
Abstract

Dear Editor,
Immune checkpoint inhibitors (ICIs), which include programmed cell death protein 1 (PD-1) inhibitors, programmed death ligand 1 (PDL-1) inhibitors, and cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) inhibitors, represent a significant breakthrough in cancer therapy. These therapies, approved by the U.S. Food and Drug Administration (FDA), have revolutionized cancer management by enhancing the body’s immune response against tumors and carcinomas. While their clinical efficacy is notable, they are also associated with a range of immune-related adverse events (IrAEs) affecting multiple organs and systems. 1 This brief report aims to spotlight the psychiatric and cognitive impacts of ICIs, an underexplored area of these adverse events, and discuss genetic predispositions, the interplay of psychological stress with immune function, and the dual role of antidepressants in managing these complexities.
Discussion
A recent pharmacovigilance study examining the FDA Adverse Event Reporting System (FAERS) highlights psychiatric complications as constituting a small but consistent component of all ICI therapy complications, occurring at a rate of 2.71%. 2 These include conditions such as confusional state, insomnia, anxiety, depression, and delirium, often co-occurring with other adverse effects, indicating a strong association with ICI treatment. This study analyzes psychiatric adverse events associated with ICIs from 2012 to 2021 using the FAERS database, extracting and deduplicating 91,683 reports to identify significant correlations through disproportionality analysis. Notably, a significant association between Notch signaling and synaptic-related pathways has been observed, hinting at potential biological mechanisms behind these psychiatric adverse reactions. 2 It is hypothesized that the activation of the peripheral immune system could have neuropsychiatric effects on the central nervous system (CNS), despite mixed evidence regarding the ability of ICIs to cross the blood–brain barrier and directly influence the CNS. The effect of ICI therapy on cognition is well documented, as highlighted by recent research using propensity score matching, which reveals significant cognitive declines at 6 and 12 months in non-small-cell lung cancer patients over 35 years, compared to controls (Table 1). 3
Summary of Psychiatric and Cognitive Manifestations of Immune Checkpoint Inhibitors.
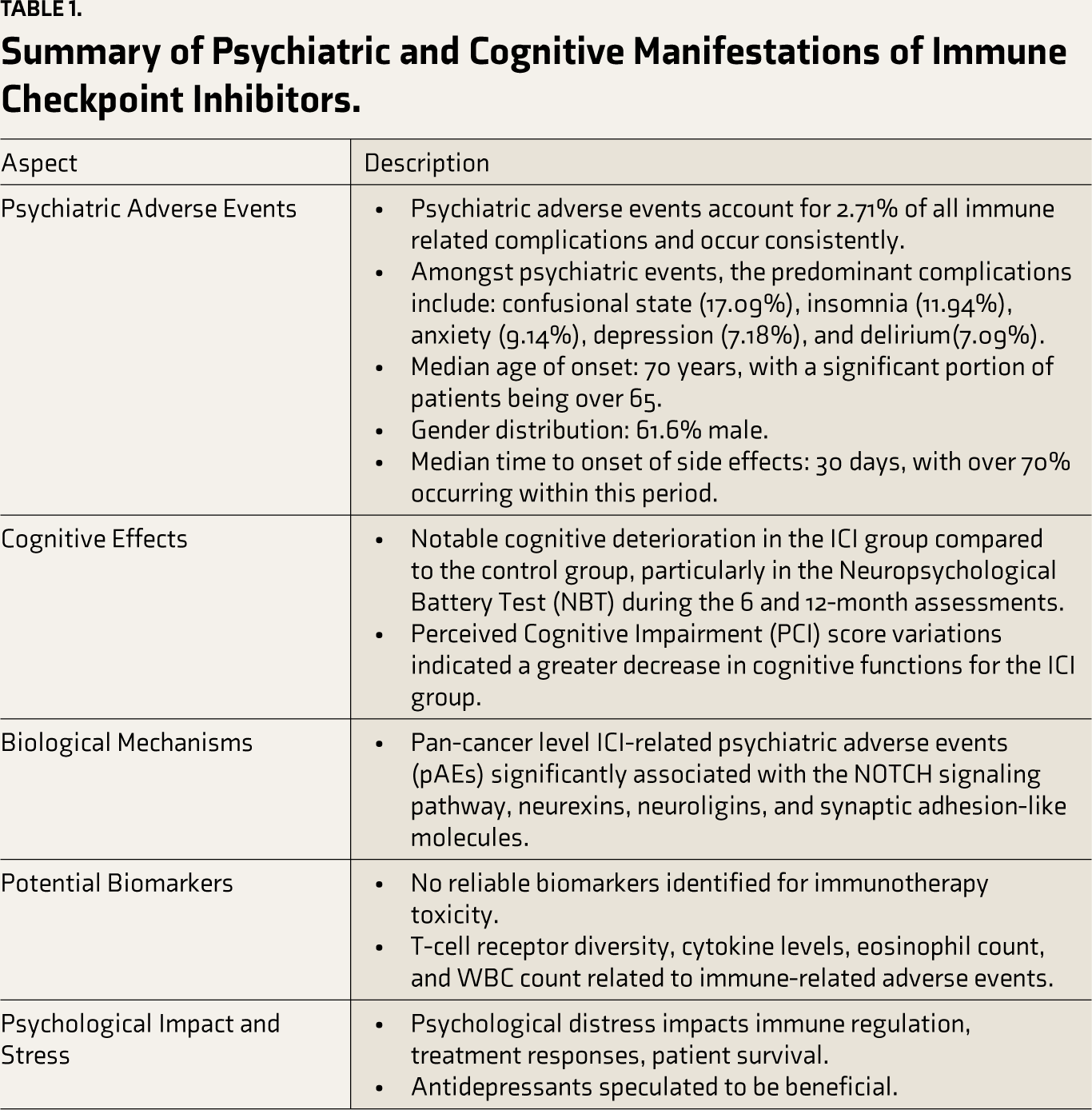
Genetic factors, especially variations in the apolipoprotein E (apoE) gene, could potentially influence both therapeutic response and side effects in cancer patients undergoing ICI therapy. The apoE4 variant, associated with Alzheimer’s disease and cardiovascular disease, may worsen neurological injury and psychiatric disease progression in various conditions, including cancer. This underscores the need for further research into how genetic predispositions affect treatment outcomes. 4 Moreover, definitive biomarkers for immunotherapy toxicity are needed to aid psychiatric intervention, though current markers such as T-cell receptor diversity and cytokine levels show promise.5,6
Research has highlighted that while ICI therapy differs from the treatment-resistant depression seen with IFN therapy, both can similarly increase anxiety levels. 7 This necessitates a more comprehensive exploration of the therapy’s impact on mental well-being. Psychological factors can affect immune regulation and ICI treatment efficacy in cancer patients with better-perceived health linked to positive treatment responses and higher stress and poor sleep associated with increased pro-inflammatory markers. 6 Interestingly, antidepressants have been observed not only to alleviate psychiatric symptoms in cancer patients but also to exhibit anti-cancer activities potentially. Tricyclic antidepressants may sensitize certain resistant cancer cells to apoptosis, while selective serotonin reuptake inhibitors have been associated with inducing cell cycle arrest and autophagy, thereby restraining cancer cell growth.8,9 Moreover, the use of indoleamine 2,3-dioxygenase (IDO) inhibitors in combination with immune checkpoint inhibitors has shown promise in enhancing tumor control by modulating immune responses within the tumor environment. 10
Conclusions
While ICIs represent a significant leap forward in cancer treatment, their psychiatric and cognitive side effects demand further attention and research. The interplay of genetic factors, psychological stress, and the potential for antidepressants to mitigate or even harness these effects presents a complex but promising field of study. By deepening our understanding of these dynamics, we can enhance the efficacy and safety of ICI therapy and improve the overall quality of life for cancer patients. This endeavor calls for a multidisciplinary approach incorporating insights from oncology, psychiatry, neurology, and genetics to fully address the challenges and opportunities presented by immune checkpoint inhibition in cancer therapy.
Footnotes
Acknowledgements
I would like to thank my mentor, Dr Sarki Abba Abdulkadir from Northwestern University, for all his guidance. I would also like to thank Robin Schroffel for proofreading and helping me polish the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
The authors assume full responsibility for the entire content of the manuscript, including the parts generated by the AI tool. The AI tool used was ChatGPT, and it was used to make a table using prompts by the authors and for grammatical proofreading of the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.