
Abstract
India’s counseling psychology landscape features a mix of regulated professionals and supervised lay counselors in task-sharing models, alongside unregulated practice by unqualified individuals offering psychotherapy via online platforms and short courses amid a large treatment gap in mental health services. While supervised lay counselors play a constructive role in evidence-based task-sharing under specialist oversight, unregulated practice risks inconsistent quality and client harm. Statutory title protection, tiered workforce models, and enforcement against deceptive mental health services are urgently needed in India.
India has seen a rapid expansion of mental health counseling services, accelerated by COVID-19. However, the current mental health treatment gap has enabled self-styled counselors to operate without regulation or training. Media reports have highlighted instances where domestic violence survivors received “avoid your husband” advice, and de-addiction center staff used forged credentials. The Mental Healthcare Act (MHCA) 2017 recognizes only clinical psychologists; counseling psychologists remain legally invisible. Short-term certificate courses fuel credential inflation while platforms list influencers alongside professionals. This unregulated marketplace may contribute to inconsistent quality of care and undermine public trust, further eroding legitimate counseling psychology. Statutory title protection, minimum supervised training standards, and tiered paraprofessional roles offer a pragmatic path forward.
Discussion
Over the past decade, India has seen an unprecedented rise in mental health awareness, alongside a rapid boom of counseling services in urban and semi-urban spaces. Clinics, NGOs, schools, workplaces, and online platforms now routinely advertise counseling, therapy, and mental wellness packages to diverse populations.1–3
These trends were accelerated during the COVID-19 pandemic by normalizing remote and online psychological support. Reviews from the Indian context describe a rapid expansion of tele-counseling services during and after lockdowns, as individuals sought help for anxiety, grief, and socio-economic stressors through hotlines, apps, and video-based platforms, often for the first time. Longitudinal and narrative accounts suggest that this period increased mental health awareness and entrenched a preference for flexible, low-threshold counseling options, while creating new opportunities for psychologists.4–7 This expansion contributed to destigmatizing help-seeking, but it also created fertile ground for individuals with minimal or no formal training in psychology to position themselves as counselors, therapists, or mental health experts.
Scroll.in’s Common Ground series describes clients who sought help from social media-driven “breakup experts” and “marriage counselors,” only to receive generic, trivializing, or unsafe advice in the face of complex issues like intimate partner violence. 2 Matharu (2023) details how a client, after seeking online therapy during a marital crisis, encountered a “therapist” who shared his own suicidal ideation and later invited her to become a counselor on the same platform. 3 Navya documents the growth of unqualified online psychotherapists in Bengaluru who may breach confidentiality, harass clients, or offer quasi-spiritual solutions for severe distress. 8
These accounts are isolated anecdotes, but they point to a deeper structural problem: India has normalized counseling as a commodity without legal, educational, or professional safeguards, enabling self-styled “lay counselors” to offer unsafe advice on complex issues.
A lay counselor refers to a non-specialist individual without formal psychology qualifications, often trained via short courses to provide basic psychosocial support under supervision in task-sharing models. 9 In contrast, a counseling psychologist is a trained professional with at least a master’s degree in psychology, supervised clinical hours, and expertise in non-directive talk therapy for everyday stressors, relationships, and adjustment issues, 10 distinct from clinical psychologists focused on diagnostic. 11
India has a severe shortage of mental health professionals, which has made some form of task-shifted psychological support inevitable, particularly in public and primary care settings. 1 There is evidence of collaborative care trials that demonstrate the effectiveness of lay or non-specialist counselors in delivering brief structured interventions when carefully selected, protocol-trained, and supervised. They highlight the potential use of lay counselors to improve recovery from common mental disorders and increase contact coverage for depression through lay counselors.12–15
This viewpoint, therefore, does not dismiss all lay providers; rather, it concerns the unregulated, unsupervised, and often self-styled practice that has proliferated in parallel to these evidence-based models. This has created a confusing landscape where clinically valuable lay roles coexist with unsafe quasi-therapeutic practices. This threatens not only individual clients but also the credibility of counseling psychology.
Approach to Evidence and Scope
This viewpoint draws on policy analyses, empirical studies, and illustrative reports to argue for regulatory reform. These reports are illustrative and not intended to represent prevalence. Sources were selected to represent documented cases of lay counseling harms, regulatory gaps, and proposed solutions. No primary data collection occurred; the analysis focuses on patterns across journalistic case studies, credential-deception incidents, and expert commentary to construct a coherent argument for regulatory reform.
Terminology
For clarity in this viewpoint, lay practice denotes non-specialist activities, such as psychoeducation, validated screening, supportive listening, and basic behavioral strategies, delivered under protocol and supervision rather than as independent psychotherapy. Lay persons/providers are individuals without accredited psychology qualifications or statutory licensure who may nevertheless receive focused short-course training to deliver such services (e.g., peer supporters, community health workers, or short-course graduates). All three terms in this article describe task-limited roles that require supervision, staged competency assessment, and explicit referral pathways to licensed mental health professionals.
Constructive Roles for Lay Counselors
Empirical Support for Supervised Lay Interventions
Lay counselors or non-specialist workers can play a constructive role in delivering brief psychosocial interventions when embedded in structured, supervised programs with clear task boundaries. The MANAS (MANashanti Sudhar Shodh) trial, a cluster randomized study in primary care in Goa, showed that a collaborative stepped-care model led by trained lay health counselors, offering psychoeducation, behavioral strategies, and case management under specialist supervision, improved 6-month recovery rates for depressive and anxiety disorders, particularly in public facilities.13,14 Building on this approach, the Healthy Activity Program (HAP) systematically developed a lay counselor-delivered behavioral activation intervention for severe depression.16,17 These trials have demonstrated that such brief therapies can reduce symptom severity and disability when delivered within a defined protocol and supervision structure.
Further evidence of a successful tiered model can be seen in VISHRAM (the Vidarbha Stress and Health ProgRAM), a grass-roots community-based program in rural Vidarbha. They have combined community health workers, lay counselors, and specialist back-up to substantially increase the proportion of people with depression who access care. Contact coverage for current depression in VISHRAM villages increased roughly six-fold, with concurrent improvements in mental health literacy.12,18 These models suggest that lay counselors can be effective bridges between communities and formal services when their role is carefully scoped and linked to a broader system of care. 19 Global task-sharing literature refers to research showing that trained lay counselors can deliver mental health interventions effectively under supervision.9,20 This supports their role in bridging gaps. However, it is essential that training, supervision, and governance mechanisms are robust.
Distinguishing Legitimate Lay Roles from Self-styled Therapists
The positive potential of lay counselors does not extend to all forms of lay practice, however. Programmatic models like VISHRAM, 12 MANAS,13,14 and HAP,16,17 use transparent recruitment, multi-week training, and supervision, unlike unregulated self-styled therapists. In contrast, current media reports from Indian cities describe self-styled “therapists” and “relationship experts” with minimal or undisclosed training, who operate outside any organizational structure, and offer psychotherapy for complex conditions. They also use misleading or unrecognized credentials to signal expertise.2,21,22
It is therefore necessary to distinguish between evidence-based lay counselors and unregulated lay practice in the Indian legal context. Recent analysis from the Indian Journal of Psychological Medicine argues that certifying laypersons as community-based mental health counselors can be ethically justified to address access gaps, but the process remains legally tenuous unless anchored in statutory frameworks and institutional oversight. The challenge for counseling psychology in India is thus not whether lay counselors should exist at all, but how to formally recognize, train, and govern a paraprofessional layer that complements professional counseling and psychotherapy rather than a “substitution.” 19
Lay Counseling, Short Courses, and Credential Inflation
Currently, a thriving ecosystem of short-term training has emerged alongside informal providers and influencers. Certificate programs in counseling, often run by private or online institutes, admit individuals from any disciplinary background and promise that graduates can start their own counseling practice, sometimes after only a few months of largely theoretical exposure. 1 These offerings blur the line between introductory education and professional qualification, especially when their marketing materials highlight employability, clinical roles, or entrepreneurial opportunities.
Matharu (2023) notes that, in the current environment, almost anyone with a master’s degree, or even a brief bridge course, can claim the title of therapist or counselor. There are cases in which professionals trained in dentistry, homeopathy, or unrelated disciplines obtained psychology degrees from open universities or unregulated private colleges and then began offering therapy for serious mental illnesses, including depression and phobias, as well as spiritual or financial counseling. 3 The lack of clear standards for what counts as “enough” training makes it difficult for clients, employers, and even policymakers to distinguish between paraprofessionals (supervised lay roles) and professionals (degree-trained psychologists).
In 2026, vigilance officials in Punjab arrested a counselor at a government de-addiction center after discovering he had secured his post using an unrecognized or forged credential. 23 Investigations in Delhi and other regions have uncovered unrecognized or unofficial degree rackets issuing credentials across multiple disciplines, which job applicants then use to enter counseling, teaching, or other sensitive roles. 24 While unrecognized or unofficial degrees are not unique to psychology, their presence in counseling contexts raises particular ethical concern, given the vulnerability of clients and the intimate nature of therapeutic work.
The net effect is credential inflation: as more people acquire questionable or superficial qualifications, the signaling value of legitimate counseling degrees decreases. This creates market confusion about established professions, as clients do not understand or are unaware of the differences.
Harm and the Erosion of Public Trust
The harms caused by unqualified counseling are often subtle, relational, and cumulative, which makes them difficult to quantify. Nevertheless, the narratives collected by journalists and professionals reveal recurring problematic practices. Minj (2025) describes sessions where a domestic violence survivor was simply advised to “avoid” her abusive husband, and where a client was encouraged to interpret her partner’s friendships as evidence of infidelity, both of which trivialize risk and reinforce victim-blaming. 2 The same report highlights NGO-based “counselors” who have not studied psychology, routinely forget details, allow interruptions, and respond to disclosures in ways that feel more like gossip than therapeutic engagement.
Matharu (2023) offers examples of “unqualified or unregistered providers,” “self-styled therapists” or “providers practicing beyond their scope of training,” who share their unresolved trauma with clients, abruptly terminate calls when overwhelmed and recommend superficial distractions such as “watch south Indian movies to feel better” in response to serious distress. 3 Navya (2022) warns of online psychotherapists who may threaten or blackmail clients, or breach confidentiality, with few effective mechanisms for redress. Such experiences do not merely fail to help; they can exacerbate symptoms, increase self-blame, and discourage future help-seeking. 8
When people encounter counseling framed as entertainment, a motivational pep talk, or casual advice, they may come to see therapy as little more than “talking to a friend with good vibes.” After a negative experience with an unqualified provider, many clients conclude that therapy itself is ineffective or invalidating, rather than recognizing that they received substandard care. Therefore, such practices erode public trust and highlight systemic issues, such as regulatory gaps, thereby affecting service legitimacy.
The Regulatory Vacuum: MHCA 2017 and the Allied and Healthcare Professions Act
These dynamics are enabled by a striking regulatory gap. MHCA, 2017, is rightly celebrated for its emphasis on rights and access to care, yet its definition of mental health professionals is narrowly focused. The Act recognizes clinical psychologists, typically those with M.Phil. degrees from Rehabilitation Council of India (RCI) approved institutions and registered with RCI, but is silent on counseling psychologists and counselors.2,25 In practice, this omission means there is no statutory protection of the title “counselor” and no clear minimum training standards for the vast majority of talk-based practitioners.
The National Commission for Allied and Healthcare Professions (NCAHP) Act, 2021, promised to bring greater order by regulating a wide range of allied health professions through national and state councils. 26 Analyses suggest that psychology-related roles are grouped under broad categories such as “community care and behavioral health sciences,” but the Act has been slow to operationalize, and it does not yet offer a dedicated, empowered council for the distinct specializations of psychology. 1 This broad-brush categorization risks diluting the voice of counseling psychologists within a large cluster of professions.
The NCAHP Act formally recognizes “community care and behavioral health sciences” professionals, creates central and state registers, and mandates minimum hours of accredited training, assessment, and continuing education for listed cadres. For psychology, this framework offers a potential statutory home for counseling and allied roles that are currently invisible under MHCA 2017. However, counseling psychologists and related specializations must be explicitly named in the schedules, their scopes of practice clearly defined, and there must be a meaningful representation of professional bodies in the proposed councils. However, at the time of writing, detailed regulations for psychology within NCAHP remain incomplete, leaving a practical vacuum between the aspirational promise of registration and the day-to-day reality of unregulated counseling practice.27–30
The result is a regulatory vacuum: only clinical psychologists enjoy clearly defined statutory recognition, while counseling psychologists, school counselors, and other key cadres occupy a gray zone. Anyone can call themselves a counselor, whether they hold a PhD in counseling psychology or a weekend certificate in generic “counseling skills.” In such a context, it is unsurprising that market dynamics and social media visibility, rather than competence or ethics, become the main drivers of who is seen as an expert.
Online Platforms, Influencers, and the Blurring of Roles
Digital platforms have intensified these challenges. Social media, therapy apps, and aggregator websites host a mixture of licensed professionals, wellness entrepreneurs, peer supporters, and influencers, often indistinguishable to the lay public. Influencer analytics cited by Minj (2025) show a surge in mental health-related content on platforms like Instagram, where self-help reels, diagnostic labels, and “healing journeys” circulate widely. 2 Matharu (2023) documents platforms that recruit “listeners” and counselors en masse, sometimes inviting current or former clients to join as counselors after minimal vetting. 3
Without clear rules about who can offer fee-based services, platform algorithms prioritize engagement and relatability over qualifications. Clients might choose a provider based on aesthetics, relatability, or follower counts rather than training and supervision. When problems arise, such as breaches of confidentiality, harmful advice, or manipulation, there is often no straightforward regulatory body to approach, especially when the provider is not registered under any statutory scheme.
While platform-level self-regulation is not a substitute for legal frameworks, it can play a complementary role. Requiring visible disclosure of qualifications, encouraging verification of professional registrations, and clearly labeling content as psychoeducation versus therapy are possible steps. However, in the absence of protected professional titles, even such measures may have a limited impact.
A Call for Continuous Monitoring, Supervised Crash Courses, and Task-limited Roles
Lessons from Short-course and Community Health Training
India’s broader health system already relies on short, competency-based training for community health workers and mid-level providers, coupled with ongoing supervision and assessment. Evaluation of mental health literacy programs for community health workers in Karnataka, for instance, shows that focused training can improve recognition of mental disorders and reduce reliance on unhelpful treatments. But the task is primarily geared toward identification, basic support and referral rather than complex psychotherapeutic work. 31 National training manuals for community health officers, multipurpose workers, and adolescent health counselors similarly emphasize building general counseling skills, recognizing “red flag” presentations, providing psychoeducation and adherence support, and knowing when and where to refer.32–34
Analogous principles underpin the “crash course” model used during the COVID-19 pandemic to rapidly train frontline health workers under the Pradhan Mantri Kaushal Vikas Yojana (PMKVY) scheme. These courses combined compressed classroom inputs with extended on-the-job training and multi-step assessments to ensure that candidates were competent for clearly defined job roles, rather than being positioned as independent clinicians.35,36 Together, these experiences suggest that short-duration training can be justified only when coupled with clear task profiles, supervised practice, staged assessments, and pathways for continuous professional development.
Proposed Task Limitations and Monitoring Mechanisms for Lay Counselors
Translating these lessons to counseling psychology, the article proposes that any cadre of lay counselors or short-course graduates be restricted to a clearly defined, task-limited scope focused on early identification, basic psychosocial support, and referrals. Appropriate tasks could include: providing structured psychoeducation about stress and common mental health problems; conducting initial, non-diagnostic screening using validated tools; offering supportive listening and simple behavioral activation strategies for mild distress; reinforcing treatment adherence; and facilitating referrals to licensed mental health professionals when red flags or complex presentations emerge. Tasks that should remain outside their remit include independent diagnosis of mental disorders, unsupervised psychotherapy for moderate to severe conditions, trauma-focused interventions, management of suicide risk or acute crises, and long-term depth-oriented therapies.19,33
To operationalize this, continuous monitoring and competency assurance mechanisms are needed. Drawing on the World Health Organization’s (WHO) task-shifting recommendations and Indian policy discussions, potential safeguards include: mandatory registration of lay counselors under a recognized institutional or council-based registry; minimum supervised practice hours before independent deployment; periodic re-certification linked to documented continuing professional development; routine supervision and case review by licensed psychologists or psychiatrists; and clear disciplinary pathways for ethical breaches or scope-of-practice violations. Embedding these requirements within NCAHP regulations or parallel professional self-regulation frameworks would help ensure that crash courses do not become de facto licenses for psychotherapy, but remain gateways to structured, supervised paraprofessional roles.19,36,37
A Pragmatic Agenda: Protecting Titles, Structuring Roles, Educating the Public
Moving beyond critique, a pragmatic four-part agenda can be introduced for addressing the lay counselor paradox in India.
The statutory protection of titles must be extended. “Counseling psychologist” and “psychologist” should become protected titles linked to defined educational and supervised training pathways, as is the case with clinical psychology under RCI. The NCAHP Act can be leveraged to create explicit sub-categories and licensure routes for counseling psychology, with clear competencies and ethical codes.1,26
A tiered workforce model is needed. Not all roles in mental health require a full professional psychology qualification; supervised paraprofessional roles such as peer supporters, lay listeners, or community mental health workers can be valuable, particularly in low-resource settings. However, these roles must be clearly distinguished from counseling and psychotherapy, with restrictions on the language they use (for example, not calling themselves counselors or therapists), the problems they address, and their responsibilities in crisis situations. 1 Evidence from task-shifting initiatives suggests that lay workers can deliver brief interventions effectively when supported, protocolized, and supervised, but unsupervised practice for complex conditions is unsafe.
The enforcement against unrecognized or unofficial credentials must be strengthened. Collaboration between health departments, education regulators, and law enforcement is essential to identify institutions issuing unrecognized or unofficial degrees and to sanction individuals who use such documents to secure counseling roles in hospitals, schools, or de-addiction centers.23,24 Publicizing these enforcement actions can help deter future misconduct and signal the seriousness with which deceptive counseling services are treated.
Public education is crucial in empowering the general public to make informed choices about mental health providers. There is confusion about professional titles and qualifications, with clients often unable to distinguish between psychiatrists (medical doctors who can prescribe medication), clinical psychologists (RCI-registered specialists trained in assessment and therapy), counseling psychologists (specialists in non-clinical talk therapy), and unregulated lay providers. Public education campaigns, led by professional bodies, platforms like Instagram/Twitter, and government portals, should clarify these distinctions through infographics, videos, and FAQs. It must be emphasized that only RCI-registered clinical psychologists and (future) NCAHP-registered counseling psychologists hold statutory protection for psychotherapy practice.
In the UK, the Health and Care Professions Council (HCPC) regulates practitioner psychologists, including counseling psychologists, via protected titles, education standards, and ethical oversight. 38 In the US, licensure requires a doctorate in counseling psychology, supervised hours (typically 3,000+), and passing the Examination for Professional Practice in Psychology (EPPP), with state boards enforcing scope. 39 India could adapt these via NCAHP for title protection and tiered registration (Table 1).
Prototype Guideline for Lay Counselor Practice Boundaries.
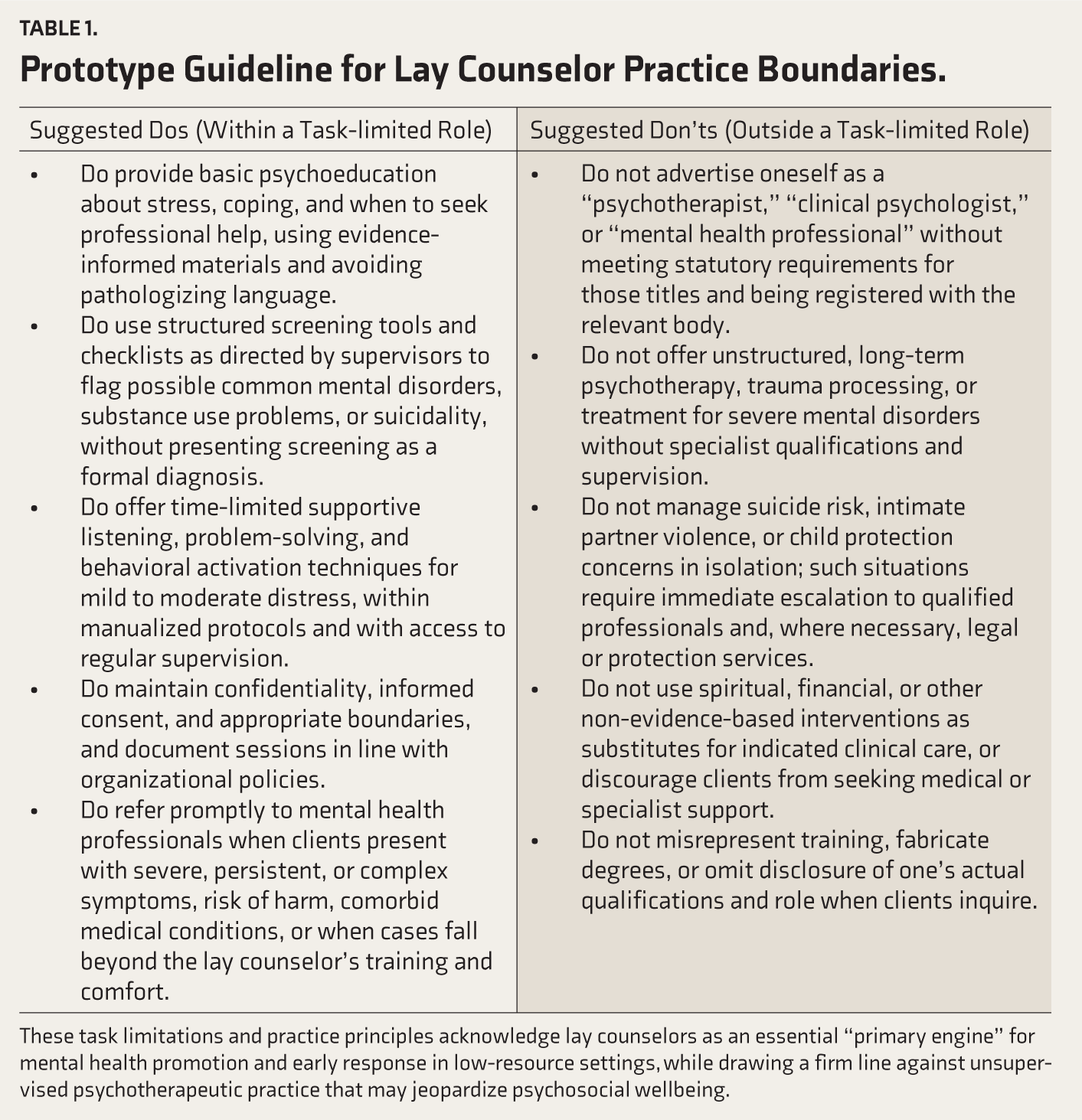
These task limitations and practice principles acknowledge lay counselors as an essential “primary engine” for mental health promotion and early response in low-resource settings, while drawing a firm line against unsupervised psychotherapeutic practice that may jeopardize psychosocial wellbeing.
Campaigns and professional bodies should also equip potential clients to ask critical questions to their “therapists,” such as information on the highest degree in psychology, and from which institution, whether they are registered with a recognized body, how many supervised hours they have completed, for what kinds of issues they refer to other professionals, and so on. These questions encourage a more informed, rights-based approach to help-seeking rather than blind trust in titles or charisma.
Conclusions
India’s mental health system is under extraordinary pressure: a severe treatment gap coexists with a plural, often chaotic ecosystem of providers. Within this landscape, the rise of unregulated lay counselors, combined with credential inflation and unrecognized or unofficial degrees, represents a systemic threat to both public safety and the integrity of counseling psychology. Media accounts from Scroll.in Deccan Herald, ThePrint, and others, the everyday harms of poorly trained counselors are made visible, along with the long shadow these experiences cast on subsequent help-seeking.
If counseling psychology is to retain public trust and assert its distinct contribution, it must take the lead in shaping regulation, defining training standards, and articulating a tiered workforce vision that integrates paraprofessional roles without romanticizing them. The choice is stark: either we build a coherent, accountable system where titles mean something and competencies are transparent, or we continue to inhabit an “everyone is a counselor” marketplace in which the line between care and harm remains dangerously blurred.
Footnotes
Acknowledgements
The authors gratefully acknowledge the work, support and insights provided by field experts and colleagues in the domains of counseling psychology and public health policy in Northeast India. No professional writing or editorial assistance was received.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
During the preparation of this work, the author used Perplexity to paraphrase and refine the language for greater coherence. It was not used as generative AI. After using this tool/service, the author reviewed and edited the content as needed and takes full responsibility for the content of the published article. The authors confirm that all references, interpretations, and conclusions were verified.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Citation Diversity Statement
We are committed to equitable citation practices and have made conscious efforts to include work from authors of diverse genders, geographic regions (including the Global South), career stages, and historically marginalized groups. We aim to support a more inclusive and representative scholarly record.