
Abstract
Background:
Somatic symptoms are frequent yet understudied manifestations of psychological distress among university students.
Methods:
This cross-sectional, observational study assessed 297 Paraguayan undergraduates using validated instruments to measure somatic symptoms, perceived stress, academic burnout, anxiety, depression, and insomnia.
Results:
Significant correlations emerged between somatic symptoms and exhaustion, perceived stress, insomnia, and psychological distress. A multiple linear regression model identified disengagement, insomnia, anxiety, and depression (–0.29 ≤ all β ≤ 0.23) as significant predictors of somatic symptoms, accounting for nearly 40% of the variance. A parallel mediation analysis revealed that academic burnout mediated the relationship between stress and somatic symptoms, with exhaustion amplifying the effect (β = 0.09) and disengagement mitigating it (β = –0.07).
Conclusions:
These findings underscore the complex interaction between psychological and physical symptomatology among university students and highlight the dual mediating role of burnout. Targeted interventions aimed at mitigating academic stress, sleep disruption, and emotional dysregulation may be instrumental in preventing somatization and fostering student mental well-being.
Question: Which psychosocial factors predict somatic symptoms in university students, and what is the mediating role of academic burnout? Findings: Somatic symptoms were significantly associated with insomnia, anxiety, depression, and exhaustion, while disengagement showed a protective effect, with the model explaining nearly 40% of the variance. Meaning: Somatic complaints among students reflect the interplay of stress, burnout, sleep disruption, and emotional distress, underscoring the need for differentiated interventions.Key Messages:
Summary
This study offers a novel contribution by elucidating the dual mediating role of academic burnout, in particular exhaustion and disengagement, in the relationship between perceived stress and somatic symptoms among university students, a population and context (Paraguay) largely underrepresented in the literature. Unlike prior research, which often treats burnout as a unidimensional construct or overlooks its mediating potential, our findings differentiate the distinct and even opposing effects of exhaustion and disengagement. By integrating validated measures across multiple domains of psychological distress and employing robust mediation analyses, this work advances understanding of psychosomatic processes in academic settings and informs targeted, multifactorial intervention strategies.
Introduction
The academic journey represents a phase characterized by profound psychological and physical challenges that significantly affect students’ well-being. Academic demands, performance-related pressure, financial strain, and familial expectations may lead to elevated stress levels. 1 If not adequately managed, these stressors can result in mental disorders, academic underperformance, and reduced quality of life. 2
A frequent manifestation of psychological distress among university students is the occurrence of medically unexplained somatic symptoms, including headaches, fatigue, gastrointestinal discomfort, palpitations, and breathing difficulties, considered non-verbal indicators of emotional suffering. 3 Somatization may be conceptualized as an alternative expression of psychological distress when coping mechanisms are insufficient.
Recent evidence shows that somatic symptoms are more prevalent in students than in the general population and are associated with stress, anxiety, depression, and sleep problems.3–6 Persistent symptoms impair quality of life, increase healthcare use, and contribute to absenteeism. 7 Burnout, defined as emotional exhaustion and disengagement, has been identified as a pivotal factor in somatization. 8 Students with high burnout report more physical complaints, sleep disturbances, and emotional difficulties. 9
Perceived stress, the appraisal that demands exceed coping resources, is consistently associated with adverse mental health outcomes and somatic symptomatology.10,11 Within universities, stress predicts anxiety and depression and exacerbates physical symptoms, compromising performance. 12 Insomnia, also highly prevalent, affects emotional regulation and is linked to anxiety, depression, and somatization.13,14 Anxiety and depression affect 20%–30% of students and often manifest with somatic complaints.15,16
The interplay among stress, burnout, insomnia, anxiety, depression, and somatic symptoms is complex and may involve both direct and indirect effects. Burnout has been proposed as a mediator between stress and physical symptoms, influencing how distress becomes embodied. 9 Investigating these mechanisms is crucial for understanding student well-being.
Building on these perspectives, this study is framed within a biopsychosocial stress model. Perceived stress acts as a primary trigger, leading to emotional distress, sleep disturbances, and burnout, which manifest as somatic complaints. Anxiety and depression are downstream affective responses, while insomnia reflects disrupted regulation that amplifies symptoms. Burnout functions as both an outcome of chronic stress and a mechanism modulating its somatic translation. Thus, including stress, burnout, insomnia, anxiety, and depression as predictors is theoretically grounded.9–12
In Latin America, and particularly Paraguay, integrative research on these variables remains limited.17,18 The local context of academic pressure, hybrid learning, and socioeconomic challenges may heighten vulnerability to somatic distress, underscoring the need for evidence-based interventions.
This study examines associations among somatic symptoms, burnout, stress, insomnia, anxiety, and depression, and tests burnout as a mediator. It contributes to the global literature on student mental health, particularly in middle-income countries, and seeks to inform strategies that foster healthier and more resilient academic environments.
Methods
Ethical Considerations
This study was conducted within the framework of the Research Improvement Program of the Research Group on Epidemiology of Mental Disorders, Psychopathology, and Neurosciences. Ethical approval was granted by the Department of Medical Psychology at the School of Medical Sciences, National University of Asunción, Paraguay (Reference 02-2025), in accordance with Resolution No. 0708-00-2022 of the Faculty’s Board of Directors, Article 2, which governs ethical approval procedures for non-experimental studies.
All data was processed in line with the principles of confidentiality, equity, and justice, as set out in the Declaration of Helsinki. Participants (all older than 18 years) provided their written informed consent before joining the survey. Those who expressed interest in receiving individualized feedback from the survey had the opportunity to voluntarily provide an email address to receive personalized information, recommendations, or relevant suggestions. Participants who were found to show significant psychological distress or clinically relevant abnormalities were appropriately referred to university mental health services for further assessment and support. The manuscript follows the STROBE cross-sectional guidelines, which are available as supplementary online material. 19
Study Design
A cross-sectional, observational study with a quantitative approach was conducted. This design enables the description of a population at a specific point in time and the examination of associations between key variables, without implying causal relationships. A cross-sectional approach is particularly suitable for assessing the prevalence of somatic symptoms and their relationship with psychosocial factors among university students, providing a structured initial exploration of this phenomenon in the local context. 20
Population and Sampling
The target population included undergraduate university students. A non-probabilistic convenience sampling method was employed, based on an open invitation extended to students from various academic disciplines. This strategy facilitated the recruitment of a diverse sample across various fields of study, allowing for the analysis of potential differences or shared patterns in somatic symptom expression and associated variables. Inclusion criteria were: (a) being an active undergraduate student, (b) aged 18 years or older, and (c) providing informed consent to participate in the study. Students on academic leave or temporarily withdrawn from their studies were excluded. Additionally, surveys with more than 20% missing responses were discarded to ensure the integrity and reliability of the data.
Data collection was conducted via an online survey, distributed through messaging applications such as WhatsApp and Telegram, as well as institutional emails, between March and June 2025. Before starting the questionnaire, participants were informed about the study’s aims, the voluntary nature of their participation, and the procedures in place to protect their privacy and confidentiality. Written informed consent was obtained electronically from all participants before commencing the survey. Online surveys are a valid and effective method for data collection, yielding results comparable to those obtained through face-to-face methods. 21
Variables
Socio-demographic, academic, and clinical (mental health) variables were defined and collected to characterize the sample and explore associations between somatic symptoms and relevant psychosocial factors.
Socio-demographic Variables
Information was collected on participants’ sex (male, female, other) and age (in completed years).
Academic Variables
Academic variables included students’ field of study (discipline), classified according to the International Standard Classification of Education – Fields of Education and Training 2013 (ISCED-F 2013), the current academic year, and the total number of weekly hours dedicated to study (including both class attendance and independent study time). 21 Participants were also asked whether they were employed (Yes/No).
Clinical and Mental Health Variables
Data were collected using internationally validated, self-administered instruments, selected based on their conceptual relevance, robust psychometric properties, and ability to assess the study’s core constructs: somatic symptoms, academic burnout, perceived stress, anxiety, depression, and insomnia.
Somatic symptoms were assessed using the Patient Health Questionnaire-15 (PHQ-15), a widely validated self-report instrument designed to evaluate the severity of somatic symptom burden over the preceding four weeks. The scale comprises 15 items, though in this study, 14 actively scored items were used, excluding the item on menstrual problems, which is often omitted in gender-mixed samples or when not applicable. Each item reflects the presence and intensity of common somatic complaints (e.g., gastrointestinal discomfort, fatigue, pain, and cardiopulmonary symptoms), rated on a 3-point Likert scale (0 = not bothered at all, 1 = bothered a little, 2 = bothered a lot). Example items include: “Stomach pain” and “Feeling tired or having low energy.” To maintain consistency with the original scoring system, raw scores were proportionally adjusted to reflect the conventional 0–30 range. The PHQ-15 has demonstrated good internal consistency and convergent validity with measures of functional impairment and health care utilization in both clinical and non-clinical populations.22,23 It has been validated in Spanish and in Latin American countries. 23
Academic burnout was evaluated using the Oldenburg Burnout Inventory – Academic Version (OLBI-S), a psychometrically adapted version of the original OLBI tailored for educational settings. The OLBI-S comprises 16 items divided into two theoretically grounded subscales: exhaustion, reflecting emotional and physical fatigue stemming from study demands, and disengagement, indicating cognitive and emotional detachment from academic work. Items are presented in both positively and negatively worded formats to reduce response bias and were recoded according to the instrument’s valence structure, following the guidelines of Reis, Xanthopoulou, and Tsaousis. 9 Example items are: “I feel emotionally drained by my studies” (exhaustion) and “I find it hard to get motivated to study” (disengagement). Responses are given on a 4-point Likert scale ranging from 1 (strongly disagree) to 4 (strongly agree), with higher scores indicating greater burnout. Subscale scores were calculated by averaging responses: disengagement from items 1–8 (with recoding for items 2, 3, 5, and 6), and exhaustion from items 9–16 (with recoding for items 9, 10, 12, and 14). Scores ≥ 2.10 (disengagement) and ≥ 2.25 (exhaustion) were considered indicative of clinically relevant burnout. 24 The OLBI-S has shown robust factorial validity and measurement invariance across student populations, supporting its cross-cultural applicability in educational burnout research. This version adapts the original model by Demerouti et al. for use in university populations and has demonstrated factorial invariance between students and employees, as well as across countries.25,26 The OLBI model has also been applied and previously validated in Paraguayan university students. 27
Perceived stress was assessed using the 10-item Perceived Stress Scale (PSS-10), a widely used self-report instrument developed to measure the degree to which individuals appraise situations in their lives as stressful. The PSS-10 evaluates the frequency of stress-related thoughts and feelings over the past month using a 5-point Likert scale ranging from 0 (never) to 4 (very often). The scale includes both negatively and positively worded items; the latter were reverse-coded to ensure uniform scoring directionality, such that higher total scores reflect greater levels of perceived stress. Sample items include: “In the last month, how often have you felt nervous and stressed?” and “In the last month, how often have you felt confident about your ability to handle personal problems?” (reverse-coded). The PSS-10 has demonstrated strong internal consistency, good construct validity, and cross-cultural reliability in diverse populations, and it is susceptible to changes in psychological stress levels in non-clinical samples.10,11 It has been validated in Spanish and in Latin American countries. 11
Insomnia was assessed using the Insomnia Severity Index (ISI), a 7-item self-report instrument designed to evaluate both the severity and impact of insomnia symptoms over the preceding two weeks. The ISI captures key dimensions of insomnia, including difficulty initiating sleep, maintaining sleep, early morning awakenings, dissatisfaction with sleep quality, interference with daily functioning, distress caused by sleep problems, and the degree to which others notice sleep difficulties. Example items are: “Difficulty falling asleep” and “Problems staying asleep.” Each item is rated on a 5-point Likert scale (0 = no problem to 4 = very severe problem), yielding a total score ranging from 0 to 28. Higher scores indicate greater insomnia severity, with established clinical cutoffs to categorize subthreshold, moderate, and severe insomnia. The ISI has demonstrated excellent internal consistency, test-retest reliability, and convergent validity with both subjective and objective measures of sleep disturbance across clinical and non-clinical populations.14,28 The Spanish version validated by Fernandez-Mendoza et al. was employed. 14
Anxiety and depression were assessed using the PHQ-4, an ultra-brief screener combining items from the GAD-7 (Generalized Anxiety Disorder, for anxiety) and PHQ-9 (for depression). 29 The Spanish version validated in Paraguay by Caycho-Rodríguez et al. was used. 30 The PHQ-4 comprises four items, each rated on a four-point Likert scale (0–3), referring to symptoms experienced in the past two weeks. Items 1–2 represent the anxiety subscale (Generalized Anxiety Disorder-2), and items 3–4 the depression subscale (PHQ-2). Example items include: “Feeling nervous, anxious, or on edge” (anxiety) and “Little interest or pleasure in doing things” (depression). The total score ranges from 0 to 12, with categories of distress: normal (0–2), mild (3–5), moderate (6–8), and severe (9–12). Scores ≥ 3 on either subscale indicate clinically relevant anxiety or depression, respectively.
Participants who were found to show significant psychological distress or clinically relevant abnormalities were appropriately referred to university mental health services for further assessment (according to the diagnostic international criteria [e.g., Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, DSM-5 31 ]) and specific support.
Statistical Analysis
We employed the SPSS Statistics 30.0.0. 32 Descriptive and inferential statistical methods were used. Absolute and relative frequencies were calculated for categorical variables, while means and standard deviations were reported for quantitative variables. Bivariate associations between instrument scores were analyzed using Pearson’s correlation coefficients.
To identify significant predictors of somatic symptoms, a multiple linear regression model was developed with the total PHQ-15 score as the dependent variable. Independent variables included perceived stress (PSS-10), academic burnout (OLBI-S), symptoms of anxiety and depression (PHQ-4), and insomnia (ISI), along with socio-demographic covariates such as age, sex, employment status, and academic workload. Assumptions of normality of residuals, homoscedasticity, multicollinearity (assessed via variance inflation factor, VIF), and linearity were evaluated. VIF values for all predictors ranged between 1.23 and 2.41, all of which were below the commonly accepted threshold of 2.5, confirming the absence of problematic collinearity.
Additionally, a multiple mediation model was tested to explore whether the OLBI-S subscales—exhaustion and disengagement—mediated the relationship between perceived stress (PSS-10) and somatic symptoms (PHQ-15). This analysis was conducted using Model 4 of the PROCESS macro for SPSS, with indirect effects estimated via bootstrapping with 5,000 resamples and 95% confidence intervals.
Comparative analyses were also conducted to examine differences in key variables according to socio-demographic characteristics, including sex, academic year, and employment status. Student’s t-tests and ANOVA were applied for continuous variables, as appropriate.
The effect of academic discipline was included as a covariate in multivariate models. Participants were categorized according to the International Standard Classification of Education – Fields of Education and Training 2013 (ISCED-F 2013), adapted to the study’s context. 33
Sample Size
Sample size was estimated based on the analytical objectives of the study, which included multiple regression analyses, mediation models, and subgroup comparisons across socio-demographic and academic variables. Since the primary aim was to identify predictors of somatic symptoms using regression models adjusted for psychosocial and demographic factors, Cohen’s method was applied to estimate the sample size in correlational and multivariate research. Assuming a small to moderate effect size (f² = 0.10), a significance level of α = 0.05, and a statistical power of 80% (1–β = 0.80), the required sample size was calculated at 172 participants. 34 This was based on a model including up to 10 predictors (perceived stress, academic burnout, insomnia, anxiety, depression, age, sex, academic discipline, academic workload, and employment status), in line with methodological guidelines. 34 The calculation was performed using G*Power software version 3.1.9.7, selecting “F tests – Linear multiple regression: Fixed model, R² deviation from zero.”
Moreover, considering the need for mediation analyses (e.g., testing academic burnout as a mediator between perceived stress and somatic symptoms), adjusted multivariate analyses, and subgroup comparisons (e.g., by sex, employment, and academic year), as well as potential data loss due to incomplete questionnaires, a conservative approach was taken. Therefore, a target minimum sample size of 250 participants was established. This ensured adequate statistical power to detect moderate effects, estimate robust confidence intervals for indirect effects using bootstrapping, and support reliable subgroup analyses. This threshold is consistent with prior studies employing similar methodologies in university populations. 6 The final sample comprised 297 students, exceeding the planned minimum and ensuring sufficient power for all analyses.
Results
Socio-demographic and Academic Characteristics of the Sample
A total of 297 undergraduate students participated in the study, with ages ranging from 18 to 44 years (M = 24, SD = 5). Most participants were women (67.0%), followed by men (32.3%), and a small proportion identified as another gender (0.7%). In terms of field of study, the largest group belonged to Health and Well-being (41.8%), followed by Engineering, Industry, and Construction (14.5%), Arts and Humanities (10.8%), and Social Sciences, Journalism, and Law (8.8%). Regarding academic year, the highest proportion of participants was in their second year (28.3%). A majority (57.2%) reported being employed, either part-time or full-time. Weekly study hours ranged from 1 to 85, with a mean of 20.32 hours (SD = 18.45). Table 1 presents the detailed distribution of the socio-demographic and academic characteristics of the participants.
Socio-demographic and Academic Characteristics of Participants (N = 297).
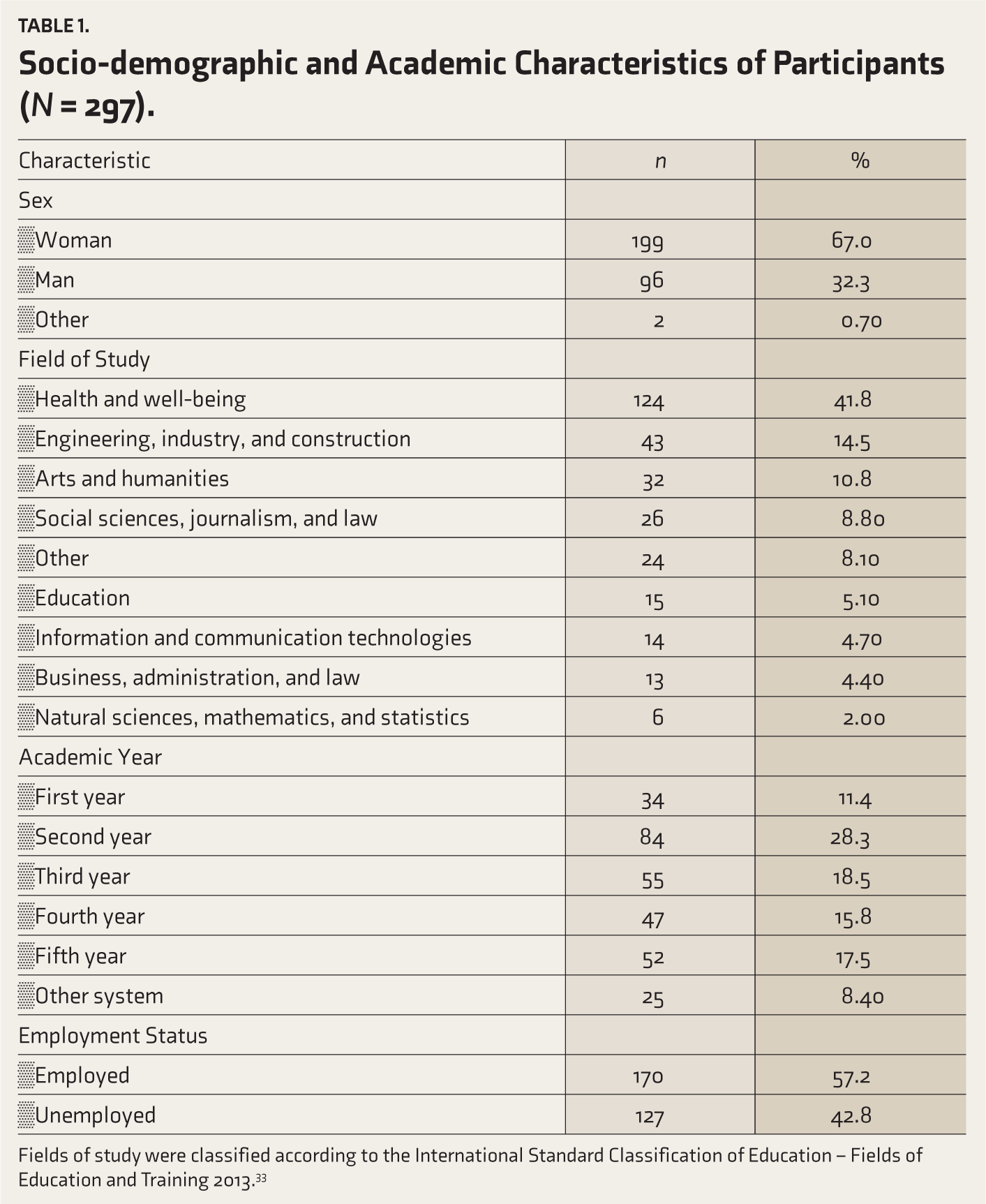
Fields of study were classified according to the International Standard Classification of Education – Fields of Education and Training 2013. 33
Description of Clinical and Mental Health Variables
The mean PHQ-15 score was 13.5 (SD = 5.14), indicating a moderate level of somatic symptoms. For academic burnout, mean scores were 2.22 (SD = 0.47) for disengagement and 2.93 (SD = 0.50) for exhaustion. The mean perceived stress score (PSS-10) was 21.2 (SD = 5.75), the ISI score was 12.1 (SD = 5.28), and the PHQ-4 total score was 5.42 (SD = 2.96).
Based on established cutoffs, 38.7% of participants reported high levels of somatic symptoms, 25.9% experienced elevated perceived stress, 62.3% had clinically relevant disengagement, and 94.9% exhibited clinically significant exhaustion. In terms of sleep, 4.7% met the criteria for severe clinical insomnia. Regarding psychological distress, 17.5% of students showed severe general distress, 58.2% presented anxiety symptoms, and 56.2% showed depressive symptoms. A detailed breakdown of clinical and psychosocial variables, including prevalence rates, is shown in Table 2.
Clinical and Psychosocial Variables of Participants (N = 297).
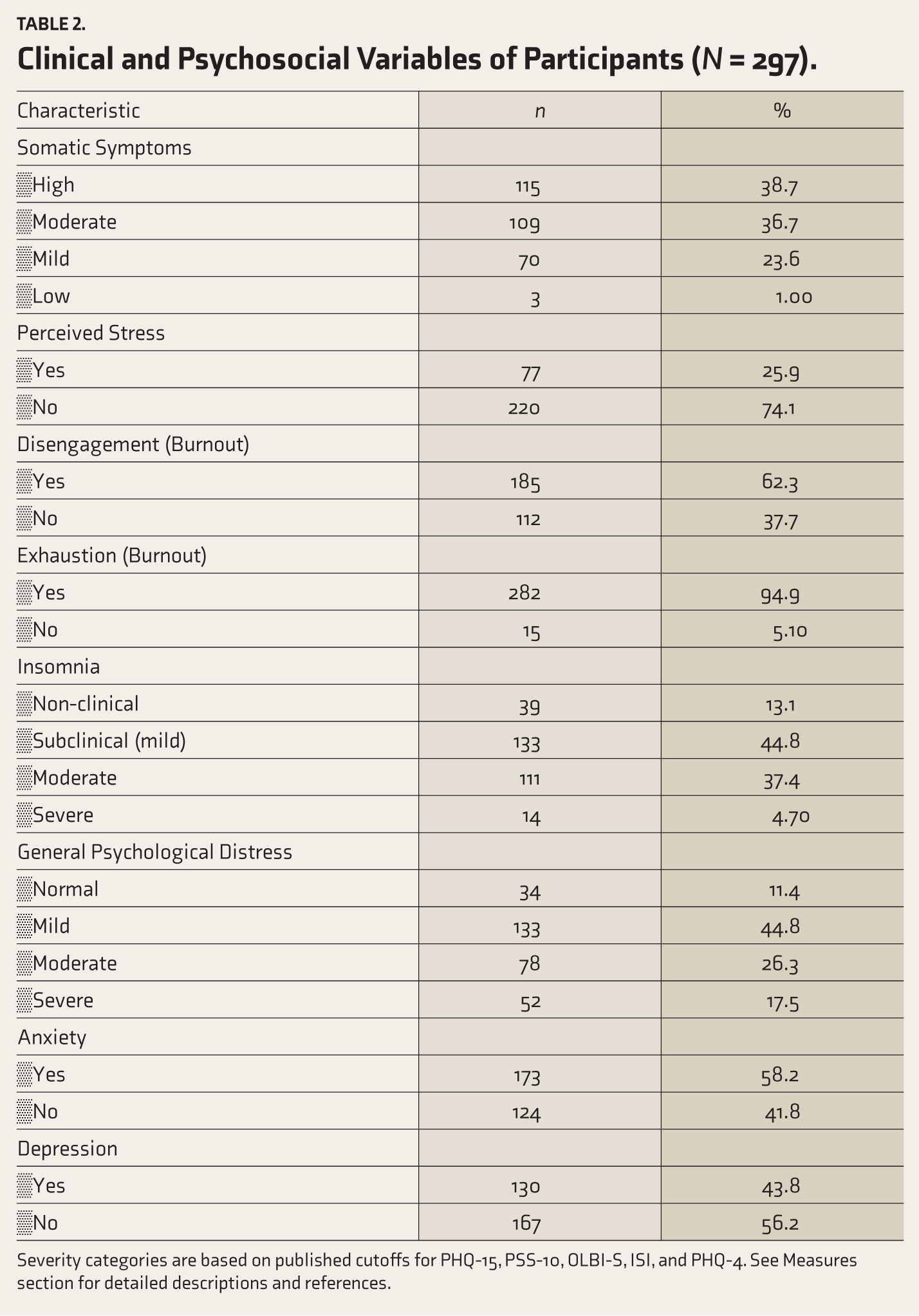
Severity categories are based on published cutoffs for PHQ-15, PSS-10, OLBI-S, ISI, and PHQ-4. See Measures section for detailed descriptions and references.
Bivariate Correlation Analysis Between Clinical and Psychosocial Variables
Pearson correlation coefficients were used to explore the relationships among variables. Results indicated that somatic symptoms (PHQ-15) were positively and significantly correlated with exhaustion (r = 0.30, p < .05), perceived stress (r = 0.36, p < .05), psychological distress (PHQ-4; r = 0.52, p < .05), and insomnia (r = 0.41, p < .05). No significant correlation was found between somatic symptoms and disengagement (r = –0.07, p > .05). These results are detailed in Table 3.
Correlation Matrix Between Clinical and Psychosocial Variables.
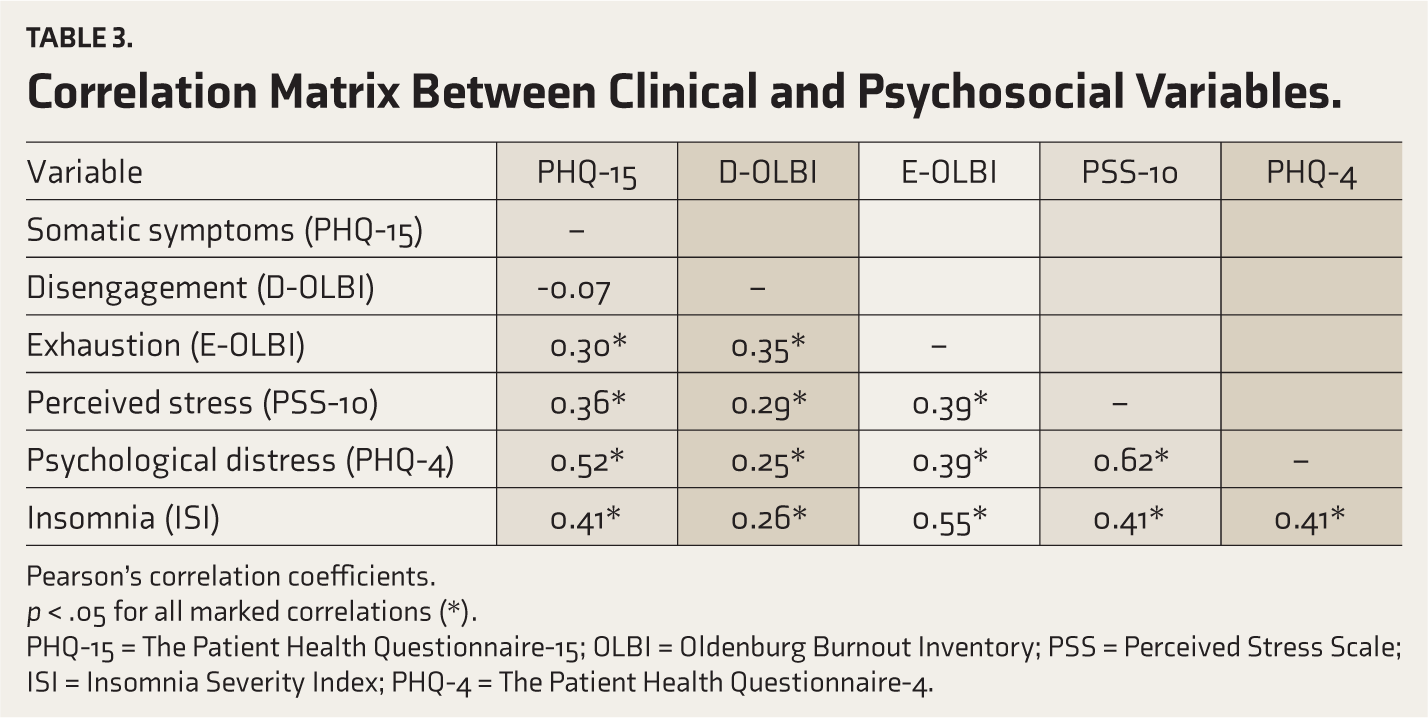
Pearson’s correlation coefficients.
p < .05 for all marked correlations (*).
PHQ-15 = The Patient Health Questionnaire-15; OLBI = Oldenburg Burnout Inventory; PSS = Perceived Stress Scale; ISI = Insomnia Severity Index; PHQ-4 = The Patient Health Questionnaire-4.
Insomnia (ISI) was positively and significantly correlated with disengagement (r = 0.26, p < .05), exhaustion (r = 0.55, p < .05), perceived stress (r = 0.41, p < .05), and psychological distress (r = 0.41, p < .05). In addition, psychological distress (PHQ-4) showed significant correlations with exhaustion (r = 0.39, p < .05), perceived stress (r = 0.62, p < .05), and disengagement (r = 0.25, p < .05). Internal consistency reliability (McDonald’s omega) for the OLBI-S was ω = 0.787 overall, ω = 0.70 for disengagement, and ω = 0.695 for exhaustion. Table 3 presents the correlation matrix between all clinical and psychosocial variables included in the study.
Predictors of Somatic Symptoms: Multiple Regression Analysis
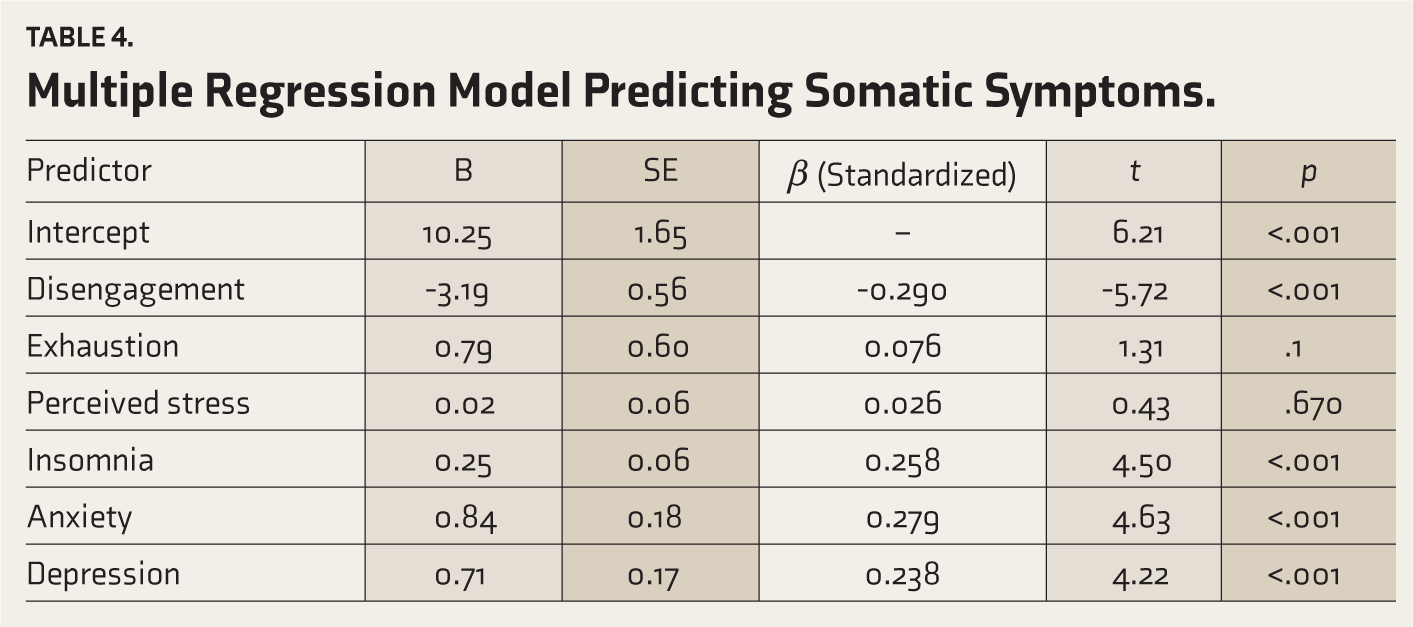
A multiple linear regression analysis was conducted to examine whether disengagement, exhaustion, perceived stress (PSS-10), insomnia (ISI), anxiety, and depression (both measured with the PHQ-4) predicted somatic symptoms (PHQ-15). The model was statistically significant, F(6, 29) = 31.8, p < .001, and explained 39.7% of the variance in somatic symptoms (R² = 0.39; adjusted R² = 0.38). The Durbin-Watson statistics were 1.94, indicating acceptable independence of residuals. VIF values were all below 2.5, suggesting no problematic multicollinearity among predictors. Among the predictors, four variables were statistically significant: disengagement (β = –0.29, p < .001), insomnia (β = 0.25, p < .001), anxiety (β = 0.27, p < .001), and depression (β = 0.23, p < .001). In contrast, exhaustion (β = 0.07, p = .19) and perceived stress (β = 0.02, p = .67) were not significant predictors of somatic symptoms. These findings are detailed in Table 4.
Multiple Regression Model Predicting Somatic Symptoms.
Mediation Analysis
A multiple mediation model was tested in which perceived stress (PSS-10) was examined as a predictor of somatic symptoms (PHQ-15), mediated by the two academic burnout subscales: disengagement and exhaustion (OLBI-S). The analysis was conducted using the PROCESS macro for SPSS (model 4) with 5,000 bootstrap samples.
Results indicated that perceived stress significantly predicted both disengagement (β = 0.023, p < .001) and exhaustion (β = 0.03, p < .001). In addition, perceived stress directly predicted somatic symptoms (β = 0.30, p < .001).
Regarding indirect effects, disengagement showed a significant adverse indirect effect on somatic symptoms (β = –0.07, 95% CI [–0.12, –0.03]), whereas exhaustion had a significant positive indirect effect (β = 0.09, 95% CI [0.05, 0.15]). However, the total indirect effect was not statistically significant (β = 0.02, 95% CI [–0.04, 0.08]) (Table 5).
Multiple Mediation Model: Direct and Indirect Effects of Perceived Stress on Somatic Symptoms Through Academic Burnout (OLBI-S).
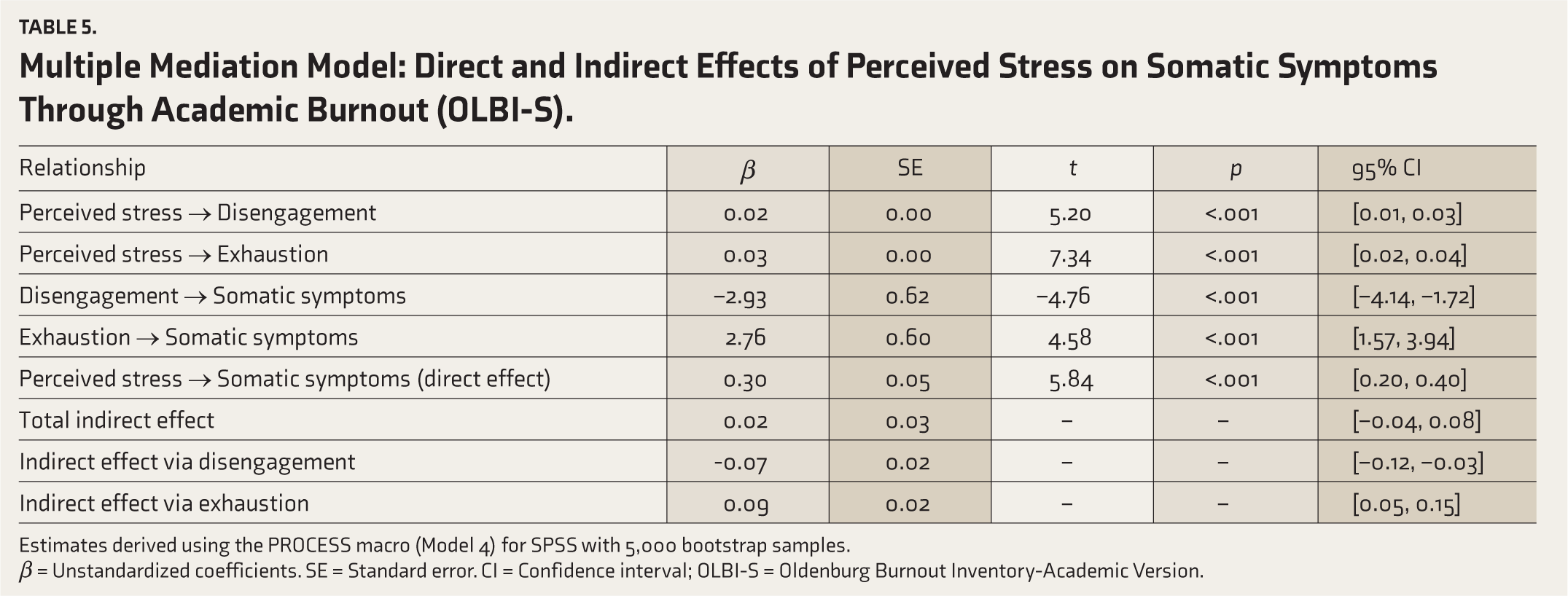
Estimates derived using the PROCESS macro (Model 4) for SPSS with 5,000 bootstrap samples.
β = Unstandardized coefficients. SE = Standard error. CI = Confidence interval; OLBI-S = Oldenburg Burnout Inventory-Academic Version.
These findings suggest contrasting mediating roles of the two burnout dimensions: while disengagement attenuated the association between stress and somatic symptoms, exhaustion intensified it. Additionally, the effect of the academic discipline was controlled, but results indicated that this covariate had no significant effect on the mediators or the outcome (p > .05 in all cases). This suggests that the observed effects of perceived stress on somatic symptoms, both direct and mediated through academic burnout, are consistent across different fields of study.
Comparative Analyses by Socio-demographic Subgroups
Comparative analyses revealed significant differences by sex in disengagement (p < .001), exhaustion (p = .036), and insomnia (p = .046), with men reporting higher scores in all three. Academic discipline was significantly associated with all clinical variables (p < .05): disengagement was highest among students in technology-related fields, exhaustion among students in the natural sciences, perceived stress among students in technology, insomnia among students in technology, anxiety among business students, and depression among science students.
The academic year was associated with disengagement (p = .00) and perceived stress (p = .01). Disengagement was highest among final-year students, while stress was highest among first-year students. Employment status was significantly associated with perceived stress (p = .00), with non-working students reporting higher stress levels.
Somatic symptoms were significantly associated with sex (p < .001), with women exhibiting higher scores; however, no significant associations were found with other socio-demographic variables. These subgroup differences are detailed in Table 6.
Comparisons of Main Variable Scores by Socio-demographic Subgroups (N = 297).
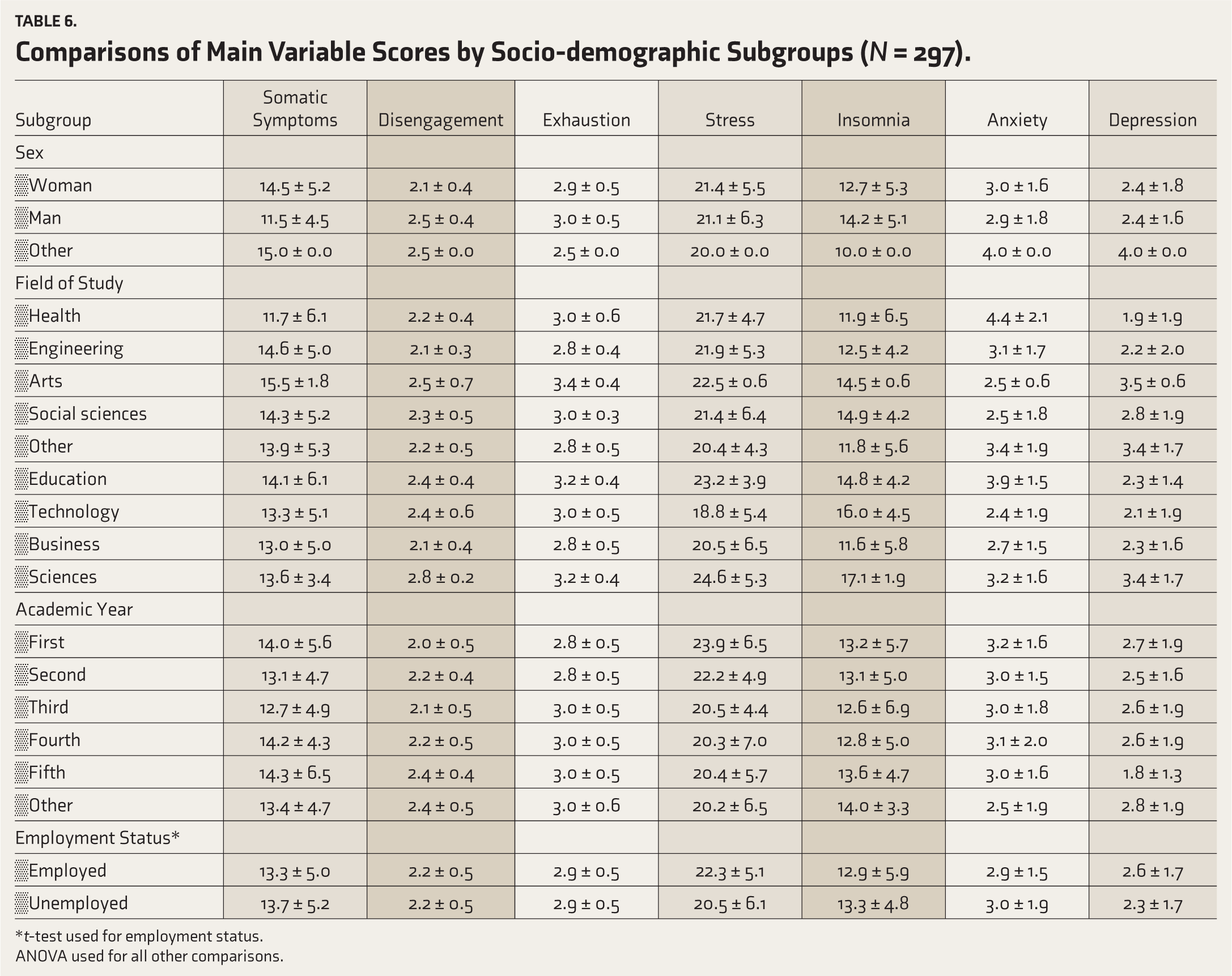
*t-test used for employment status.
ANOVA used for all other comparisons.
Discussion
The high levels of burnout reported in this study are consistent with the broader literature, which emphasizes the psychosocial challenges faced by students. The transition to higher education can generate significant stress due to increased academic demands and expectations, ultimately leading to burnout.17,27 Academic stressors correlate with psychological distress, suggesting that interventions targeting such stressors could improve students’ mental health.
In our sample, more than half of the participants combined studies with work, likely aggravating stress and contributing to the 94.9% rate of exhaustion. The coexistence of multiple stressors may have cumulative detrimental effects, as previous studies highlight the role of institutional factors in shaping student well-being and call for structural reforms to alleviate pressures. 35
Severe insomnia was observed in 4.7% of participants. Given that chronic insomnia impairs attention, memory, and emotion regulation, interventions to improve sleep are essential. A Paraguayan study found that poor sleep before a high-stakes medical exam was associated with worse performance, highlighting the importance of sleep in academic outcomes. 36
Bivariate and regression analyses confirmed strong associations between somatic symptoms and psychological distress (r = 0.52), echoing prior evidence linking anxiety, depression, and somatic complaints. 37 Findings parallel those in healthcare professionals, where depression correlated with somatic symptoms, and in COVID-19 studies, where burnout and distress overlapped with physical manifestations.38,39
By contrast, disengagement showed no bivariate association with somatic symptoms (r = –0.07). This aligns with Sun et al., who argued that burnout can lead to psychological distress without evident somatic symptoms. 40 Insomnia correlated significantly with both exhaustion and disengagement, consistent with prior research on sleep disorders as consequences of burnout.39,40 Insomnia is increasingly recognized not only as a symptom but also as a contributor to psychosocial distress. 41
Regression analysis revealed a suppression effect: disengagement was negatively associated with somatic symptoms (β = –0.29) when anxiety and depression were controlled. This pattern may indicate that disengagement exerts a potential buffering effect on the somatic expression of psychological distress. However, this interpretation remains tentative and would require longitudinal confirmation before firm conclusions can be drawn.42,43 Insomnia also emerged as a robust predictor (β = 0.25), reinforcing evidence that addressing sleep problems can reduce somatic complaints. 44 Our model explained 39.7% of the variance, underlining the explanatory value of psychosocial predictors. Although all VIF values were below 2.5, indicating no problematic multicollinearity, the strong intercorrelations among stress, exhaustion, anxiety, and depression likely attenuated their individual contributions, explaining why stress and exhaustion lost significance in the regression model. Although all VIF values in our models were below 2.5, indicating the absence of problematic multicollinearity, it is essential to acknowledge that the predictors included—such as stress, exhaustion, anxiety, and depression—are conceptually and empirically interrelated. This interdependence may have attenuated the individual regression coefficients despite acceptable VIF values. As Johnston et al. emphasize, low VIF values do not entirely preclude the influence of confounding and collinearity, and therefore, the coefficients observed in our models should be interpreted with caution. 45
Mediation analysis confirmed that stress predicted disengagement and exhaustion. Stress directly predicted somatic symptoms, while disengagement reduced and exhaustion amplified this effect, echoing prior findings on psychological flexibility as a resilience mechanism. 46 These contrasting roles highlight that burnout is not monolithic but has differential pathways through which stress is embodied. Treating burnout as a single construct can therefore be misleading, as exhaustion and disengagement exert distinct and even opposing effects on the relationship between stress and somatic symptoms. However, as the mediation was conducted on cross-sectional data, these findings should be interpreted as exploratory and not as evidence of causal pathways, which require longitudinal confirmation.
Taken together, these results support a biopsychosocial model of somatization. Perceived stress acts as a trigger, insomnia reflects disrupted physiological regulation, and anxiety and depression amplify vulnerability. Burnout functions both as an outcome and as a mechanism that modulates the translation of stress into physical complaints. Thus, the simultaneous inclusion of multiple predictors is theoretically justified as they represent interrelated components of a unified stress–response process.9–12
The lack of a total indirect effect, despite the opposite influences of burnout subdimensions, suggests a complexity in how students cope with stress. Academic discipline showed no significant association, supporting prior evidence that the stress–burnout– distress relationship transcends disciplinary boundaries. 46
Subgroup analyses revealed sex differences, with men reporting higher disengagement, exhaustion, insomnia, and stress; however, Gao et al. suggest that such differences may not always be significant. 47 The gender distribution of our sample was skewed, with women representing the majority of participants. Although gender was statistically controlled as a covariate in the regression analyses, this imbalance may have influenced the overall results and should be considered when interpreting our findings. From a theoretical perspective, gender differences in somatic symptoms are well documented, with women more frequently reporting somatic complaints than men. 48 Such disparities may reflect a combination of biological vulnerability, psychological processes such as emotion regulation, and sociocultural influences on symptom expression and reporting. Future research should aim for more gender-balanced samples to clarify further the role of sex and gender in the manifestation of somatic symptoms. 48
Beyond sex-related differences, our analyses also revealed disciplinary patterns. Specifically, science students reported greater exhaustion, whereas technology students showed higher levels of insomnia, which aligns with previous evidence suggesting that demanding academic fields impose heavier psychological burdens. 49 Academic transitions also mattered: final-year students showed greater disengagement, while first-year students reported higher stress, supporting frameworks on transitional vulnerability. 50 Employment status further shaped outcomes, with non-working students reporting higher stress, likely reflecting financial insecurity and lack of structured routine. 50 Malakcioglu similarly noted that unemployment during university years increases distress due to economic uncertainty. 51
Strengths and Limitations
This study assessed multiple psychosocial and clinical factors using validated instruments, and mediation analysis added theoretical value. The large, heterogeneous sample enhances external validity and provides novel data for a relatively unexplored Latin American population. However, the cross-sectional design precludes causal inference, and online self-report questionnaires may introduce bias. Convenience sampling limits generalizability, and variables such as social support, academic performance, or psychiatric history were not assessed. In addition, the exceptionally high prevalence of exhaustion observed in this sample (94.9%) should be interpreted cautiously, as it may reflect sample-specific characteristics rather than broader population trends, further limiting generalizability. As all data were obtained via self-report questionnaires, the potential influence of Common Method Bias (CMB) cannot be entirely ruled out. While the use of validated instruments and scales with both positively and negatively worded items helps mitigate this risk, and the divergent effects observed across burnout subcomponents (e.g., exhaustion amplifying while disengagement attenuated the stress–somatic symptom association) argue against a single-method artifact, the absence of a formal statistical test remains a limitation. Future studies should incorporate specific procedures to assess CMB, such as Harman’s single-factor test or confirmatory factor analysis with a marker variable, to further strengthen methodological rigor.
Implications for Policy and Practice
The high prevalence of burnout, distress, and somatic symptoms highlights the need for systemic interventions in universities. Strategies should include counseling, sleep education, stress management, and peer support. Notably, interventions should differentiate between exhaustion and disengagement rather than treating burnout as a unitary construct. Organizational flexibility, autonomy, and workload reduction may help mitigate stress. Gender-sensitive approaches are also essential, given observed disparities.
Future Directions
Longitudinal studies are necessary to investigate the bidirectional relationships between stress, burnout, sleep disturbances, and somatic symptoms. Qualitative approaches could enrich the understanding of coping strategies. Cross-cultural comparisons within Latin America would clarify contextual influences. Evaluating digital interventions for stress and sleep management, resilience training, and integrating biomarkers of stress could further advance multidimensional assessments of student well-being. In addition, while the predictors examined in this study were primarily psychological, future research should adopt a broader biopsychosocial perspective. Specifically, the inclusion of biological markers (e.g., inflammatory processes, neuroendocrine functioning) and social determinants (e.g., socioeconomic status, family context, institutional and peer support) would provide a more holistic understanding of somatic symptoms in university students. Such integration may enable the development of interventions that more effectively address the complex interplay of biological, psychological, and social factors influencing student well-being.
Conclusions
This study highlights the complex interplay between perceived stress, burnout, insomnia, anxiety, depression, and somatic symptoms in Paraguayan university students. Exhaustion and insomnia emerged as key contributors, while disengagement may buffer somatic distress. These findings underscore the importance of multidimensional, context-sensitive strategies for promoting student mental health in middle-income countries.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Data Sharing Statement
De-identified individual participant data, together with the study protocol, statistical analysis plan, and informed-consent form, will be available for six months following publication upon reasonable request to the first author. Data will be shared with researchers who submit a methodologically sound proposal consistent with the study’s approved objectives. Requests should be directed to
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Ethical Approval
This study was conducted within the framework of the Research Improvement Program of the Research Group on Epidemiology of Mental Disorders, Psychopathology, and Neurosciences. Ethical approval was granted by the Department of Medical Psychology, School of Medical Sciences, National University of Asunción, Paraguay (Reference 02-2025), in accordance with Resolution No. 0708-00-2022 of the Faculty’s Board of Directors, Article 2, which governs ethical approval procedures for non-experimental studies. Date of Approval: 3 April 2025.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Participants provided written informed consent and assent prior to enrollment. All data were handled in accordance with the principles of confidentiality, equity, and justice set out in the Declaration of Helsinki. Participants who wished to receive individual feedback could voluntarily provide an email address to obtain personalized information or recommendations.
Registration
Registration on PROSPERO or other platforms was not required, in line with Resolution No. 0708-00-2022 of the Faculty’s Board of Directors, Article 2, which governs ethical approval procedures for non-experimental studies.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.