
Abstract
Background:
Despite a high burden of psychological issues in low- and middle-income sub-Saharan countries, no national-level assessment exists for Senegal.
Methods:
To assess the prevalence and predictors of psychological issues, we analyzed the 2023 Senegal Demographic and Health Survey (DHS) data from 75,080 household members.
Results:
The prevalence of psychological issues in Senegal was 5% (95% CI = 5.2–5.6). It was highest in the Matam region (8.7%) and lowest in the Saint-Louis region (3.5%). Female gender (adjusted odds ratios [aOR] = 1.11, 95% CI = 1.02–1.22), no education (aOR = 1.24, 95% CI = 1.11–1.36), singlehood (aOR = 1.64, 95% CI = 1.46–1.85), owned housing (aOR = 1.52, 95% CI = 1.26–1.84), rural residency (aOR = 1.18, 95% CI = 1.05–1.32), higher household size (aOR = 1.01, 95% CI = 1.01–1.02), indoor second-hand smoke (SHS) (aOR = 1.57, 95% CI = 1.43–1.73), and shock events (aOR = 1.61, 95% CI = 1.48–1.76) increased the likelihood of psychological issues. Access to video players (aOR = 0.22, 95% CI = 0.12–0.41), mobile phones (aOR = 0.77, 95% CI = 0.68–0.87), and the internet (aOR = 0.79, 95% CI = 0.66–0.96) reduced the likelihood of psychological issues.
Conclusions:
The burden of psychological issues is high in Senegal. Socio-demographic predictors suggest higher vulnerability among females, the uneducated, unmarried, and rural residents. Stressors such as shock events and indoor SHS increase the risk of psychological issues among household members. Access to recreational tools such as video players, mobiles, and the internet is beneficial in reducing psychological issues. Policy reforms prioritizing strategies to reduce psychological issues and integrating mental health services into healthcare delivery are discussed and recommended.
One out of every 20 Senegalese household members is prone to psychological issues. Females, uneducated, unmarried individuals, and rural residents are vulnerable to psychological issues. Exposure to indoor SHS and experience of shock events in the past are key stressors that triggered psychological issues among household members.Key Messages:
Mental health is a dynamic state of internal balance that enables individuals to use their abilities in alignment with societal values. It involves cognitive and social skills, emotional awareness, empathy, resilience in the face of challenges, and a harmonious connection between body and mind. 1 The psychological impact of recent global events, such as the COVID-19 pandemic, geopolitical events, and environmental change, is likely to persist and require coordinated care approaches for those in need of psychosocial support.2,3
Access to effective mental health services in low- and middle-income countries (LMICs) is limited, leading to a substantial global treatment gap. 4 Psychological issues continue to impact vulnerable populations disproportionately, and treatment coverage continues to be low globally. 5 Inequities also exist in funding for global mental health, and there has been gradual progress in terms of building local capacity for mental health care programs and research. 6 Advances in integrating mental health care and adopting task-shifting are accompanied by implementation challenges. 7
A scoping review reported the three most frequently encountered barriers to accessing mental health services in Africa (Ethiopia, Mali, Egypt, South Africa, Nigeria, and Tunisia) were a preference for traditional, alternative, and complementary treatments (33.3%), followed by stigma (25%) and a lack of knowledge, unfamiliarity with the mental health condition (25%). 8 People exposed to more unfavorable social circumstances are more vulnerable to poor mental health over their life course. The focus is on mental health among marginalized groups (refugees, asylum seekers, displaced persons, ethno-racial minorities, and people in poverty) exposed to intersecting social risk factors. 9
Rationale for the Study
It is important to address psychological issues across the life course, which lays the foundation for long-term and intergenerational health and well-being. 10 Timely interventions would strengthen individuals, families, and social resources, decrease risk factor levels, and prevent much of the disease burden in adulthood. 11 Strengthening resilience in individuals leads to positive health outcomes. 12 The literature from other sub-Saharan countries reported the high burden of psychological issues in the region.8,13 However, to the best of our knowledge, no study has assessed the situation in Senegal. Further, most recently, in July 2024, the Demographic and Health Surveys (DHS) program released the Senegal DHS 2023 data. Considering this, it is crucial to assess the prevalence and associated contributing factors of psychological issues in Senegal using nationally representative DHS 2023 data. Therefore, the current study aimed to assess the prevalence and predictors of psychological issues among the household population in Senegal.
Aim
The current study aimed to assess the prevalence of psychological issues and identify associated risk factors among the household population in Senegal.
Objectives
To assess the prevalence and predictors of psychological issues among the household population in Senegal.
Methods
A cross-sectional descriptive study design was used to assess the prevalence and predictors of psychological issues in Senegal using recent DHS 2023 data. 14
Ethical Considerations
This study used anonymized secondary data from the Senegal DHS 2023, 14 collected by the DHS program, the Inner-City Fund (ICF), and the ANSD. The dataset contains no personal identifiers or precise geographic information. The authors obtained authorization from the DHS program to access and use the data for research purposes. As the study involved analysis of publicly available de-identified secondary data and did not involve direct interaction with human participants, separate Institutional Review Board (IRB) approval and informed consent were not required. All analyses were conducted in accordance with data-use agreements and principles of confidentiality, privacy, and non-disclosure.
Data
We analyzed secondary data from the household member recode dataset (SNPR8RFL.DTA file) of the Senegal DHS 2023. 14 This is the most recent DHS, which covered a total of 76,675 household members across all 14 regions of Senegal.
Study Setting and Sampling
Senegal is located at the westernmost point of Africa in the Atlantic Ocean.15,16 There are 14 administrative regions in Senegal. The Senegal DHS 2023 covered all 14 regions. 16 The DHS program had collected data for the Senegal DHS 2023 from February to August 2023. The Senegal DHS 2023 used a nationally representative sample consisting of 400 clusters and 8,800 households, with an expected number of 16,142 women (aged 15–49) and 6,267 men (aged 15–59) respondents.16,17 All women (aged 15–49) and men (aged 15–59) who were members of households or who spent the night before the survey day in the selected households were eligible for the survey.16,17 The survey collected data of all de jure household members (usual residents), all women and men, and all children residing in the household.16,17 Initially, 8,782 households were selected, of which 8,591 were occupied.16,17 Of these occupied households, 8,423 were successfully interviewed, yielding a response rate of 98%.16,17 From these 8,423 households, the Senegal DHS 2023 covered a total population of 76,675 household members.
For sampling, we initially selected data on 76,675 household members of all ages. Further, from this selected sample, 1,595 entries (2% of the total population) with missing values and “don’t know” responses (as insignificant numbers) were removed. The remaining 75,080 entries, covering household members of all ages, were used as the study sample.
Outcome Variable
We have adopted the definition of psychological issues, as specified in the Senegal DHS 2023 report. 18 The DHS report defines it as problems or psychological illnesses experienced by each household member in the last 6 months. 18 The DHS did not clinically assess psychological issues; however, it did so through a household-level survey based on self-reported responses.
In the Senegal DHS 2023 household recode dataset, 14 self-reported psychological issues are presented as a categorical variable, “sh165,” labeled “problems or psychological illnesses in the household” (responses were in two categories: 0 = no, 1 = yes). This dichotomous categorical variable, representing self-reported psychological issues among Senegalese household members, was treated as the dependent variable in the analysis.
Explanatory Variables
To have sufficient representation (minimum 5%) for each categorical value, five raw variables, that is, education, current marital status, housing occupancy status, indoor second-hand smoke (SHS), and language, were recoded into three new variables (with smaller categories). The definitions of these variables (derived from the Guide to DHS Statistics) 19 and details of the recoding are given in Table 1. The remaining explanatory variables representing socio-demographic and economic characteristics were derived directly from the DHS dataset (as original variables). The selection of these variables was based on conceptual frameworks presented in previously published studies covering diverse psychological issues.20–23
List of All Recoded Explanatory Variables Used in the Analysis.
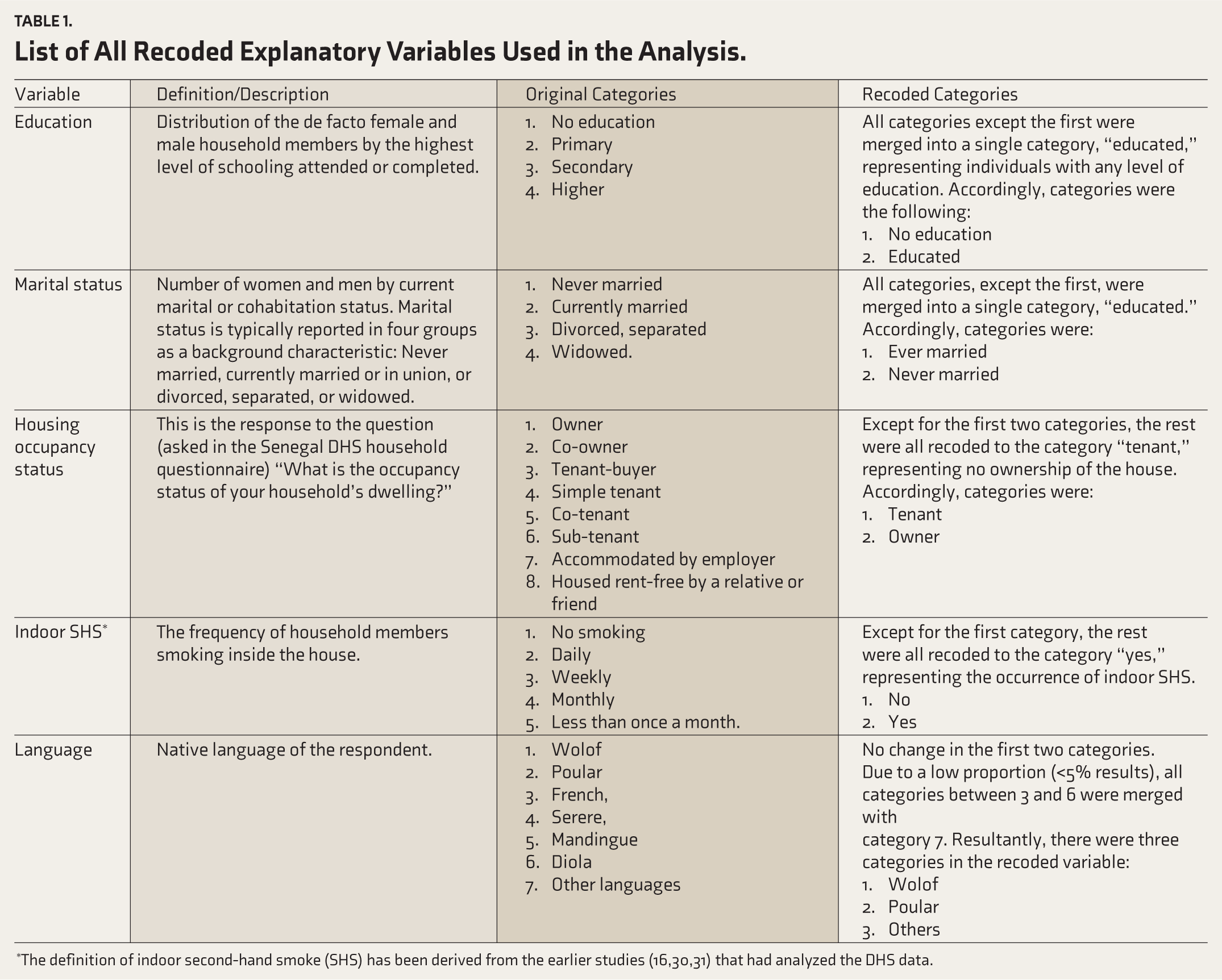
*The definition of indoor second-hand smoke (SHS) has been derived from the earlier studies (16,30,31) that had analyzed the DHS data.
Accordingly, the independent variables selected for this analysis were age of household members (continuous variable), number of household members, that is, household size (continuous variable), gender of household members (male or female), educational status (educated, no education), marital status (never married or ever married), housing status (tenant, owner), place of residence (urban or rural), region (Dakar, Ziguinchor, Diourbel, Saint-Louis, Tambacounda, Kaolack, Thiës, Louga, Fatick, Kolda, Matam, Kaffrine, Kedougou, and Sedhiou), wealth index (poorest, poorer, middle, richer, and richest), and major shock events experienced by household members (yes or no). As specified in the Senegal DHS 2023 household questionnaire, 18 the main shock events experienced by household members in the past 3 months included events such as disease, death, loss of job/unemployment, reduced income/transfers received, floods/drought/loss of livestock, conflict/insecurity/theft or loss of livestock, fire, loss of money, and other adverse events. 16 Further, to present the access to information and entertainment, five additional variables were included, which include the availability of radio (yes or no), television (yes or no), video player (yes or no), mobile (yes or no), and internet (yes or no) in the household.
Statistical Analysis
The data were analyzed using Python (version 3.14.2) 24 with Spyder IDE, 25 employing libraries such as pandas and statsmodels for statistical analysis. Descriptive, bivariate, and binomial logistic regression analyses were conducted to assess the prevalence and predictors of psychological issues in Senegal. Additionally, QGIS v3.14 was used to prepare a map presenting the region-specific prevalence of psychological issues in Senegal.
For bivariate analysis, a first-step chi-square test was performed to assess the association between the outcome and independent variables. For hypothesis testing, p < .25 was considered significant. Any variable significantly associated with the outcome variable was considered for further multivariate analysis. A binomial logistic regression was carried out to assess factors associated with psychological issues in Senegal. Adjusted odds ratios (aOR) were reported to present the association between the outcome variable and explanatory variables.
The model’s goodness-of-fit was assessed using the Hosmer–Lemeshow test. Additionally, the Akaike Information Criterion (AIC) and the Bayesian Information Criterion (BIC) were calculated.
Results
The mean age for the study population was 23.3 years (SD ± 19.7). Fifty-three percent were females. Forty-three percent were educated. Two-thirds were ever married. 91% lived in owned houses, while the remaining 9% were tenants (rented houses). Fifty-eight percent lived in rural areas. Almost half of the household population belonged to the poorest and poorer wealth quintiles. Forty-six percent of household members experienced shock events. Twenty-four percent were exposed to indoor SHS. The mobile penetration (i.e., the percentage of individuals with access to mobile phones) in Senegal is 87% (95% CI = 86.9–88.2). The prevalence of psychological issues in Senegal was 5.4% (95% CI = 5.2–5.6) (Table 2).
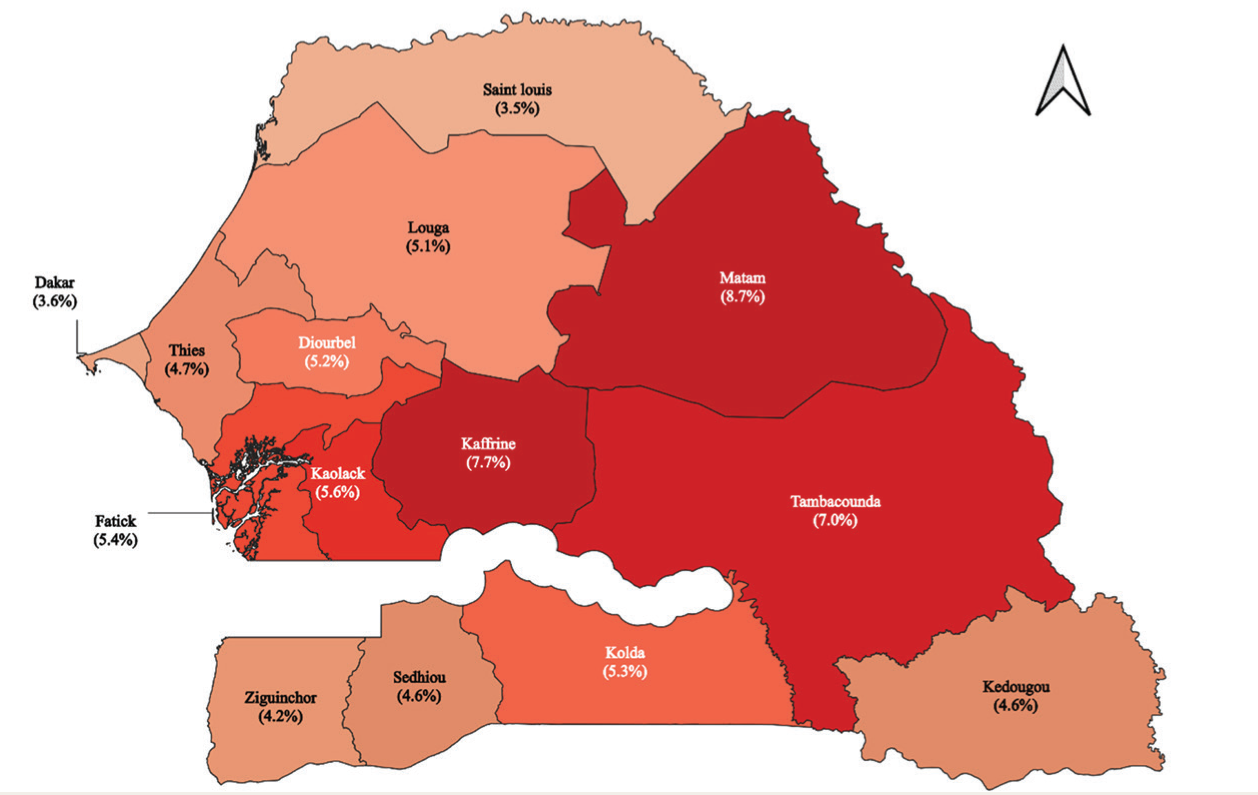
Descriptive Statistics of Study Sample (N = 75,080).
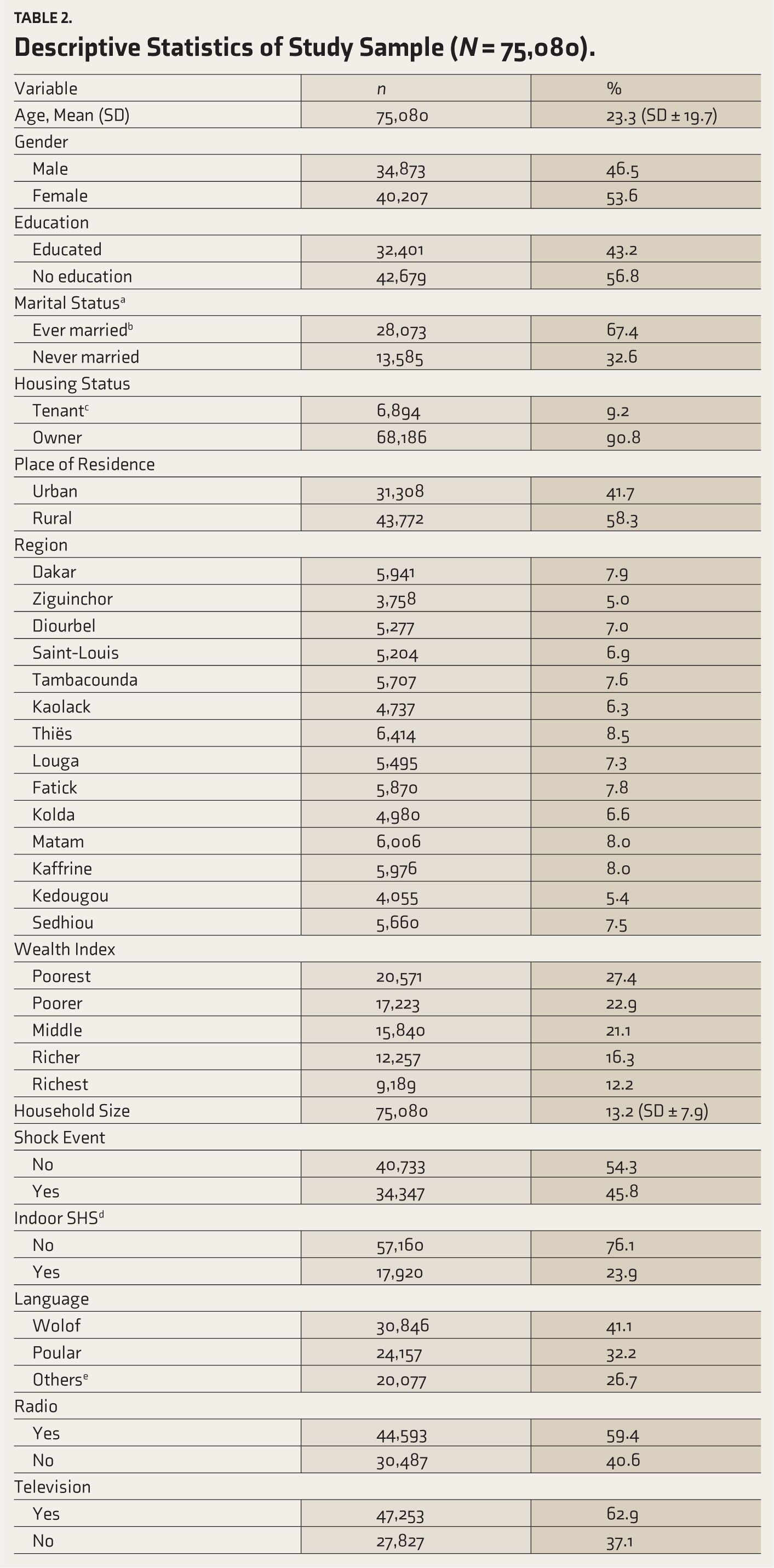
an = 41,658, a total of 33,422 missing entries were excluded. bIncluded currently married, divorced, and widowed. cIncluded tenant, co-tenant, sub-tenant, accommodated by the employer. dSHS: second-hand smoke. eIncluded French, Serere, Mandingue, Diola, and other languages.
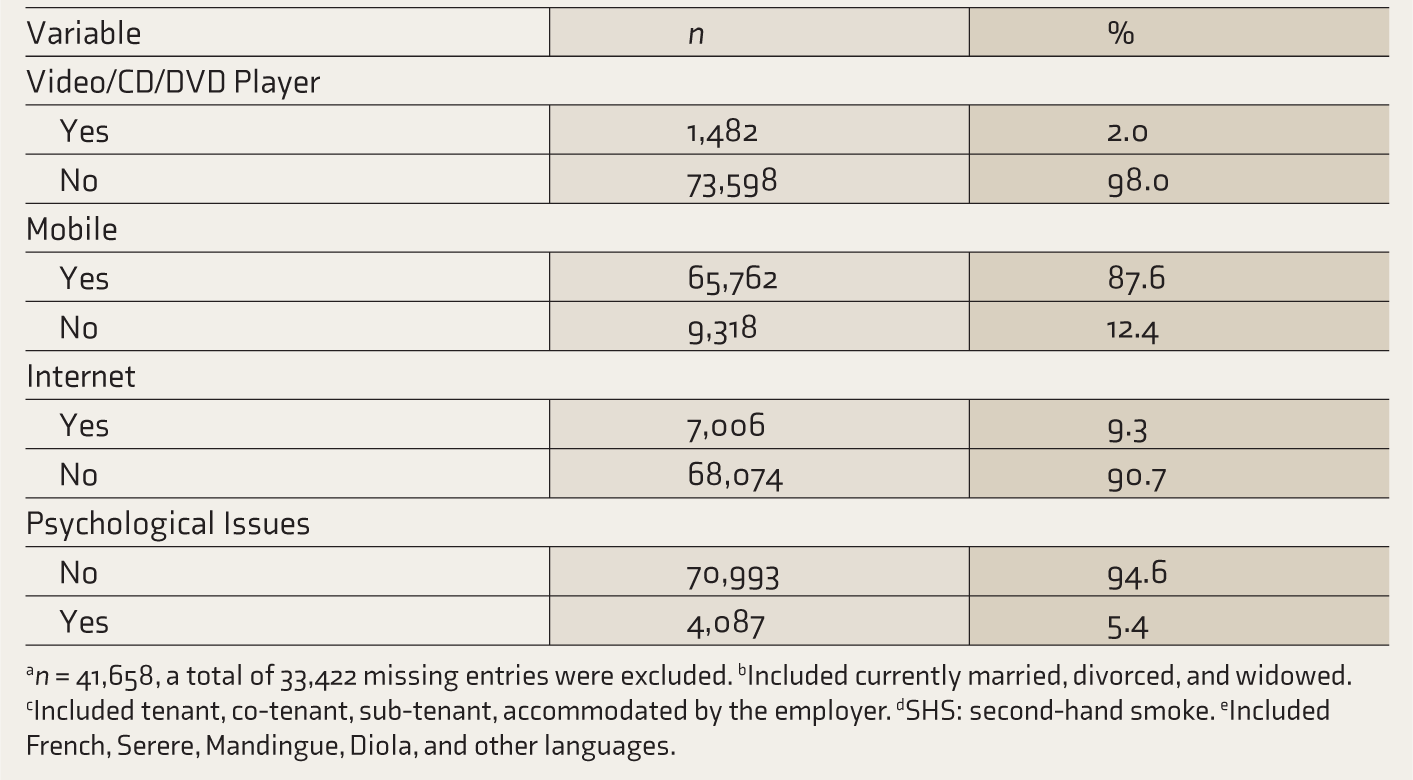
The prevalence of psychological issues across 14 Senegalese regions ranged from the highest in Matam (8.7%) to the lowest in Saint-Louis (3.5%) (Figure 1). More than half of Senegal’s regions had a prevalence higher than the national prevalence of 5%. These regions included Matam (8.7%), Kaffrine (7.7%), Tambacounda (7%), Kaolack (5.6%), Fatick (5.4%), Kolda (5.3%), Diourbel (5.2%), and Louga (5.1%). The difference in prevalence among these 14 regions was statistically significant (Table 3).
The Prevalence of Psychological Issues Across 14 Senegalese Regions.
Bivariate Analysis of Psychological Issues in Senegal.
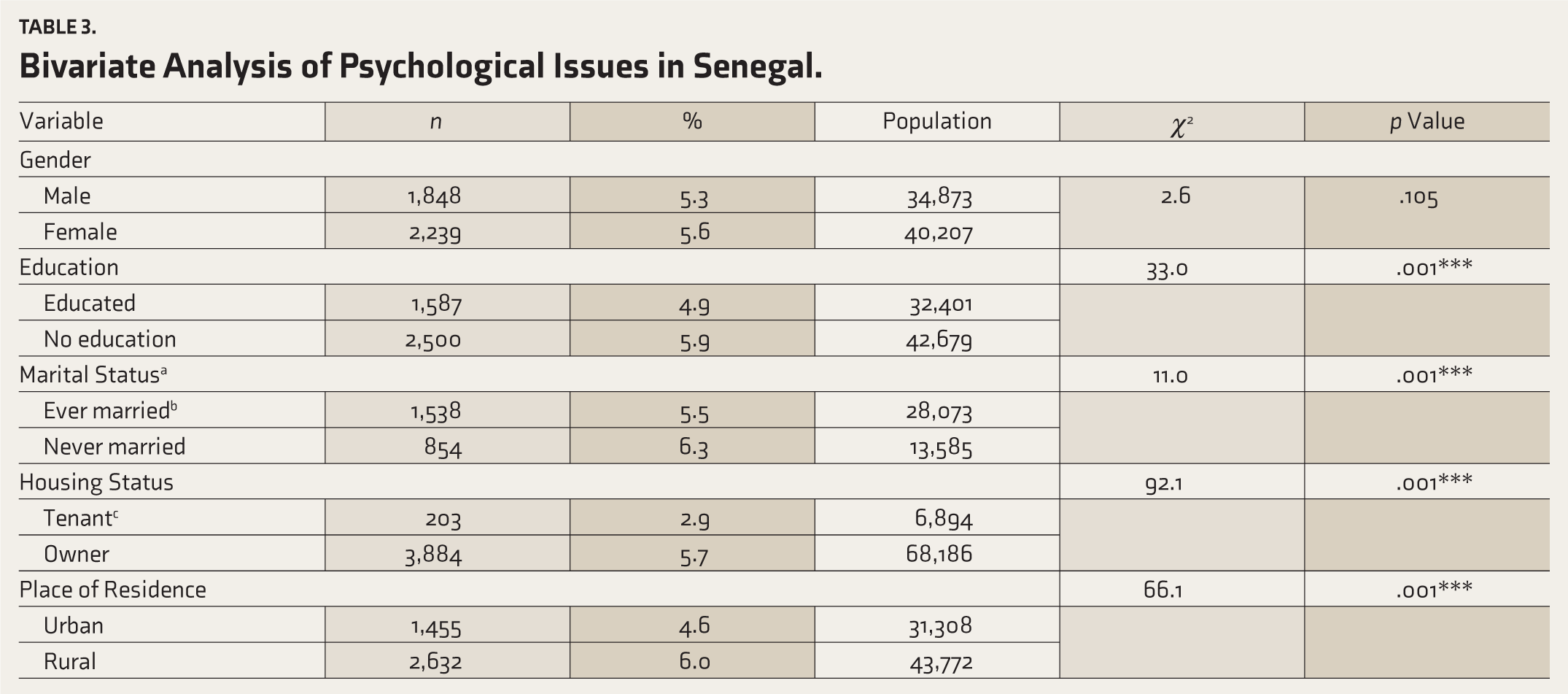
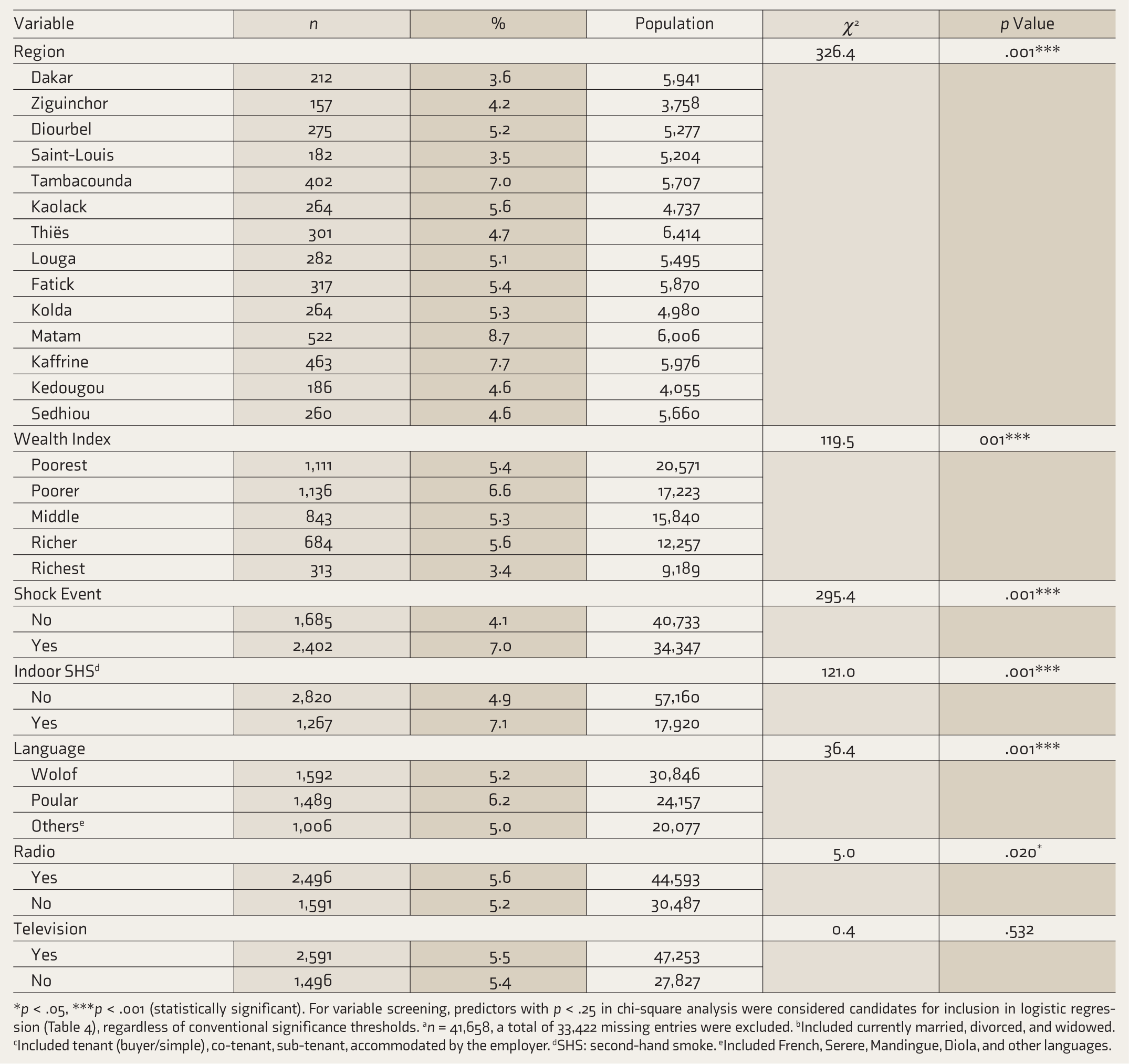
*p < .05, ***p < .001 (statistically significant). For variable screening, predictors with p < .25 in chi-square analysis were considered candidates for inclusion in logistic regression (Table 4), regardless of conventional significance thresholds. an = 41,658, a total of 33,422 missing entries were excluded. bIncluded currently married, divorced, and widowed. cIncluded tenant (buyer/simple), co-tenant, sub-tenant, accommodated by the employer. dSHS: second-hand smoke. eIncluded French, Serere, Mandingue, Diola, and other languages.
In the bivariate analysis, all independent variables except access to television showed a statistically significant association (p < .25) with the dependent variable (Table 3). Further, all these variables were entered into a multivariate analysis. Age, education, marital status, housing, place of residence, household size, indoor SHS, access to video players, internet, mobile phones, and exposure to the shock events were significantly associated (p < .05) with psychological issues among Senegalese households (Table 4).
Predictors of Psychological Issues in Senegal.
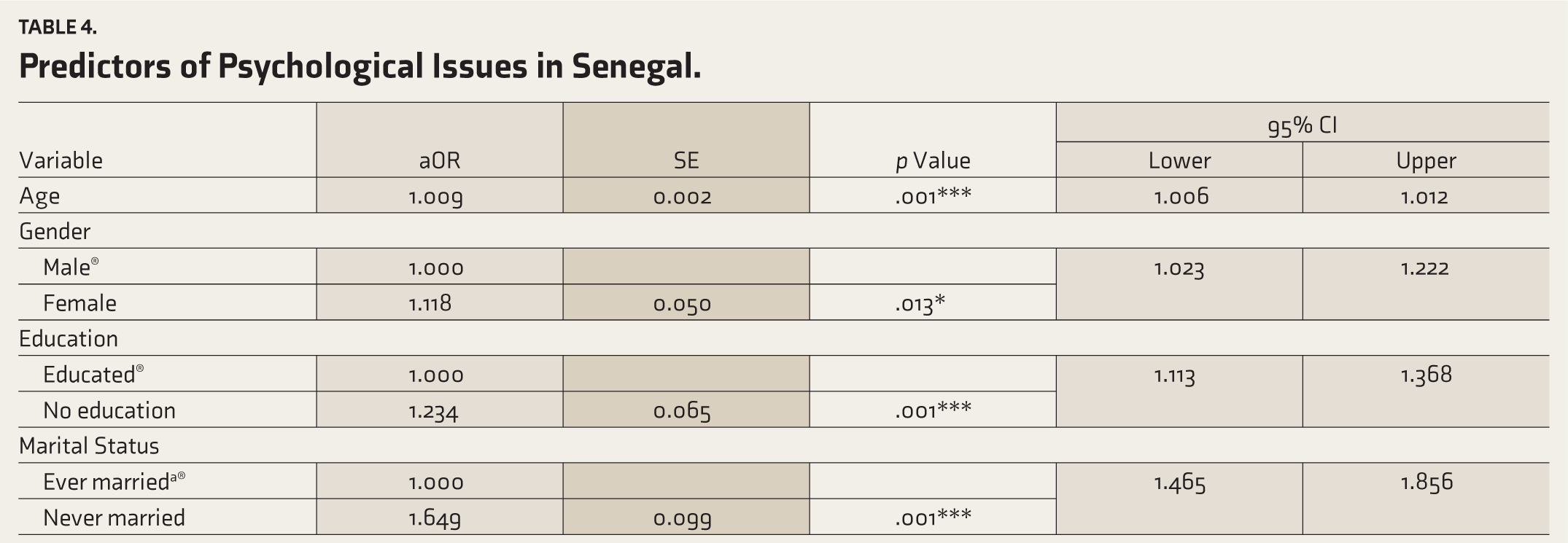
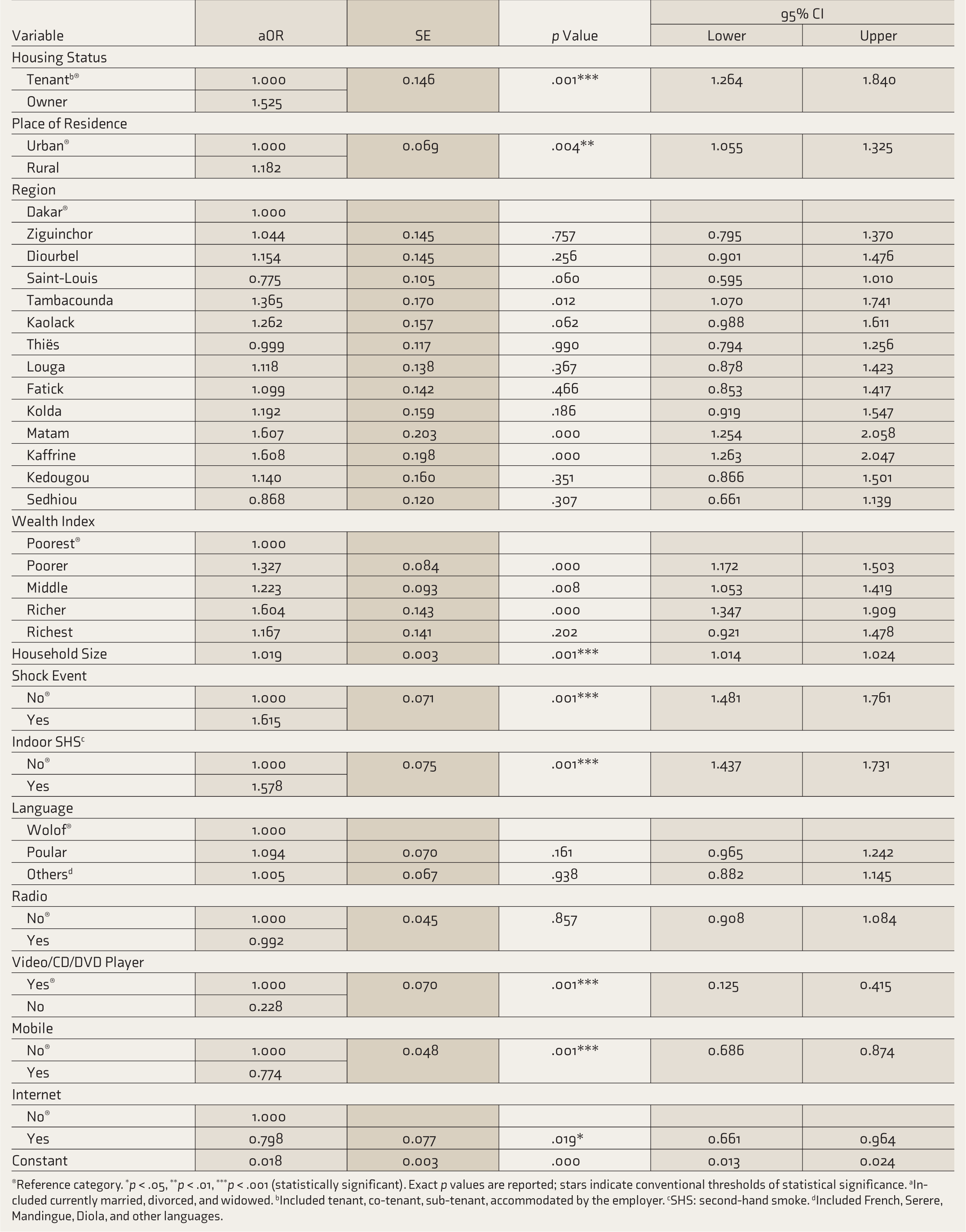
→Reference category. *p < .05, **p < .01, ***p < .001 (statistically significant). Exact p values are reported; stars indicate conventional thresholds of statistical significance. aIncluded currently married, divorced, and widowed. bIncluded tenant, co-tenant, sub-tenant, accommodated by the employer. cSHS: second-hand smoke. dIncluded French, Serere, Mandingue, Diola, and other languages.
Compared to males, females were more likely to experience psychological issues (aOR = 1.11, 95% CI = 1.02–1.22). Compared to educated individuals, individuals with no education were more likely to experience psychological issues (aOR = 1.24, 95% CI = 1.11–1.36). Unmarried (never married) individuals were more likely to experience psychological issues than ever-married individuals (aOR = 1.64, 95% CI = 1.46–1.85). Compared to tenants, owners were more likely to experience psychological issues (aOR = 1.52, 95% CI = 1.26–1.84). Those who lived in rural areas were more likely to experience psychological issues than urban residents (aOR = 1.18, 95% CI = 1.05–1.32). For every additional household member, the odds of psychological issues increased by 1% (aOR = 1.01, 95% CI = 1.01–1.02).
Those who experienced shock events were more likely to experience psychological issues than those who had no such exposure (aOR = 1.61, 95% CI = 1.48–1.76). Those who lived in houses where household members smoked inside the house were more likely to experience psychological issues than those who lived in households with no indoor smoking (aOR = 1.57, 95% CI = 1.43–1.73).
Those who had access to video players were less likely to experience psychological issues than those who had no access to video players (aOR = 0.22, 95% CI = 0.12–0.41). Those living in households with mobile phones were less likely to experience psychological issues than those without access to mobile phones (aOR = 0.77, 95% CI = 0.68–0.87). Those with internet access were less likely to experience psychological issues than those without (aOR = 0.79, 95% CI = 0.66–0.96).
The goodness-of-fit of the logistic regression model was assessed using the Hosmer–Lemeshow test. The model was fitted using a total of 41,658 observations, which included 40,470 unique covariate patterns. The Pearson chi-square statistic was χ2(40,437) = 40,300.7, with a p value of .683. This p value indicates that we cannot reject the null hypothesis, suggesting that the model fits the observed data well.
Discussion
Our research provides evidence for the growing burden of psychological issues in Senegal. Several studies have pointed out the high burden of psychological issues in other sub-Saharan African countries,8,13 and still found that there is limited research presenting the situation in Senegal.26,27 The only available study on the topic, which is a qualitative study conducted a decade ago, has raised concerns associated with limited access to mental healthcare, the influence of traditional faith healers (TFH), and a lack of knowledge about psychological issues among Senegalese healthcare workers. 26 The same study has also pointed out discrepancies in community screening and found that, attributed to a lack of knowledge among healthcare professionals, psychological issues remain underreported. 26 Our study attempted to fill this gap by using the recently released nationally representative Senegal DHS 2023 data.
Gender, education, marital status, housing, place of residence, household size, indoor SHS exposure, access to video players, internet, mobile phones, and exposure to shock events had significant associations with psychological issues in Senegal. We found that females were more likely to experience psychological issues than males. An earlier qualitative assessment had highlighted the role of widespread polygamy (that is, being practiced in Senegal, particularly in rural areas), relationship conflicts, and sexually transmitted infections (STIs), causing psychological issues among Senegalese women. 26
Furthermore, as compared to urban areas, rural areas had a significantly higher prevalence of psychological issues. Some of the possible factors leading to a high burden in rural areas, as mentioned in previous studies regarding general health issues, include irregular income, socio-economic disparities, limited access to healthcare, and differences in the stressors faced by rural and urban residents.26,28 Further, vulnerability to psychological issues among the rural population increased due to disparities in the distribution of mental health services.26,28 In Senegal, mental health services are concentrated in large cities and are scarce in remote rural areas. 26 Possibly, these factors are also responsible for the high burden of psychological issues in rural Senegal.
Indoor SHS is a significant public health issue that is prevalent in several LMICs.16,29–31 Exposure to indoor SHS reflects multiple underlying socio-economic conditions, such as poverty, indoor air pollution, poor housing, illiteracy, and lack of access to health information,32,33 ultimately leading to health hazards16,29–31 and psychological issues.16,34 In alignment with previous studies that presented strong linkages between indoor SHS and psychological issues,16,34 we found a positive association between indoor SHS exposure and psychological issues in Senegal. This underscores the need to address issues such as tobacco use, poor housing with no ventilation, and overcrowded households. Targeted interventions intended to create smoke-free homes and improve housing conditions are essential in this regard. Additionally, policy reforms, including higher cigarette or tobacco taxes, clean indoor air laws, and comprehensive interventions to increase access to tobacco cessation services and smoke-free homes, are recommended.16,31,35–37
The adverse effect of household crowding, due to large household size, on psychological well-being has been discussed elsewhere. 33 Similarly, in our study, we sought to examine the relationship between the likelihood of psychological issues and household size. Senegal is a polygamous society, leading to large family and household sizes. Resultantly, the psychological issues of women are neglected and remain unnoticed in a patriarchal Senegalese society. 26
The most important finding in our study is that we identified stressors, such as shock events, that triggered psychological issues among the Senegalese household population. We found a significant association between the existence of psychological issues among family members who experienced shock events such as disease, death, loss of employment, income loss, natural disasters, conflicts, and other adverse events. 18 This aligns with studies from other countries that have highlighted the long-term consequences of household shock events.16,38–41 For instance, Alem and Tato (2023) analyzed South African National Income Dynamics Study (NIDS) panel data and found that the death of a family member and loss of income were significantly associated with psychological issues. 38
The peculiarity of our study is that we have also assessed the beneficial role of entertainment and recreational tools in reducing the occurrence of psychological issues. The availability of video players, mobile phones, and the internet in the household reduced the likelihood of psychological issues among household members. The strong positive association between mobile and internet use and psychological issues is widely discussed elsewhere.42,43 Conversely, we have found a beneficial role of mobile and internet use in reducing the risk of psychological issues among the Senegalese household members. Similarly, those with access to video players were less likely to experience psychological issues. This aligns with the earlier studies that highlighted the positive impact of motivational and comedy videos on psychological well-being.44–46 Further, the role of digital technology in treating and preventing mental disorders in LMICs has been discussed elsewhere. 47 Similarly, in resource-deficient settings, internet-delivered programs and telepsychiatry can be used to improve access to mental health care and reduce the burden of psychological issues. 47
Further, by using language as a proxy indicator, we also attempted to assess the influence of ethnicity on psychological issues. However, we could not find a significant association between language and psychological issues, suggesting equal vulnerability among all ethnic groups in Senegal. In this regard, future research with a qualitative approach can be beneficial in investigating the unexplored underlying socio-cultural context of each ethnic group.
Our study made a significant contribution in presenting the magnitude and socio-demographic predictors of the psychological issues in Senegal. However, there is a major limitation to using secondary data from the Senegal DHS 2023. Senegal DHS 2023 did not follow any specific criteria from ICD or DSM to diagnose psychological issues. Senegal DHS had collected self-reported data on psychological issues experienced by the household members. In the Senegal DHS 2023, no clinical or psychological assessment was done to confirm the diagnosis of psychological issues. Self-reported information as an outcome variable (i.e., “psychological issues”) may lead to reporting bias. No clinical diagnosis and reporting bias may have ultimately led to underreporting of undetected cases, a major limitation of our study. This can be addressed with a national-level assessment, using standardized tools to diagnose psychological issues in Senegal. Further, at the micro-level, we recommend an integrated approach to build capacity for frontline health workers and TFH to conduct community -based screening and counseling, using telepsychiatry and other digital technology tools, 48 and to integrate mental health services into primary healthcare in Senegal.
Conclusions
The burden of psychological issues is high in Senegal, and it is closely associated with socio-demographic and behavioral factors, availability of recreational tools, and adverse life events. In alignment with the conceptual frameworks presented in earlier studies, we found a complex interaction between psychological issues, socio-economic determinants, access to resources, and exposure to stressors. At the intersection of these factors, there exists the vulnerability of the Senegalese household population to psychological issues. The stressors, such as the experience of shock events and exposure to indoor SHS, intensified the risk of psychological issues among the Senegalese household population. Simultaneously, access to certain resources, such as entertainment and recreational tools (mobile phones, the internet, and video players), was beneficial in reducing psychological issues.
The study findings are instrumental, as psychological issues are not given priority in Senegalese health policies. Considering this, to reduce the burden of psychological issues and improve mental health care delivery in the country, Senegal should prioritize strategies to reduce the burden of psychological issues in its national health policy.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
We are grateful to the Demographic and Health Surveys (DHS) Program, Rockville, MD 20850 USA, for authorizing the use of the Senegal DHS 2023 dataset for this study.
Reporting Guideline (Supplementary Online Material)
Name: The STrengthening the Reporting of OBservational studies in Epidemiology (STROBE)
Citation: von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 2007; 370: 1453–1457.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethical Approval
Separate ethics approval was not applicable to this study, as the DHS program has issued the authorization letter (dated. 11 August 2025) in the name of the corresponding author (and affiliating organisation), clearly mentioning that separate ethics approval is not needed for any registered study, as the DHS data does not include personal identifiers and geographical details, and does not include clinical data. The current study uses secondary collective data without names, and these details of any human/s interviewed by the DHS program. There was no separate collection of primary data. The study has followed all protocols specified in the authorization letter issued by the DHS program.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable, as there was no data collection for primary data. The study analyzed only the secondary data issued by the DHS program.
Prospective Registration
Not applicable.
Citation Diversity Statement
We acknowledge the importance of citation diversity in academic research. Among the 48 references cited, around 33% have women as first authors. Geographically, ~29% of citations are from African researchers, reflecting the study's focus on Senegal. We made a conscious effort to include literature from low- and middle-income countries; however, we acknowledge that Western publications remain overrepresented and encourage future work to further diversify the cited sources.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.