
Abstract
Objectives
The hemodynamic significance of coronary artery stenosis is associated with graft patency in coronary artery bypass grafting. However, it remains unclear whether hyperemic or nonhyperemic intracoronary pressure indices better predict graft patency. This study aimed to compare the ability of intracoronary pressure indices to predict the graft patency of the in-situ internal thoracic artery (ITA) to the left anterior descending (LAD) artery.
Methods
This study included the patients who had the LAD artery evaluated with both hyperemic and nonhyperemic intracoronary pressure indices prior to surgery, underwent the in-situ ITA to LAD artery bypass, and subsequently underwent coronary computed tomography angiography to assess the graft patency postoperatively. The study endpoint was graft hypoperfusion, defined as either graft occlusion or graft string formation.
Results
Of the 105 patients, 10 patients (9.5%) showed graft hypoperfusion (occlusion; six patients, string; four patients). Patients with graft hypoperfusion had significantly less severe coronary artery stenosis determined by intracoronary pressure indices (fractional flow reserve (FFR): 0.74 vs 0.66; p = .013, nonhyperemic pressure ratio (NHPR): 0.88 vs 0.76; p < .01) and significantly lower intraoperative mean graft flow (16 vs 24 mL/min, p < .01) compared to those with patent grafts. Receiver operating characteristic curve analysis indicated that NHPR was more predictive of graft hypoperfusion than FFR (area under the curve: 0.74 vs 0.86, p = .049).
Conclusion
NHPR showed a greater ability to predict graft hypoperfusion in the ITA to LAD artery bypass than FFR.
Introduction
The hemodynamic significance of target vessel stenosis plays a crucial role in graft patency after coronary artery bypass grafting (CABG). The in-situ left internal thoracic artery (ITA) to the left anterior descending (LAD) artery is considered the most durable conduit, 1 however, in daily surgical practice, graft failure sometimes occurs when conduits are anastomosed on lesions with limited physiological severity, leading to competitive flow from native coronary artery and reduced graft function. 2 Recent international guidelines endorse the use of fractional flow reserve (FFR) or nonhyperemic pressure ratios (NHPR) to evaluate intermediate coronary stenoses.3–5 In CABG, several reports have demonstrated the utility of FFR for predicting graft patency, highlighting its role in surgical decision-making.6,7 However, the clinical significance of NHPR in this context remains less well established, and consensus has not been reached. Given the increasing use of physiological assessment in preoperative planning, clarification of these indices is of particular importance to cardiac surgeons. Therefore, this study sought to compare the predictive value of preoperative FFR and NHPR for patency of in-situ ITA–LAD using postoperative coronary computed tomography angiography (CCTA).
Material and methods
Study design
This study was designed as a single-center retrospective cohort analysis. Consecutive patients who underwent elective CABG with an in-situ ITA graft to the LAD at our institution between August 2010 and April 2023 were retrospectively reviewed. Participants were categorized into two groups based on postoperative graft findings: a patent graft group and a graft hypoperfusion group, defined as graft failure or a string sign, in which the conduit remained patent but exhibited minimal antegrade flow.
Inclusion and exclusion criteria
Patients were included if they underwent preoperative invasive physiological assessment and had complete data available for both invasive physiological measurements and postoperative coronary computed tomographic angiography for graft evaluation. Patients were excluded if the LAD had not been evaluated using both FFR and NHPR, or if postoperative CCTA was unavailable due to contraindications or patient refusal. The study flow is summarized in Supplemental Figure S1.
Ethical statement
This study was approved by the Wakayama Medical University Institutional Review Board (Approval No. 3539, approval date: 21st June, 2022). The need for informed consent was waived because of the retrospective and observational nature of this study, but the study was conducted in accordance with the principles of the Declaration of Helsinki.
Coronary angiography
Coronary angiography was performed following standard procedure, with images acquired from multiple projections and digitally stored for quantitative analysis. Quantitative coronary angiography was conducted for LAD or left main lesions using dedicated software (CAAS-5, Pie Medical, Maastricht, The Netherlands) to determine minimal lumen diameter, reference diameter, percent diameter stenosis (%DS), and lesion length. Lesions were categorized as focal (<28 mm), diffuse (≥28 mm) or tandem (two or more focal lesions separated by ≥10 mm of angiographically normal segment), and the severity of angiographic calcification was also categorized as non/mild, moderate or severe according to previous reports.8,9
Invasive coronary physiological assessments
Physiological measurements were performed based on clinical indications using a 0.014-inch pressure guidewire (Verrata or Verrata PLUS, Philips/Volcano, Amsterdam, the Netherlands; or PressureWire X, Abbott Vascular, Santa Clara, CA). After calibration and normalization at the guiding catheter tip, the wire was advanced distal to the lesion. We recorded NHPR (instantaneous wave-free ratio [iFR] or resting full-cycle ratio [RFR]) and FFR under resting and maximal hyperemic conditions, respectively.10,11 Hyperemia was induced by intravenous adenosine 5′-triphosphate (ATP, 180 μg/kg/min) or intracoronary nicorandil (2 mg). If a Philips/Volcano system was used before 2014 when iFR became commercially available, or if Abbott Vascular system was used before 2018 when RFR was clinically measurable, pressure data were sent to an external laboratory (Coroventis Research AB, Uppsala, Sweden) for offline NHPR calculation. 12 As described previously, RFR and iFR were considered equivalent. 13 A lesion was considered physiologically significant when either NHPR ≤0.89 or FFR ≤0.80.10,12
Coronary artery bypass grafting
CABG was performed using standard surgical techniques, either on-pump or off-pump, at the surgeon's discretion. The LAD was routinely grafted with the in-situ ITA. During surgery, graft flow parameters were assessed under stable hemodynamic conditions (systolic pressure ≈120 mmHg, heart rate 60–80 bpm) using a transit-time flow meter (TTFM; VeriQ System, Medistim, Oslo, Norway). Parameters included mean graft flow (MGF, mL/min), pulsatility index (PI = [max flow − min flow]/mean flow), diastolic filling percentage, and reverse flow (RF, retrograde flow ≥3% of total flow during systole). Intraoperative fluorescence imaging (IFI) was also performed using the Photodynamic Eye system (Hamamatsu Photonics K.K., Shizuoka, Japan) to visually confirm graft flow.
Coronary computed tomographic angiography
Postoperative graft patency was evaluated by CCTA at least three months after surgery, except in patients with chronic kidney disease (estimated glomerular filtration rate <45 mL/min/1.73 m2), contrast allergy, or lack of consent. Prior to imaging, patients received sublingual nitroglycerin (0.3 mg) and, when necessary, beta-blockers (metoprolol 20–40 mg orally, propranolol 2–4 mg intravenously, or landiolol 0.125 mg/kg intravenously) to maintain heart rate <60 bpm unless contraindicated. Scans were performed using ≥256-slice CT scanners. Images were reconstructed with 0.5-mm slice thickness using retrospective ECG-gating (temporal resolution 50–137 ms). Datasets were analyzed with dedicated workstations enabling 3D volume rendering and multiplanar reconstruction. Graft hypoperfusion was defined as total occlusion or diffuse narrowing consistent with a string sign.
Statistical analysis
Continuous data are presented as mean ± standard deviation or median (interquartile range), as appropriate, and compared using the Student's t-test or Wilcoxon rank-sum test. Categorical data are shown as frequencies and percentages and analyzed using Pearson's chi-square or Fisher's exact test. Differences among the three groups were assessed by the Kruskal–Wallis test. Receiver operating characteristic (ROC) curves were generated to assess the ability of NHPR and FFR to predict postoperative graft hypoperfusion and the area under the curve (AUC) values were compared using DeLong's method. Optimal cutoff values were determined using the Youden index. Statistical analyses were performed with JMP Pro version 18 (SAS Institute, Cary, NC, USA). Two-tailed p-values <.05 were considered statistically significant.
Results
Patients demographics
A total of 1289 patients underwent scheduled CABG with in-situ ITA–LAD bypass from August 2010 to April 2023 in our institute. Of the screened patients, 1161 patients did not undergo preoperative FFR or NHPR measurements of the LAD. Postoperative graft assessment using CCTA had not been performed for 23 patients due to chronic kidney disease or allergy to contrast. Therefore, 105 patients had complete data on preoperative invasive physiology, including both FFR and NHPR, and postoperative CCTA. Of those patients, 10 patients (9.5%) had hypoperfusion ITA grafts (graft failure; six patients, graft string; four patients), and 95 patients (90.5%) had the patent grafts (Supplemental Figure S1). The median duration between CABG and CCTA was 75 (46–139) days.
Baseline patient characteristics are shown in Table 1. There was no significant difference between the two groups except for age. In the hypoperfusion graft group, the age was younger than that of the patent graft group (66 ± 9.9 vs 71 ± 9.5, p < .01).
Patients characteristics.
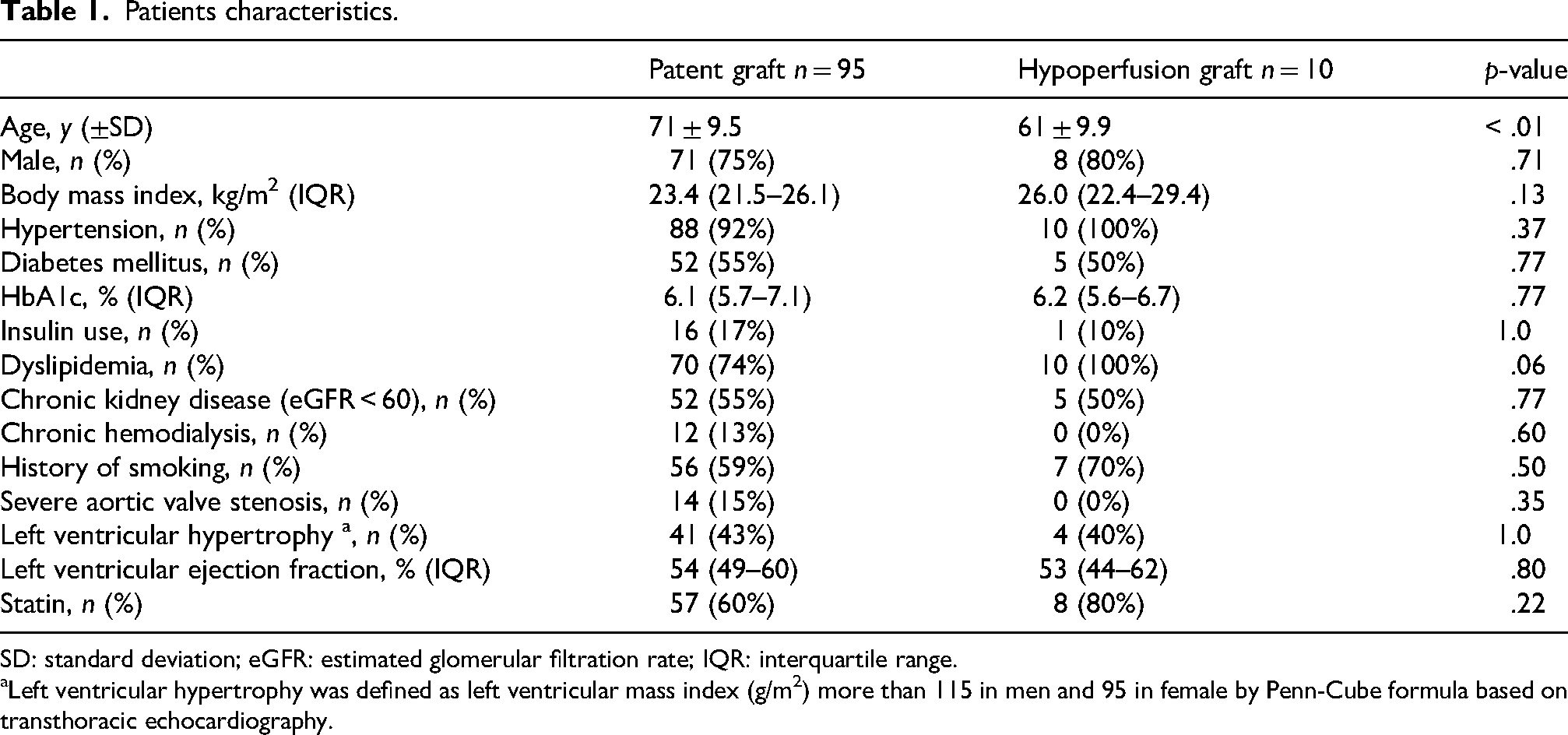
SD: standard deviation; eGFR: estimated glomerular filtration rate; IQR: interquartile range.
Left ventricular hypertrophy was defined as left ventricular mass index (g/m2) more than 115 in men and 95 in female by Penn-Cube formula based on transthoracic echocardiography.
Angiographic and invasive physiological findings
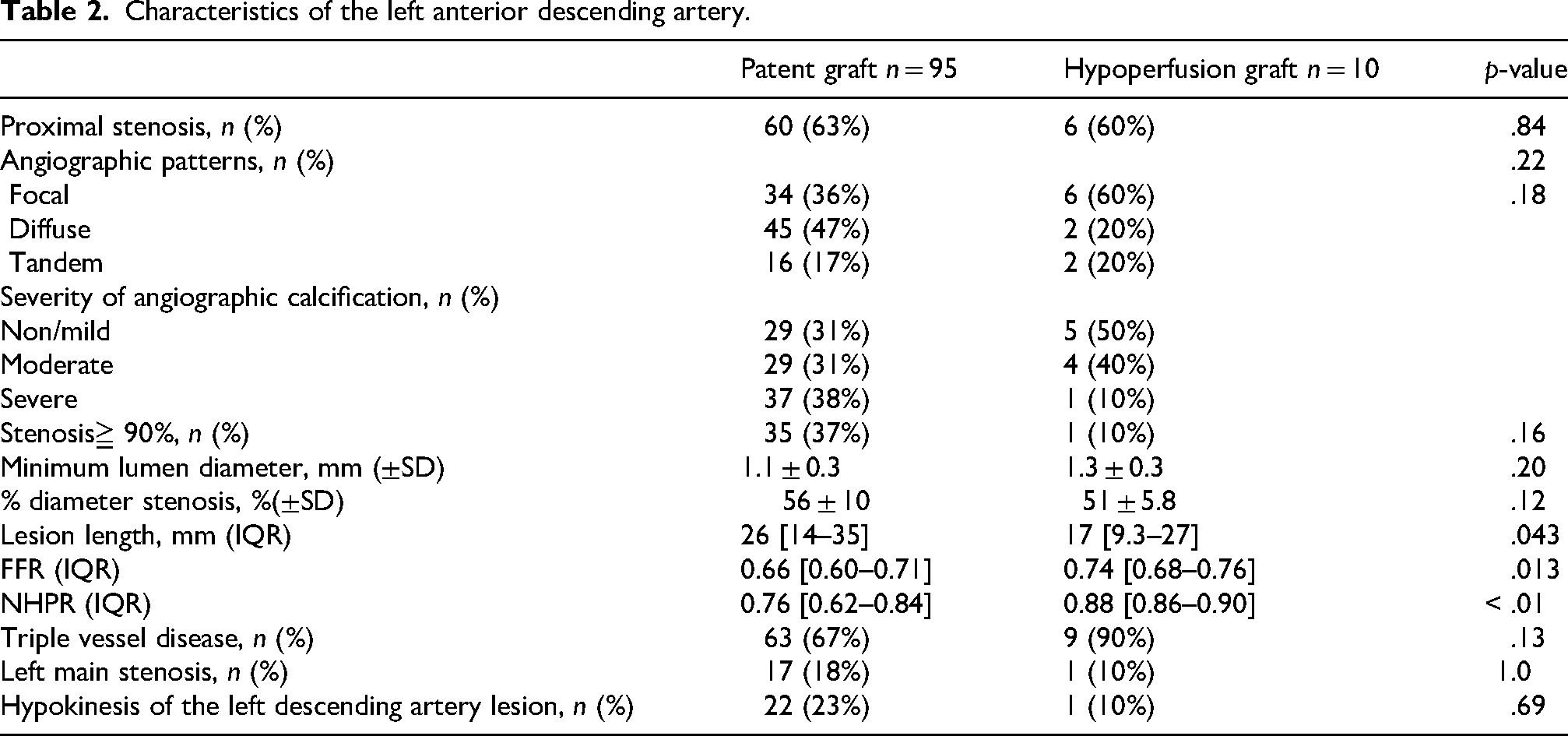
Angiographic and physiological characteristics of the LAD were summarized in Table 2. Lesion length was significantly shorter in the hypoperfusion graft group than in the patent group (17 mm vs 26 mm, p = .043), but other angiographic variables, including angiographic patterns and %DS, were similar between the two groups. In terms of the physiological variables, the hypoperfusion graft group had significantly higher NHPR (0.88 [0.86–0.90] vs 0.76 [0.62–0.84], p < .010) and higher FFR (0.74 [0.68–0.76] vs 0.66 [0.60–0.71], p = .013) than the patent graft group. The distribution of FFR and NHPR related to the graft hypoperfusion was shown in Supplemental Figure S2. The graft hypoperfusion occurred mostly in the vessels whose NHPR was more than 0.86.
Characteristics of the left anterior descending artery.
Intraoperative characteristics
Intraoperative characteristics, including MGF, PI, DF, and RF determined by TTFM, and operative characteristics were shown in Table 3. In the hypoperfusion graft group, MGF was significantly lower and RF was higher than those in the patent graft group. MGF increased significantly as NHPR values decreased, as shown in Figure 1. Other intraoperative characteristics were comparable between the two groups.
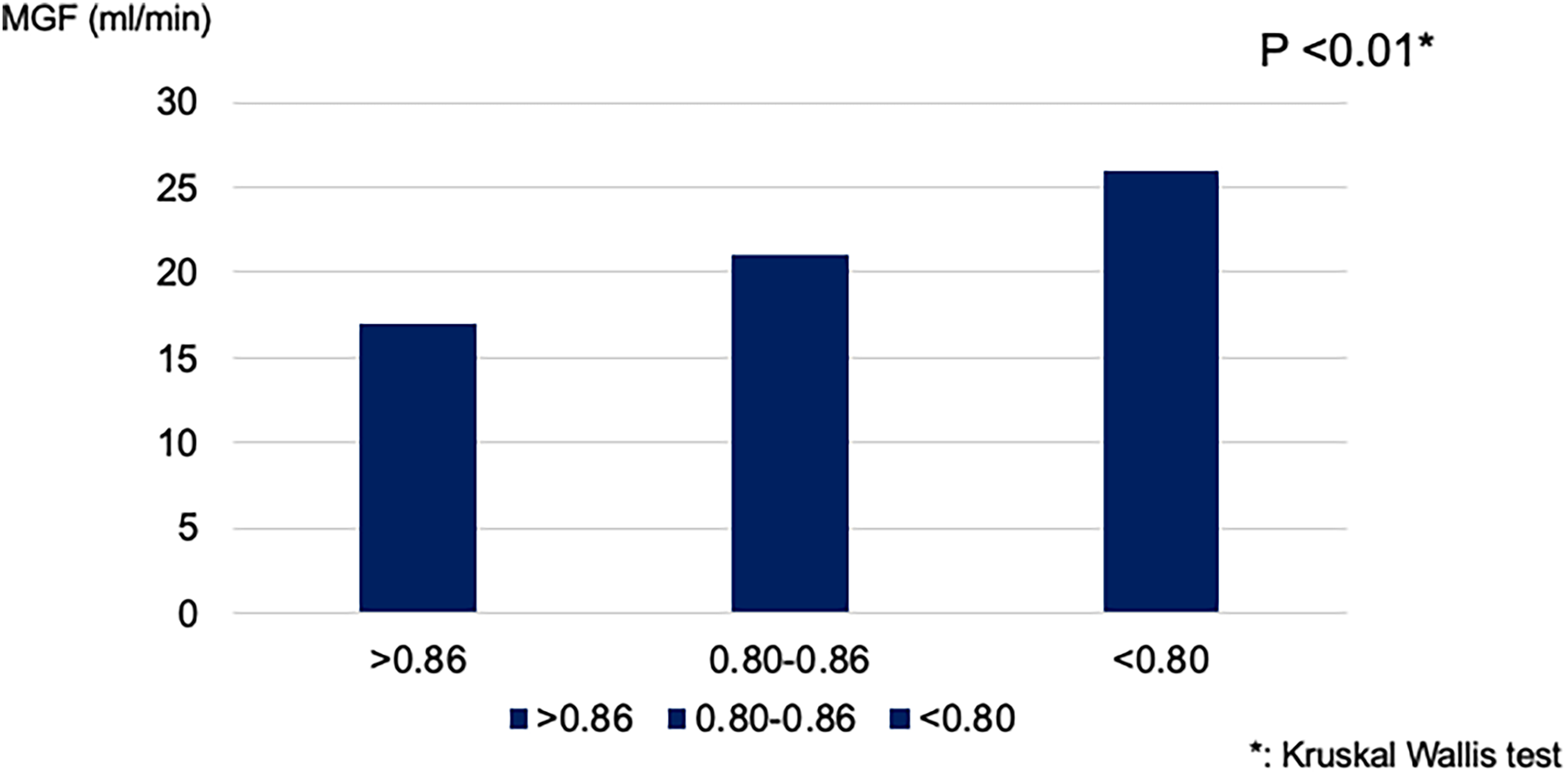
MGF increased significantly as NHPR values decreased. MGF: mean graft flow, NHPR: nonhyperemic pressure ratios.
Intraoperative characteristics.
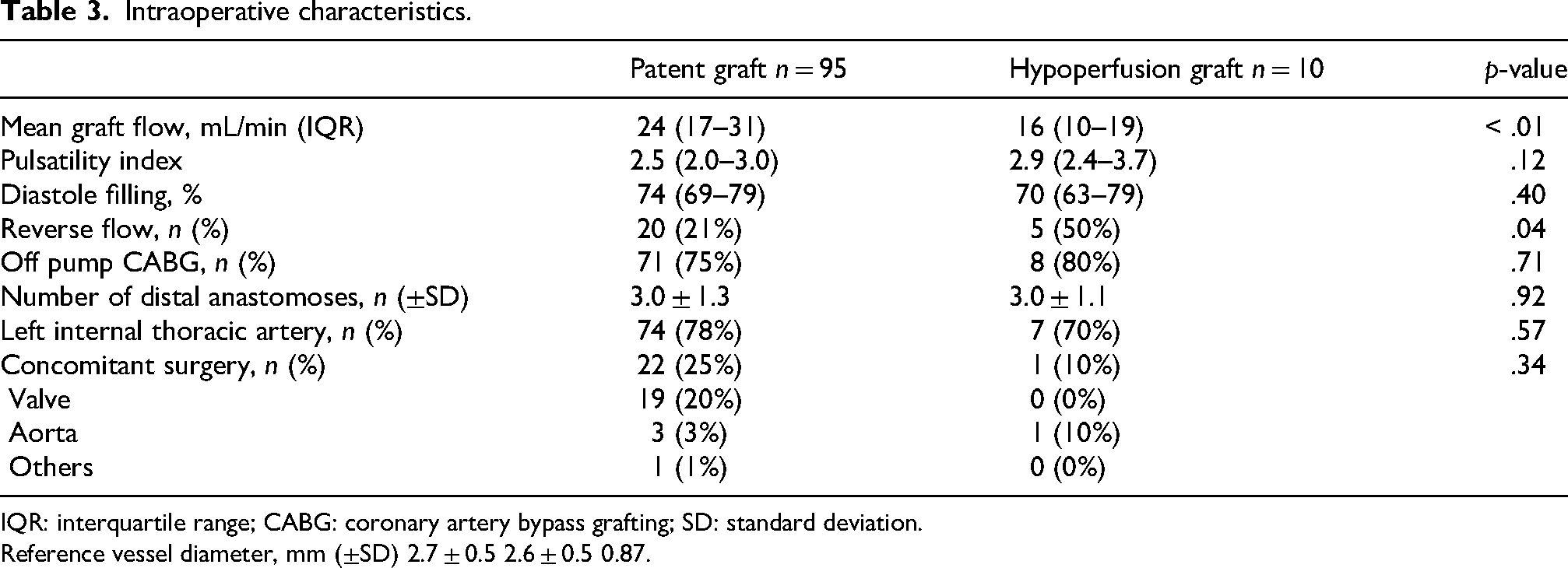
IQR: interquartile range; CABG: coronary artery bypass grafting; SD: standard deviation.
Reference vessel diameter, mm (±SD) 2.7 ± 0.5 2.6 ± 0.5 0.87.
Prediction of the hypoperfusion graft by NHPR and FFR
The ROC curve showed significantly larger AUC in NHPR as compared with FFR in terms of the prediction of the graft hypoperfusion (0.86 [0.60–0.96] vs 0.74 [0.55–0.87], p = .049) (Figure 2). The cutoff value of NHPR and FFR to predict the graft hypoperfusion was determined as 0.86 and 0.72 by an ROC analysis. The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy were 90%, 85%, 39%, 99%, and 86% for NHPR, and 70%, 76%, 23%, and 76% for FFR, respectively.
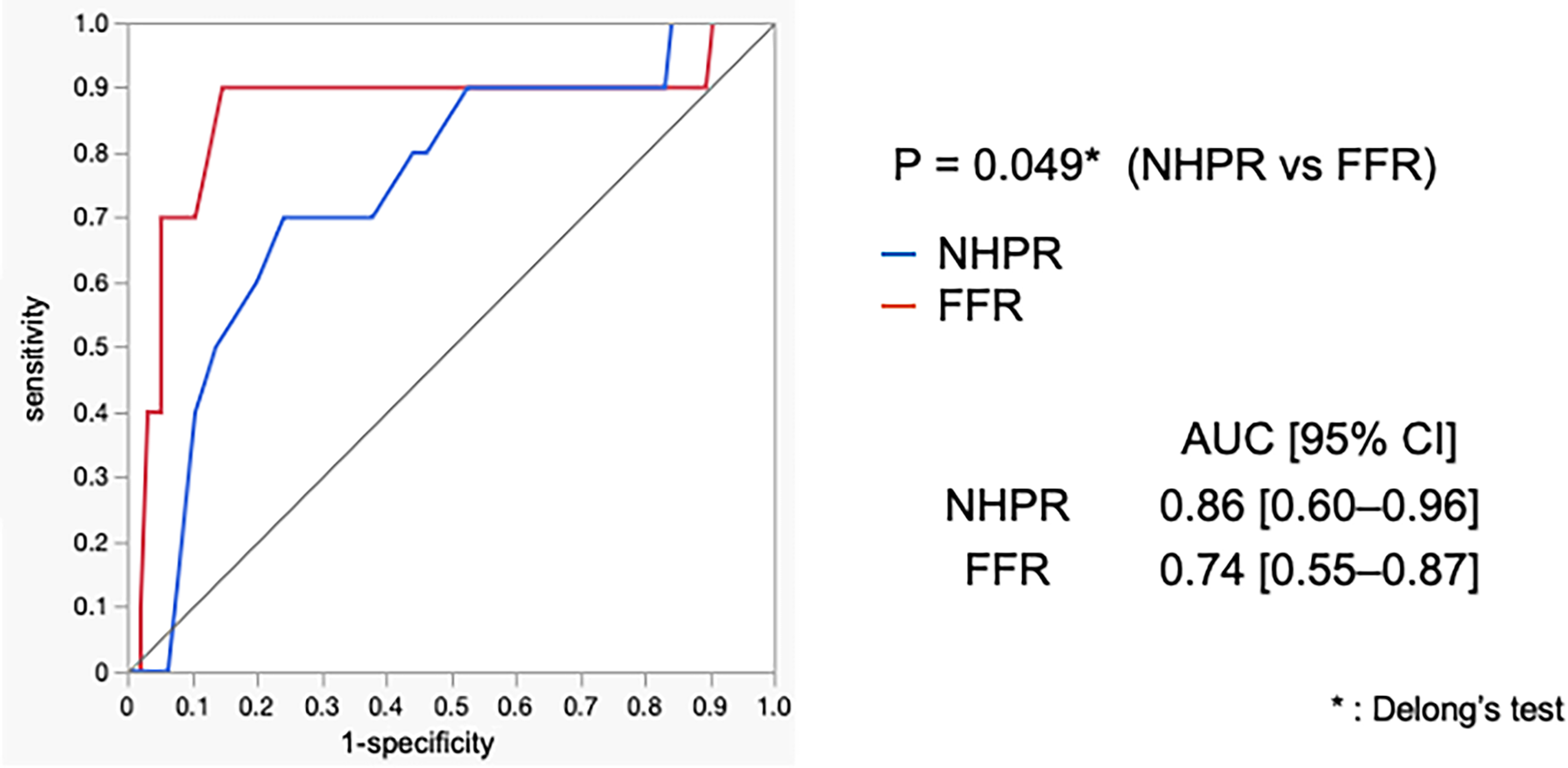
The receiver operating characteristics curve showed significantly larger area under the curve in NHPR as compared with FFR in terms of the prediction of the graft hypoperfusion (0.86 [0.60–0.96] vs 0.74 [0.55–0.87], p = .049). ROC: receiver operating characteristics, NHPR: nonhyperemic pressure ratios, FFR: fractional flow reserve, AUC: area under the curve.
Discussion
We evaluated the ability of FFR and NHPR to predict the graft hypoperfusion of in-situ ITA–LAD in patients undergoing CABG. The major findings of this study are summarized as follows: (1) patients with postoperative graft hypoperfusion had significantly lower degrees of stenosis in the LAD as preoperatively assessed with NHPR and FFR than those with patent grafts; (2) NHPR showed superior predictive ability for postoperative graft hypoperfusion compared with FFR.
Physiological severity and graft patency
The severity of native coronary artery lesions is thought to be associated with graft patency after CABG. Our study demonstrated that patients with a greater degree of coronary lesions in the LAD, as indicated by lower preoperative FFR and NHPR values, were more likely to have patent grafts, whereas those with higher values were more likely to experience graft hypoperfusion. These findings are consistent with previous studies reporting that the native coronary arteries with higher FFR values were more prone to competitive flow when bypass grafts were anastomosed, which hampered the adequate graft flow and could lead to graft hypoperfusion.2,14 As shown in the representative case in Figure 3 and Supplemental Video S1, TTFM revealed significantly low MGF and the presence of RF when the LITA was anastomosed on the LAD, showing FFR and NHPR values above the optimal cutoff values identified in this study (FFR: 0.72 and NHPR: 0.86). IFI also demonstrated slow ITA flow competing with LAD flow, and postoperative CCTA eventually showed a string sign of the ITA graft. These findings indicate that the functional degree of coronary stenosis in the native coronary artery is a key factor influencing graft patency.
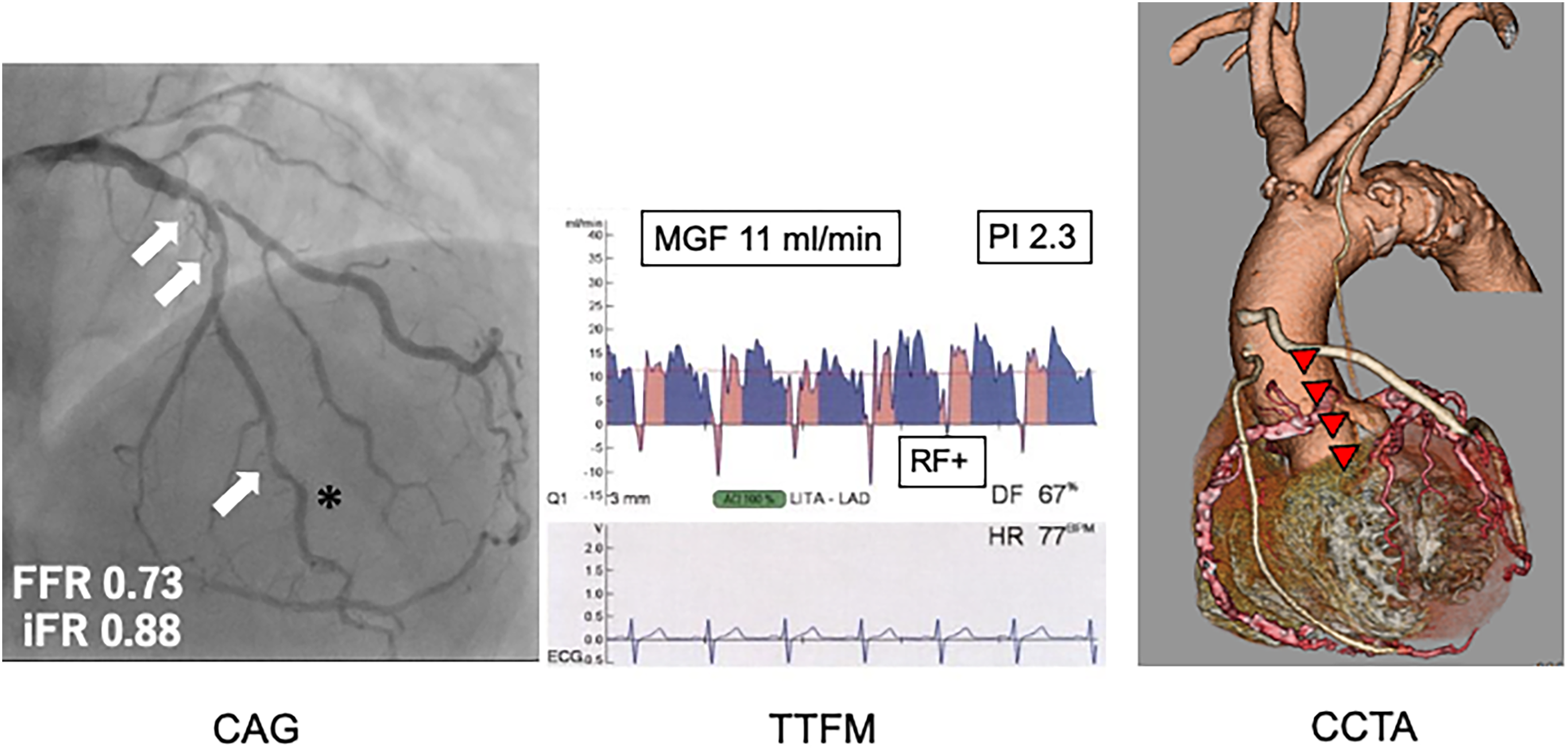
This 70-year-old male was a representative case of graft hypoperfusion (graft string) at postoperative CCTA. Preoperative coronary angiography showed the moderate tandem LAD stenosis with FFR 0.73 and iFR 0.88 at far distal of the LAD, which revealed functionally significant but not very severe stenosis. In-situ LITA-LAD (#8), SVG-DG-PL and SVG-4PD anastomoses were performed successfully. Intraoperative TTFM showed low mean graft flow and reversed flow, indicating competitive flow from the LAD, although there was no TTFM change after SVG-DG-PL bypass were performed. White arrow: stenosis lesions; *: anastomosed site; CCTA: coronary computed tomography angiography; LAD: left anterior descending artery; FFR: fractional flow reserve; iFR: instantaneous wave-free ratio; LITA: left internal thoracic artery; SVG: saphenous vein graft; DG: diagonal branch; PL: posterolateral branch; TTFM: transit time flow meter; CAG: coronary angiography.
While previous studies that investigated the association between preoperative physiological indices and graft hypoperfusion mainly focused on FFR,2,14–16 our research included NHPR. We found that both FFR and NHPR can predict graft hypoperfusion, but NHPR proved to be superior. Since patients are rarely in a maximally hyperemic state during daily life, it is reasonable to assume that the competitive flow seen in intraoperative TTFM and IFI, measured in nonhyperemic conditions, reflects the hemodynamics experienced most of their lives. Therefore, the better performance of NHPR in predicting graft hypoperfusion is a reasonable observation.
Differences in NHPR/FFR cutoff values for PCI and CABG
Previous studies have established the optimal cutoff values for physiological indices in percutaneous coronary intervention (PCI) as 0.80 for FFR and 0.89 for NHPR.17,18 In the present study, however, the optimal thresholds for predicting graft hypoperfusion in the in-situ ITA to LAD bypass differed from those used in PCI. Specifically, the cutoff values were 0.72 for FFR and 0.86 for NHPRs. From a surgical perspective, it should be noted that PCI and CABG are fundamentally different revascularization strategies. Coronary bypass surgery restores blood flow to the ischemic territory using a low-resistance conduit in parallel to the diseased coronary artery, while PCI directly dilates the flow-limiting stenoses and reduces the resistance of the diseased coronary artery. Because of these different approaches, it remains uncertain whether the same physiological thresholds established for PCI apply to CABG. In fact, the IMPAG trial showed a different cutoff value of FFR <0.78 for predicting arterial graft hypoperfusion. 15 In addition, the hemodynamics between the graft and the native coronary artery must differ between arterial and venous grafts. It is proposed that when FFR is <0.78, an arterial graft should be preferred, whereas when FFR is ≧0.78, a vein graft may be preferred as it is a low-resistance conduit compared with an arterial graft and can provide adequate flow even when anastomosed on a coronary artery with relatively low resistance. 16 However, the ability of FFR and NHPR to predict graft hypoperfusion of vein grafts remains unexplored.
How to prevent graft hypoperfusion
Since several studies have shown that graft failure is associated with worse clinical outcomes,1,19 strategies to reduce the risk of graft hypoperfusion remain crucial. Based on our findings that high preoperative NHPR values indicate a greater likelihood of graft hypoperfusion of the ITA-LAD graft, one strategy may involve intraoperative TTFM and IFI. It has been reported that when TTFM shows satisfactory MGF, PI, and absence of RF, and IFI confirms no flow competition, the graft can be left in place with confidence. 20 In such cases, the ITA-LAD can be anastomosed even if the LAD has FFR and NHPR values exceeding the thresholds. However, if intraoperative TTFM or IFI suggests potential flow competition, converting the in-situ ITA to an aorto-coronary configuration may be a reasonable option to increase graft flow and reduce flow competition with the native coronary artery. 16 Nevertheless, it has not yet been fully investigated whether these strategies can mitigate the risk of graft hypoperfusion. These would be subjects for future research.
Study limitations
This study has several limitations. It was conducted at a single center with a relatively small sample size, and the number of hypoperfusion events was limited. The follow-up period was confined to early postoperative assessment by coronary CTA, and long-term outcomes remain to be determined. Furthermore, our analysis focused exclusively on in-situ ITA–LAD grafts; extrapolation to other conduits or target vessels should be made with caution. Finally, although NHPR demonstrated better predictive value than FFR in this study, larger multicenter investigations are needed to confirm these findings.
Conclusions
In patients undergoing CABG with in-situ ITA–LAD, both FFR and NHPR were associated with postoperative graft patency, but NHPR showed superior predictive performance for identifying graft hypoperfusion. Incorporating NHPR into preoperative evaluation and intraoperative decision-making may assist surgeons in optimizing graft selection and configuration, ultimately contributing to improved graft patency and patient outcomes after CABG.
Supplemental Material
Footnotes
Acknowledgments
We acknowledge calculation of the iFR value from digitally stored pressure data by Dr Johan Svanerud.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Wakayama Medical University (No. 3539) on 21st June 2022, with the need for written informed consent waived.
Informed consent
Not applicable
Author contributions
Ryo Nakamura: data curation, formal analysis, investigation, methodology, project administration, and writing-original draft; Kentaro Honda: conceptualization, data curation, methodology, validation, and writing-review and editing; Yasutsugu Shiono: data curation, formal analysis, investigation, and writing-review and editing; Hidaki Kunimoto: data curation and investigation; Manabu Kashiwagi: data curation, conceptualization, and methodology; Teruaki Wada: data curation and investigation; Masahiro Takahata: data curation; Yuichi Ozaki: data curation; Yu Kajimoto: data curation; Mizuho Ikuchi: data curation; Kota Agematsu: supervision and validation; Atsushi Tanaka: supervision and validation; Yoshiharu Nishimura: supervision and validation.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Clinical trial registration
UMIN000059450.
Supplemental material
Supplemental material for this article is available online.