
Abstract

Dear Editor,
Community-based mental health research (CBMHR) is crucial for understanding community mental health (MH) issues and their determinants, as well as the characteristics of interventions to address them. Conducting CBMHR, however, is challenging, especially when the target population is non-help-seeking or non-clinical. This challenge may stem from potential service users prioritizing other life pursuits (i.e., employment, family, finances) over MH, lack of MH awareness, logistical issues in availing services, and poor treatment adherence (pharmacological or non-pharmacological).1–3
We undertook field research as part of the Indian Council of Medical Research (ICMR)-funded study on the feasibility of delivering psychosocial interventions and their effectiveness for sub-clinical common mental disorders in the community, following a randomized controlled trial design. Here, we had to sensitize the target population for our research, engage them through recruitment and interventions, and solicit support from community stakeholders and healthcare workers who are routinely involved in care delivery and are well-networked within the community. During our field experience, we encountered several systemic, cultural, logistical, and training-related bottlenecks that hindered the flow of our study. Therefore, to systematically analyze the bottlenecks and determine the future course of action, we conducted a Strengths, Weaknesses, Opportunities, Threats (SWOT) analysis of the situation.
There is limited literature from India as to challenges in conducting CBMHR in the area of preventive psychiatry, involving non-clinical and non-help-seeking populations for the common MH issues (such as depression, anxiety, and stress) and how to address them. Therefore, we intended to report our experience to inform researchers, clinicians, and policymakers involved in, or embarking on, this field. This research work has been reported as per the LETter To the EditoR Standards (LETTERS) 4 (Supplementary File 1).
Discussion
We faced challenges in limited public transport to reach remote areas for fieldwork, limited budgetary allocation to cover private travel expenses to the community, and mobilizing participants for the research, who were often not formally educated and had difficulty identifying their MH needs. Our concerns was echoed in an other literature in this area from India, focusing on medical undergraduates’ CBMHR. 1 The above challenges were compounded by inadequate engagement of community health officers, either because of parallel commitments that limit their support for the research or because of hesitancy to provide any help, as also evidenced in the literature from Asia.2,5
Additionally, we experienced systemic barriers like health infrastructural constraints, for example, a lack of private space to conduct assessments, well-lit & ventilated rooms, furniture, internet connectivity, and unavailability of prompt stationery facilities for Information, Education, and Communication activities as and when needed in the health facility.
Cultural factors such as service users’ limited interest in discussing MH issues, prioritizing socio-cultural or household events over MH assessment or interventions, cultural beliefs not promoting or supporting MH-related help-seeking, and undervaluation of promotive and preventive services, particularly when community members perceive common MH issues (depression, anxiety, stress) as a part of their daily hassles. We also observed the potential service users’ dependency on their partner/family, particularly in females. Additionally, a pervasive reliance on pharmacological treatment, so-called “pills” for the perceived MH issues, vis-à-vis psychosocial interventions or counseling, was observed, which would merely be perceived as some casual conversation. These issues reflect logistic issues with frequently accessing the MH services, poor MH literacy among the individuals with MH issues and key decision makers of the family, and community members’ lack of psychological mindedness to undergo non-pharmacological interventions.
Therefore, to better understand the situation, we undertook a comprehensive SWOT analysis, an effective yet underutilized tool in CMHR.3,6 This framework enabled us to critically evaluate our position and develop targeted strategies to enhance appeal, acceptability, and smooth implementation of our research work, including MH assessment and intervention delivery (Table 1).
SWOT Analysis Field Challenges in Conducting Community-based Mental Health Research.
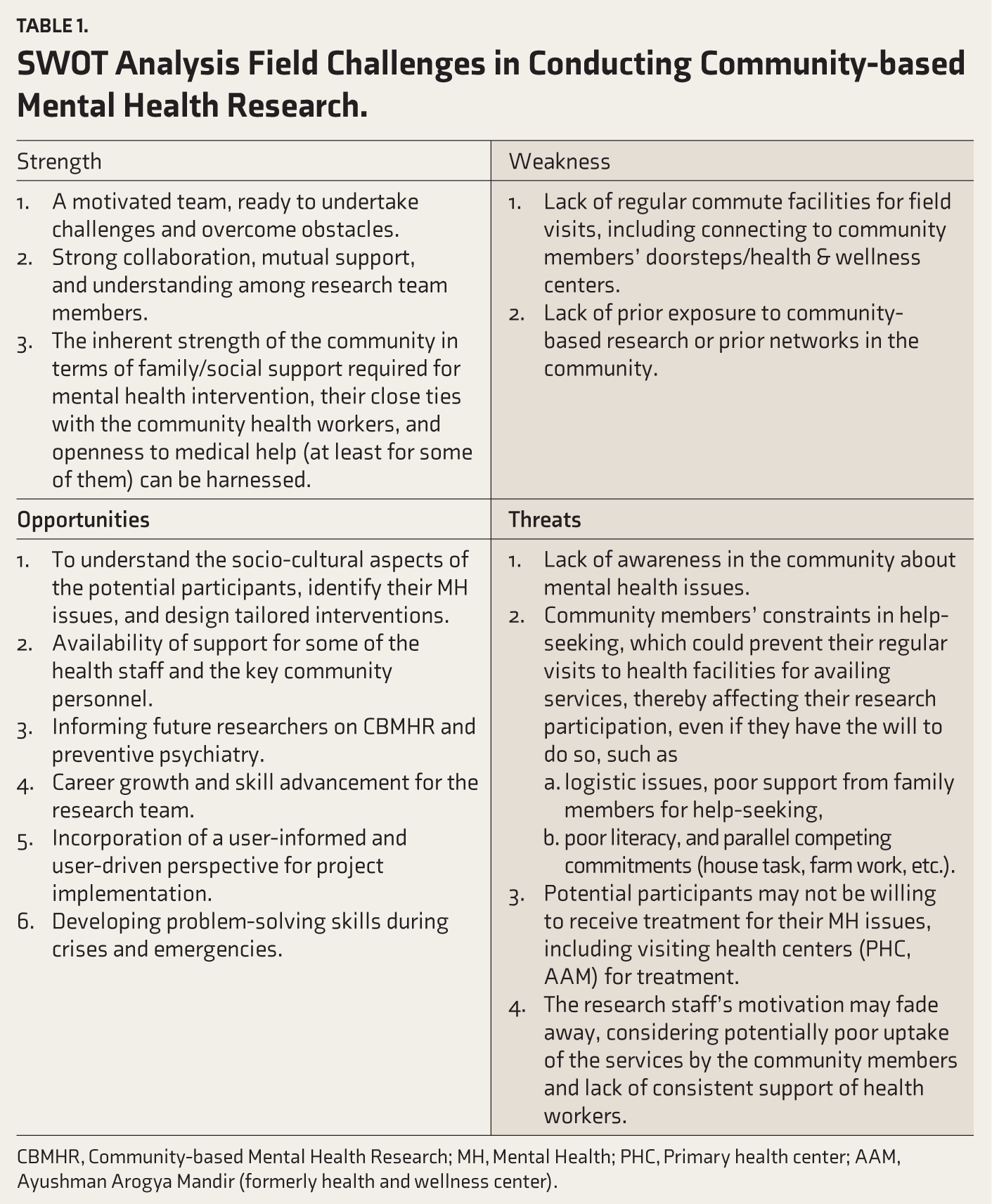
CBMHR, Community-based Mental Health Research; MH, Mental Health; PHC, Primary health center; AAM, Ayushman Arogya Mandir (formerly health and wellness center).
Conducting a SWOT analysis provided us with valuable insights into the local population’s prevalent health issues, socio-cultural and educational characteristics, the availability of current MH services, and how the research can be carried out effectively. The insights included:
Ensuring regular community visits (twice a week) to engage stakeholders, provide consistent services, and conduct research activities. Conduct more Information, Education, and Communication (IEC) activities to sensitize the community on the scope of the research and MH services. Greater engagement of key stakeholders, for example, medical officers, Accredited Social Health Activist workers (provisioning implicit incentives), staff at health centers, and panchayat members. This can be achieved by orienting them on the magnitude and burden of MH problems within the community, including its relationship with major public health issues such as suicide, substance use, intimate partner violence, and chronic physical disorders. Utilizing their networks within the community and health system to sensitize the public on MH issues, organize awareness programs, and incentivize them for their efforts will be crucial. This would also make the community’s preventive psychiatry interventions sustainable. Simplifying the MH screening process to suit their participants’ educational and socio-cultural background. Initial screening at the participants’ vicinity (e.g., Anganwadi center, panchayat office, etc.), later encouraging them to visit the community health center for follow-ups. Tailoring the psychosocial intervention package to enhance its acceptability to the participants by incorporating more images, infographics, using simple language, and involving family members.
Conclusion
The SWOT analysis demonstrated the need for consistent community engagement, culturally and linguistically appropriate intervention designs, and the involvement of local health workers, community stakeholders, and family members. Our work can guide future CBMHR efforts.
Keywords
Common mental disorders, depression, anxiety, stress, community psychiatry, field research, preventive psychiatry
Reporting Guidelines (Supplementary Material)
Coskun Benlidayi I and Gupta L. LETter To the EditoR Standards (LETTERS): Considerations for authors, reviewers, and editors. J Korean Med Sci 2024; 39(37): e296.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
None.
Data Availability Statement
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethical Approval
The study was approved by the Institutional Human Ethics Committee, All India Institute of Medical Sciences, Bhopal (Approval No.: IHEC-LOP/2022/EL031; dated 20 August 2022).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Indian Council of Medical Research, New Delhi.
Informed Consent
Not applicable.
Prospective Registration
Clinical Trials Registry of India (CTRI), registration number: CTRI/2024/04/065769. Available at:
Citation Diversity Statement
We are committed to equitable citation practices and have made conscious efforts to include work from authors of diverse genders, geographic regions (including the Global South), career stages, and historically marginalized groups. I aim to support a more inclusive and representative scholarly record.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.