
Abstract
From September 1997 to January 1998, minimally invasive harvesting of the long saphenous vein was carried out on 30 randomly selected patients undergoing coronary artery bypass grafting. Two to 4 small skin incisions were made for subcutaneous dissection of the vein. The mean ratio of skin incision length to conduit length was 0.29 ± 0.01. The mean time for conduit preparation was 55 ± 2.6 minutes. Mean hospital stay was 9.2 ± 0.2 days. Morbidity in these patients was significantly lower than that of a control group of 100 patients who underwent the conventional open technique. The method was simple and effective in providing good quality venous conduits at low cost with improved patient satisfaction.
Introduction
In spite of the increasing use of arterial conduits provided by the left and right mammary arteries as well as the radial, gastroepiploic, and superior epigastric arteries, the saphenous vein continues to be an essential conduit in some coronary artery bypass procedures. 1 The success of revascularization depends on good quality venous conduit and requires careful handling and preparation of the vein. The established factors responsible for graft failure include subendothelial proliferation and subintimal fibrous hyperplasia with later atherosclerosis of the graft. Thus, avoiding trauma during venous conduit preparation is important for long-term patency of the graft. 2
The conventional longitudinal skin incision for harvesting the saphenous vein or the alternative short skin bridging technique can lead to many complications. The most common are minor complications such as pain, paresthesia, chronic edema, wound dehiscence, wound discharge, and superficial or deep infections. Rare complications include sepsis and amputation. 3 –5 In an attempt to expedite vein removal without compromising its structure and to minimize tissue dissection, thus reducing early and late complications due to the leg incision, we used a simple minimally invasive harvesting technique. We report our initial experience with this technique in 30 patients undergoing coronary artery bypass grafting.
Patients and Methods
From September 1997 to January 1998, 30 patients undergoing coronary artery bypass graft operations were randomly selected for minimally invasive harvesting of the long saphenous vein. There were 28 male (93.3%) and 2 female (6.7%) patients. The mean age was 50.4 ± 1 years, ranging from 42 to 64 years old. All patients underwent standard coronary artery bypass grafting using cardiopulmonary bypass, aortic cross-clamping, and blood cardioplegia. The technique of vein harvest was evaluated for the quality and length of the venous conduits, number and length of the skin incisions, time for conduit preparation, number of grafts per patient, use of the left internal mammary artery, incidence of perioperative myocardial ischemia or infarction, incidence of complications related to vein harvesting, and degree of patient satisfaction. In addition, we examined the histological structure of the vein conduit for damage during preparation.
Technique of Vein Harvest
The technique consisted of 2 to 4 small incisions, 2 to 3 cm long, and subcutaneous dissection of the long saphenous vein. After removal of the saphenous vein, preparation for grafting was completed in vitro. Subcutaneous dissection was performed with an illuminated retractor (182-mm Craig Aufricht fiberoptic nasal retractor; Downs Surgical Ltd., Sheffield, England, UK), or a Langenbeck retractor (Downs Surgical Ltd., Sheffield, England, UK), or an AutoSuture mini harvest retractor system (AutoSuture International, Inc., Norwalk, CT, USA). Long dissection scissors and a long clip applicator (Premium Sugiclip II; AutoSuture International, Inc., Norwalk, CT, USA) were employed. The first incision was made 4 cm above the medial malleolus, the saphenous vein was exposed, and a Silastic sling was used to tape the vein. Subcutaneous dissection was continued both distally and proximally. The distal end of the saphenous vein was double-clamped with two medium Liga clips (Ethicon Endosurgery, Inc., Cincinnati, OH, USA) and divided. The distal end was cannulated with a metal cannula (PO-27-1090; Pilling Weck, Le Faget, France) and distended with saline containing heparin 1000 units·L−1. The proximal dissection was completed subcutaneously with clamping of the distal part of the tributary and division of all tributaries as far from the conduit as possible. A second skin incision was made in the middle of the leg and the technique was repeated up to a third incision below the knee joint. When a length of vein adequate for the procedure was obtained, it was divided proximally after double-clamping. When a longer vein conduit was required, dissection was extended subcutaneously to above the knee joint with an additional skin incision above the knee.
The vein was removed and major tributaries were tied with 4/0 Ti-Cron ligature (Davis & Geck, Danbury, CT, USA). Smaller tributaries were secured with 6/0 Prolene suture (Ethicon Ltd, Edinburgh, Scotland, UK). The vein was distended with papaverine solution (1 mg in 10 mL saline) for 10 minutes. The length of the venous conduit was measured. The vein was washed with heparin-saline and kept in heparinized blood for 10 to 20 minutes until used for grafting. The small incision wounds were closed in a single layer using 3/0 Ti-Cron in a subcuticular manner. Three venous specimens were sent for histological examination: one from the distal end (minimal traction); one from the central section (high traction); and one from the proximal end (no traction).
Postoperative care included crepe bandaging of the leg for 24 hours followed by support with an elastic stocking during the day for one month postoperatively. All patients were given postoperative aspirin, 75 mg per day, for at least 3 months. To compare the incidence of complications in the 30 patients in this study group with patients who underwent saphenous vein harvest by the conventional longitudinal skin incision, we reviewed retrospectively the records of 100 age-matched patients (mean age, 51.5 ± 1 years) who underwent coronary artery bypass grafting in our center.
Qualitative data were analyzed using the standard error of the difference between percentages (U test). A p value of less than 0.05 was considered significant. Data were expressed as mean ± standard error of the mean.
Results
The mean number of distal grafts per patient was 3.7 ± 0.1. The left internal mammary artery was used in 27 patients (90%) and 3 (10%) had only venous grafts because of unstable hemodynamics during induction of anesthesia. The mean length of the harvested venous conduit was 39.5 ± 1.5 cm (range, 23 to 53 cm). The mean number of skin incisions was 3.1 ± 0.1 and the mean combined length of the skin incisions was 11.9 ± 0.6 cm. The skin incision length to conduit length ratio was 0.29 ± 0.01. The mean time for conduit preparation was 55.9 ± 2.6 minutes.
The mean duration of hospital stay was 9.2 ± 0.2 days. We observed no increase in hospital stay related to leg wounds and the patients were mobilized on the first postoperative day. In the 100 control patients who underwent coronary artery bypass grafting with conventional longitudinal skin incisions for saphenous vein harvesting, we found that 20% had an extended hospital stay due to complications related to the leg wounds (Table 1).
Complications Associated With Saphenous Vein Harvest
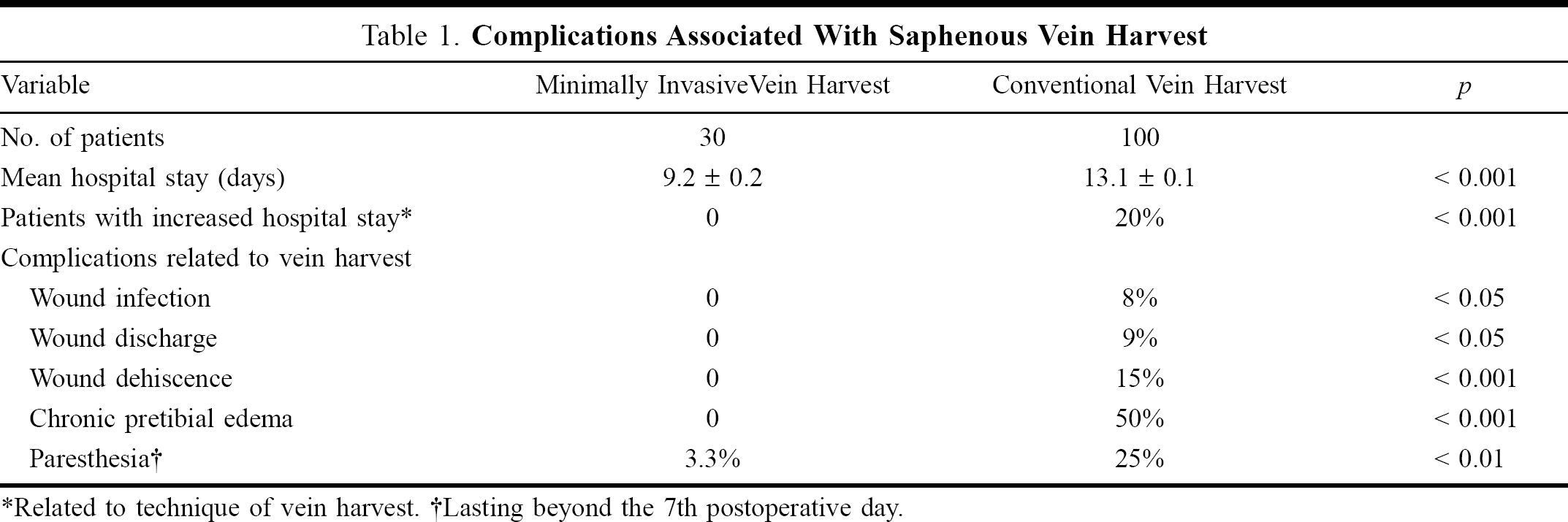
Related to technique of vein harvest.
Lasting beyond the 7th postoperative day.
There was no incidence of postoperative chronic pretibial edema or infection, discharge, or dehiscence in any of the leg wounds in the 30 patients who underwent the minimally invasive vein harvest technique. There was no postoperative paresthesia after the 7th postoperative day in the study patients, except for one patient who developed paresthesia that improved after 6 weeks. In contrast, patients in the control group experienced a higher incidence of such complications (Table 1). Twenty-nine (97%) of the 30 patients in the study group expressed satisfaction with the vein harvest procedure.
Histological examination of the venous specimens showed no marked difference between the proximal, middle, and distal specimens and there was no evidence of significant intimal endothelial damage in any of the study patients. There was no evidence of perioperative ischemia or infarction in the myocardial regions supplied by the venous grafts as documented by analyses of ST segments on the electrocardiographic monitor as well as by intraoperative transesophageal echocardiography.
Discussion
Coronary artery bypass graft surgery is the most common cardiovascular surgical procedure nowadays. 6 Its success depends on the quality of the conduit harvested, whether arterial or venous. 7 The conventional method using a long skin incision along the course of the saphenous vein carries the risk of many complications, as seen in our control group. These complications were in addition to the dissatisfaction of patients generally with this technique. The only complication in the study group was one case of paresthesia and 97% of the patients reported satisfaction with the procedure.
Over recent years, the trend for minimally invasive procedures (keyhole surgery) in cardiovascular operations has grown, including minimally invasive coronary artery bypass grafting, aortic and mitral valve replacements, and saphenous vein harvesting. These techniques use minimal incisions to achieve less morbidity, earlier ambulation, and shorter hospital stay. 8 In our center, we routinely discharge patients who undergo conventional coronary artery bypass grafting on the 8th postoperative day when they have an uneventful postoperative course (with 24 to 48 hours preoperative admission). In this study, the mean hospital stay was 9.2 ± 0.2 days with no increase in the hospital stay for leg wound related complications. The longer hospital stay in the control group (13 ± 1 days) was due to leg wound related complications.
In this simple technique for subcutaneous harvesting of the long saphenous vein under direct vision with dissection through a few small incisions, care was taken to preserve the vein structure and function as a conduit. Histological examination demonstrated the effectiveness of vein preservation and the minimal traction provided by the use of the Silastic slings had no damaging effect on the vein conduits. It was noted that the duration of conduit preparation decreased with experience; in the early cases, we spent more time preparing the conduit (80 to 90 minutes) compared with the later stage of the study where conduit preparation took 30 to 40 minutes. We also found that the skin incision length to conduit length ratio was gradually reduced by experience from 0.4 to 0.2.
Currently, there are a number of commercial devices available for minimally invasive vein harvesting such as the AutoSuture Mini Harvest System that we used in 30% of our patients and the Endopath System (Ethicon Endosurgery, Inc., Cincinnati, OH, USA) that we are currently assessing. We employed a reusable illuminated subcutaneous retractor and found that the procedure was simple, cost-effective, reliable, and comparable to the conventional open technique in terms of time. A good quality of venous conduit for coronary artery grafting was obtained with a marked reduction in morbidity and earlier ambulation of the patients, who expressed a high degree of satisfaction with this technique.