
Abstract
Background
This study determined the incidence of major adverse cardiovascular events and identified independent predictors of in-hospital mortality in patients with acute limb ischemia undergoing revascularization.
Methods
A retrospective cohort study was conducted on 240 consecutive patients with acute limb ischemia who underwent revascularization at a tertiary-care academic hospital between February 2014 and February 2022. Perioperative adverse events were recorded, and multivariable logistic regression was used to identify independent predictors of in-hospital mortality.
Results
In-hospital major adverse cardiovascular events occurred in 42 patients (17.5%), while cardiovascular death accounted for 1.7%. All-cause in-hospital mortality was 13.3% (32 patients). On univariable analysis, markers of physiological stress including leukocytosis and elevated neutrophil-to-lymphocyte ratio, renal dysfunction, and multiple postoperative complications were significantly associated with mortality. Multivariable analysis identified four independent predictors: preoperative leukocytosis with white blood cell count greater than 15,000 per microliter (adjusted odds ratio 4.05, 95% confidence interval 1.52–10.75), intraoperative vasopressor use (adjusted odds ratio 4.00, 95% confidence interval 1.48–10.83), postoperative respiratory failure (adjusted odds ratio 8.44, 95% confidence interval 3.20–22.27), and postoperative bowel ischemia (adjusted odds ratio 15.24, 95% confidence interval 2.40–96.90).
Conclusions
Major adverse cardiovascular events are frequent but not independently associated with in-hospital mortality in patients with acute limb ischemia undergoing revascularization. Mortality is determined by a cascade of perioperative systemic insults rather than isolated cardiovascular events. Postoperative surveillance should prioritize early recognition of respiratory failure and bowel ischemia, particularly in patients presenting with leukocytosis or requiring intraoperative vasopressor support.
Introduction
Acute limb ischemia (ALI) is a vascular emergency that can lead to limb loss or death without appropriate treatment. Although in-hospital mortality decreased from 12% in 1998 to 9% in 2009, the 1-year mortality rate remains high at 40% 1 since patients with ALI often have preexisting vascular risk factors, which requires early recognition and prompt diagnosis for immediate therapeutic action.
Rutherford's classification guides assessment of ALI severity, prognosis, and treatment strategy. Stage 3 ALI represents irreversible limb ischemia with permanent tissue damage, for which amputation is required due to its unsuitability for revascularization. In all other stages, timely revascularization is crucial for ALI treatment. 2 Revascularization can be achieved through surgical or endovascular approaches, each carrying distinct perioperative implications. Surgical options include thromboembolectomy and bypass, while endovascular strategies encompass catheter-directed thrombolysis and percutaneous mechanical thrombectomy. Although current evidence cannot definitively establish the superiority of one approach over the other, they are considered complementary rather than competing strategies.2,3
The urgent nature of ALI limits the ability to conduct thorough cardiovascular assessments in these high-risk patients. In addition to vascular imaging, a detailed medical history and physical examination are imperative. Perioperative biomarkers may help estimate the extent of ischemia, although their utility in guiding treatment remains uncertain. 2 Effective pain control and fluid management are crucial, with careful monitoring for hyperkalemia and other metabolic disturbances. While surgeons typically drive treatment decisions, collaborative decision-making between surgeons and anesthesiologists is essential to ensure awareness of perioperative risks.
Patients with ALI often have concurrent cardiovascular disease, placing them at high risk for major adverse cardiovascular events (MACE). Previous studies have reported perioperative MACE rates ranging from 6.3% 4 to 29% 5 following revascularization for ALI; yet the relationship between MACE and in-hospital mortality in ALI patients remains inadequately characterized, especially in the context of modern revascularization techniques and contemporary perioperative care.
Given this knowledge gap, this study aimed to determine the incidence of MACE and to identify factors associated with in-hospital mortality among patients with ALI undergoing revascularization. We hypothesized that MACE would be a significant predictor of mortality, and sought to quantify its contribution relative to other perioperative complications. The findings may help improve clinical awareness and inform decision-making regarding postoperative monitoring and intensive care unit (ICU) admission.
Materials and methods
Study design
This single-institution retrospective chart review analyzed a database of adult patients (≥18 years old) diagnosed with ALI who underwent revascularization at a tertiary-care academic hospital in Thailand from February 2014 to February 2022. The study protocol was reviewed by the Institutional Review Board of the authors’ institution and deemed exempt from full review because it involved secondary analysis of de-identified data. All patients provided routine clinical consent for treatment. The study adhered to the Declaration of Helsinki and institutional data-protection policies.
Cases were identified from inpatient electronic medical records using ICD-10 code I74.3 (embolism and thrombosis of arteries of the lower extremities). A total of 240 consecutive patients were enrolled.
Patient selection
The inclusion criteria encompassed adult patients diagnosed with ALI who underwent surgical, endovascular, or hybrid revascularization, or catheter-directed thrombolysis. This study defined ALI as a sudden reduction in unilateral or bilateral lower limb perfusion threatening limb viability due to arterial thromboembolism, in situ thrombosis of native vessels, or thrombosis of a previous bypass graft or stent. Consistent with prior literature, we included patients with symptom onset within 2 weeks before presentation. Patients who did not undergo revascularization, those treated with medical revascularization only, or those with inadequate data were excluded. The severity of ALI was assessed using the Rutherford classification.
Preoperative data
Collected variables included demographic information, comorbidities, and ALI-related clinical data. The demographic data comprised age, sex, and physical status according to the classification of the American Society of Anesthesiologists. The comorbidities included hypertension, dyslipidemia, chronic kidney disease (CKD), diabetes mellitus, atrial fibrillation, coronary artery disease, cerebrovascular disease, a prior diagnosis of critical limb ischemia the patients’ smoking status. ALI-related variables included etiology (embolism or thrombosis), location, and Rutherford classification severity. Procedural variables included the type of revascularization, anesthetic technique, and procedural success parameters. Technical success was defined as residual thrombus less than 30% diameter stenosis with adequate contrast flow to the foot on completion angiography. Completeness of thrombus removal and the need for additional revascularization procedures were also recorded.
Follow-up and outcomes
Primary outcome: The primary outcome was the incidence of in-hospital MACE, defined as a composite of myocardial infarction, ischemic stroke and cardiovascular death. 6
Secondary outcomes: Secondary outcomes included all-cause mortality, resuscitated cardiac arrest (cardiac arrest with return of spontaneous circulation, ROSC) and other in-hospital adverse events, including the following.
Preoperative adverse events included new-onset arrhythmia, hypotension necessitating vasopressors, and markers of physiologic stress (leukocytosis, elevated neutrophil-to-lymphocyte ratio (NLR), and marked tachycardia [heart rate >115 beats per minute]). Intraoperative adverse events included new-onset arrhythmia, hypotension requiring vasopressors, oliguria (urine output <0.3 ml/kg/h), intraoperative hemodialysis, intraoperative rhabdomyolysis, and major bleeding. Postoperative adverse events included new-onset arrhythmia, renal failure, respiratory failure, sepsis, major bleeding, rhabdomyolysis, compartment syndrome, fasciotomy, reoperation (including thromboembolectomy, angioplasty, and amputation), and bowel ischemia.
Major bleeding was defined as overt bleeding with a hemoglobin (Hb) drop of ≥3 g/dL, blood transfusion in patients with pre-procedure Hb >8 g/dL, symptomatic bleeding in a critical location, or fatal bleeding.
Sepsis was defined as clinically diagnosed by the treating physician and documented in the medical record. Given that the study period spanned 2014 to 2022, diagnostic criteria applied by clinicians may have evolved from SIRS-based frameworks toward the Sepsis-3 definition during this interval; formal retrospective reclassification was not performed, and this variability is acknowledged as a limitation.
Postoperative respiratory failure was defined as a clinician-assigned diagnosis documented in the medical record, based on the presence of arterial hypoxemia (PaO2 < 60 mmHg or SpO2 < 90%), hypercapnia (PaCO2 > 45 mmHg with pH <7.35), prolonged mechanical ventilation (>48 hours), unplanned reintubation, or initiation of noninvasive ventilation for acute respiratory compromise. 7
Statistical analysis
Based on an expected MACE incidence of 6.3%from a previous study, 4 a minimum sample size of 222 was calculated. Continuous variables are presented as mean ± standard deviation or median (interquartile range) as appropriate, and were compared using the independent samples t-test or Mann–Whitney U test. Categorical variables are presented as frequencies and percentages and were compared using the Chi-squared test or Fisher's exact test where cell counts were small. Variables with p < 0.05 on univariable logistic regression were considered candidates for multivariable analysis. A parsimonious multivariable model was constructed using backward stepwise logistic regression (removal criterion p > 0.10) to minimize the risk of overfitting. Results are expressed as adjusted odds ratios (aORs) with 95% confidence intervals (CIs). A two-tailed p-value <0.05 was considered statistically significant for all analyses. All analyses were performed using PASW Statistics version 31 (IBM Corp., Armonk, NY, USA).
Results
Patient demographics and clinical characteristics
The demographic data is summarized in Table 1. The mean patient age was 65.3 ± 17.5 years, with 125 men (52.1%) and 115 women (47.9%). Hypertension was the most prevalent underlying disease (158 patients, 65.8%), followed by current smoking status (157 patients, 65.4%), dyslipidemia (90 patients, 37.5%), and atrial fibrillation (86 patients, 35.8%).
Baseline patient characteristics stratified by in-hospital mortality (N = 240).
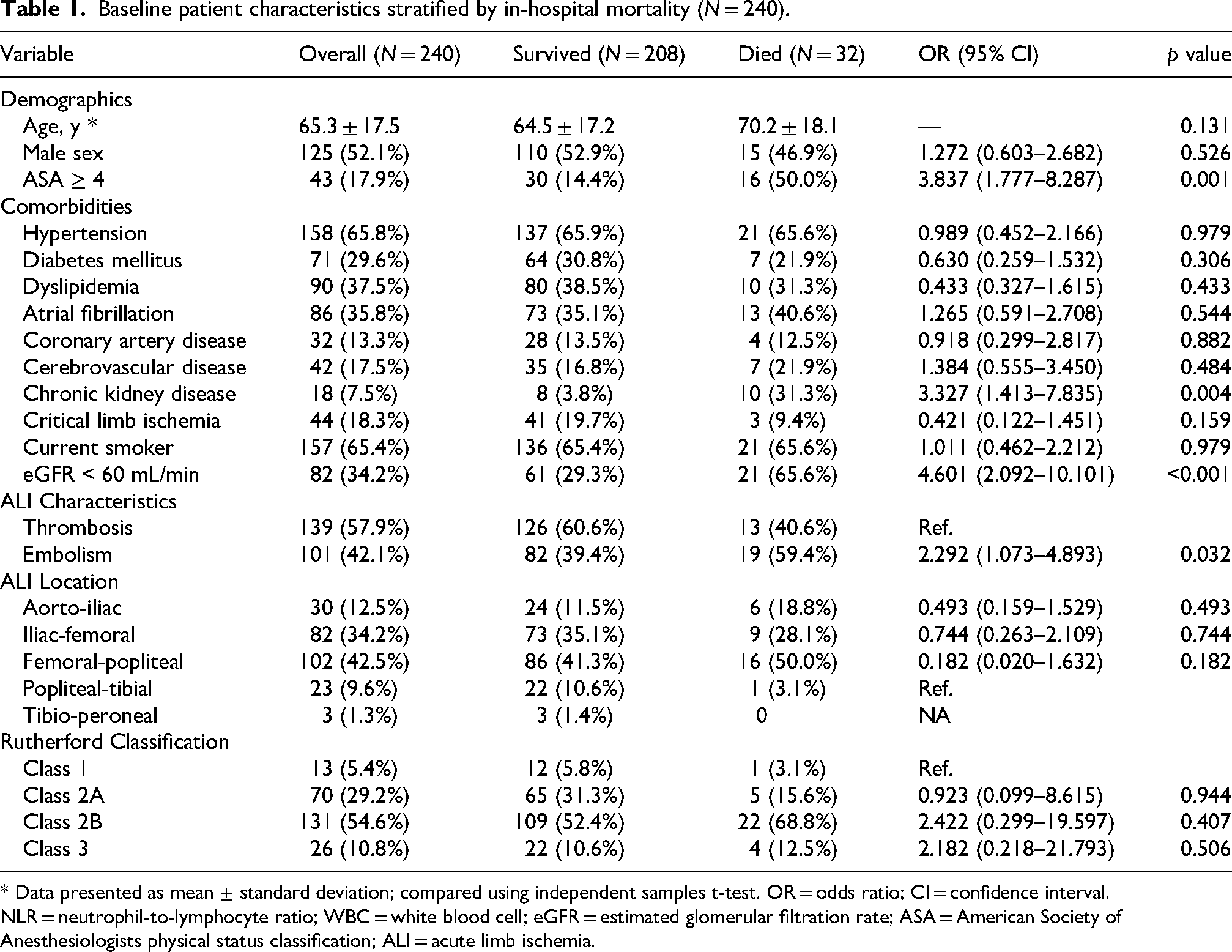
* Data presented as mean ± standard deviation; compared using independent samples t-test. OR = odds ratio; CI = confidence interval. NLR = neutrophil-to-lymphocyte ratio; WBC = white blood cell; eGFR = estimated glomerular filtration rate; ASA = American Society of Anesthesiologists physical status classification; ALI = acute limb ischemia.
Etiology and lesion location
Thrombosis was the most frequent etiology of ALI (139 patients, 57.9%), followed by embolism (101 patients, 42.1%). The femoral-popliteal artery was the most common lesion location (102 patients, 42.5%), followed by the iliac-femoral region (82 patients, 34.2%). Rutherford category 2B was the most prevalent severity grade (131 patients, 54.6%).
Revascularization procedures and anesthetic techniques
Hybrid revascularization was the most performed procedure (109 patients, 45.4%; Table 2). Technical success was achieved in 223 patients (92.9%). General anesthesia was predominant (172 patients, 71.7%), followed by monitored anesthesia care (54 patients, 22.5%).
Procedural details and intraoperative characteristics (N = 240).
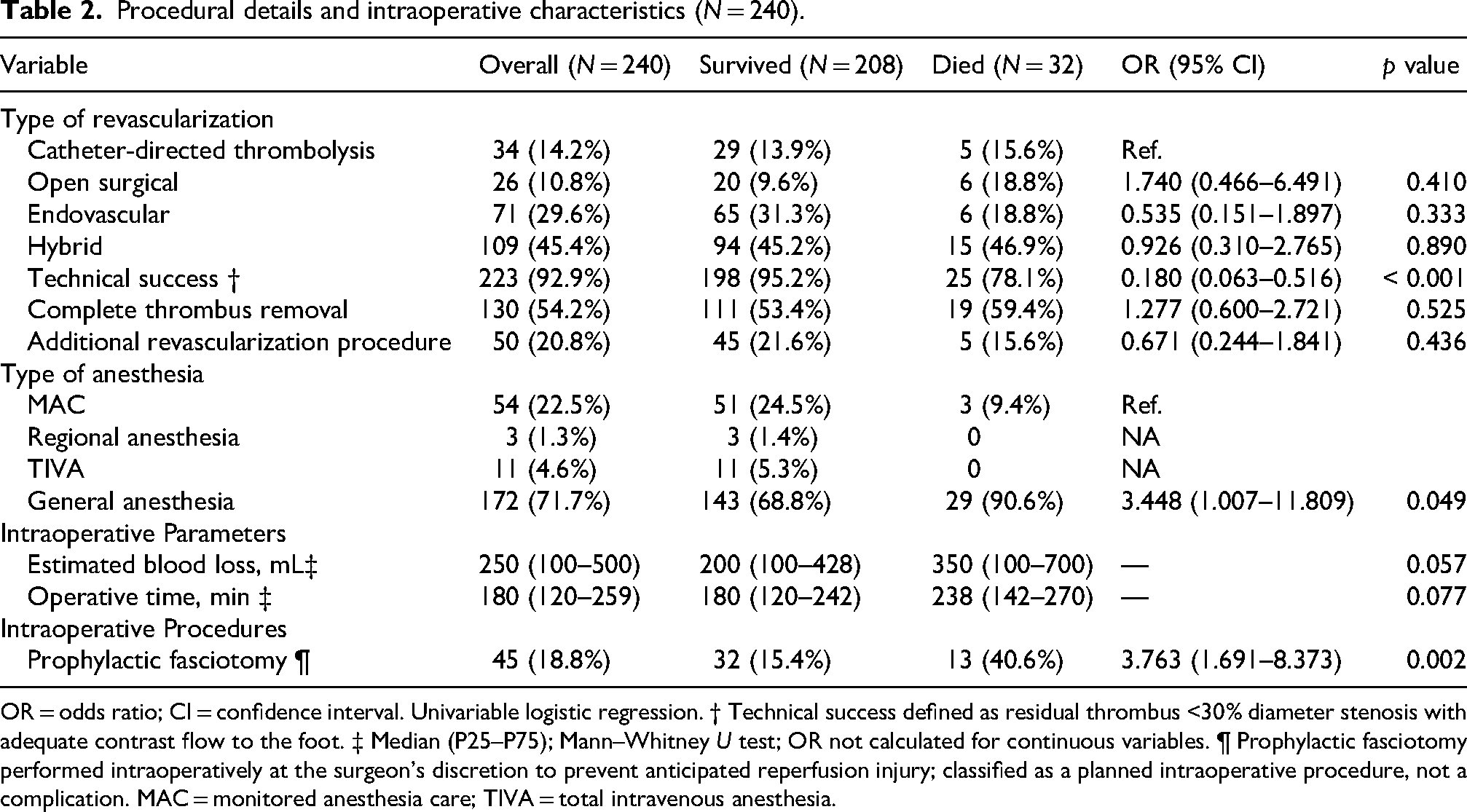
OR = odds ratio; CI = confidence interval. Univariable logistic regression. † Technical success defined as residual thrombus <30% diameter stenosis with adequate contrast flow to the foot. ‡ Median (P25–P75); Mann–Whitney U test; OR not calculated for continuous variables. ¶ Prophylactic fasciotomy performed intraoperatively at the surgeon's discretion to prevent anticipated reperfusion injury; classified as a planned intraoperative procedure, not a complication. MAC = monitored anesthesia care; TIVA = total intravenous anesthesia.
Adverse events
Adverse events were recorded across the preoperative, intraoperative, and postoperative phases. The primary outcome, MACE, occurred in 42/240 patients (17.5%). By phase, 22 patients (9.2%) experienced a preoperative event, five patients (2.1%) an intraoperative event, and 21 patients (8.8%) a postoperative MACE event. These counts are not mutually exclusive because some patients experienced events in more than one phase. MACE comprised myocardial infarction, ischemic stroke and cardiovascular death; component-specific incidence is reported in Figure 1. All-cause in-hospital mortality occurred in 32 patients (13.3%).
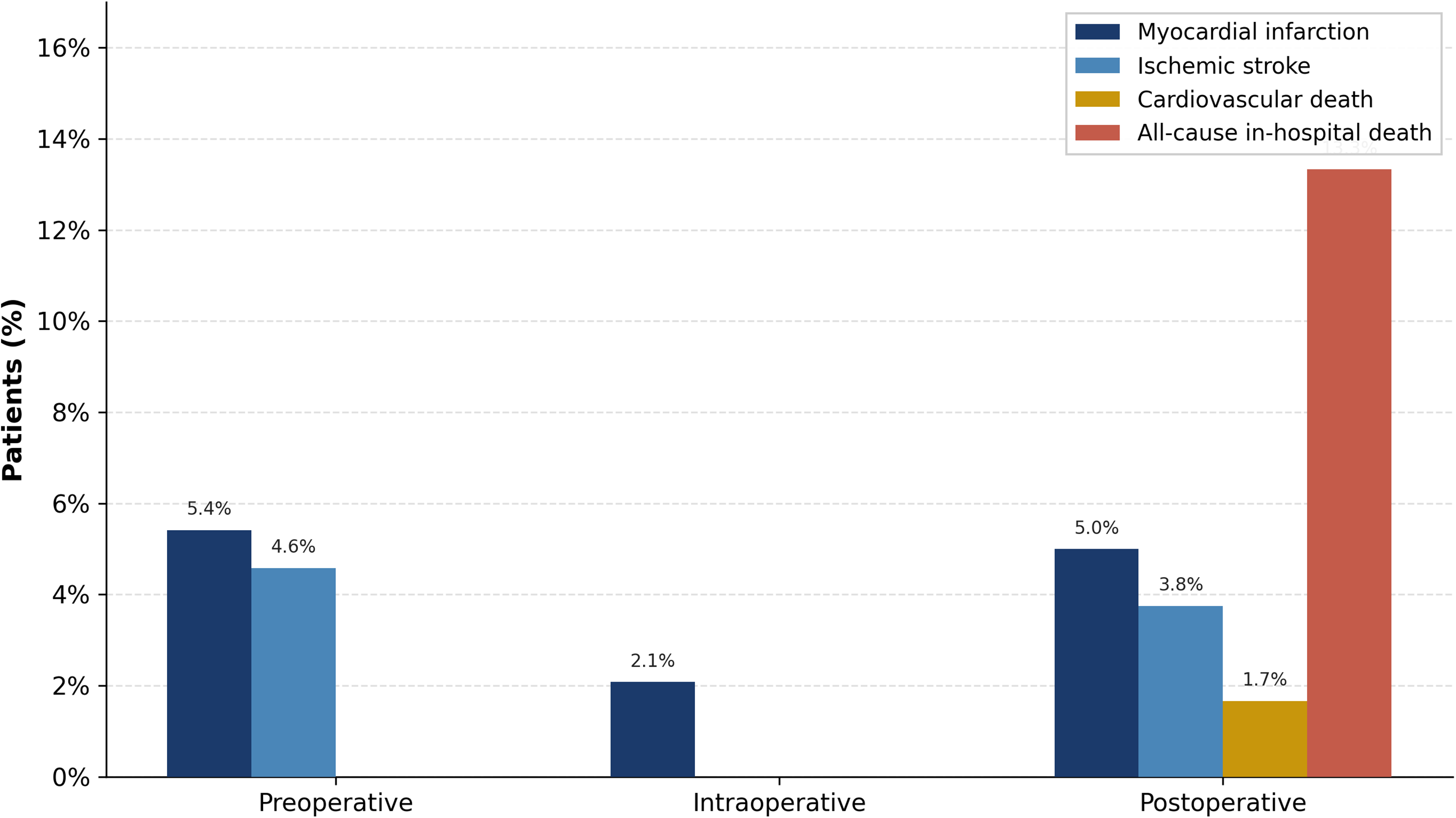
Incidence of major adverse cardiovascular events (MACE) components and all-cause in-hospital death by perioperative phase (N = 240). Bars represent the percentage of patients experiencing each event during the preoperative, intraoperative, and postoperative periods. Navy bars = myocardial infarction; steel blue bars = ischemic stroke; amber bars = cardiovascular death; coral bars = all-cause in-hospital death. MACE was defined as the composite of myocardial infarction, ischemic stroke, and cardiovascular death. All-cause death (13.3%) substantially exceeded cardiovascular death (1.7%) in the postoperative period, indicating that mortality was predominantly driven by non-cardiovascular causes.
Factors associated with in-hospital mortality
Bivariate analysis identified several factors significantly associated with in-hospital mortality (Tables 1–3). Regarding baseline characteristics, the mortality group had a higher prevalence of ASA ≥4 (50%, p = 0.001), CKD (31.3%, p = 0.004), leukocytosis (white blood cell [WBC] >15,000/µL; 62.5%, p < 0.001), and elevated NLR >5 (87.5%, p < 0.001). Embolism was more frequent among non-survivors (59.4%, p = 0.032). Procedurally, technical success was significantly less frequent in the mortality group (78.1% vs. 95.2%; OR 0.180, 95% CI 0.063–0.516; p < 0.001). Preoperative tachycardia (HR >115 bpm; 37.5%, p < 0.001), intraoperative vasopressor use (68.8%, p < 0.001) and oliguria (21.9%, p < 0.001), and postoperative respiratory failure (71.9%, p < 0.001), sepsis (40.6%, p < 0.001), acute kidney injury (68.8%, p < 0.001), bowel ischemia (25.0%, p < 0.001), and rhabdomyolysis (31.3%, p = 0.001) were all significantly more frequent among non-survivors.
Perioperative adverse events and postoperative complications (N = 240).
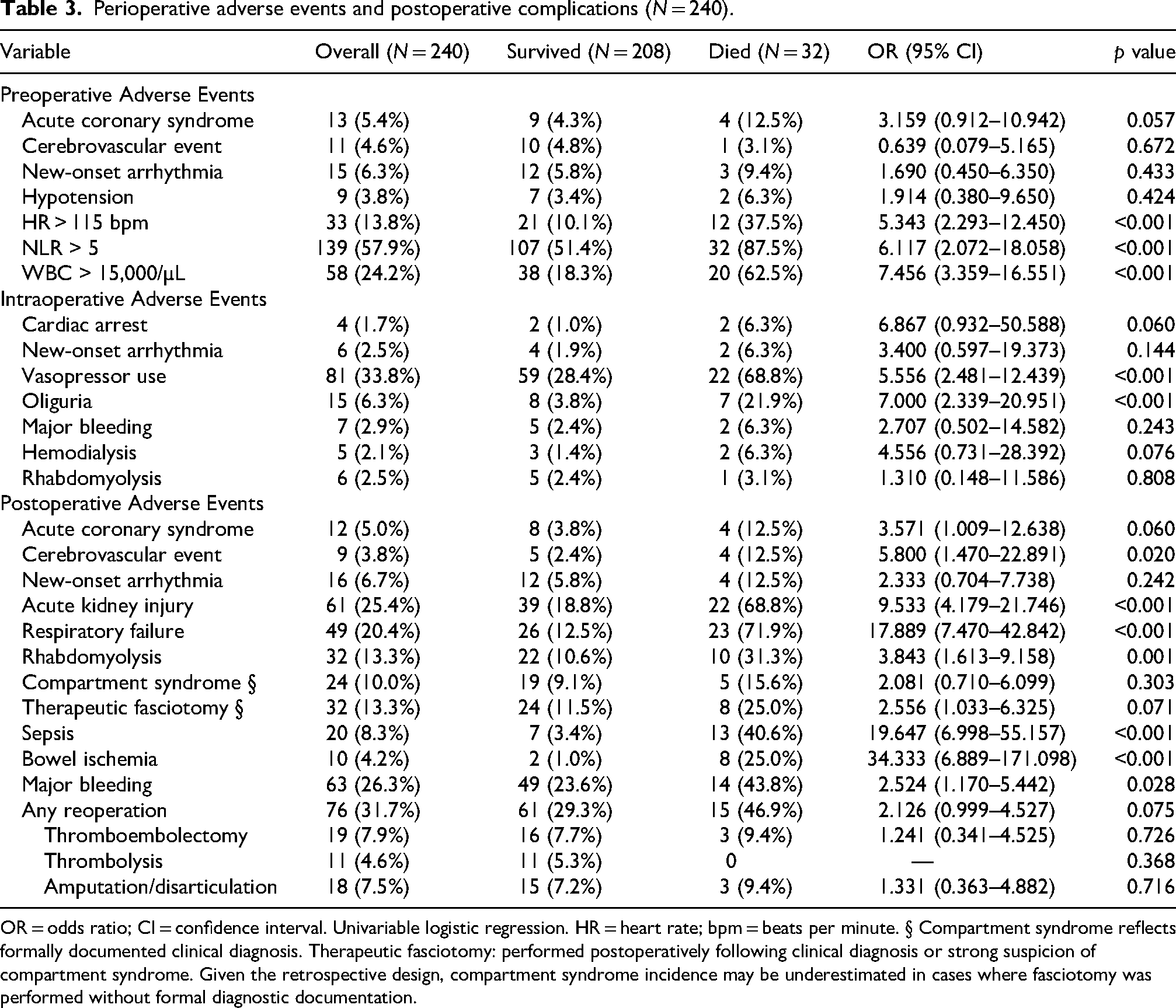
OR = odds ratio; CI = confidence interval. Univariable logistic regression. HR = heart rate; bpm = beats per minute. § Compartment syndrome reflects formally documented clinical diagnosis. Therapeutic fasciotomy: performed postoperatively following clinical diagnosis or strong suspicion of compartment syndrome. Given the retrospective design, compartment syndrome incidence may be underestimated in cases where fasciotomy was performed without formal diagnostic documentation.
Multivariable analysis
Multivariable logistic regression identified four independent predictors of in-hospital mortality (Table 4): preoperative leukocytosis (WBC >15,000/µL; aOR 4.046, 95% CI 1.522–10.754; p = 0.005), intraoperative vasopressor use (aOR 4.000, 95% CI 1.477–10.831; p = 0.006), postoperative respiratory failure (aOR 8.441, 95% CI 3.199–22.272; p < 0.001), and bowel ischemia (aOR 15.242, 95% CI 2.398–96.903; p = 0.004).
Multivariable logistic regression analysis: independent predictors of in-hospital mortality.
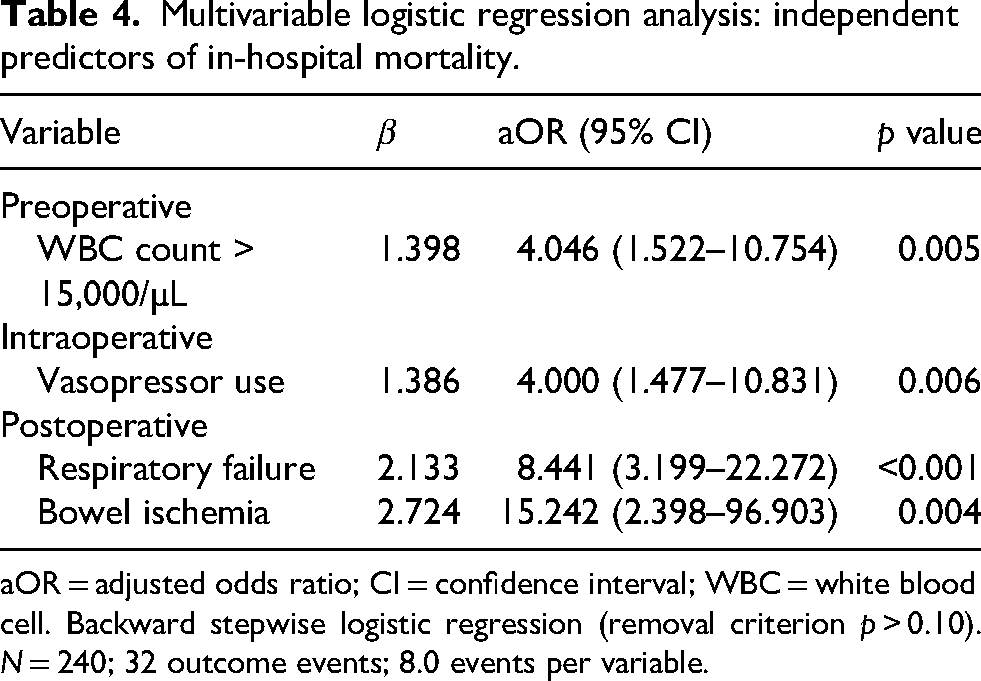
aOR = adjusted odds ratio; CI = confidence interval; WBC = white blood cell. Backward stepwise logistic regression (removal criterion p > 0.10). N = 240; 32 outcome events; 8.0 events per variable.
Discussion
ALI is a distinct vascular disease characterized by severe systemic presentations, often driven by underlying comorbidities and preoperative conditions. Disease progression, treatment-related factors, and individual patient responses contribute to a spectrum of outcomes, including MACE and mortality.
In this study, the perioperative MACE incidence was 17.5%, and all-cause in-hospital mortality was 13.3%. Compared with a contemporary single-center cohort reporting MACE in 29% and perioperative mortality in 20% of patients undergoing urgent revascularization for ALI, 5 our cohort demonstrated lower event rates, possibly reflecting differences in case mix, the inclusion of hybrid endovascular approaches, or the more contemporary study period. Although MACE occurred in nearly one in five patients, only 1.7% of deaths were directly attributed to cardiovascular causes. This dissociation between MACE incidence and cardiovascular mortality underscores that most ALI-related deaths result from multiorgan failure rather than isolated cardiovascular events, and highlights the need for comprehensive perioperative vigilance beyond cardiac monitoring alone.
Technical success, achieved in 92.9% of our cohort, was significantly associated with survival on univariable analysis (OR 0.180; 95% CI 0.063–0.516; p < 0.001). Although technical success did not retain independent significance in the multivariable model, likely due to limited statistical power with 32 outcome events, this finding is consistent with results from the RESCUE ALI study, in which technical failure was an independent predictor of 1-year amputation-free survival. 8 Collectively, these findings underscore the prognostic importance of achieving adequate revascularization and support the reporting of procedural success parameters as clinically relevant outcome measures in ALI.
In our univariate analysis, markers of physiological stress and inflammation specifically preoperative tachycardia (HR > 115 bpm), leukocytosis (WBC > 15,000), and elevated NLR (> 5) along with renal dysfunction (history of CKD and eGFR < 60), were significantly associated with increased in-hospital mortality. This aligns with previous studies linking leukocytosis to adverse outcomes in percutaneous coronary intervention 9 and endovascular aortic aneurysm repair. 10 Similarly, elevated NLR has been established as a significant prognostic marker in vascular surgery 11 and specifically associated with mortality and amputation in patients with ALI. 12
Notably, preoperative leukocytosis (WBC > 15,000/µL) remained a significant independent predictor of in-hospital death in the multivariable model (aOR 4.046; 95% CI 1.522–10.754; p = 0.005), suggesting that an elevated WBC count at presentation carries independent prognostic value beyond serving as a general marker of physiologic stress. In contrast, tachycardia (HR >115 bpm) and elevated NLR, despite their significance on univariable analysis, did not retain independent effects in the final model, suggesting that these parameters reflect overall physiologic stress rather than independent causal pathways, with their prognostic effect likely mediated through downstream complications such as intraoperative vasopressor requirement and postoperative organ failure.
Regarding renal function, univariate analysis identified history of CKD and reduced eGFR (<60 mL/min/1.73 m2) as significant predictors of mortality. However, these factors did not retain statistical significance in the multivariate model, likely because their impact is captured by overlapping comorbidity markers. From a clinical perspective, preoperative renal dysfunction plays a critical role by compromising the patient's ability to tolerate intraoperative stress. Moreover, kidney disease after major vascular surgery is associated with significant increases in 90-day mortality and cost, with the highest risk observed among patients developing postoperative renal failure regardless of previous CKD. 13 Patients with reduced renal reserve have limited capacity to regulate fluid and electrolyte balance and are more susceptible to the hemodynamic shifts inherent to major vascular surgery. In our study, this instability was clinically evident, often necessitating intraoperative vasopressor support (p < 0.001) and resulting in oliguria (p < 0.001), reflecting a “fragile” physiologic state in which even minor intraoperative insults can precipitate a cascade of organ dysfunction.
Intraoperative management of ALI therefore requires meticulous hemodynamic optimization, in which anesthetic technique plays a contributory role. In our cohort, general anesthesia was the predominant technique (71.7%), yet nearly a quarter of patients tolerated monitored anesthesia care. Although general anesthesia was associated with higher mortality on univariable analysis (OR 3.448; p = 0.049), it did not remain an independent predictor in the multivariable model, likely reflecting confounding by indication. Patients requiring general anesthesia tended to undergo more complex procedures with greater hemodynamic compromise. Regardless of anesthetic modality, maintaining adequate perfusion pressure is paramount. Intraoperative hypotension has been associated with postoperative adverse outcomes across multiple surgical populations. 14 Although randomized data suggest that targeting a lower MAP may not impact mortality, 15 the significant association between vasopressor use and mortality in our cohort suggests a complex relationship: while vasopressors are necessary to maintain organ perfusion, they may simultaneously contribute to myocardial strain and ischemic injury in vulnerable end-organs. 16 A comprehensive intraoperative strategy should therefore include targeted blood pressure management, judicious vasopressor use, optimization of volume status, and vigilant monitoring for reperfusion injury.
Ischemia/reperfusion injury initiates a cascade of systemic events following revascularization. Restoration of blood flow triggers a surge in reactive oxygen species, inflammatory mediators, and toxic metabolites, causing endothelial injury, increased pulmonary vascular permeability, and acute lung injury, 17 mechanisms that likely underlie the high incidence of postoperative respiratory failure (20.4%) and its strong association with mortality (affecting 71.9% of non-survivors vs 12.5% of survivors). Hemodynamic instability requiring vasopressor support may further impair pulmonary microcirculation, and patients with limited cardiopulmonary reserve are particularly susceptible to ventilator dependence following prolonged general anesthesia. Beyond the pulmonary system, rhabdomyolysis significantly more prevalent in non-survivors (31.3% vs 10.6%, p = 0.001), reflects the severity of skeletal muscle necrosis and the systemic release of nephrotoxic myoglobin, contributing to postoperative renal failure (p = 0.001). Compartment syndrome occurred in 24 patients (10.0%), with therapeutic fasciotomy performed in 32 patients (13.3%), further underscoring the clinical burden of reperfusion injury in this cohort. The systemic inflammatory response triggered by reperfusion may also precipitate a sepsis-like syndrome or SIRS, which can be clinically indistinguishable from true infectious sepsis; notably, 25% of patients with postoperative sepsis had concurrent rhabdomyolysis, illustrating this diagnostic challenge. Taken together, these findings highlight that minimizing reperfusion injury is as critical as achieving revascularization itself, and that postoperative surveillance must extend beyond the revascularized limb to include respiratory, renal, and mesenteric systems.
Postoperative renal failure was common and strongly associated with mortality, occurring in 61 patients (25.4%) overall and in 22 of 32 non-survivors (68.8%). ALI patients are predisposed to renal complications due to preexisting renal dysfunction, volume depletion, contrast media exposure, and the systemic inflammatory cascade triggered by ischemia-reperfusion injury, which drives multiorgan dysfunction including renal impairment. Although postoperative renal failure was not included in the multivariable model owing to variability in diagnostic criteria across the study period, its strong univariable association (OR 9.53, 95% CI 4.18–21.75) and high prevalence among non-survivors (68.8%) underscore its clinical importance as an early warning sign requiring vigilant postoperative monitoring.
In this study, bowel ischemia developed in 4.2% of patients and carried an 80% mortality rate, exceeding the pooled short-term mortality of 59.6% reported in systematic review and meta-analysis of acute mesenteric ischemia. 18 Proposed etiologies for bowel ischemia include arterial embolism, arterial thrombosis, venous thrombosis, and nonocclusive mesenteric ischemia, with arterial causes being more common than venous causes. 18 If left untreated, reduced blood flow in the splanchnic circulation, regardless of cause, can lead to bowel ischemia. Although the exact etiology of bowel ischemia may be indeterminate, factors such as the timing of revascularization and the length of the remaining functional bowel are crucial risk factors of its high mortality.19,20 Given the prevalence and severity of bowel ischemia, early diagnosis and prompt treatment are essential components of postoperative care for ALI patients. 20
Ultimately, our multivariable analysis identified four independent predictors of in-hospital mortality: preoperative leukocytosis (WBC >15,000/µL; aOR 4.046), intraoperative vasopressor use (aOR 4.000), and the postoperative complications of respiratory failure (aOR 8.441) and bowel ischemia (aOR 15.242). This finding highlights a clear paradigm: mortality in ALI is not driven by a single catastrophic event but by a cascade of systemic insults beginning with preoperative physiologic stress and culminating in postoperative organ failure. The particularly high odds associated with bowel ischemia and respiratory failure underscore that in ALI, the thromboembolic burden and reperfusion injury frequently extend beyond the limb to vital visceral organs and the respiratory system. Improving survival therefore requires a dual strategy: early recognition of patients at high preoperative risk evidenced by leukocytosis and hemodynamic instability requiring vasopressors and aggressive postoperative surveillance for respiratory deterioration and mesenteric ischemia in all patients undergoing revascularization for ALI.
This study has several limitations. First, its retrospective design introduces the inherent risks of incomplete data collection and treatment selection bias, particularly given that cases were drawn from a single tertiary institution where clinical practices may not reflect broader practice patterns. Second, the sample size calculation was based on a MACE incidence of 6.3% derived from elective vascular surgery literature, whereas our ALI cohort exhibited a substantially higher rate of 17.5%, reflecting the more acute and higher-risk nature of this population. Third, the diagnosis of sepsis was based on clinical documentation rather than prospectively applied standardized criteria, and diagnostic heterogeneity across the 2014–2022 study period cannot be excluded. As sepsis did not emerge as an independent predictor in multivariable analysis, this limitation has limited impact on the primary findings. Fourth, the multivariable model includes four predictors with 32 outcome events (8.0 events per variable), which, while improved over the original model, remains below the conventionally recommended threshold of ten events per variable; results should therefore be interpreted with caution and confirmed in larger prospective cohorts. Finally, follow-up was confined to the duration of the index hospitalization, precluding assessment of longer-term outcomes in a population known to carry substantial one-year mortality.
Conclusions
In-hospital MACE occurred in 17.5% of ALI patients undergoing revascularization but was not independently associated with mortality, refuting our hypothesis that MACE would be the primary driver of death. Instead, mortality was determined by four independent perioperative predictors: preoperative leukocytosis (WBC >15,000/µL), intraoperative vasopressor requirement, and postoperative respiratory failure and bowel ischemia. These findings demonstrate that death in ALI results from systemic multiorgan failure rather than isolated cardiovascular events and should guide postoperative surveillance priorities and ICU admission decisions in this high-risk population.
Footnotes
Acknowledgments
The authors thank Miss Julaporn Pooliam, MSc, for her guidance on study design, sample-size calculation, and statistical analyses. Writing and language assistance was provided by Grammarly and Gemini (Google); the authors reviewed and approved the final content and take full responsibility for the results.
Consent to participate
The requirement for written informed consent was waived by the Institutional Review Board due to the retrospective nature of the study using de-identified data.
Consent for publication
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project was supported by the Siriraj Research and Development Fund (Grant Number (IO) R016531040).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study protocol was reviewed and approved by the Institutional Review Board of the Faculty of Medicine Siriraj Hospital, Mahidol University (Protocol Number: COA no. Si 359/2022).
Data availability statement
Statistical summaries are presented in the article; datasets are available from the corresponding author on reasonable request.