
Abstract
Background:
Pregnant women are at increased risk for mental health issues such as anxiety and depression, influenced by multiple psychosocial factors. The current study aimed to develop and validate a proforma for screening psychosocial concerns in Indian pregnant women.
Methods:
This study used a mixed-methods design. In Phase 1, a detailed literature review and in-depth interviews with nine pregnant women at a private hospital in India were conducted, leading to the development of a preliminary draft of the proforma to understand the psychosocial concerns of pregnant women. In Phase 2, the proforma was validated by six subject matter experts in perinatal care. Content validation of the proforma was calculated using the item content validity index and the modified kappa (k*) statistic.
Results:
Thematic analysis identified three major themes: Informed choice about pregnancy, navigating the journey of pregnancy, and social support. These themes and other major psychosocial risk factors, derived from an extensive literature review, guided the development of the screening proforma. All items in the screening proforma met the criteria for relevance and simplicity; however, two items required revision for clarity. After the necessary revisions, the final screening proforma consisted of eight domains and 20 items.
Conclusion:
Screening pregnant women using a psychosocial proforma during routine antenatal checkups facilitates timely referrals to mental health professionals, thereby promoting holistic, and culturally sensitive maternal care.
Psychosocial issues in common mental disorders during pregnancy often go unnoticed, leaving women vulnerable during a time of major change. This study aims to create a screening form for obstetricians and gynecologists to easily identify psychosocial concerns in pregnant women. Integrating psychosocial screening into antenatal care enables early detection, referral, intervention, and better maternal mental health.Key Messages:
Pregnancy is generally a life-altering change that brings a permanent shift in women’s lives. 1 During this sensitive period, women are more prone to mental disorders such as depression and anxiety. These disorders are prevalent among pregnant and postpartum women across the globe, hence also known as perinatal common mental disorders (CMDs). According to the World Bank, in high-income countries (HIC), the prevalence of depressive disorders antenatally and postnatally is approximately 11% and 13%, respectively. In contrast, in low- and middle-income countries, the mean prevalence rates of perinatal CMDs are significantly higher, at 15.6% and 19.8%, respectively.2,3 Perinatal CMDs impact a woman’s mental and physical health and have long-term effects on her and her offspring’s well-being, quality of life, and overall functioning.4,5
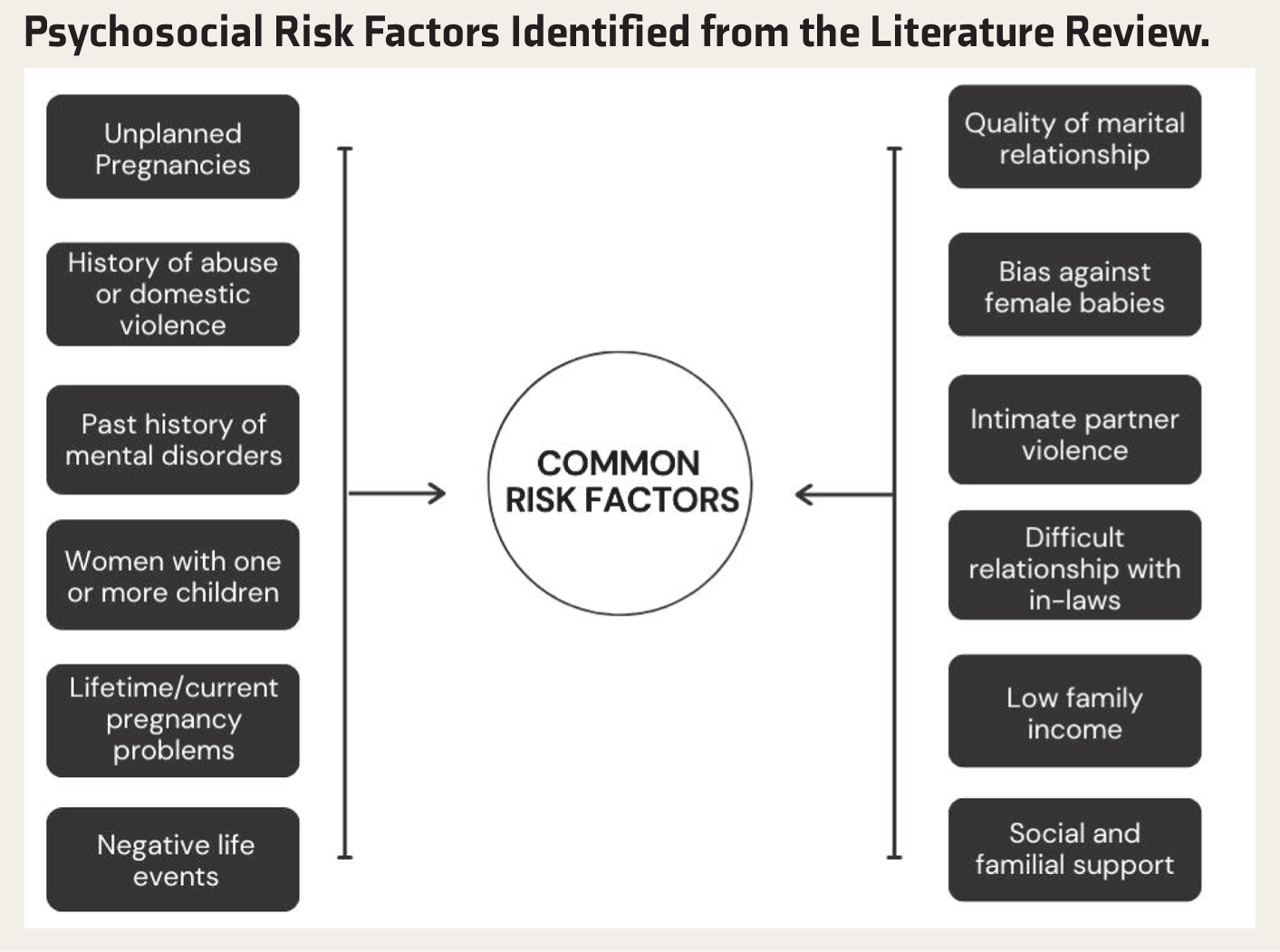
A systematic review of 97 studies examining risk factors for the onset of antenatal anxiety and depression found that these factors were predominantly psychosocial, obstetric, and environmental in nature. Key risk factors identified included unplanned pregnancies, a history of abuse or domestic violence, lack of partner or social support, exposure to negative life events, high perceived stress, and both lifetime and current pregnancy-related complications. 2 Gender-based issues, such as discrimination against female infants, restrictive roles in household tasks and childcare, and heavy unpaid workloads, where women have limited autonomy, significantly increase the risk for perinatal CMDs in pregnant women. 6
Often, motherhood is seen as a glorious time in a woman’s life. This makes it difficult for a woman to talk about experiencing negative emotions during and after the pregnancy. Additionally, CMDs during pregnancy frequently go undiagnosed and untreated, as their symptoms are often attributed to the typical experiences of pregnancy. 6 In India, hospitals are often crowded with long waiting queues in outpatient settings. Women feel hesitant in bringing up mental health concerns on their own when they are not asked about it directly by the health professionals. It may also be left uncovered due to normalization of those symptoms or the fear of stigmatization, which may act as a barrier in addressing mental health concerns during routine perinatal checkups.7,8
In 2016, the World Health Organization recommended incorporating maternal mental health care into primary health care to improve accessibility. 9 Given the valuable opportunity for early intervention during pregnancy and the frequent interactions women have with healthcare professionals during this period, there has been considerable interest in developing an antenatal psychosocial assessment tool. These tests could be more helpful in providing primary care physicians with a structured method of doing psychological assessment. 10
In India, evidence on the validity of existing screening tools is limited, and much of it focuses exclusively on the Edinburgh Postnatal Depression Scale (EPDS) as the best alternative in the absence of any locally validated tool. EPDS, although psychometrically validated for the Indian population, investigates the symptom domain specifically for depressive disorder and does not cover the psychosocial risk assessment or look for other perinatal CMDs. 11
The existing literature highlights a significant gap in the availability of locally developed and validated tools specifically designed for Indian pregnant women. This study aims to address this need by creating a proforma informed by a comprehensive literature review and qualitative interviews with pregnant women. This may help expand on evidence from existing quantitative studies, go a step further in understanding the concerns from the women’s perspective, and develop a culturally appropriate proforma that reflects the unique psychosocial challenges faced by this population.
Methods
The present study used the mixed-methods approach. The study was conducted in two phases. In Phase 1, in-depth interviews and a detailed review of the literature were conducted, leading to the construction of a preliminary draft of the antenatal psychosocial screening proforma.
In the literature review phase, the following databases were searched for relevant publications from 2000 to 2024: PubMed, Scopus, Web of Science, and Google Scholar search engine using keywords “antenatal,” “postnatal,” “prevalence,” “perinatal mental disorders,” “psychosocial concerns,” “social support,” “low-middle-income countries,” and “India.”
For in-depth interviews, nine pregnant women were recruited, three from each trimester between December 2023 and April 2024, from the Department of Obstetrics and Gynecology of a private hospital in India. The sampling was purposive in nature. The inclusion criteria were that women be married and above 21 years of age, have a working knowledge of English or Hindi, and have a confirmed intrauterine pregnancy on ultrasound. The exclusion criteria were the presence of any comorbidities such as pre-eclampsia, eclampsia, antepartum hemorrhage, conditions such as fetal growth restriction and twin pregnancy requiring prolonged bedrest, HIV, severe pre-existing cardiac disease, connective tissue disorder, self-reported current diagnosis of any psychiatric illness, presence of congenital abnormalities in the fetus, or the mode of conception through assisted reproductive treatment.
The decision to exclude individuals with a current diagnosis of psychiatric illness at the time of the interview for Phase-1 interviews was taken in line with the study’s objective of developing a preventive screening proforma to identify psychosocial concerns in a general antenatal population that may increase vulnerability to clinical or subclinical mental health conditions. While these concerns are not indicative of pathology, they may act as potential risk factors when present cumulatively. The inclusion of participants with a current psychiatric diagnosis at the time of the interview could have confounded the findings, as their responses may reflect established psychopathology rather than early psychosocial risk markers.
In Phase 2, the proforma was validated by six experts in perinatal care and reviewed by five pregnant women for feedback on its feasibility and utility. The phase-wise progression of the study ensured both depth and methodological rigor in developing this culturally relevant screening proforma for psychosocial concerns.
Socio-demographic datasheet was used to collect relevant details of the participants regarding their age, religion, education, occupation, relationship status, duration of relationship, number of completed weeks of pregnancy, parity index, previous pregnancy losses, partner’s employment status, comorbid conditions, mode of conception, total family income, total number of earning members in family, type of family, total number of family members and age of any other children if present.
The interviewer used a semi-structured interview guide comprising open-ended questions to explore psychosocial concerns that could significantly influence women’s experiences of pregnancy. The guide was designed to elicit detailed accounts of participants’ lived experiences, focusing on domains such as physical and emotional changes during pregnancy, perceived social support, attachment to the developing fetus, mental health concerns, cultural pressures regarding the preferred gender of the child, and issues related to physical safety, all of which were considered relevant to their psychological well-being. The interview guide was validated by three subject experts with at least five years of experience in perinatal care and/or qualitative research. The experts qualitatively evaluated each question for adequacy, accuracy, and relevance, and provided additional remarks where necessary. The interview guide was subsequently revised in accordance with their feedback before administration to the research participants.
Procedure
Approval for this study was obtained from the Institutional Ethics Committee (IEC 305/2023). A socio-demographic datasheet and a semi-structured interview guide were developed. The researcher then recruited pregnant women from the obstetrics and gynecology outpatient department in accordance with the proposed inclusion and exclusion criteria. After participants were selected, they were given a participant information sheet, and informed consent was obtained from those willing to participate in the study. The study was conducted in two phases. In Phase 1, face-to-face in-depth interviews were conducted in person using the semi-structured interview guide. With participants’ informed consent, the interviews were audio-recorded. All the interviews were conducted by the first author in a separate room within the Outpatient Department (OPD), with only the participant and the interviewer present, to ensure confidentiality and minimize interruptions. The interviews were being transcribed and analyzed alongside ongoing interviews to better understand the emerging themes. The researcher conducted an extensive review of the literature to simultaneously explore and identify various psychosocial concerns that affect maternal mental health. Based on these findings, the proforma was subsequently developed. This marked the end of Phase 1. In Phase 2, the first draft of the proforma was sent to six subject experts and five pregnant women for expert validation, and based on their feedback, the items were modified to improve the clarity and utility of the proforma.
Data Analysis
The transcribed data were analyzed using thematic analysis. 12 The researcher familiarized herself with the data, and subsequently coding categories and themes were generated, reviewed, defined, and named, concluding with appropriate exemplars on MS Excel.
Expert validation of the proforma was conducted using content validity. Six subject experts shared their opinions on the pro forma’s content domains. They were provided with an information sheet, in which they graded the proforma items on relevance, simplicity, and clarity on a four-point Likert scale. The four-point scale avoids a neutral, ambivalent midpoint. If the grading for the particular question is two or three, the expert was asked to suggest how to revise the question or its choices. Subsequently, an item-wise content validity index (I-CVI) was calculated for each question on the proforma using the method outlined by Polit and Beck (2006). 13 I-CVI was computed as the number of experts who rated each item three or four, divided by the total number of experts.
Then, the probability of chance agreement (Pc) was calculated using the formula Pc = [N! / {A! (N − A)!}] ×0.5 N, where N represents the total number of experts and A denotes the number of experts in agreement. 14 The modified kappa (k*) statistic, which helps determine interrater agreement, was calculated using the following formula for each of the questions: “k* = I-CVI − Pc/1 – Pc.” The calculation was done on the three criteria of relevance, clarity, and simplicity.
The items were then reported based on the I-CVI values for relevance, simplicity, and clarity, along with the calculated k* and their interpretations. An I-CVI greater than 0.78 is considered excellent. Items with an I-CVI slightly below 0.78 are candidates for revision. At the same time, those with significantly low values should be considered for deletion. 15 The evaluation criteria for k* are as follows: Values above 0.74 are considered excellent, values between 0.60 and 0.74 are considered good, and values between 0.40 and 0.59 are considered fair. 16
Results
This study identified the various psychosocial concerns associated with perinatal CMDs through an extensive literature review and the thematic analysis of participants’ interviews. A total of three themes and seven subthemes were generated from the qualitative data. These psychosocial concerns led to the development of a preliminary draft of the proforma. The proforma assesses these concerns through a series of multiple-choice questions designed to assist Obstetrics and Gynecology (OBGs) in identifying when a pregnant woman may require additional support from a mental health professional.
The psychosocial concerns identified from an extensive review of literature of both global and Indian studies as shown in
Psychosocial Risk Factors Identified from the Literature Review.
A total of 16 pregnant women who met the study criteria were approached to participate in the in-depth interviews. Of these, seven declined to provide consent, and nine consented to participate. The socio-demographic profile of the study participants revealed a diverse range of backgrounds and characteristics. The participants’ ages ranged from 28 to 32 years. Seven out of nine women were Hindu, and the two women were Muslim. Most of the participants had completed undergraduate degrees. Six out of nine women were employed in either the government or private sectors, and three were homemakers. All participants were married, with relationship duration ranging from 2 to 11.5 years. Two women reported previous pregnancy losses.
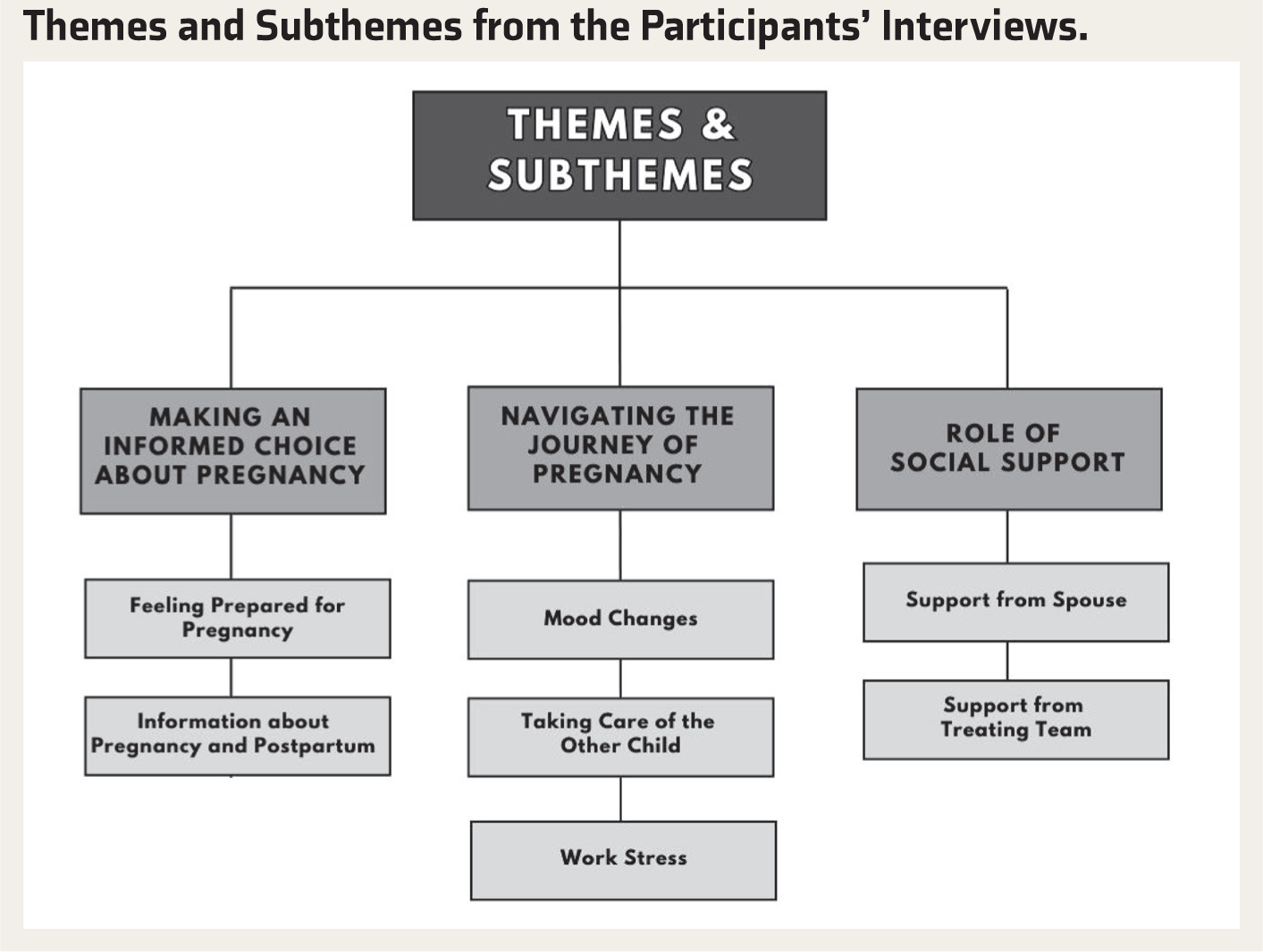
The thematic analysis of interviews identified three themes of “making an informed choice about pregnancy,” “navigating the journey of pregnancy,” and “role of social support,” and seven subthemes as shown in
Themes and Subthemes from the Participants’ Interviews.
Making an Informed Choice About Pregnancy
This theme looks at the women’s preparedness and how informed they feel about the pregnancy process, especially for first-time mothers.
Feeling Prepared for Pregnancy
Participants’ responses revealed that feeling physically and emotionally prepared for pregnancy is a crucial preliminary step that helps the mother-to-be be ready for the various changes that may occur during this period. Additionally, when she feels ready, she is more likely to embrace the experience and handle the associated changes and challenges with greater resilience.
“I had conceived six months before, actually. At that time, I had taken some tablets thinking that I needed to work now, and I am not able to, I am not in mental condition to get pregnant” (PW2, first trimester, multigravida).
“….Even I should be ready for it, like see the hormonal changes, there will be mood swings, they should not completely take me aback. I should be ready for it first…” (PW8, third trimester, primigravida).
Information About Pregnancy and Postpartum
The analysis of women’s interviews reveals the lack of adequate, reliable spaces in India that teach them how to take care of themselves and their babies after birth. Access to reliable information enables parents to make informed choices and prepare effectively for the journey ahead.
“In Germany, they train the mothers and the fathers as well, like, starting from diaper changing to the everything giving bath……So, I felt that must be there in India as well, like so that we are aware of it, and here what we do is we Google everything…” (PW 8, third trimester, primigravida).
Navigating the Journey of Pregnancy
Pregnancy can bring about numerous daily challenges that contribute to a woman’s overall stress levels.
Mood Changes
Women talk about how it is difficult for them to deal with the mood changes that come as a part of their pregnancy. They discuss how these changes make them feel frustrated and irritated more easily than usual, and can frequently disrupt their daily routine.
“Yeah, it changes a lot, too much sometimes. Like we have these emotional things also going on, the mood swings and all that…..it is like the patience level has decreased a lot” (PW6, third trimester, multigravida).
Taking Care of the Other Child
The interviews with pregnant women highlighted an important aspect that pregnant women who are already parents, particularly of toddlers, find it difficult to attend to the needs of an additional child.
“I just came back three months ago to India. Before that, I was there (outside India), so managing the toddler all alone gets a little bit difficult with another child” (PW6, third trimester, multigravida).
Work Stress
The interviews highlight the difficulties of managing work responsibilities and performing efficiently while also getting their home chores done, and the added challenges that pregnancy brings for these women.
“Presently I am working, this pregnancy process will be for nine months, I have to work, which needs struggle right, we have to work at home, work at the office, and we cannot get the rest…It is just that I am getting tired doing both jobs and unable to get the rest….” (PW4, first trimester, multigravida).
Role of Social Support
Social support during pregnancy is essential, as it addresses the physical and emotional needs of the expecting mother, enhances the pregnancy experience, and contributes to a healthier outcome for both mother and baby.
Support from Spouse
Spousal support during pregnancy is crucial for the well-being of pregnant women. A supportive spouse helps manage the physical demands of pregnancy and reduces the emotional burden of navigating pregnancy-related concerns alone.
“The main thing is the support from family members, especially my husband, even though he stays in Bangalore, for every appointment he makes sure that he comes with me, so that kind of support is needed…he used to help me a lot in the household work and managing the stress…” (PW9, third trimester, primigravida).
Support from Treating Team
The women’s interview highlights the importance of reliable hospital care, particularly during pregnancy. For pregnant women, knowing they are receiving care from a reliable and familiar provider contributes significantly to their overall well-being and peace of mind.
“Yeah, if I go somewhere, it means I will not feel better. I will stick to my Dr S. I feel very satisfied and comfortable here. A secure feeling will come” (PW2, first trimester, multigravida).
Development of the Screening Proforma
The screening proforma was developed from the themes that emerged from the interviews and the relevant psychosocial risk factors identified from the literature review. The screening proforma is divided into eight domains and 19 items related to psychosocial concerns that impact the mental health of pregnant women. These domains are feelings toward pregnancy, mental health during pregnancy, relationship with spouse, social support, home, and career, abuse/violence, gender of the child, and perinatal services. This marked the completion of Phase 1 of the study.
In Phase 2 of the study, the researcher selected six subject experts from psychiatry, clinical psychology, obstetrics and gynecology, and psychiatric nursing, all with extensive experience in perinatal health. The experts were requested to evaluate the proforma on the criteria of relevance, clarity, and simplicity on a four-point Likert scale (one–not relevant/clear/simple, two–item needs some major revision, three–relevant/clear/simple but needs minor revision, and four–very relevant/clear/simple. The experts were asked to provide suggestions for changing the questions or choices if a grade of two or three was provided.
Based on expert feedback, I-CVI was calculated for three criteria: Relevance, simplicity, and clarity. In the next stage of analysis, Pc and k* were calculated.
As shown in
I-CVI, Pc, Modified Kappa (k*) of the Items of the Screening Proforma on the Three Criteria of Relevance, Clarity, and Simplicity.
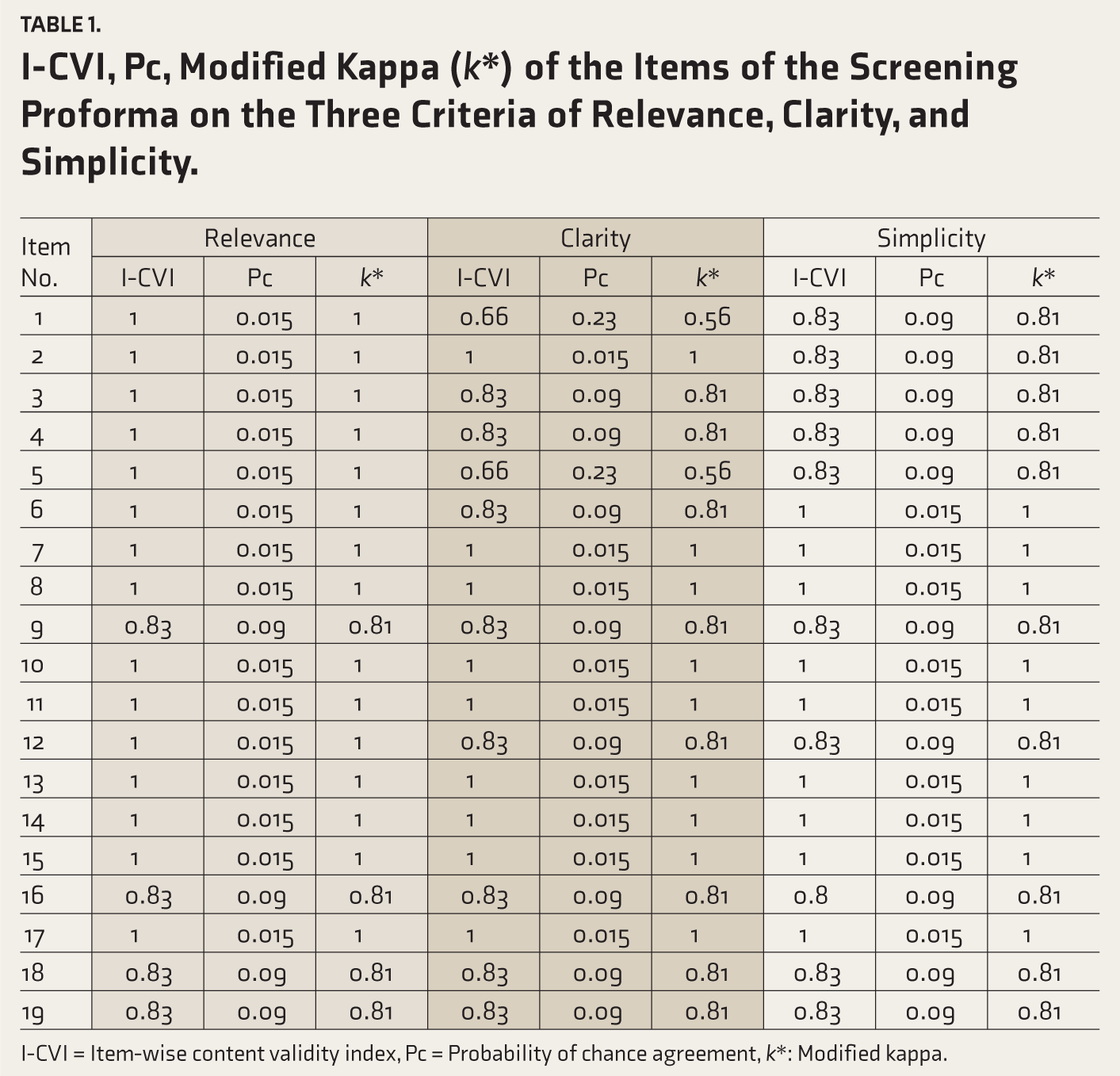
I-CVI = Item-wise content validity index, Pc = Probability of chance agreement, k*: Modified kappa.
A sample of five pregnant women was requested to evaluate the relevance of the items. All the items were scored 0.80 or above, except items 16 and 17, which were scored 0.6. These questions were regarding abuse and feeling pressured to have a baby of a particular gender. The low scores for these questions may be due to their sensitive nature, which could have made respondents uncomfortable. After rating the items, women were also asked about their overall opinion regarding the proforma. Some women recognized that these questions are important to ask, yet others were cautious about answering them due to the stigma attached to them. They highlighted that some women may not answer these questions honestly. Hence, it is important to administer the proforma only by clinicians after the second or third visit. This allows trust to develop and makes pregnant women feel more at ease in responding to sensitive questions.
After the initial round of validation, the expert suggestions were incorporated to reframe the items, making the proforma more comprehensive and effective. The final screening proforma consists of 20 items across eight domains, primarily in closed-ended question formats (yes/no and Likert scales). This format was chosen to ensure ease of administration in busy clinical settings and to facilitate quick decision-making regarding referrals. The referral will be implemented in two ways:
Referral for critical items (4, 6, 7, 9, 11, 15, 16, 17, 18): If the patient says yes to any of the critical items, the doctors are to make a referral to a clinical psychologist and a psychiatrist, respectively. Referral based on additional items: For the rest of the 11 items, if the patient says yes to three or more items, then the referral needs to be made.
The referral system will help OBGs identify when a referral to a mental health professional is necessary.
Discussion
The present study aimed to contribute to the existing literature by exploring the psychosocial concerns of pregnant women through qualitative interviews and by developing an antenatal psychosocial screening proforma for pregnant women in the Indian context. The final proforma included eight domains that capture key psychosocial concerns among pregnant women.
The first domain—feelings toward pregnancy indicates the importance of whether a woman feels mentally prepared to carry the pregnancy and for the upcoming changes that it brings. Indian women are shaped by social and cultural norms that epitomize motherhood, which, once attained, lead to societal approval. Often, women are expected to meet familial and societal expectations by conceiving soon after marriage, which can create pressure to do so regardless of their emotional readiness. 23 A study shows that women with unplanned pregnancies reported more physical issues, had more negative experiences and pain during labor, and faced greater mental health challenges in the early postpartum period. 24 They also exhibited elevated levels of depressive symptoms throughout all three trimesters of pregnancy and during the first 12 months postpartum. 25 The proforma includes questions assessing whether the pregnancy was wanted or unwanted, the woman’s subjective experience of pregnancy on a rating scale, and her perceived mental preparedness for motherhood. These questions help clinicians identify ambivalence, distress, or adjustment difficulties that may not have been addressed or discussed.
The domain of mental health during pregnancy specifically looks at symptoms that may indicate underlying mental health conditions, such as depression and anxiety, which may go unnoticed during the antenatal period. Normalizing such concerns and providing space for women to speak about their emotional well-being can promote early intervention and reduce stigma. Research showed that introducing EPDS for screening of mental health problems facilitated the initiation of discussions about mental health and effectively shifted the focus from the infant to the mother, thereby fostering a more open dialogue about mental health concerns. 26 The proforma includes questions assessing excessive worry, pregnancy-related fears, low mood, loss of interest, and prior help-seeking behavior. These items enable early identification of emotional distress and determine whether further mental health evaluation is necessary or not.
Social support from spouse, in-laws, and family is a very important factor because it can help mitigate pregnancy-related stress. Research found that support from a partner in terms of emotional, instrumental, and effective communication can be protective against perinatal anxiety and depression. 27 A systematic review on the impact of social support on pregnant women found that women who received low social support are more likely to develop mental illness as compared to women who received good social support. 28 In the Indian context, women after marriage are expected to shift to their in-laws’ home, so their relationship with them and the treatment meted out to her can significantly impact their journey of pregnancy. This domain is assessed through questions exploring satisfaction with the relationship with the spouse, perceived emotional support during pregnancy, and concerns related to the spouse’s employment or mental health. In addition, the proforma includes items assessing emotional support from in-laws, parents, and siblings, thereby enabling evaluation of the availability and reliability of familial support systems during pregnancy.
The domain of home and career captures the dual burden many women face: Meeting workplace expectations while managing home responsibilities. Pregnancy is sometimes perceived as a limitation at work, and for women with additional caregiving duties (e.g., older children), the stress may be amplified. Women are expected to balance their roles as mothers and professionals, demanding excellence and dedication in both, which places a significant burden on them in reality. 29 To capture these challenges, the proforma includes questions on satisfaction with support for household tasks, difficulties caring for other children, and pregnancy-related challenges at work. These items help identify areas where practical or social assistance may be required.
Any form of abuse or threat to safety can undermine the mental and physical health of pregnant women. Additionally, in families with a strong preference for a male child, the burden of this expectation often falls on the woman, influencing how she is treated. This can adversely affect women’s health, well-being, and reproductive rights. To meet expectations of producing a male heir, many women are subjected to repeated pregnancies, coerced abortions, and, in extreme cases, infanticide. In the absence of a male child, they may face humiliation, emotional abuse, or even violence from their husbands and in-laws. 30 To address such risks, the proforma includes direct questions assessing threats to safety within the household and experiences of abuse, thereby providing an opportunity for women to disclose sensitive concerns that might otherwise remain unreported. Additionally, the proforma includes a specific item assessing whether the woman feels pressured to give birth to a male child and identifying the source of such pressure, which helps clinicians recognize sociocultural stressors that may influence maternal well-being.
The final domain assesses the availability and reliability of perinatal healthcare services. Research shows that healthcare providers identify themselves as key sources of emotional support, support networks, and advocates for these women. 31 Access to a responsive treatment team and accurate information can help pregnant women feel more secure and supported throughout their journey, thereby enhancing both maternal and fetal outcomes. The proforma, therefore, includes questions assessing perceived access to appropriate healthcare services and the adequacy of information provided during antenatal consultations, thereby identifying potential gaps in care or informational needs.
The American College of Obstetricians and Gynecologists guidelines emphasize the use of standardized and validated tools for the assessment of pregnant women in the peripartum period for anxiety and depression and recommend their use during postpartum visits for every patient. It further emphasizes that, in accordance with the American Pediatric Association’s recommendations, psychosocial screening should be conducted at least once in each trimester to improve the likelihood of identifying major issues and reducing the risk of adverse birth outcomes. 32 Additionally, the antenatal period was the focus of the present study because it is linked to poor perinatal outcomes. This association is stronger in lower-middle-income countries than in HICs. By systematically assessing psychosocial concerns during the antenatal period, the proforma aims to facilitate early identification of difficulties and timely referral to mental health professionals, thereby promoting holistic and culturally sensitive maternal care.
Strengths and Limitations
This study’s strength lies in its integrative approach, drawing on both in-depth interviews and the literature to develop a culturally sensitive screening proforma for psychosocial concerns among pregnant women. Furthermore, expert validation from well-experienced clinicians across multiple disciplines enhances the credibility and clinical relevance of the proforma. To the best of the researcher’s knowledge, it is the first study from India to have developed a screening proforma for psychosocial concerns in women during the antenatal period. This study has important implications for perinatal care in India, as the screening proforma can facilitate crucial conversations around maternal mental health, especially in busy hospital settings. By providing a structured tool for early identification and intervention, it has the potential to improve mental health outcomes and enhance overall maternal health care quality.
However, the sample primarily consisted of women from middle- to upper-socioeconomic backgrounds, limiting the exploration of diverse experiences. Additionally, the developed screening proforma could not be used on a larger sample of pregnant women to assess its feasibility. Future research should focus on expanding the sample for greater generalizability, establishing standardized cut-off scores, and developing a referral system. Longitudinal studies assessing its effectiveness over time and its integration into routine antenatal care will further validate its impact on maternal and fetal health.
Conclusion
The antenatal period is an important window for maternal mental health, shaping both the well-being of the mother and the infant. This study highlights the need for early psychological assessment during pregnancy and introduces a validated screening pro forma designed for obstetricians and gynecologists. By enabling early detection and timely intervention, this proforma has the potential to transform maternal care, fostering healthier mothers, stronger parent-infant bonds, and better long-term outcomes for future generations.
Reporting guideline (Supplementary online material)
The Good Reporting of A Mixed Methods Study (GRAMMS) Checklist was used for drafting this manuscript.
Citation: GRAMMS - O'Cathain A, Murphy E, Nicholl J. The quality of mixed methods studies in health services research. J Health Serv Res Policy. 2008;13(2):92–98.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
We would like to extend our gratitude to Dr Geetha Desai, Dr Veena Satyanarayana, Dr Roopa PS, Dr Rajeshwari Bhat, Dr Sonia Shenoy, Dr Savitha Prabhu, Dr Sujatha BS, Dr Supraja TA, and Dr Sumita Rege for their precious time and feedback, which significantly enriched this study. We would like to thank all the participants whose cooperation made this study possible.
Data Availability Statement
The authors can be contacted for data. It will be considered upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethical Approval
The ethics approval was obtained prospectively.
Name of the IEC/Independent Review Board: Kasturba Medical College and Kasturba Hospital IEC Approval Ref. No.: 305/2023 Date: November 10, 2023
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent for participation in the study was obtained from all the study participants.
Registration Number
The study was registered prospectively.
Trial registry name: Clinical Trials Registry—India URL: Registration number: 2024/01/061176
Citation Diversity Statement
The authors have made a conscious effort to include references that reflect diversity across geography, gender, and academic perspectives. The cited literature represents a balanced selection of global and Indian research, ensuring inclusivity and minimizing bias in scholarly representation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.