
Abstract
Keywords
Specific learning disabilities (SLD) encompass difficulties with accurate and/or fluent word recognition and/or spelling, which are often inconsistent with other cognitive skills and hinder the student’s effective engagement in the classroom. 1 The invisible nature of SLD presents significant challenges, exposing students with these disabilities to stigma and peer bullying, which can result in low self-esteem, anxiety, and depression.2–3 The hidden nature, therefore, influences educational outcomes and has substantial implications for the student’s mental health and overall well-being. 4
In India, SLD were officially recognized as a disability for the first time under the Rights of Persons with Disabilities (RPwD) Act of 2016, 5 which expanded the total recognized disabilities from 7 to 21. The act established a comprehensive legislative framework, with operational directions issued by the Department of Empowerment of Persons with Disabilities through a notification in the Gazette of India, Extraordinary. The Gazette notification serves as the official and legal documentation of the legislative amendment. This document is crucial for enhancing transparency and providing a legal basis for the administrative and judicial process of the RPwD Act. The document outlines procedures for identification, assessment, certification, and accommodations for persons with disabilities. The most recent Gazette of India, Extraordinary, was published on 12 March 2024. This article references the Gazette of India: Extraordinary (hereafter referred to as Gazette), Part II-Section 3(ii), specifically Section B: Specific learning disability (pp. 491–495), which outlines the official guidelines and diagnostic framework for SLD. 6
Based on this Gazette notification, the Central Board of Secondary Education (CBSE) issues directives to schools recognized under its authority to implement the RPwD Act within their premises. In accordance with the Gazette notification, the CBSE also formulates examination byelaws and circulates official guidelines, thereby implementing these provisions within its academic settings. These regulations establish the legal basis for school admissions and offer examination-related accommodations, such as extended time, scribes, and exemptions from specific subjects. 7
In this article, the authors draw on over a decade of experience working with students with SLD to critically examine ambiguities and contradictions in the Gazette that hinder accurate SLD diagnosis. The first author is a Rehabilitation Council of India–certified Clinical Psychologist Associate, and the second is a researcher in inclusive education. In this article, the authors underscore the need for immediate clarity and alignment of the guidelines with global best practices.
Discussion
Global diagnostic criteria, including the Diagnostic and Statistical Manual of Mental Disorders (DSM-5-TR) published by the American Psychiatric Association (2022),
8
and the International Classification of Diseases (ICD-11) developed by the World Health Organization (2019; implemented in 2022),
9
explicitly require that intellectual disability (ID) be ruled out before diagnosing SLD. This makes standardized cognitive assessments essential, as they estimate intellectual functioning through intelligence quotient (IQ) scores. Standardized tests evaluate human intelligence and categorize individuals based on their IQ.
10
The following IQ ranges represent psychometric classifications used in standardized intelligence testing:
130 +: Very superior 120–129: Superior 110–119: High average 90–109: Average 80–89: Low average 70–79: Borderline 69 and below: Extremely low.
These ranges, derived from psychometric scales such as the Wechsler tests, 10 serve as statistical reference points for describing cognitive functioning and do not constitute diagnostic categories. The borderline IQ range (70–79), therefore, represents a non-diagnostic statistical category, rather than a clinical or legal classification. 8 The Gazette functionally excludes students with an IQ range of 70–85, thereby omitting both the borderline (70–79 IQ) and low average range (80–85 IQ) from its diagnostic classifications.
The DSM-5-TR 8 explicitly identifies, and the ICD-11 9 recognizes, this category as borderline intellectual functioning (BIF). BIF is a descriptive, non-diagnostic category used in psychiatry, psychology, and special education to indicate IQ scores generally falling within the 70–85 range, although some test manuals may specify a range of 71–84. In the DSM-5-TR, it is classified as a V-code, indicating that these students require intervention but are not categorized as having disabilities. The BIF identifies individuals with intellectual abilities that are below average but who do not meet the criteria for ID, acknowledging the considerable challenges they may encounter in education, employment, and daily life.11,12 The ICD-11 identifies BIF as separate from ID. Importantly, ICD-11 does not identify BIF solely on the basis of IQ; functional impairment must also be demonstrated.
India relies on diagnostic frameworks recognized under the Mental Healthcare Act, 2017. 13 The 2024 Gazette notification relies on earlier ICDs, despite the release of ICD-11 in 2022, and is grounded in the outdated discrepancy model of SLD assessment. This model posits that a diagnosis of SLD occurs when a student has an IQ > 85 but performs significantly below expected standards in one or more specific academic areas, such as reading, writing, or mathematics. 14 According to the Gazette, a student is diagnosed with ID if their IQ is 69 or below, 15 and with SLD if their IQ is 86 or above and they exhibit significant literacy challenges. As a result, students in the 70–85 IQ range fall outside both categories, making them invisible twice. The exclusion situates them in a diagnostic and policy blind spot, thereby denying them access to formal support services. This exclusionary policy approach is problematic, as students within this IQ range frequently encounter functional impairments in reading, writing, and mathematical reasoning that are comparable to, or even exceed, those of their peers with higher IQs who have been diagnosed with SLD. 16 However, their difficulties stem from global cognitive limitations, not specific neurocognitive deficits as required for SLD.
The widespread use of the IQ achievement discrepancy criteria in the United States emerged from the Individuals with Disabilities Education Act (IDEA), 17 which permitted (and in practice encouraged) schools to identify students with SLD based on a significant discrepancy between intellectual ability and academic achievement, even though IDEA never mandated a specific IQ cut-off. Neurobiological and cognitive research conducted in the 1990s challenged this approach, highlighting that these disorders are associated with atypical neurocognitive pathways, including altered brain connectivity within reading and/or arithmetic networks, and cannot be attributed solely to general intelligence. These findings led to revisions to IDEA, removing the necessity for the discrepancy model. Current diagnostic frameworks emphasize that the diagnosis of SLD should be based on enduring academic deficits rather than a predetermined IQ threshold, provided that global ID (IQ < 70) has been excluded.
The most recent DSM-5-TR and ICD-11 incorporate the above-mentioned principles in their diagnostic frameworks for SLD. Unfortunately, the Gazette has not been updated accordingly, resulting in students with BIF who exhibit clear learning challenges continuing to be marginalized by policy. This lack of recognition of the group’s learning difficulties as clinically significant or worthy of institutional support contributes to their exclusion and neglect within the educational framework.
Although BIF and SLD are conceptually distinct, BIF is characterized by global cognitive limitations and associated challenges to adaptive functioning. In contrast, SLD reflects domain-specific learning difficulties in the context of otherwise average intellectual ability. Students with BIF are often unable to access appropriate accommodations within current policy frameworks because it is not formally recognized as a diagnosable disability category. This distinction is crucial, as academic underperformance in BIF arises from diffuse cognitive vulnerability, rather than isolated neurocognitive deficits characteristic of SLD.
Because the cognitive and functional profile of BIF falls between that of ID and SLD, students with BIF cannot be subsumed under either category to obtain accommodations, given the strict diagnostic and eligibility thresholds defining both conditions. As a result, despite precise educational and support needs, this group continues to lack an appropriate pathway to access support, underscoring the urgent need for formal recognition and policy alignment to ensure equitable service provision. Additionally, there are significant discrepancies both within and between official documents that further exacerbate this exclusion.
Inconsistencies Within and Between Documents
The Gazette exhibits a notable inconsistency in the presentation of IQ thresholds for diagnosing SLD. According to the Gazette (p. 492), Section B: SLD, Step 2 of the SLD diagnostic criteria states that “If IQ is determined to be ‘more than 85’, then Step 3 will be applied.” Step 3 indicates that “a diagnosis of specific learning disability will be given if all of the following criteria are fulfilled.” The first criterion listed states, “IQ 85 or more.” The Gazette, in Step 2, states an IQ of more than 85, whereas Criterion 1 of Step 3 specifies 85 as inclusive. The ambiguity surrounding the consideration of a student scoring 85 for SLD results in inconsistencies in establishing a definitive cut-off point.
Added to this, as can be seen in Figure 1 below, the diagnostic flowchart indicates that if a student’s “IQ is < 85,” then the student is “not SLD, consider workup for ID” (p. 495). According to DSM-5-TR 8 and ICD-11 9 diagnostic criteria, ID is diagnosed when IQ is 70 or below (along with impairment in adaptive function), rather than when it is less than or equal to 85, as indicated in the flow chart. This effectively expands the ID referral range far beyond internationally accepted standards (DSM-5-TR and ICD-11).
Screenshot of the Diagnostic Flowchart on Page 495 of the Gazette. 6
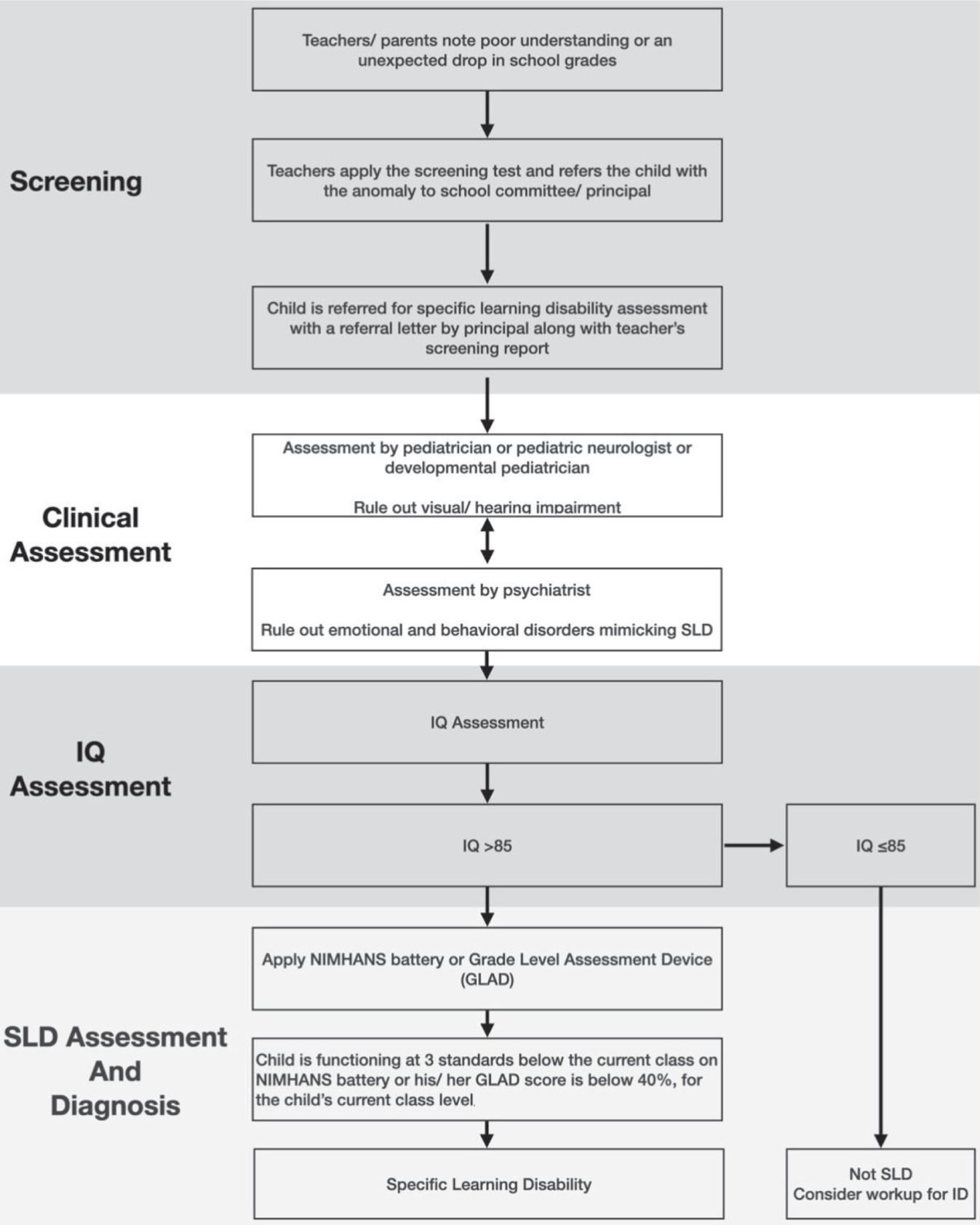
This significant shift from an IQ < 85 to 69 further disregards students with IQs between 70 and 85, effectively placing them also in the diagnostic void, where they are excluded from both SLD and ID categories. The document, therefore, constructs a contradictory and clinically difficult-to-justify system, one that establishes a paradoxical set of “rewards” and “penalties” contingent upon a student’s position on the IQ continuum.
Further, according to the diagnostic criteria outlined in DSM-5-TR and ICD-11, an ID diagnosis necessitates an IQ of 70 or lower, rather than 85. An unexpected decline in academic performance, rather than IQ thresholds alone, is central to identifying SLD as defined in DSM-5-TR and ICD-11, which locate SLDs within the context of adequate intellectual functioning. However, the Gazette’s wording “not SLD, consider workup for ID” has the potential to cause confusion or misinterpretation. As a statutory instrument, the Gazette is expected to provide unambiguous guidance, ensuring that clinicians across all levels of experience arrive at a consistent understanding of both clinical and administrative matters. Moreover, ambiguous phrasing in official policy documents, particularly when addressing relatively newer diagnostic categories such as SLD, may inadvertently reinforce outdated IQ-centric assumptions that DSM-5-TR and ICD-11 discourage, thereby perpetuating historical conceptual confusion and undermining appropriate identification and evaluation.
Further analysis of the National Institute of Mental Health and Neuro Sciences (NIMHANS) SLD test battery, referenced on page 492 of the Gazette as a mandatory diagnostic tool for the legal recognition of SLD in India, reveals additional discrepancies. Page 100 of the NIMHANS SLD manual specifies that individuals with “IQ 85 and above” qualify for this test, referencing the 2018 Mental Health Gazette, which clearly states the criterion as “IQ more than 85.” The continued use of both thresholds (≥85 and >85) across editions of the NIMHANS manual indicates a persistent conceptual error. Furthermore, despite multiple searches, no publicly accessible document titled “Mental Healthcare Gazette, 2018” was located. The conclusion is that the reference was intended to the Gazette extraordinary, 2018.
The distinction between “>85” and “≥85” may seem minor at first glance; however, it has substantial practical implications. Defining the threshold as “more than 85” excludes students with an IQ score of exactly 85 from eligibility for an SLD diagnosis, thereby limiting the number of students who can obtain formal recognition and intervention. This single-point ambiguity has the potential to lead to widespread misclassification and inconsistent eligibility decisions across states and institutions.
This ambiguity in the language and recommendations presents a challenge for clinical and rehabilitation psychologists. They are frequently compelled to reevaluate established diagnostic criteria due to the Gazette’s inconsistency and inaccurate recommendations. The primary aim of any policy document is to reduce confusion, eliminate inconsistencies, and establish a reliable, clinically sound reference point that upholds a high national professional standard. The inconsistency in the Gazette signifies more than a mere semantic concern; it illustrates how the language of policy can significantly influence diagnostic results and the availability of accommodations. These errors in the Gazette permit excessive, arbitrary interpretation, undermining the fundamental purpose of a standardized document. This oversight is not merely technical; it carries ethical, moral, and legal implications, as it fails to provide recognition, support, and accommodations to a vulnerable group of students who require structured educational interventions.
Distinction Between Disability Certification and Examination Concession Certification for Students with SLD
An official disability certificate, along with a Unique Disability ID (UDID) card, provides access to education and job reservations, travel discounts, tax exemptions, and subsidized loans or grants in India. Disability certification thus functions as a central administrative mechanism through which access to state-supported benefits and accommodations is regulated.
In practice, BIF is typically assigned a disability percentage of 25%, for which a UDID card may be issued. However, as this falls below the 40% benchmark for disability, it does not qualify for benefits under the RPwD Act. 5 While major statutory benefits are linked to the benchmark threshold, holding a UDID card or certificate may still facilitate access to some limited or discretionary facilities. These certification thresholds, therefore, shape the administrative context in which educational accommodations, such as examination-related support, are sought.
The Gazette specifies that only government hospitals or centers may diagnose and certify students with SLD through government medical boards comprising specialists, pediatricians, psychiatrists, and clinical or rehabilitation psychologists. Government hospitals in India are already overburdened with the responsibility of certifying multiple other recognized disabilities, and their existing infrastructure remains inadequate to meet the volume of required assessments. 18 Disability certification has direct implications for government spending, administrative capacity, and resource allocation. This understandably warrants government regulatory caution.
Similar to other disabilities, an SLD diagnosis could lead to lifelong certification, increasing permanent beneficiaries, and placing pressure on the welfare system. This has implications for fiscal and logistical sustainability, diverting resources from more potentially debilitating disabilities. Relaxing diagnostic criteria without safeguards could unintentionally increase eligibility and economic and administrative costs.
At the same time, SLD typically does not impair overall functioning but primarily affects academic performance. Students with SLD typically require additional exam time, subject exemptions, or scribes. Unlike students with ID or autism, many with SLD may not need employment, taxation, or travel concessions across the life course. Notably, the Gazette does not explicitly mandate the possession of a UDID card as a prerequisite for availing examination concessions. However, in practice, schools and educational boards often require a UDID card, reflecting an institutional misunderstanding rather than the stated policy.
The consequences of this misinterpretation are significant. The wait time in mandated government hospitals is long. Moreover, several hospitals insist on a UDID card before approving examination concession letters. As a result, students are trapped in a bureaucratic loop, unable to obtain timely diagnoses and necessary accommodations. This disjunction between policy intent and institutional practice further exacerbates the exclusion of students whose needs are time-sensitive and context-specific, undermining the purpose of both certification and accommodation frameworks.
Students with SLD can benefit from appropriate examination accommodations, progress to higher education, and become productive members of society without depending on a UDID-based certification. Many nations employ a differentiated framework for learning disabilities. Students with dyslexia or similar conditions in the United Kingdom, under the Cambridge Assessment International Education, may receive “access arrangements” such as extra time or modified papers. 19 These are approved for specific educational levels and require reassessment every four years, and do not result in a lifelong disability status. The Singapore Examinations and Assessment Board offers access arrangements for students with special educational needs, including learning disabilities. 20 Accommodations include more time, separate rooms, larger print, and exam exemptions for specific components. These models demonstrate that appropriate educational accommodations can be implemented while preserving long-term benefits for persons with enduring functional challenges.
The Way Forward
The discussion above highlights critical gaps in current policy and practice, including the lack of recognition of BIF, inconsistencies both within and across official documents, and the misalignment between disability certification and examination concessions. These challenges collectively underscore the urgent need for greater conceptual clarity, systemic coherence, and alignment with global best practices.
The legal IQ threshold does not align with the functional needs of many students. The IQ cut-off specified in the Gazette is grounded in a medical model of disability, which locates the source of difficulty within the individual. Consequently, access to educational accommodations is deferred until a formal diagnostic assessment is completed. This approach places greater emphasis on identifying causal factors than on providing timely, practical interventions that could offer meaningful support to students. 21 In contrast, the social model of disability locates disability within the external barriers that restrict an individual’s full participation in educational and social environments. This perspective adopts a more learner-centered approach, emphasizing the need to modify structures, practices, and resources to enhance accessibility. In the Indian context, the principles of the RPwD Act and the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) are inconsistently and only partially implemented on a few occasions. 22
Even when examined strictly in the context of supporting students with BIF, the diagnostic manuals clearly articulate the need for assistance. The DSM-5-TR acknowledges BIF as a condition that may require support, while the ICD-11 emphasizes the importance of adaptive functioning and contextual assessment. Unfortunately, such support remains inaccessible unless the student meets the formal criteria for a disability diagnosis. Therefore, in addition to relying on a diagnostic and medically oriented framework, it is essential to incorporate the values of inclusion and equity to ensure that this deserving yet often invisible group receives the support it needs. The government must update diagnostic and certification standards to recognize SLD and BIF in line with contemporary research and global best practices, and honor National Education Policy (NEP) 2020 and the RPwD Act, 2016.
If the government wants to use the discrepancy model, it should recognize BIF as a standalone diagnosis eligible for examination concessions, as the Council for the Indian School Certificate Examinations does for the Indian Certificate of Secondary Education and the Indian School Certificate examinations in its revised Guidelines for Comprehensive Support Measures in Examinations. 23 This demonstrates that an Indian school board has already operationalized a model that acknowledges functional limitations even in the absence of a formal disability category. This example also highlights that stakeholders can collaborate to align policies with the needs of students with disabilities while maintaining best practices and adapting to students’ requirements.
Such policy alignment finds support at the global level. The Girona Declaration on BIF proposes BIF as a health meta-condition rather than a mere statistical IQ label, based on a combination of borderline cognitive abilities (typically IQ 71–85) plus demonstrable limitations in adaptive functioning across academic, social, and occupational domains. 24 It calls for formal recognition, establishment of clear diagnostic criteria that emphasize adaptive functioning (not IQ alone), integration within neurodevelopmental classification frameworks, and the provision of appropriate support services. Importantly, it also clarifies that individuals with borderline IQ scores who do not exhibit functional impairments should not be classified under BIF, thereby addressing risks of over-identification and misclassification.
A government notification of this stature must be airtight. To clarify SLD diagnosis criteria, legislation documents, and diagnostic manuals should be made internally consistent and aligned. This includes clearly distinguishing BIF-related learning difficulties (stemming from global cognitive and adaptive limitations) and SLD (characterized by domain-specific deficits despite average cognitive ability). Without such clarity, there is a real risk of misclassification and inappropriate denial of accommodations.
The government can issue two types of certificates. The first type, an Examination Concession Certificate (Temporary), would be provided for accommodation in school board or competitive exams and will be valid for a fixed period (e.g., until formal schooling is completed). This certificate will not automatically make a holder eligible for permanent benefits under the RPwD Act. The second type, a Lifelong Disability Certificate (Permanent), should only be issued if SLD significantly affects daily life beyond education and requires ongoing accommodations for adults.
Conclusions
The lack of updates in the Indian Gazette affects many vulnerable students with disabilities who feel despondent and helpless. From a policy perspective, the cloak of invisibility surrounding this population is difficult to justify ethically and morally. It contradicts the inclusive ethos of the NEP 2020, 25 the RPwD Act 2016, 5 and the UNCRPD, 26 which emphasize non-discrimination and equal access to education. Attention must be paid to the underlying disjuncture between policy definitions and individuals’ practical support needs.
Footnotes
Note
All opinions expressed in this manuscript are solely those of the authors and do not represent the official stance of the Indian Psychiatric Society—South Zonal Branch, the Editorial Board, or the publisher of the journal.
Data Sharing Statements
This is not an empirical study, and there has been no data collection undertaken for this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethics Committee Details
The submitted manuscript is for “Viewpoint” and is a commentary on the identification procedures. It has not involved any research sample at all.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Prior Presentations
Not applicable.
PROSPERO/CTRI Details
Nil
Registration
Not applicable to this manuscript.
Trial registry name URL Registration number
Simultaneous Submission to Another Journal or Resource
This manuscript has not been submitted anywhere else.
Status of Your Study (for Study Protocol)
The present manuscript is a commentary on the Gazette.