
Abstract
Clinical and angiographic rates of restenosis after angioplasty were compared in 80 patients (group A) with ejection fractions below 40% (mean, 28.3% ± 5.2%) and 50 (group B) with ejection fractions above 50% (mean, 58% ± 5.4%). Mean angina class improved to the same degree in both groups after angioplasty. Recurrence of significant angina within 6 to 12 months affected 30 patients (38%) in group A compared to 12 (24%) in group B (p > 0.05). Angiographic restenosis occurred in 42 patients (53%) in group A compared to 14 (28%) in group B (p = 0.006). Restenosis after single-vessel angioplasty was 46% in group A and 25% in group B (p > 0.05), after multivessel angioplasty it was 62% in group A and 33% in group B (p = 0.05). In group A, restenosis was more frequent in the left anterior descending coronary artery (46%) compared to the right coronary (41%) or circumflex (30%). Higher rates of restenosis occurred in patients with prior coronary artery bypass grafting (64%) or recanalization of chronic total occlusion (61%). Angina was a less reliable indication of restenosis in group A. We attribute the higher rate of restenosis in patients with low ejection fractions partly to low coronary perfusion pressure.
Introduction
Luminal narrowing after successful percutaneous transluminal angioplasty (PTCA) is a complex process that is only partially understood and is probably related to elastic recoil, intimal proliferation, and arterial remodelling. 1 –4 Although anginal status, cardiac event rate, and noninvasive tests can indicate restenosis, the angiographically-determined change in lumen diameter is currently the most reliable indicator of the extent of restenosis. 2,3,5,6 Numerous clinical and experimental studies have been carried out to elucidate the factors that may predict luminal narrowing after a successful PTCA procedure but the results of these studies are conflicting. 2,3,5 –7 Patients with coronary artery disease and impaired left ventricular (LV) function are currently candidates for PTCA for whom it gives reasonably good immediate results with low rates of acute complications. 8 However, no data are available regarding the rate of restenosis in the long term for this group of patients. This study was undertaken to determine the clinical and angiographic rates of restenosis after PTCA in patients with impaired LV function.
Patients and Methods
The study group was selected from patients referred during 1995 and 1996 to the University Hospital of Homburg for diagnostic or interventional cardiac catheterization. Patients were included if they had impaired LV function with an ejection fraction (EF) of less than 40%, had undergone successful coronary angioplasty of one or more vessels, and could be followed up clinically and by angiography between 6 and 12 months after angioplasty. There were 80 patients (65 males and 15 females) in the study group (group A). They were compared with a control group of 50 aged-matched patients (40 males and 10 females) with an EF greater than 50% who had PTCA during the same period and could be followed up (group B). The mean age in group A was 56 ± 13 years compared to 58 ± 12 years in group B. The mean EF was 28.3% ± 5.2% in group A and 58% ± 5.4% in group B.
Angina pectoris before and after PTCA was assessed and classified according to the Canadian Cardiovascular Society (CCS). 9 Coronary angiograms were obtained in each patient just before PTCA, immediately after, and at follow-up. The angiograms were recorded and analyzed by quantitative computer-assisted coronary angiography using a Phillips DCI system (Phillips, Eindhoven, The Netherlands). 10 Standard PTCA procedures were per-formed using guidewires and balloon catheters, intracoronary stents were implanted in 56 patients of group A and 21 patients of group B, according to angiographic indications. Successful PTCA was defined as a reduction in luminal diameter narrowing at the lesion site to below 50%. 5,7,11,12 Clinical restenosis was con-sidered if there was a recurrence of angina to the same severity or at least moderate (CCS class II) angina during follow-up. 2 Angiographic restenosis was defined as luminal diameter narrowing at the lesion site of more than 50% or an improvement of less than 30% of the pre-dilatation narrowing. 2,3,5 –7,12,13 This was further classified into complete restenosis if further narrowing was observed in all the dilated lesions, or partial restenosis if there was a recurrence of stenotic lesions in some sites and not in others or if the improvement in luminal diameter was greater than 30%. 11
The Z test was used for comparison of two different proportions of the studied variables in the two different groups.
Results
The clinical data and angiographic findings in both groups are shown in Table 1. In group A, 61 patients had a previous myocardial infarction, usually anterior, in contrast to group B where significantly fewer (19) patients had a previous myocardial infarction. There was also a significantly greater extent and severity of coronary artery disease in the patients in group A. Before PTCA, 10 patients in group A were in CCS class I, 32 were in class II, 32 were in class III, and 4 were in class IV. The mean CCS angina class of group A was 2.4 ± 0.6 before PTCA and 1.2 ± 0.5 at follow-up. In group B, there were 6 patients in CCS class I, 19 in class II, 21 in class III, and 3 in class IV, with a mean CCS angina class of 2.3 ± 0.5 before PTCA and 1 ± 0.4 at follow-up.
Clinical and Angiographic Data in 80 Patients with Left Ventricular Dysfunction (Group A) and 50 Control Patients (Group B)
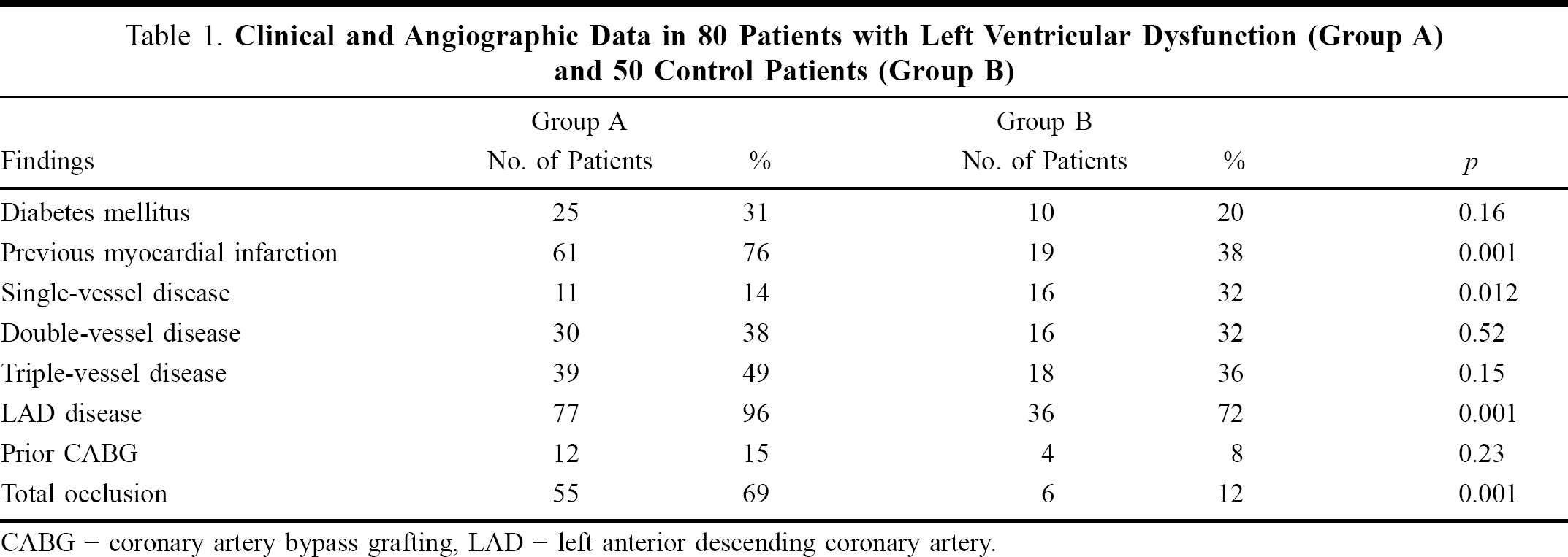
CABG = coronary artery bypass grafting, LAD = left anterior descending coronary artery.
During follow-up of 6 to12 months, 38% of patients in group A had at least moderate angina comprising 23 patients in CCS class II and 7 in class III, compared to 24% in group B but the difference was not statistically significant (Table 2). However, a significantly higher rate of angiographic restenosis (53%) was observed among group A patients of whom 10 had complete restenosis in all the dilated sites and 32 had partial restenosis (comprising 23 patients with recurrence of a lesion milder by at least 30% and 9 patients who had restenosis at some of the dilated lesions but not others). Angiographic re-stenosis was detected in significantly fewer (28%) patients in group B of whom 6 had complete and 8 had partial restenosis. The difference between the two groups was most marked in patients with multivessel disease (Table 2 and Figure 1).
Rates of Clinical and Angiographic Restenosis in Groups A and B
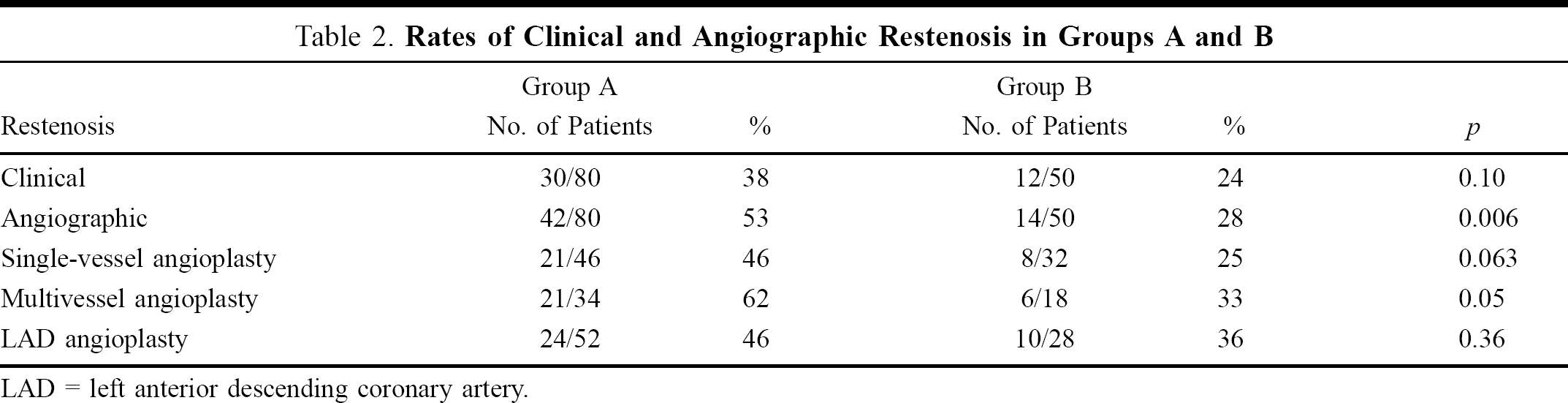
LAD = left anterior descending coronary artery.
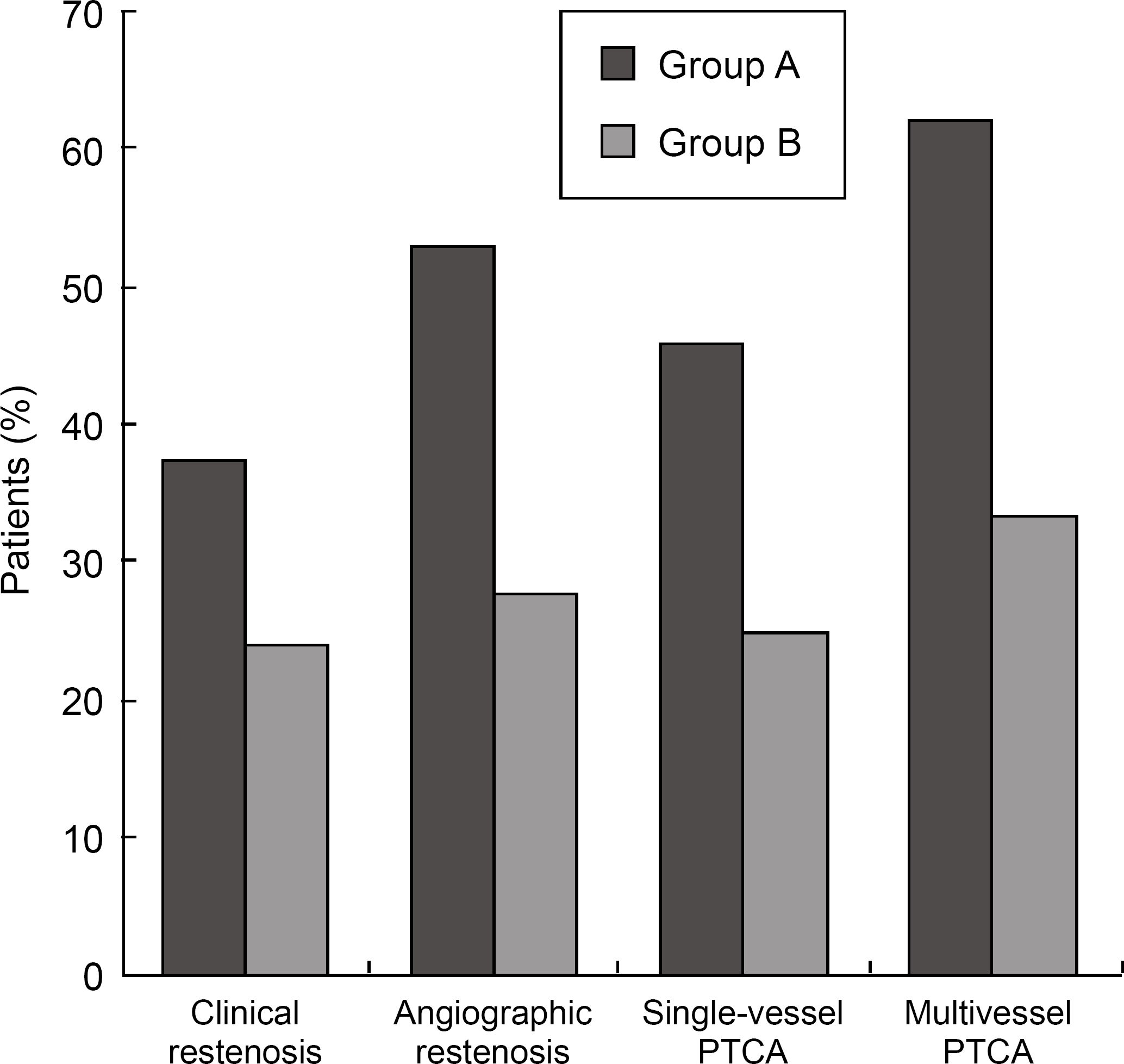
Rates of restenosis in 80 patients with left ventricular dysfunction (group A) and 50 control patients (group B) after percutaneous transluminal coronary angioplasty (PTCA).
In group A, angioplasty was performed on the left anterior descending coronary artery (LAD) in 52 patients of whom 24 had restenosis (not statistically significant from group B), comprising 13 cases of partial restenosis and 11 of complete restenosis of the LAD (Figure 2). Thirty patients had PTCA for circumflex stenosis that recurred in 9; 4 had partial and 5 had complete restenosis. PTCA of the right coronary artery was performed in 32 patients, restenosis occurred in 13 (41%); 9 had partial and 4 had complete restenosis. Of 11 patients who had PTCA after coronary artery bypass grafting, 7 (64%) had restenosis. Recanalization of chronic total occlusion was performed in 31 patients with restenosis in 19 (61%); 15 had partial and 4 had complete reocclusion.

Angiographic restenosis of the proximal left anterior descending coronary artery 6 months after angioplasty.
Among the 42 patients in group A with angiographic restenosis, 20 (48%) had significant angina, including 12 patients in whom angina was the same or worse and 8 who had slightly less (but at least moderate CCS class II) angina than before PTCA. Twenty-two patients in group A had angiographic restenosis without significant symptoms. Of the 30 group-A patients with clinical angina, only 21 (70%) had angiographic restenosis. On the other hand, among 14 patients with angiographic restenosis in group B, 10 (71%) had angina and 4 had no significant symptoms. Of the 12 patients in group B with angina, 10 (83%) had angiographic restenosis. There were significant differences between the two groups in terms of the percentage of patients with restenosis who had angina (p = 0.04) and the percentage of patients with angina who has restenosis (p = 0.05).
Discussion
Advances in catheter design and improvements in the technique have enhanced the immediate results and safety of coronary angioplasty. However, little progress has been made in controlling the problem of restenosis that can impair the long-term outcome after a successful procedure. 2,7 A number of retrospective and prospective studies have determined some patient-related, lesion-dependant, and procedural risk factors for restenosis, although some of these findings are conflicting. 1,5,7,13 Patients with coronary artery disease and significantly impaired left ventricular function pose a difficult clinical problem and they are currently referred for PTCA as an alternative to surgical revascularization; both can definitely improve the prognosis compared to medical treatment alone. 8 There have been no previous reports of the rate of restenosis in such patients. In our study, the clinical profile showed more diabetics among the patients with a low EF compared to those with good LV function. Patients with LV dysfunction had twice the rate of previous myocardial infarction, more multivessel disease, and higher rates of LAD involvement, total occlusion, and previous coronary artery bypass graft (CABG) surgery. These factors probably contributed to the poor LV function in group A. Extensive multivessel disease, involvement of the LAD, and recanalization of total occlusions were reported to be associated with higher rates of restenosis. 7,11,14
Assessment of restenosis may be based on: detection of local neointimal hyperplasia (histologic), which is not practical; late recurrence of symptoms (clinical), which is patient-dependent and can be misleading; or the development of significant (greater than 50%) luminal narrowing at the treatment site (angiographic) usually between 2 and 6 months after PTCA, which is considered to be most reliable and has become the gold standard for evaluation. 2,3,5 –7 In our study, we evaluated anginal symptoms but we relied on the angiographic method of evaluation and excluded patients who could not be studied by angiography at follow-up.
Among the clinical factors that have been shown to correlate with restenosis, diabetes mellitus, advanced age, hypertension, and severe angina before the procedure were associated with higher rates of restenosis, while hyperlipidemia, gender, previous myocardial infarction, and prior CABG were not related to restenosis. 1,5,7,13 In our study, diabetes, previous myocardial infarction, and prior CABG were more common in group A and we consider these factors to be responsible for the left ventricular dysfunction and not directly related to restenosis. Severity of angina was similar in groups A and B before PTCA and both groups improved significantly at follow-up. Therefore, the higher restenosis rate in group A could not be explained by more severe pre-procedural angina that has been reported to be an independent risk factor for restenosis. 1,5,7,13 Among the angiographic characteristics, multivessel disease and multi-lesion PTCA were related strongly to restenosis as well as the severity of the lesion before and after the procedure and recanalization for total occlusion. 13,15,16 In this study, group A patients had more multivessel disease, multi-lesion PTCA, and recanalization, which may partly explain their higher restenosis rate.
Although patients with poor LV function have not been specifically studied before, those with an EF below 50% were not noted to have different rates of angiographic restenosis from those with an EF above 50% in two reports. 5,13 In our study, we investigated patients who had severely impaired LV function with an EF below 40% (mean EF, 28%) and we observed almost double the restenosis rate of those with good LV function (mean EF, 58%). The higher prevalence of multivessel multi-lesion PTCA, recanalization, and diabetes among group A may explain the difference in restenosis rates. However, analysis of the restenosis rates after single and multivessel PTCA showed they were significantly higher in group A, which indicates that the hemodynamic effects of a low EF may contribute to a high restenosis rate, possibly as a result of low cardiac output, low perfusion pressure in the coronary arteries, and impaired coronary flow.
Some studies have shown that restenosis was not related to the site dilated, while others found a higher restenosis rate with proximal lesions, LAD involvement, previous CABG, angioplasty, and recanalization. 1,13 In our patients with low EF, we observed a slightly higher restenosis rate in cases of LAD disease compared to right coronary and circumflex lesions. However, there was a much higher trend for restenosis with CABG, recanalization, and multivessel PTCA. Restenosis occurs to some extent in all lesions and several investigators have reported no correlation in the restenosis rates of multiple treated lesions in the same patient, in the same way that atherosclerotic progression may occur in multiple untreated sites. 6,11 We also observed different restenosis rates in different lesions, varying from no restenosis to complete restenosis, and we demonstrated significant clinical improvement even with partial restenosis. The occurrence of angina in some patients without angiographic restenosis and the lack of angina in others with confirmed restenosis showed that angina was a less reliable indicator of restenosis in patients with a low EF.
We concluded from this study that coronary angioplasty in patients with LV dysfunction leads to significant clinical improvement but it is associated with a relatively high restenosis rate, especially in those with multivessel disease, recanalization, or previous CABG. We attribute the high restenosis rate partly to the hemodynamic effects of low perfusion pressure in patients with LV dysfunction.