
Abstract
A 73-year-old male developed early prosthetic aortic valve endocarditis complicated by haemorrhagic cerebral lesions 45 days after tissue valve replacement. Transesophageal echocardiography revealed bulky vegetations and an annular abscess. Urgent surgical valve replacement with extensive debridement was performed, while broad-spectrum antifungal therapy was initiated. Aspergillus terreus was subsequently confirmed. Postoperatively, the patient experienced acute hydrocephalus, subarachnoid haemorrhage, and recurrent vegetations, ultimately precluding further surgery. He died on postoperative day 57. This case highlights the diagnostic and therapeutic challenges of early fungal prosthetic endocarditis with intracranial haemorrhage, emphasizing individualized management by multidisciplinary teams and the high mortality associated with Aspergillus infections.
Introduction
Fungal prosthetic valve endocarditis (PVE) is a rare condition associated with high recurrence rates and poor outcomes. Early-onset PVE caused by Aspergillus species is particularly uncommon, carrying an extreme risk of cerebral embolization and devastating neurological complications. We report a case of early PVE caused by Aspergillus terreus complicated by intracranial haemorrhage. This case highlights the diagnostic challenges, intricate therapeutic dilemmas, and dismal prognosis associated with this clinical entity.
Case description
A 73-year-old male patient was referred for fever, malaise and a recent sudden loss of vision in the right eye.
He had undergone tissue aortic valve replacement (25 Inspiris Resilia; Edwards Lifesciences, Irvine, CA, US) via ministernotomy 45 days prior at another facility.
Upon arrival, the patient was febrile, hemodynamically stable, alert and oriented without neurological deficits. Transesophageal echocardiography (TEE) revealed an annular abscess, trivial aortic regurgitation and voluminous prosthetic vegetations, the largest measuring 32 × 21 mm, (Figure 1 and Video 1).
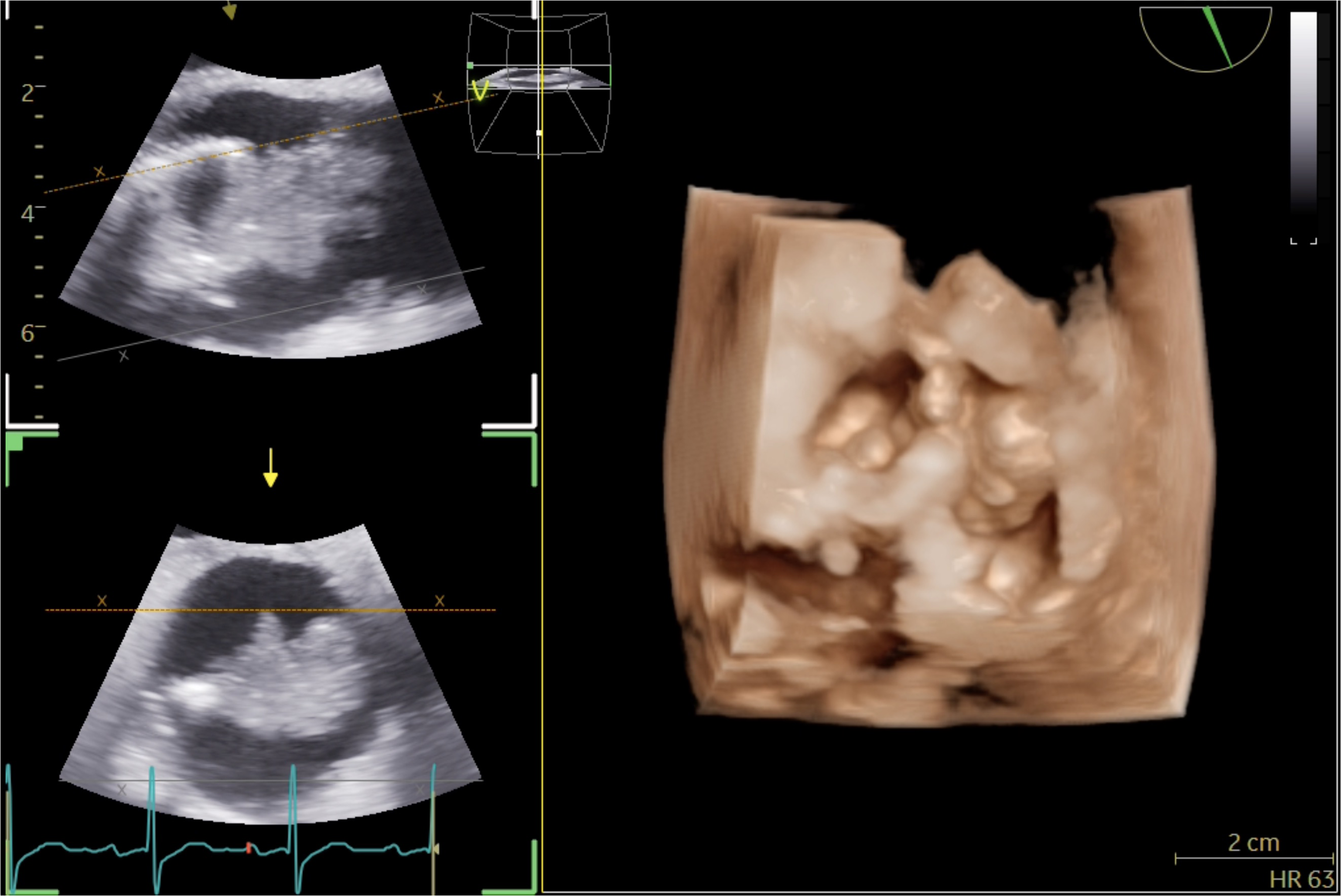
Transesophageal echocardiography showing bulky vegetations on the aortic valve prosthesis.
Brain computed tomography (CT) and angiography demonstrated a small subarachnoid haemorrhage (SAH) in the right central sulcus without mycotic aneurysms. Pending blood culture results, empirical broad-spectrum therapy was initiated following an infectious disease consultation: intravenous daptomycin (10 mg/kg/24 h), meropenem (2 g/8 h), and high-dose caspofungin (150 mg/24 h).
Surgery was scheduled for the next morning. Via full sternotomy and central cannulation, the infected bioprosthesis was explanted and all vegetations were meticulously removed, with the largest measuring 35 × 24 mm (Figure 2 and Video 2). Following extensive debridement, the aortic annulus was reconstructed with bovine pericardial strips, and a 23 mm CE Perimount Magna Ease bioprosthesis (Lifesciences Corp., Irvine, CA, US) was implanted. The immediate postoperative course was uneventful. The patient was extubated on postoperative day (POD) 2 without neurological sequelae. Follow-up Brain CT scans on POD 1 and 5 showed a slight reduction in the known SAH.
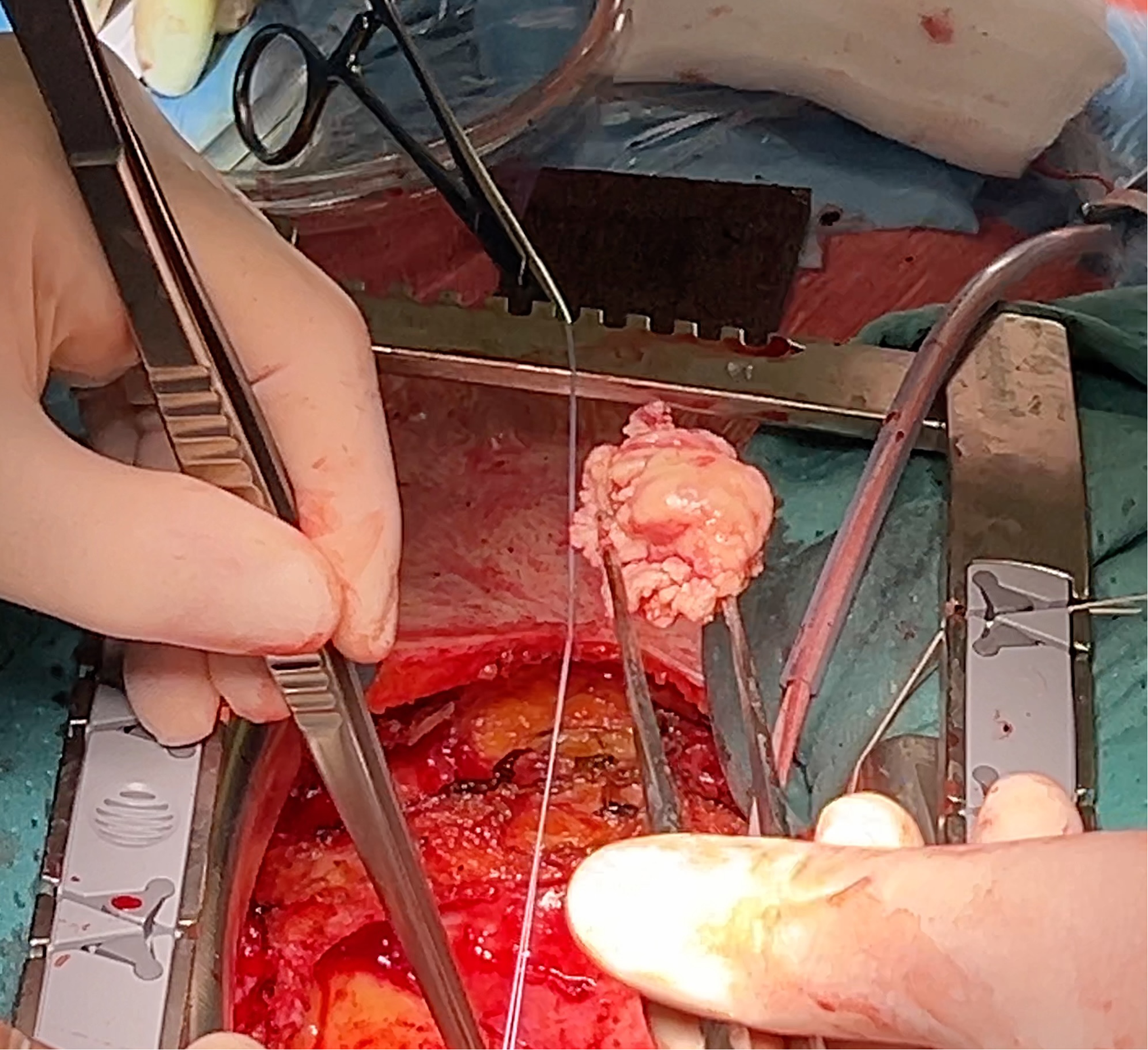
A large vegetation was removed from the aortic root.
Direct microscopy of the explanted valve tissue demonstrated septate, acutely branching fungal hyphae consistent with Aspergillus spp. (Figure 3). On POD 2, preoperative blood and intraoperative tissue cultures yielded Aspergillus terreus, prompting a targeted switch to isavuconazole.

Direct microscopy of the explanted valve tissue demonstrated septate, acutely branching fungal hyphae consistent with Aspergillus spp.
Surveillance TEEs on PODs 3, 7, and 12 showed no residual vegetations or valve dysfunction. On POD 14, the patient became acutely unresponsive. Brain CT revealed acute hydrocephalus from a new, diffuse SAH, requiring emergent external ventricular drainage. Angiography identified a mycotic aneurysm in a branch of the right cerebellar artery, which was successfully coiled. Aspergillus terreus was detected in the cerebrospinal fluid (CSF).
A repeat TEE demonstrated early disease recurrence, showing a 9 × 6 mm vegetation on the right cusp and thickening of the non-coronary cusp (Video 3).
Based on infectious disease recommendations, micafungin (100 mg/24 h) was added to provide broader antifungal coverage, optimizing local biofilm synergy. Due to confirmed neuro-invasion evidenced by positive CSF and urinary galactomannan, targeted therapy was eventually escalated by replacing isavuconazole with voriconazole (6 mg/kg/12 h for 2 loading doses, followed by 4 mg/kg/12 h) to maximize central nervous system penetrance and utilize therapeutic drug monitoring.
Subsequent TEEs showed further progression of the vegetations.
The patient was deemed inoperable, due to an irreversible comatose status.
He underwent a ventriculoperitoneal shunt and tracheostomy and was transferred to a peripheral facility.
He eventually passed away on POD 57.
Discussion
Fungal endocarditis is an uncommon condition characterized by exceptionally high rates of recurrence and mortality (up to 30% and 68%, respectively) despite radical surgical debridement and swift treatment initiation.1,2
Aspergillus represents the second etiological cause, after Candida spp.
Its rising incidence in recent years can be attributed to the increased number of invasive procedures, the extended use of intravenous catheters and devices and broad-spectrum antibiotics.
Diagnosis may be late and requires a high index of suspicion, since clinical manifestations are often unspecific, and blood cultures are usually negative or, if positive, may be dismissed as contaminants.
Definitive diagnosis relies on advanced imaging, histopathology, molecular techniques (PCR), or serum/CSF biomarkers like galactomannan and β-D-glucan.
TEE findings include bulky, friable vegetations, consistent with the high embolic tendency of this disease.
In our case, fungal etiology was not confirmed at the time of surgery, although strongly suspected.
According to the latest ESC endocarditis guidelines, 3 after an ischaemic stroke, surgery is recommended without delay in case of heart failure, uncontrolled infection, abscess or persistent high embolic risk. By contrast, the optimal timing in case of intracranial haemorrhage is controversial since evidence is scarce and inconsistent.
Ideally, it should be delayed for at least 1 month, with periodical imaging and clinical reassessment. Urgent/emergent surgery should be considered only in case of heart failure, uncontrolled infection or persistent high embolic risk, weighing the likelihood of a meaningful neurological outcome.
This case highlights the complexity of determining surgical timing in early fungal PVE with intracranial bleeding. The clinical team must balance opposing priorities: the absolute indication for prompt, radical debridement versus the high risk of expanding a brain bleed due to intraoperative systemic anticoagulation.
In this clinical scenario, urgent surgery was planned despite the potential for brain bleeding in the belief that a prompt extirpation of all the infected material was the only possibility, albeit improbable, of healing.
The postoperative management of fungal PVE demands a nuanced pharmacological strategy that balances local biofilm penetration against targeted central nervous system delivery. While isavuconazole offers predictable pharmacokinetics and excellent accumulation in solid brain tissue, voriconazole remains the preferred choice for Aspergillus PVE with active neuro-invasion due to its superior CSF penetration and amenability to therapeutic drug monitoring.
The management of such complex cases should be reserved for experienced multidisciplinary endocarditis teams, which should also include a neurologist, and decisions made on a case-by-case basis. To our knowledge, this represents only the fourth documented case of PVE caused by Aspergillus terreus.4,5
Supplemental Material
Supplemental Material
Supplemental Material
Footnotes
Acknowledgement
The authors would like to express their gratitude to Prof. A. Mencacci and Dr. A. Graziani from the Department of Microbiology at the University of Perugia for providing the microscopy image used in this report.
Ethical approval
Not applicable.
Informed consent
Written informed consent was obtained from the patient.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.