aortic repair promotes favourable aortic remodelling and may improve survival in selected patients with high-risk disease, although heterogeneity in patient selection remains substantial.
Conclusions
High-risk uncomplicated TBAD likely represents a transitional phenotype within a broader spectrum of disease progression. Moving beyond binary classification toward integrated clinical, imaging, and haemodynamic risk stratification may enable more precise identification of patients who would benefit from early intervention while avoiding overtreatment in stable disease.
Keywords
Introduction
Acute type B aortic dissection (TBAD) remains a complex and heterogeneous disease entity associated with substantial early morbidity and long-term aortic-related complications. Although epidemiological studies estimate an incidence ranging between 3 and 16 cases per 100,000 individuals annually, the true burden of TBAD is likely underestimated due to multiple reasons, including pre-hospital mortality, inconsistent registry reporting across healthcare systems, diagnostic/coding misclassification, and loss to follow-up in the community. 1 Beyond its epidemiology, the greatest contemporary challenge lies not in diagnosis but in the accurate early classification of disease severity and instability.
Traditionally, TBAD has been divided into two categories: complicated and uncomplicated presentations. Complicated TBAD (coTBAD) is defined by the presence of rupture, impending rupture, or end-organ malperfusion, typically prompting urgent intervention. In contrast, patients without these overt features have historically been labelled as uncomplicated (unTBAD) and managed with optimal medical therapy (OMT) and surveillance. 2 This binary framework has provided a pragmatic clinical guide for decades; however, increasing clinical experience and advances in imaging have exposed important limitations in this simplified classification.
A substantial proportion of patients initially deemed uncomplicated subsequently develop aneurysmal degeneration, refractory symptoms, or delayed complications requiring intervention. 3 Contemporary reporting standards from major vascular and cardiothoracic societies have therefore introduced a third category of “high-risk unTBAD,” encompassing patients who lack classical complicated features but possess clinical or radiological markers associated with adverse outcomes. These markers include persistent pain or hypertension, large false lumen (FL) dimensions, unfavourable entry tear characteristics, and specific morphological patterns identified on computed tomographic angiography (CTA). 4 Despite growing recognition of this subgroup, there is no universally accepted framework for how high-risk disease should inform classification or management strategies.
Advances in cross-sectional imaging, haemodynamic modelling, and longitudinal registry data increasingly suggest that TBAD represents a dynamic pathophysiological continuum rather than a static binary state. Features traditionally considered “high risk” often reflect underlying biomechanical instability of the dissected aorta, which may precede overt malperfusion or rupture. 5 Consequently, the distinction between unTBAD and coTBAD may be less discrete than current terminology implies. The persistence of this binary classification may contribute to variability in treatment strategies, uncertainty about the optimal timing of thoracic endovascular aortic repair (TEVAR), and ongoing debate about pre-emptive intervention. 6
This narrative review synthesises contemporary clinical, imaging, and outcome data on high-risk features of TBAD. It aims to examine whether high-risk unTBAD represents a transitional phenotype within a dynamic disease spectrum. By exploring the pathophysiological basis of instability, the prognostic significance of radiological markers, and the evolving evidence supporting early endovascular intervention, this review seeks to reassess the conceptual framework underpinning TBAD classification and highlight areas where future research may refine risk stratification and therapeutic decision-making.
Methods
This manuscript was developed as a structured narrative review to synthesise contemporary evidence on high-risk features in unTBAD and their implications for disease classification and management. A focused literature search was conducted in January 2026 using PubMed, Ovid MEDLINE, Embase, and Web of Science to identify relevant studies published between January 1980 and December 2025. Search terms included combinations of “type B aortic dissection,” “uncomplicated dissection,” “high-risk features,” “false lumen,” “optimal medical therapy,” “thoracic endovascular aortic repair,” and “disease progression.”
Eligible publications included original research articles, observational cohort studies, retrospective analyses, systematic reviews (and meta-analyses), and major guideline or consensus documents addressing clinical outcomes, imaging predictors, or therapeutic strategies in adult patients with TBAD. Studies limited to paediatric populations, non-English language publications, or reports without relevance to disease progression or risk stratification were excluded. Titles and abstracts were reviewed by two authors, followed by a collaborative review among all co-authors to ensure inclusion of clinically and scientifically relevant literature.
Findings were synthesised narratively with emphasis on recurring clinical and radiological predictors of instability, underlying pathophysiological mechanisms, and evolving treatment paradigms. The objective of this approach was to integrate available evidence into a conceptual framework examining whether high-risk unTBAD represents a transitional phenotype within a broader disease continuum.
Pathophysiological continuum of TBAD
TBAD has traditionally been conceptualised as a condition that can be categorised at presentation into either a complicated or an uncomplicated form. However, accumulating clinical and imaging data suggest that this binary framework may oversimplify a fundamentally dynamic disease process. Rather than representing discrete entities, TBAD appears to evolve along a pathophysiological continuum driven by haemodynamic forces, FL pressurisation, and progressive structural changes within the aortic wall. 7
Initiation of aortic dissection creates a communication between the true lumen (TL) and the FL through one or more entry tears, resulting in complex flow redistribution. Persistent perfusion of the FL exposes the already weakened aortic media to abnormal wall stress and shear forces, promoting progressive dilation and potential aneurysmal degeneration. 8 Early observational studies demonstrated that continued FL patency is associated with adverse long-term outcomes, including higher mortality and increased risk of aortic rupture. 9 Subsequent work highlighted that partial thrombosis of the FL may represent an even more unstable configuration, potentially creating a “blind sac” in which distal outflow is limited and intraluminal pressure rises. 10
Haemodynamic factors play a central role in determining disease trajectory. Larger proximal entry tears, limited distal re-entry channels, and unfavourable tear location along the lesser curvature of the aortic arch can amplify FL pressurisation, resulting in compression of the TL and dynamic obstruction of branch vessels. 11 These morphological features may precede the clinical manifestations traditionally used to define coTBAD. Consequently, patients who appear clinically stable at presentation may already possess underlying biomechanical instability that predisposes them to subsequent deterioration.
Emerging studies using computational flow modelling further emphasise the importance of flow dynamics in TBAD evolution. Parameters such as FL diameter, TL compression, and entry tear geometry are increasingly recognised as surrogates for haemodynamic stress within the dissected aorta. Observational studies have shown that greater FL size, longer dissection length, and involvement of major branch vessels correlate with accelerated aortic growth and higher rates of late intervention. 12 These findings support the concept that morphological features represent measurable expressions of the same pathophysiological processes that ultimately lead to clinical complications.
Viewing TBAD through a continuum model helps explain why a substantial proportion of patients initially classified as uncomplicated later experience aneurysmal degeneration or require delayed intervention despite OMT. It also underscores the limitations of relying solely on early clinical presentation to determine management strategy. Features currently labelled as “high risk” may therefore reflect an intermediate phase characterised by haemodynamic instability rather than a separate clinical category (Figure 1).
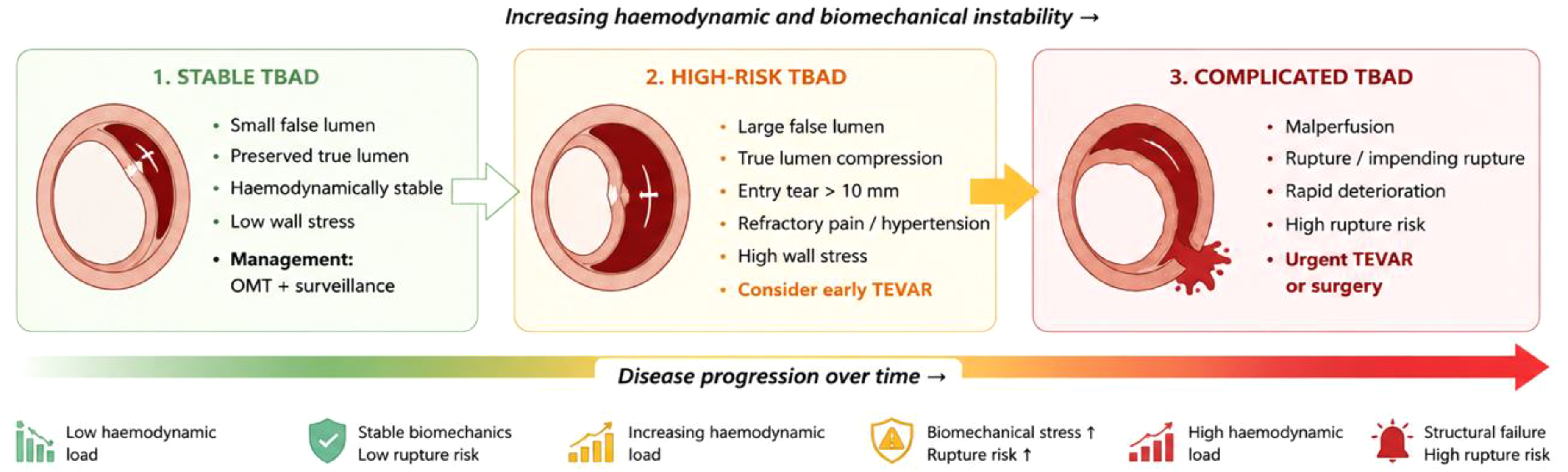
Conceptual continuum of instability in type B aortic dissection (TBAD).
Understanding TBAD as a progressive biological process provides a framework for integrating clinical symptoms, imaging markers, and treatment outcomes into a unified model of disease behaviour. This perspective forms the basis for examining clinical and radiological predictors of instability in subsequent sections and for reassessing whether high-risk unTBAD should be viewed as an early manifestation of complicated disease rather than a distinct classification.
Clinical predictors of instability
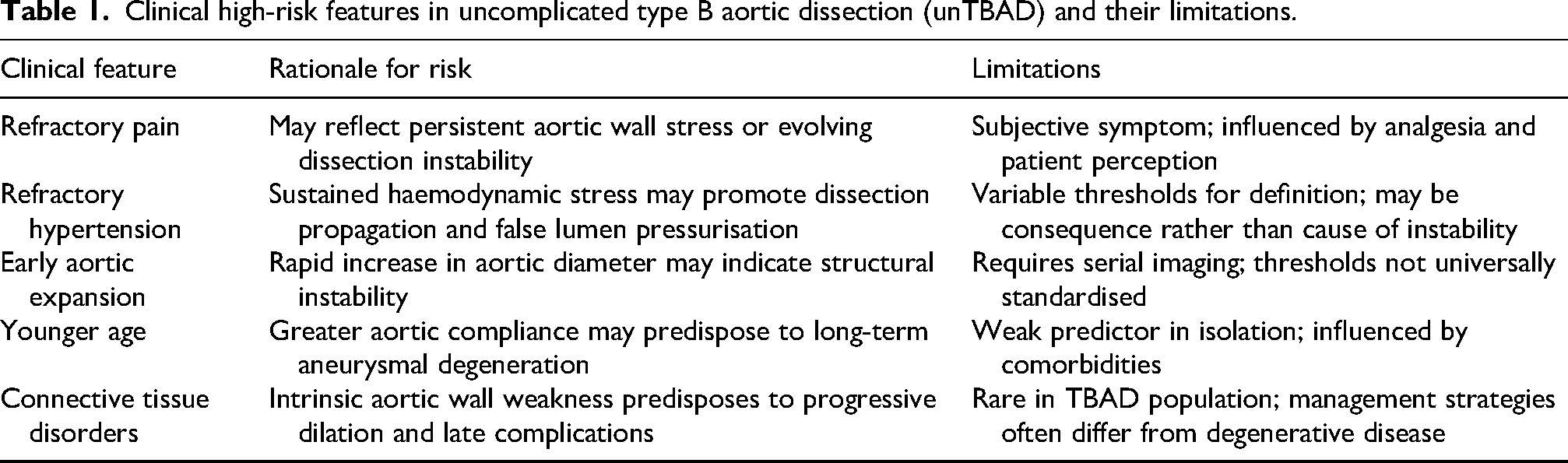
Although imaging findings have increasingly dominated risk stratification in TBAD, clinical presentation remains a critical component in identifying patients at risk of early deterioration. Contemporary reporting standards have introduced specific clinical features, most notably refractory pain and persistent hypertension, as markers of “high-risk” unTBAD. These features are thought to reflect ongoing haemodynamic stress within the dissected aorta, even in the absence of overt rupture or malperfusion (Table 1). 13
Clinical high-risk features in uncomplicated type B aortic dissection (unTBAD) and their limitations.
Persistent or refractory pain
Chest or back pain is the most common presenting symptom of acute TBAD, reported in the majority of patients within large registries. While pain at presentation is not itself a marker of disease severity, persistent or refractory symptoms despite adequate medical therapy have been associated with increased likelihood of adverse events and subsequent intervention.5–7 Observational series have demonstrated that patients undergoing TEVAR for refractory pain often exhibit favourable aortic remodelling compared with those treated for overt complications, suggesting that ongoing symptoms may reflect underlying biomechanical instability rather than purely subjective discomfort. 14
However, the use of pain as a high-risk criterion remains controversial. Pain perception is inherently subjective and influenced by analgesic strategy, patient comorbidities, and institutional thresholds for intervention. Proposed temporal definitions, such as failure to resolve symptoms within 12 h, may be difficult to standardise across clinical settings. Consequently, while refractory pain may serve as an important clinical warning sign, it should be interpreted in conjunction with objective radiological parameters rather than as an isolated indication for intervention. 15
Refractory hypertension
Persistent hypertension despite aggressive medical therapy has similarly been incorporated into definitions of high-risk TBAD. Ongoing elevation of systolic blood pressure increases shear stress across the intimal flap, potentially promoting expansion of the FL and propagation of the dissection. Retrospective studies have reported a higher prevalence of refractory hypertension among patients ultimately undergoing TEVAR, reinforcing its potential role as a surrogate marker of haemodynamic instability. 15
Nevertheless, hypertension as a predictor of progression is also subject to variability. Differences in antihypertensive protocols, patient adherence, and comorbid cardiovascular disease complicate interpretation. Furthermore, elevated blood pressure may represent a consequence rather than a cause of underlying morphological instability, underscoring the need for integrated clinical and imaging assessment.
Patient characteristics and comorbidities
Beyond acute symptomatology, several patient-level factors have been associated with increased risk of adverse outcomes in TBAD. Younger age has been linked to accelerated aortic growth, possibly reflecting greater intrinsic aortic elasticity and susceptibility to dilation. Conversely, connective tissue disorders such as Marfan syndrome and Ehlers–Danlos syndrome confer heightened vulnerability to progressive dissection and late aneurysmal degeneration. These conditions may amplify the biomechanical effects of FL pressurisation and are often considered when determining thresholds for early intervention.15,16
Despite these associations, clinical predictors alone have limited specificity for identifying patients who will progress from uncomplicated to complicated disease. Many individuals with persistent pain or hypertension remain stable under OMT, whereas others with minimal symptoms develop significant morphological changes over time. This variability highlights the importance of integrating clinical findings with objective imaging markers to achieve more accurate risk stratification.
Taken together, clinical features provide valuable insight into the dynamic nature of TBAD but should be viewed primarily as indicators of potential instability rather than definitive determinants of disease classification. Their greatest utility lies in prompting closer surveillance and comprehensive radiological evaluation, which remain central to identifying patients who may benefit from earlier intervention.
Imaging predictors of instability
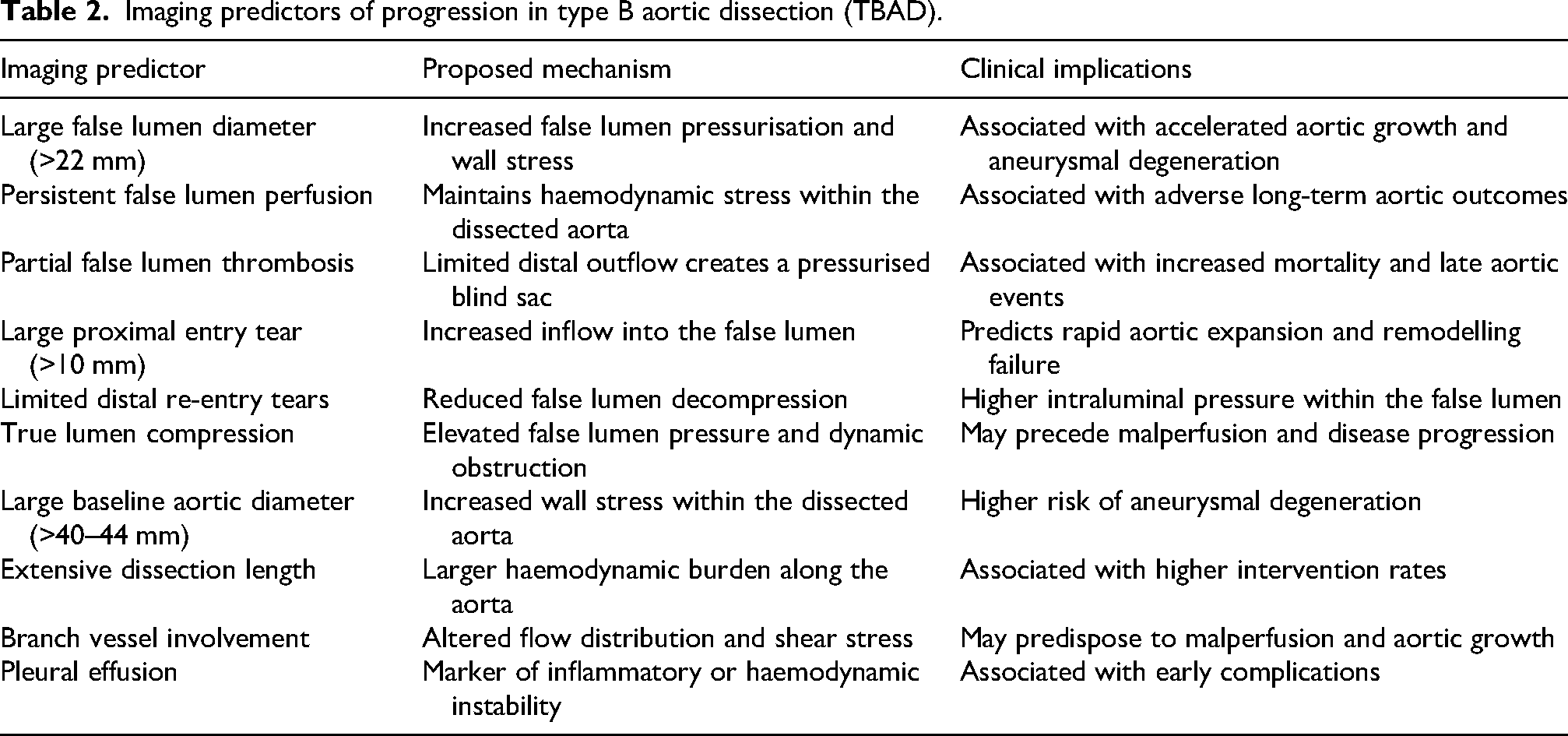
Advances in CTA and image-based haemodynamic assessment have significantly enhanced the ability to identify morphological features associated with adverse outcomes in TBAD. Unlike clinical predictors, which may be subjective or influenced by treatment variability, radiological parameters provide reproducible markers of structural instability within the dissected aorta. Increasing evidence suggests that these imaging findings may represent early expressions of the same pathophysiological processes that ultimately lead to rupture, malperfusion, or aneurysmal degeneration (Table 2). 17
Imaging predictors of progression in type B aortic dissection (TBAD).
False lumen characteristics
The morphology and behaviour of the FL remain among the most important predictors of disease progression. Persistent FL perfusion has been consistently associated with accelerated aortic growth and increased long-term mortality. Studies have demonstrated that a larger initial FL diameter, particularly measurements exceeding approximately 22 mm, correlates with higher rates of aneurysmal expansion and late intervention. The mechanism underlying this association is thought to relate to sustained pressurisation of the FL, which increases wall stress and promotes progressive dilatation of the aortic wall.5–7
As aforementioned, partial thrombosis of the FL has emerged as a particularly high-risk configuration. In this setting, limited distal re-entry may create a pressurised blind sac, increasing haemodynamic stress despite apparent thrombosis. Observational data have suggested that patients with partially thrombosed FLs experience worse long-term outcomes than those with either complete patency or complete thrombosis, highlighting the complexity of interpreting FL morphology. 10 Additionally, extensive branch vessel involvement and increased dissection length have been linked to adverse events, potentially reflecting greater overall haemodynamic burden. 11
Aortic diameter and true lumen compression
Baseline aortic diameter represents another well-established predictor of progression. Maximal thoracic aortic dimensions exceeding 40–44 mm have also been associated with increased risk of late aneurysmal degeneration and intervention. The relationship between aortic size and outcomes likely reflects cumulative wall stress rather than diameter alone, as larger vessels are subjected to greater radial force during systolic pressure fluctuations.5–7
Compression of the TL by an expanding FL is also an important radiological marker of instability. Severe TL narrowing may indicate elevated FL pressures and can precede dynamic malperfusion even in the absence of overt clinical symptoms. Morphological patterns such as circumferential or free-floating TL configurations further suggest advanced dissection mechanics and may identify patients at heightened risk of deterioration. 18
Entry tear characteristics
The location, size, and number of entry tears significantly influence haemodynamic behaviour within the dissected aorta. Larger proximal entry tears, particularly those exceeding 10 mm in length, have been associated with increased FL pressurisation and faster growth. Tears located along the lesser curvature of the proximal descending thoracic aorta or in proximity to the left subclavian artery have similarly been linked to poorer outcomes, possibly due to altered flow dynamics and increased wall shear stress in these regions.5–7
The number of re-entry tears may also affect disease trajectory. Limited distal outflow can lead to elevated intraluminal pressure within the FL, whereas multiple re-entry sites may allow decompression of the false channel. These observations reinforce the importance of assessing entry tear geometry as part of comprehensive risk stratification. 8
Additional radiological markers
Several additional imaging findings have been proposed as markers of high-risk TBAD. The presence of a left-sided pleural effusion has been associated with increased rates of complications and may reflect ongoing inflammatory or haemodynamic stress within the thoracic cavity. 19 Similarly, longitudinal expansion of intramural haematoma and greater dissection length have been suggested as predictors of poor outcomes, although their prognostic value remains less consistently defined. 18
Collectively, these imaging predictors illustrate that morphological instability often precedes clinical deterioration. Rather than representing isolated measurements, features such as FL diameter, entry tear geometry, and TL compression should be interpreted as interrelated indicators of underlying haemodynamic stress. Integrating these parameters into a unified assessment may improve early identification of patients who fall along the unstable end of the TBAD spectrum and may benefit from closer surveillance or earlier intervention (Figure 2).
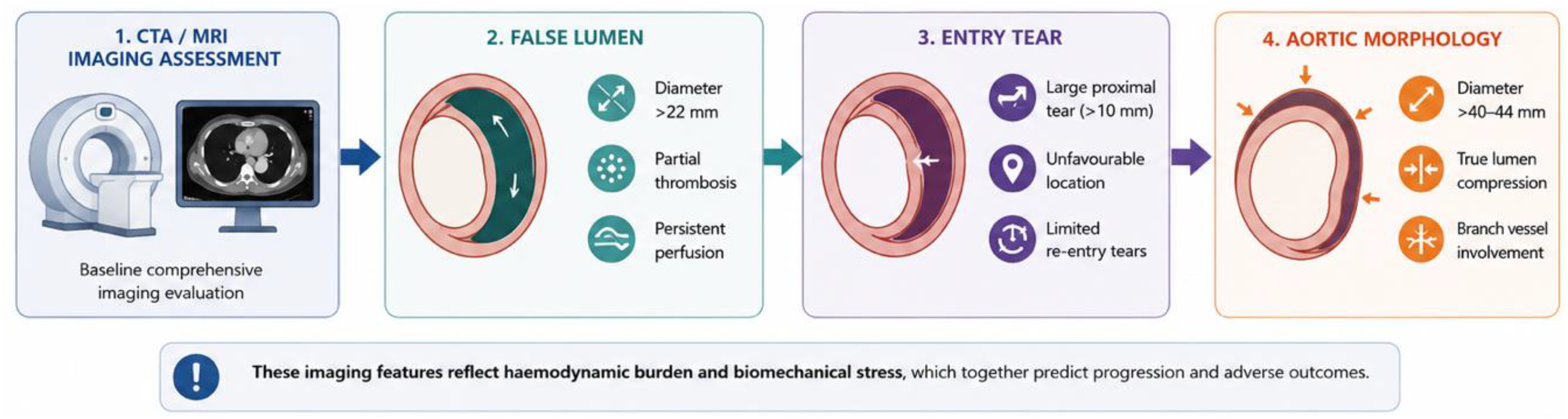
Imaging predictors associated with progression in type B aortic dissection (TBAD).
Relative prognostic weight and interaction of high-risk features
While numerous clinical and imaging features have been associated with adverse outcomes in TBAD, their relative prognostic importance and independence are not uniform. Among radiological markers, FL diameter, baseline aortic diameter, and entry tear characteristics demonstrate the most consistent independent associations with aortic growth and late intervention across observational studies and meta-analyses. In particular, FL diameter has emerged as one of the strongest predictors of aneurysmal degeneration, likely reflecting cumulative haemodynamic stress within the dissected aorta.2,16,17
Other features, including partial FL thrombosis, TL compression, and pleural effusion, are also associated with adverse outcomes but may function more as surrogate markers of underlying haemodynamic instability rather than independent drivers of disease progression. Their prognostic value is therefore context-dependent and may vary across patient populations and study designs.2,16,17
Importantly, increasing evidence suggests that risk is not determined by individual features in isolation but rather by their interaction. For example, combinations of morphological characteristics, such as large FL diameter with limited distal re-entry, or proximal entry tear location with TL compression, may amplify FL pressurisation and confer disproportionately higher risk than any single parameter alone. This synergistic effect supports the concept that TBAD progression is governed by integrated biomechanical forces rather than discrete anatomical thresholds.
From a clinical perspective, these observations reinforce the need for composite risk assessment strategies. Patients exhibiting multiple high-risk imaging features may represent a subgroup with morphologically unstable disease who are more likely to benefit from early intervention, whereas isolated findings may warrant closer surveillance rather than immediate treatment escalation.
Outcome evidence
Management strategies for unTBAD have evolved considerably over the past decade, shifting from a paradigm centred exclusively on OMT toward increasing consideration of early TEVAR in selected patients. While early randomised trials provided foundational insight into endovascular intervention, contemporary understanding is now largely shaped by large observational datasets and recent meta-analyses that incorporate broader patient populations and modern endovascular techniques.
Recent European pre-trial work from the European UnTBAD (EU-TBAR) collaborative has provided important contemporary context for these findings. A multicentre cross-sectional evaluation demonstrated substantial variability in European practice patterns, with increasing adoption of pre-emptive TEVAR and recognition that unTBAD represents a dynamic disease process rather than a static clinical state. Notably, rapid aortic enlargement and morphological instability were consistently prioritised as key risk factors, reinforcing the importance of imaging-driven risk stratification when interpreting contemporary outcome data. 20
Contemporary data from the EU-TBAR Pillar 2 further contextualise these findings by providing real-world clinical outcomes following TEVAR in unTBAD. In a prospective multicentre cohort of 263 patients undergoing TEVAR across six European countries, in-hospital mortality was 9.9%, with a follow-up mortality of 14.1% at approximately one year. Reintervention occurred in 18.3% of patients at a median of 168 days, with discharge endoleak independently associated with a threefold increase in reintervention risk. Postoperative acute kidney injury emerged as the strongest predictor of mortality, whereas higher baseline haemoglobin and renal function were protective. Imaging follow-up demonstrated complete FL thrombosis in 42.1% and partial thrombosis in 39.3%, reinforcing the role of TEVAR in promoting aortic remodelling while highlighting persistent heterogeneity in outcomes. 21 These data illustrate both the potential benefits and limitations of pre-emptive TEVAR and underscore the need for refined patient selection strategies.
Recent pooled analyses have highlighted the complex relationship between TEVAR, aortic remodelling, and long-term survival. A comprehensive systematic review and meta-analysis encompassing more than 25,000 patients with unTBAD demonstrated that TEVAR was associated with improved mid-term survival compared with OMT alone, despite no significant differences in early mortality. Survival rates at 1, 2, and 3 years were consistently higher in patients undergoing TEVAR, although the magnitude of benefit varied across studies and patient subgroups. Furthermore, TEVAR resulted in significantly lower all-cause and aorta-related mortality rates. Importantly, this analysis also emphasised the greater morphological remodelling observed with TEVAR, which was nearly 10-fold greater than with OMT in the unTBAD cohort. 22
These contemporary findings reflect a broader trend within the literature. Large meta-analyses and registry-based studies increasingly suggest that TEVAR may reduce aortic-related adverse events and promote favourable aortic remodelling, particularly in patients with morphological features associated with instability. However, heterogeneity in patient selection remains substantial. In many studies, individuals undergoing TEVAR tend to exhibit larger aortic diameters, greater FL dimensions, or other high-risk characteristics at baseline, raising the possibility of selection bias when comparing outcomes with medically managed cohorts. Differences in dissection chronicity, extent of aortic coverage, and institutional thresholds for intervention further complicate the interpretation of pooled results.23–28 Reviews have suggested that earlier endovascular intervention in the acute or subacute phase of unTBAD offers better outcomes than in chronic dissections, which often feature less compliant dissection flaps. 29
Another important observation emerging from recent analyses is that the potential advantages of early TEVAR, including improved FL thrombosis and reduced rates of late aneurysmal degeneration, must be weighed against procedural risks such as retrograde type A dissection, stroke, spinal cord ischaemia, and device-related complications. Yet overall, contemporary datasets show a positive trend in the short-, mid- and long-term following pre-emptive TEVAR relative to OMT in high-risk unTBAD cohorts.23–28 Nevertheless, current evidence still does not support indiscriminate application of TEVAR in all unTBAD patients.
The variability observed across modern meta-analyses reinforces the importance of risk stratification rather than uniform treatment algorithms. Patients exhibiting high-risk clinical or radiological features may represent a subgroup in whom early endovascular therapy confers greater benefit, whereas truly stable dissections may derive limited advantage from intervention beyond careful surveillance. This distinction aligns with the emerging concept that TBAD exists along a continuum of instability, and that treatment decisions should be guided by integrated assessment of morphology, haemodynamics, and clinical trajectory.
Taken together, current outcome evidence suggests that TEVAR offers meaningful improvements in aortic remodelling and may confer survival advantages in selected populations, yet definitive proof of universal benefit remains lacking. The heterogeneity of available data highlights a central challenge in TBAD management: identifying which patients truly represent high-risk disease and therefore stand to benefit most from early intervention. This uncertainty provides a rationale for re-examining current classification systems and supports the need for a more dynamic framework integrating both clinical and imaging predictors of instability (Figure 3).
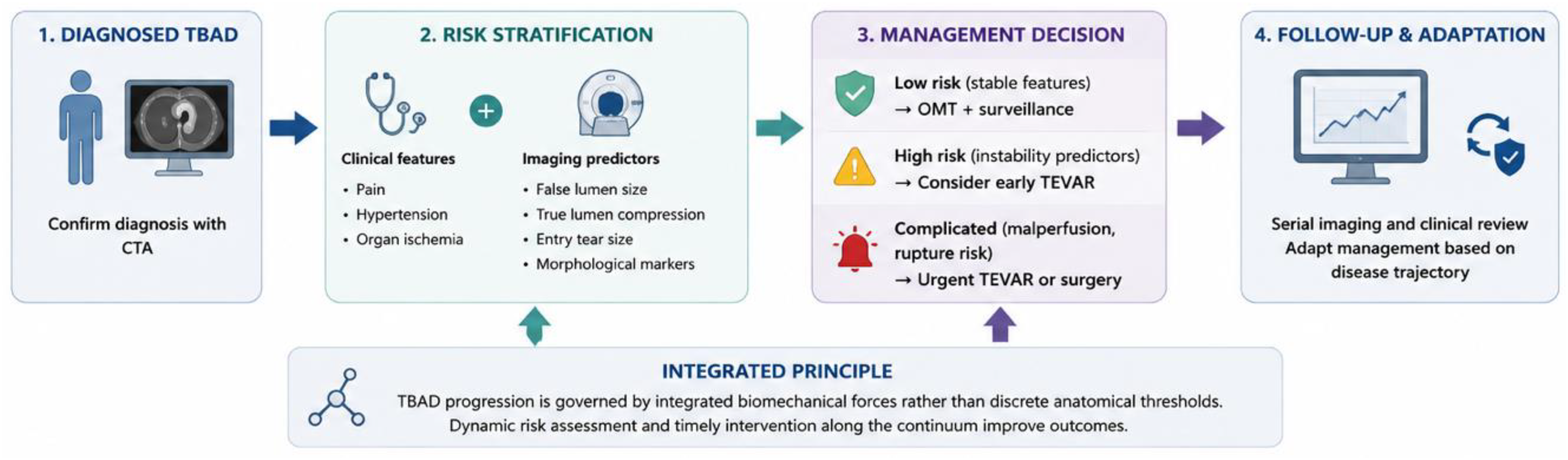
Clinical decision framework for management of type B aortic dissection (TBAD).
Why the current classification fails
The traditional classification of TBAD into “complicated” and “uncomplicated” categories has provided a pragmatic framework for clinical decision-making for decades. However, accumulating evidence suggests that this binary model may inadequately capture the biological and haemodynamic complexity of the disease. Increasingly, both clinical experience and contemporary literature highlight substantial heterogeneity within patients labelled as uncomplicated, raising concerns that current definitions may oversimplify risk stratification and inadvertently delay appropriate intervention. 7
Recent critical analyses of existing guidelines have underscored inconsistencies in the interpretation and application of high-risk criteria. A contemporary review comparing international recommendations noted that, despite broad consensus on the need for risk-based management, significant variation persists in defining high-risk features and determining when TEVAR should be considered. 13 These discrepancies reflect ongoing uncertainty regarding whether high-risk unTBAD represents a distinct clinical entity or an early manifestation of complicated disease.
Similarly, recent work examining challenges in diagnosing and categorising unTBAD has emphasised that reliance on overt malperfusion or rupture as defining thresholds may fail to identify patients with underlying morphological instability. The authors highlighted that many patients initially categorised as uncomplicated exhibit dynamic disease progression driven by FL pressurisation and unfavourable anatomy, suggesting that early classification may not reliably predict long-term behaviour. 2
Contemporary European governance analyses further highlight limitations of the classification paradigm. The EU-TBAR Pillar 1 pre-trial study revealed wide variation in risk-assessment strategies, transfer pathways, and intervention thresholds across participating centres, reflecting ongoing uncertainty about the definition of uncomplicated disease. 20 These findings underscore the practical challenges clinicians face when applying static classifications to a condition increasingly recognised as biologically heterogeneous and temporally dynamic.
The limitations of the binary paradigm are further illustrated by studies questioning the very concept of “uncomplicated” TBAD. Emerging literature suggests that this terminology may be a misnomer, as many patients who appear stable exhibit imaging or clinical characteristics associated with adverse outcomes. Rather than reflecting true stability, the absence of overt complications at presentation may represent an early phase within an evolving disease process.6,7
Another important issue lies in the evolving criteria for intervention. Contemporary discussions regarding indications for endovascular repair increasingly emphasise morphological features, including FL size, entry tear characteristics, and aortic diameter, rather than solely clinical complications. This shift highlights a growing recognition that haemodynamic instability may precede overt symptoms, challenging traditional definitions that separate uncomplicated from coTBAD.4,5,15
Collectively, these observations suggest that current classification systems may inadequately reflect the dynamic nature of TBAD. A model based solely on the presence or absence of immediate complications risks overlooking patients in an intermediate state characterised by morphological instability and elevated long-term risk. Such misclassification may contribute to variability in treatment strategies, uncertainty about the timing of TEVAR, and persistent debate in contemporary practice.
Reconsidering TBAD classification, therefore, requires moving beyond static definitions toward a framework that incorporates clinical presentation, imaging morphology, and underlying haemodynamic processes. Recognising high-risk unTBAD as part of a continuous spectrum rather than a discrete category provides a foundation for developing more individualised and biologically grounded treatment strategies.
Proposed conceptual model
The growing recognition of heterogeneity within unTBAD has prompted calls for a more nuanced conceptual framework that better reflects disease biology. Rather than representing a separate classification, high-risk unTBAD may be more accurately understood as a transitional phenotype situated between stable dissection and overtly complicated disease. This perspective aligns with emerging data highlighting the central role of FL dynamics, morphological instability, and haemodynamic stress in determining clinical trajectory.
A continuum-based model proposes that TBAD progresses through overlapping stages characterised by increasing biomechanical instability. In the earliest phase, patients may present with stable haemodynamics and limited morphological disruption, responding well to OMT and surveillance. As the dissection evolves, features such as progressive FL expansion, adverse entry tear geometry, or persistent hypertension may indicate an intermediate stage in which structural instability exists despite the absence of classical complications. Ultimately, continued FL pressurisation and aortic wall stress may culminate in rupture, malperfusion, or rapid aneurysmal degeneration; the hallmarks of coTBAD.
The evolving EU-TBAR trial framework provides a pragmatic example of how a continuum-based conceptual model can be translated into a clinical research design. The structured pre-trial setup emphasises equipoise in high-risk uncomplicated TBAD and highlights the need for refined risk stratification incorporating morphological and haemodynamic parameters, supporting the notion that transitional phenotypes exist between stable and overtly complicated disease.20,21
Within this framework, the aforementioned high-risk features are interpreted not as separate diagnostic criteria but as markers of evolving instability along the TBAD spectrum. This perspective helps reconcile apparent contradictions within the literature, where patients labelled as uncomplicated nonetheless experience high rates of delayed intervention or aortic-related events. In practical terms, the presence of multiple high-risk imaging features may have additive or synergistic prognostic significance. A composite approach incorporating both the number and type of risk factors may therefore provide a more clinically useful framework than reliance on any single parameter.
Importantly, adopting a continuum-based model does not imply that all high-risk patients should undergo early intervention. Instead, it emphasises the need for integrated assessment combining clinical trajectory, imaging morphology, and individual patient factors. The goal is not to replace existing classifications entirely but to refine them by recognising that TBAD represents a dynamic process rather than a static diagnosis.
Conceptually, TBAD may therefore be viewed as progressing across three overlapping domains:
Haemodynamically stable dissection: characterised by limited FL pressurisation and favourable morphology. Morphologically unstable dissection (high-risk TBAD): defined by radiological and clinical indicators of increasing biomechanical stress. Clinically complicated dissection: marked by rupture, malperfusion, or rapid deterioration.
This model provides a framework for interpreting contemporary outcome data, guiding individualised decision-making, and informing future research aimed at identifying objective markers of instability. By shifting the focus from rigid categorisation toward dynamic risk stratification, clinicians may better align treatment strategies with the biological behaviour of the disease.
Future research priorities
Despite significant advances in imaging and endovascular therapy, the optimal management of unTBAD remains constrained by limitations in risk stratification and predictive modelling. Current clinical decision-making relies heavily on static anatomical measurements and symptom-based definitions that may not adequately capture the dynamic biomechanical environment of the dissected aorta. Future research must therefore move beyond descriptive risk factors toward integrated, data-driven frameworks capable of predicting disease evolution at an individual level (Figure 4).
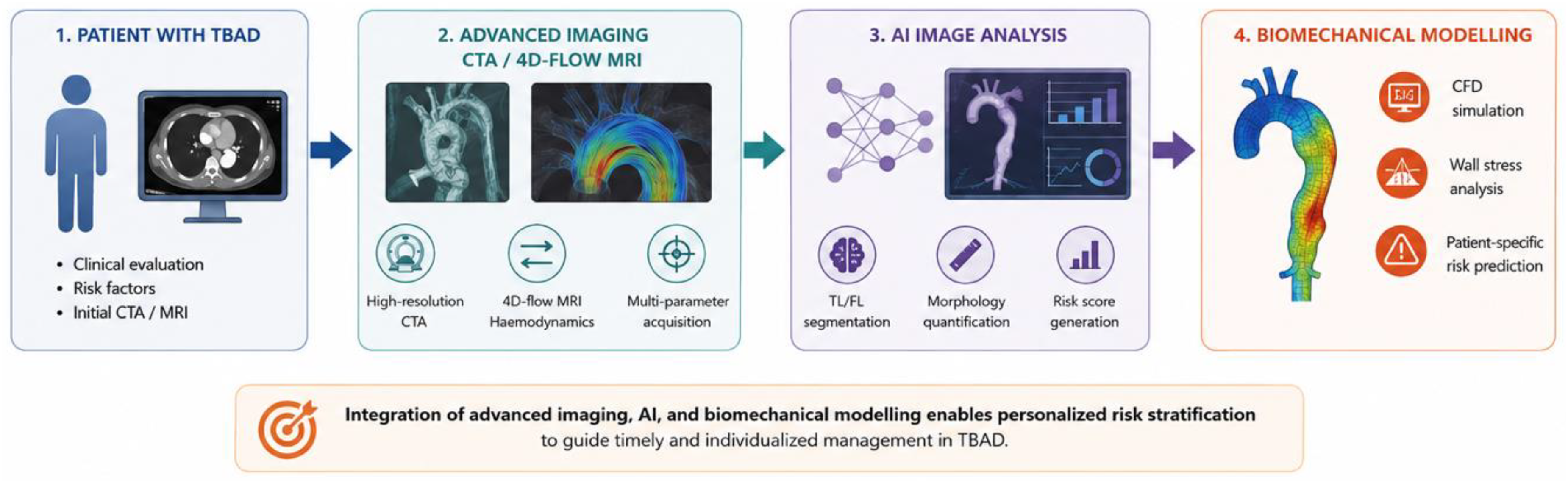
Proposed precision framework for future risk stratification in type B aortic dissection (TBAD).
Artificial intelligence and advanced imaging analytics
Recent developments in artificial intelligence (AI) and automated image analysis have demonstrated considerable potential for transforming TBAD assessment. Machine learning algorithms capable of segmenting true and FL morphology, quantifying volumetric changes, and identifying subtle radiological patterns may enable more precise identification of high-risk dissections. Emerging studies suggest that AI-based models can integrate multiple imaging parameters, including lumen geometry, branch vessel involvement, and entry tear characteristics, to generate predictive risk scores that outperform those based solely on diameter thresholds.30,31
Beyond static measurements, dynamic imaging modalities, such as four-dimensional flow magnetic resonance imaging, and advanced computational fluid dynamics (CFD) modelling, offer insight into the haemodynamic forces driving disease progression. Quantification of wall shear stress, flow vortices, and pressure gradients within the FL may reveal early indicators of instability before clinical complications arise.32,33 As these technologies mature, integration of AI-driven analysis with biomechanical modelling could enable real-time prediction of FL pressurisation and individualised assessment of intervention timing.
Biomechanics and haemodynamic modelling
The conceptual shift toward viewing TBAD as a continuum of biomechanical instability underscores the need for deeper investigation into aortic wall mechanics. Current classification systems rely primarily on anatomical descriptors, yet experimental and computational studies increasingly demonstrate that tear geometry, flow distribution, and wall stress patterns may be more informative predictors of progression. 8 Future research should focus on developing validated biomechanical indices, potentially derived from CFD simulations, that quantify instability in a reproducible manner.
Recent work exploring the integration of haemodynamic modelling with clinical imaging highlights the potential for personalised simulations to guide endovascular planning and device selection. Such approaches could allow clinicians to predict the haemodynamic consequences of TEVAR, including alterations in FL pressure and long-term remodelling trajectories. 34 The development of standardised computational pipelines and multicentre validation studies will be essential to translating these tools into routine clinical practice.
Registry science and data integration
A major barrier to advancing TBAD management is the relative scarcity of comprehensive longitudinal datasets capturing detailed morphological, procedural, and outcome variables. Contemporary analyses emphasise the need for large-scale, prospectively maintained registries capable of integrating imaging, clinical, and procedural data across diverse populations. Enhanced registry infrastructure would enable more robust evaluation of high-risk features, facilitate validation of AI-based prediction models, and support adaptive clinical trial design.
The EU-TBAR collaborative represents an important step toward a harmonised European data infrastructure. Pre-trial analyses have demonstrated the feasibility of integrating governance, outcome reporting, and economic evaluation into a unified framework designed to support prospective randomised evaluation of pre-emptive TEVAR. Such initiatives exemplify how coordinated registry science and trial development can bridge the gap between observational insights and definitive evidence generation.20,21
Centralised multidisciplinary aortic programmes are well-positioned to drive these initiatives by standardising imaging protocols, ensuring consistent data collection, and promoting collaborative research networks. Importantly, future registries should incorporate granular haemodynamic and biomechanical variables rather than relying solely on traditional anatomical descriptors, thereby enabling deeper exploration of disease mechanisms.
Evolving clinical trial design
Randomised trials evaluating TEVAR in unTBAD have historically struggled with heterogeneous patient populations and variable definitions of high-risk disease. Future studies may benefit from incorporating imaging-derived risk scores or biomechanical markers as inclusion criteria, enabling more targeted evaluation of interventions in morphologically unstable dissections. Adaptive trial designs that integrate real-world registry data and machine learning-driven risk stratification could provide a more efficient framework for evaluating evolving endovascular technologies.28,35
Collectively, these advances point toward a future in which TBAD management transitions from reactive classification toward precision risk stratification. By combining AI-driven imaging analysis, biomechanical modelling, and comprehensive registry science, clinicians may ultimately move beyond binary definitions toward individualised prediction of disease trajectory. Such an approach has the potential to refine intervention timing, reduce overtreatment, and improve long-term outcomes for patients across the TBAD spectrum.
Conclusion
TBAD is increasingly recognised as a dynamic disease process that may not be adequately captured by the traditional binary classification of complicated versus uncomplicated presentations. A growing body of clinical, imaging, and outcome data suggests that patients described as ‘high-risk uncomplicated’ frequently exhibit morphological and haemodynamic features consistent with evolving instability, supporting the concept of a continuum rather than discrete disease states. Clinical indicators such as persistent pain and refractory hypertension, together with objective imaging markers including FL size, entry tear characteristics, and TL compression, may identify patients at heightened risk of progression despite the absence of overt complications at presentation. Contemporary evidence demonstrates that TEVAR promotes favourable aortic remodelling in selected patients, yet uncertainty remains regarding universal benefit, emphasising the importance of individualised risk stratification. Future integration of AI-assisted imaging, biomechanical modelling, and large-scale registry data may enable more precise identification of unstable phenotypes and guide intervention timing. Reframing high-risk unTBAD within a continuum-based model offers a path toward more nuanced classification and personalised management strategies aligned with the biological behaviour of the disease.
Footnotes
Ethical approval
Not applicable.
Informed consent
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting this manuscript is publicly available in electronic databases.