
Abstract
Scimitar syndrome is a rare congenital anomaly characterized by abnormal pulmonary venous drainage. This report describes the case of a 15-year-old girl with scimitar syndrome in which the scimitar vein drained into the hepatic vein. Surgical correction was successfully performed using an intra-atrial tunnel technique with right atrial anastomosis of the scimitar vein to reroute the scimitar vein to the left atrium. This case demonstrates the efficacy of this technique in managing complex cases of scimitar syndrome.
Introduction
Scimitar syndrome is a rare congenital anomaly featuring an abnormal right pulmonary vein, the scimitar vein (SV), which typically drains into the inferior vena cava (IVC).1,2 Hepatic vein drainage, which complicates surgical planning combined with cardiac rotation, occurs in the rarest cases. Herein, we report a hepatic-draining SV case of scimitar syndrome successfully treated using an intra-atrial tunnel technique.
Case report
An asymptomatic 15-year-old girl was admitted for surgery after a scimitar syndrome diagnosis. Chest X-ray showed a heart shifted to the right and a hyper dense area parallel to the right cardiac border, indicating SV. Transthoracic echocardiography revealed a mildly enlarged right atrium and right ventricle with an intact atrial septum and the SV draining into the hepatic vein. Computed tomography (CT) confirmed all right pulmonary veins entering the hepatic vein below the diaphragm (Figure 1), with the left atrium (LA) rotated posterolaterally. The shortest distance between the SV at the hepatic vein junction and the LA was measured at 5 cm on preoperative CT. Additionally, a pulmonary sequestration was identified in the right lower lobe, which was fed by systemic collateral arteries; therefore, transcatheter coil embolization of these collateral arteries was successfully performed prior to surgery. Cardiac catheterization demonstrated a mean pulmonary arterial pressure of 14 mmHg, Qp/Qs of 1.8, and Rp of 1.33 Unit/m2.
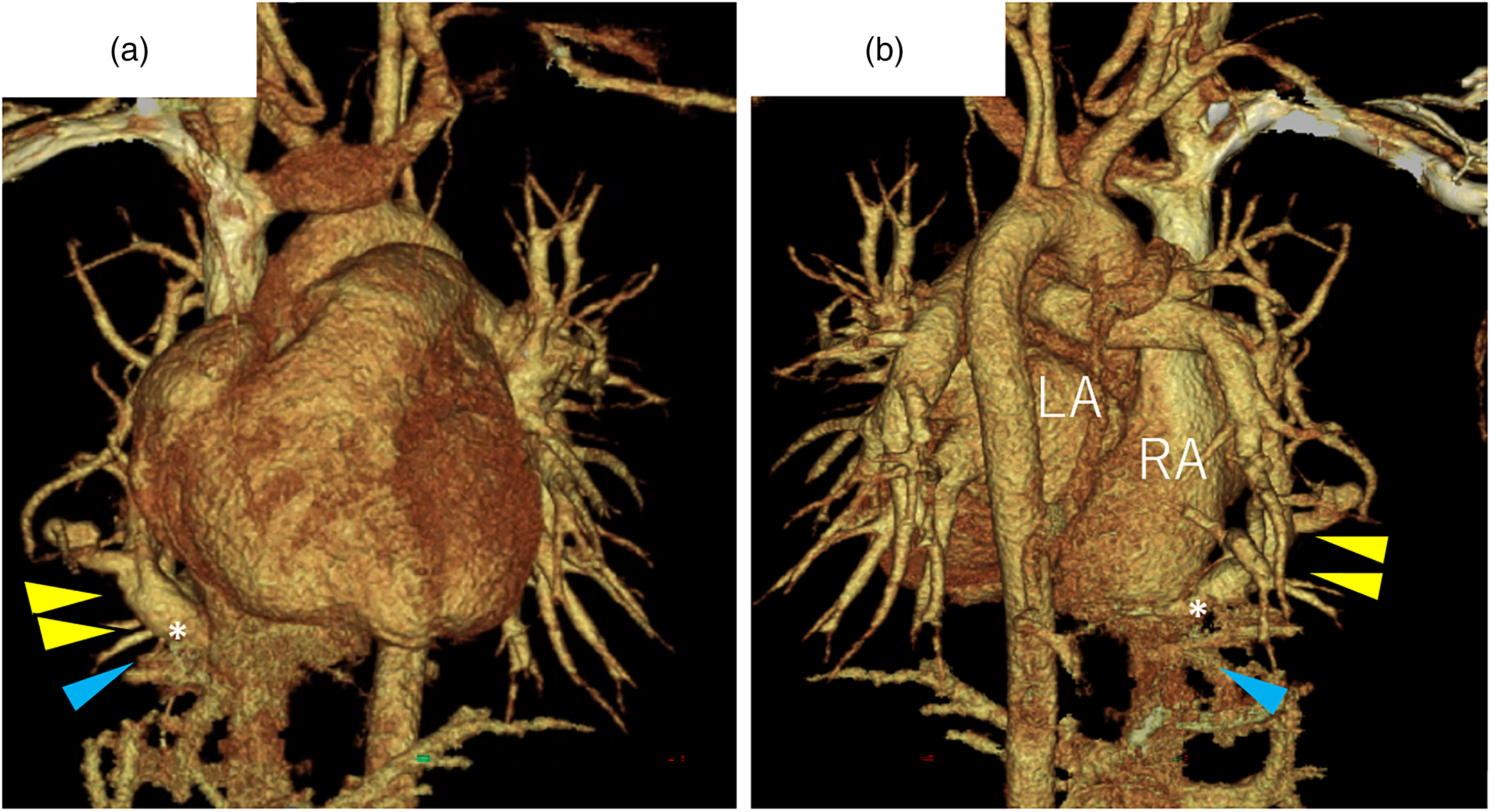
Preoperative, enhanced CT scans: (a, b) Preoperative CT showing all right pulmonary veins draining into the hepatic vein at the diaphragm level (yellow arrows), hepatic vein (blue arrow), and anomalous draining point (white asterisk). The left atrium appears small and displaced. LA = left atrium; RA = right atrium.
Through a median sternotomy, the right thoracic cavity was opened, revealing two large, converged SVs connected to the hepatic vein (Figure 2). Cardiopulmonary bypass was then initiated with ascending aortic and SVC cannulation, along with IVC cannulation approached via the right femoral vein. After thoroughly dissecting out the SV, it was divided from the hepatic vein at the junction and mobilized into the pericardium, passing beneath the phrenic nerve. The SV was anastomosed to a trapdoor incision on the posterolateral right atrial wall. Under cardioplegic arrest, a 20 mm atrial septal defect (ASD) was created. An intracardiac baffle using autologous pericardium treated with 0.6% glutaraldehyde for 3 min was sewn over the ASD and the SV anastomosis, rerouting the right pulmonary veins to the LA via the ASD. The post-operative course was uneventful. Postoperative CT showed no stenosis in the SV route or intra-atrial tunnel (Figure 3). The patient has been followed up for 1 year postoperatively, remaining entirely asymptomatic.
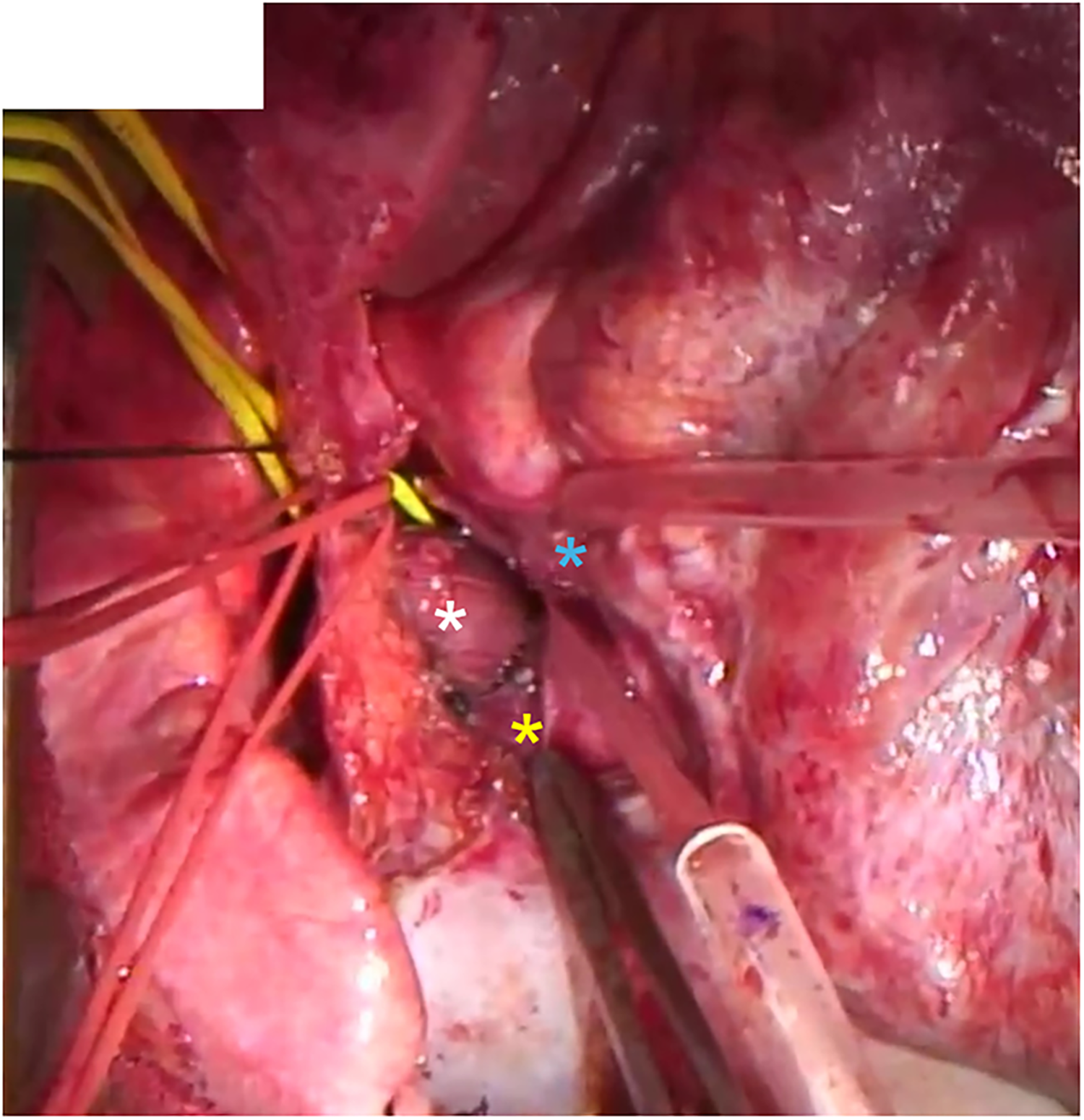
Surgical site images. The scimitar vein (white asterisk) draining into the hepatic vein (yellow asterisk) adjacent to the inferior vena cava (blue asterisk).
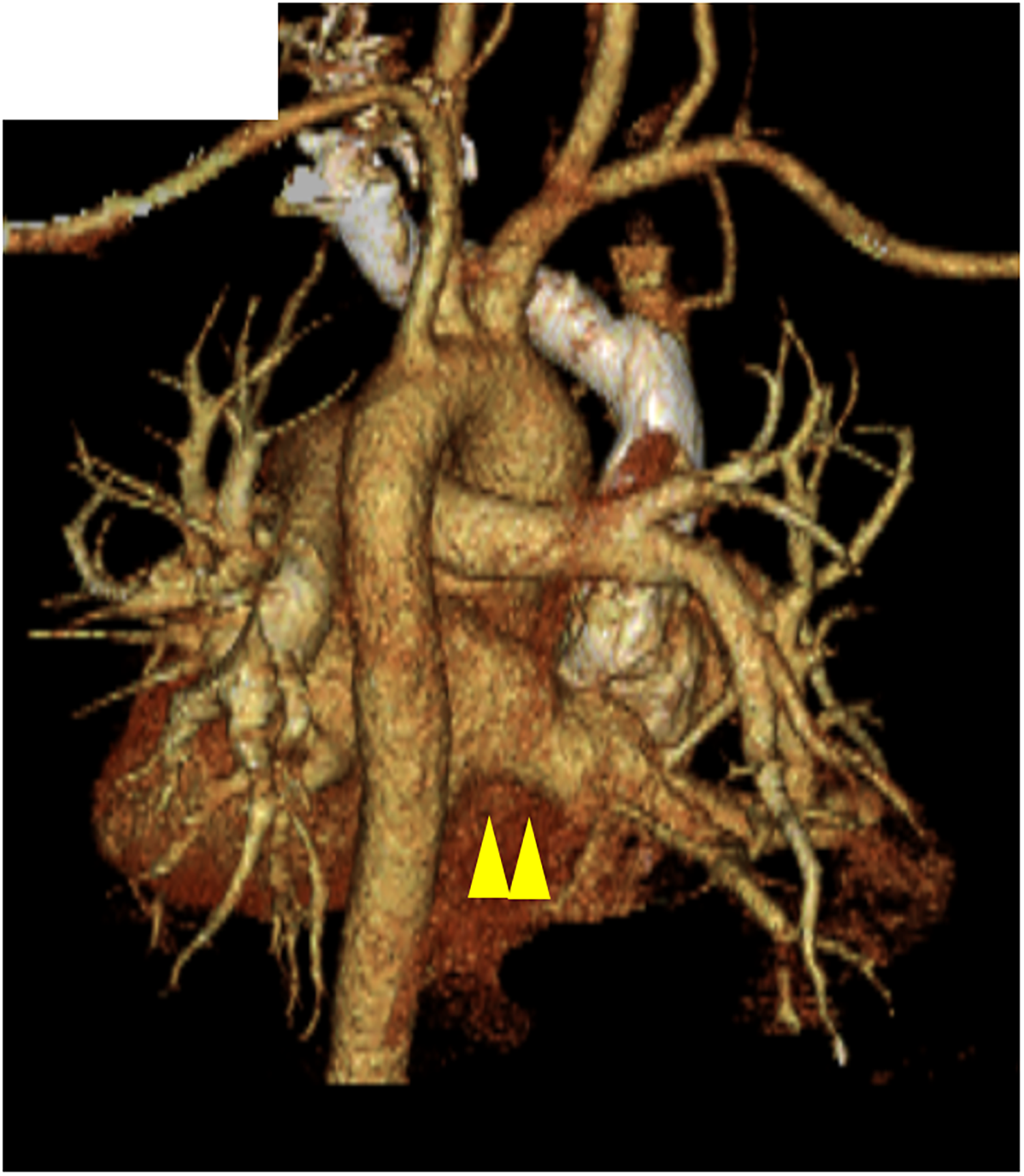
Postoperative, enhanced CT scans: postoperative CT scan showing no stenosis of the right pulmonary vein or intra-arterial tunnel (yellow arrows).
Comments
Scimitar syndrome comprises approximately 3–5% of all anomalous pulmonary venous return cases. 3 It is evidenced by reflux of the right pulmonary vein into the IVC, with extremely rare cases of influx into the hepatic vein. To our knowledge, only one other case of a hepatic-draining SV treated with a baffle procedure has been reported. 4
Multiple surgical approaches for scimitar syndrome have been described in the literature, including: traditional intra-atrial baffle repair; direct reimplantation of the SV into the LA; combined right atrial connection with intra-atrial baffle repair; and the modified Double-Decker technique utilizing exclusively autologous right atrial wall tissue to minimize postoperative obstruction risks.5,6 The optimal approach remains controversial, dictated largely by anatomical conditions and surgeon preference.1,7,8 Direct reimplantation is often preferred in younger patients as it avoids prosthetic materials. 7 However, it requires extensive mobilization and sufficient SV length to reach the LA without tension. Conversely, the intra-atrial tunnel repair is often chosen for adolescents and adults. It reduces anastomotic tension, albeit with a potential risk of tunnel obstruction. 9 In our patient, traditional intra-atrial baffle, direct LA anastomosis, and the modified Double-Decker technique were precluded by the significant distance between the hepatic-draining SV and the LA, further exacerbated by cardiac rotation. We successfully compensated for this by combining intra-atrial rerouting with a right atrial SV anastomosis, effectively bridging the gap and eliminating tension on the repair (Figure 4).
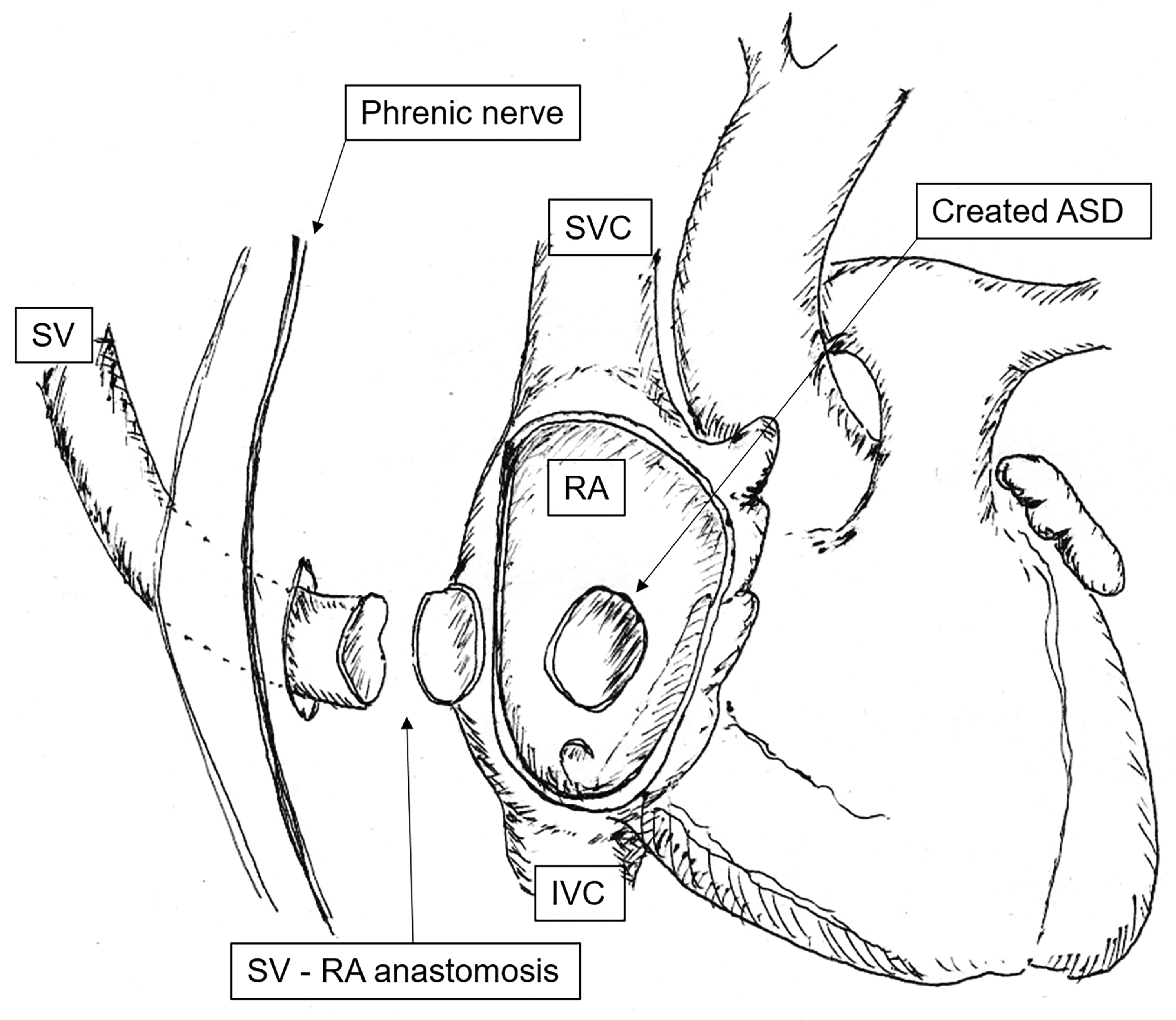
Surgical schema of the procedure: schematic illustration demonstrating the creation of the right atrial trap-door incision, direct anastomosis of the scimitar vein to the right atrium, and rerouting right pulmonary venous flow to the left atrium via the atrial septal defect. SV: scimitar vein; RA: right atrium; SVC: superior vena cava; IVC: inferior vena cava; ASD: atrial septal defect.
Baffle or anastomotic stenosis is widely recognized as the most clinically significant late complication following surgical repair of scimitar syndrome. 9 To monitor for this risk, regular postoperative transthoracic echocardiography and clinical evaluations were conducted. Should significant late stenosis or tunnel obstruction develop during longer follow-up, management strategies would involve transcatheter interventions, such as balloon angioplasty or stent placement, or surgical re-intervention depending on the anatomical severity.
Conclusion
This case demonstrates the successful surgical management of a rare hepatic-draining scimitar syndrome. The intra-atrial tunnel technique with right atrial anastomosis of SV effectively addressed the SV-LA gap, avoiding tension at the anastomotic site and minimizing complications. This approach highlights the importance of individualized surgical strategies to achieve favorable outcomes in complex cases of scimitar syndrome.
Footnotes
Ethical approval
This study was approved by the institutional review boards of the University of Tsukuba (R04-065).
Informed consent
Consent for publication was obtained from the patient and family.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.