
Abstract
Background:
Mental health experts commonly rely on subjective interviews and resource-intensive projective tools to assess adolescent mental health problems. A validated Hindi version of the depression, anxiety, and stress scale for youth-21-item (DASS-Y-21) remains unavailable for the Indian adolescent population.
Methods:
The present study aimed to translate and validate DASS-Y-21 into Hindi among juvenile delinquents in India. The study complied with COnsensus-based Standards for the selection of health measurement instruments and STrengthening the Reporting of OBservational studies in Epidemiology guidelines for reporting findings. This study utilized a cross-sectional design with purposive sampling to study 351 Hindi-speaking male juvenile delinquents within the age range of 10–19 years from two detention centers across Delhi, India. The analysis was conducted in four stages: (a) descriptive statistics, (b) reliability testing, (c) confirmatory factor analysis (CFA), and (d) Rasch analysis.
Results:
All recruited participants were males with a mean age of 16.3 (±1.18) years. Descriptive and normality analysis suggested higher variability in the data. The item-rest correlations ranged from moderate to high levels. Item drop test revealed Cronbach’s (α) and McDonald’s (ω) values > 0.90. In CFA, the comparative fit index, Tucker-Lewis index, standardized root mean square residual, and root mean square error of approximation, the model showed good fit. The rating scale method (RSM) had a lower log-likelihood value (−7,989) than the partial credit model (PCM) (−7,870). CFA confirmed the good fit of the 3-factor model of DASS-Y among Indian Hindi-speaking juvenile delinquents. In Rasch analysis, PCM indicated moderate difficulty for the items.
Conclusion:
The study translated DASS-Y-21 into Hindi and evaluated its psychometric properties among Indian juvenile delinquents. Reliability tests confirm good internal consistency. Both PCM and RSM models demonstrated adequate fit with slight differences in log-likelihood values.
Keywords
Question: What are the psychometric properties of the Hindi depression, anxiety, and stress scale for youth-21-item (DASS-Y-21) for assessing mental health in Indian male juvenile delinquents? Findings: The Hindi DASS-Y-21 demonstrates good internal consistency and fits well with its three-factor structure—depression, anxiety, and stress. It has moderate item difficulty. Meaning: The Hindi DASS-Y-21 is appropriate for use among Indian juvenile delinquents.Key Messages:
Mental health problems are cosmopolitan and span all developmental stages. 1 According to a nationwide survey, 197.3 million people are affected by such conditions in India. 1 Around 45.7 million individuals in India meet the criteria for depressive disorders; likewise, 44.9 million individuals meet the criteria for anxiety disorders, together prevalent in about 3.3% India population. 1 The World Health Organization (WHO) states that one in seven adolescents (14.3%) belonging to the age group of 10–19 years experience mental health problems, and most of these problems go unnoticed and untreated until they reach the age of maturity.2–4 Similar trends were reported by other studies, with depression being prevalent among 14.19% of Indian adolescents.1,5 This may be attributed to the rapid changes in biopsychosocial domains during the phase of adolescence and certain learning disabilities, making them more prone to developing such negative emotions and related mental health problems.5,6 This rate further elevates in the forensic sample to 19.51% of juvenile delinquents exhibiting characteristics of mental health disorders. 7 The term Juvenile here depicts an individual coming in conflict with the law under the age of 18 years. 7 Meanwhile, the term adolescent depicts an individual experiencing biopsychosocial changes between 10 and 19 years of age.6,7 In this study, the researchers used these terms interchangeably, depending on the context of the Juvenile Justice System and the psychological characteristics of the study sample, respectively.7,8
The rising menace of juvenile delinquency has also highlighted growing concerns over mental health problems prevalent among juvenile delinquents.7,8 And it is worth noting that these mental health problems find their way into adulthood in the absence of timely intervention. 6 Literature indicates that mental health issues such as depression, anxiety, and stress frequently co-exist among adolescents; however, studies evaluating them simultaneously are limited in number, with most of them concentrating only on the interrelation between depression and anxiety.6,9,10 Primary gaps in this regard are the availability of psychometric assessment tools and procedures for adolescents. Mental health practitioners exclusively rely on subjective interviews and resource-intensive projective tools like the Rorschach psychodiagnostics or the Draw-A-Person test to assess adolescent mental health. 7 These tools may provide deeper insights, but they lack scalability, and their reliability remains doubtful among adolescents. 7 Other self-reported adult forms like the original DASS-Y-21-item adult form, for instance, provide a quicker screening for underlying mental health problems and therefore, have been extensively used among adolescents for screening purposes.5,11 However, researchers have questioned its validity among adolescents due to its factorial structure, complex wording, and poor comprehension.3,12 Keeping this in mind, Szabo and Lovibond developed the DASS-Y for children and adolescents aged 7–18 years. 11
Although DASS-Y is relatively new, several validated translations are available in various languages, except Hindi. 13 It is also worth noting that most DASS-related studies focused on the adult version of DASS-21 for providing a formal diagnosis of mental health problems among adolescents, 14 and those that utilized DASS-Y are mainly based on community settings like schools in the Western context.11,13,15,16 As mentioned earlier, many authors have also raised concerns about inconsistencies in the factorial structure of DASS-Y relative to its predecessor, with some items (e.g., Items 5 and 17) not suitably adapted to and underperforming in particular settings such as China or Indonesia.3,15,17,18 This further raises concerns regarding the lack of validation and reliability of this tool in clinical or specialized settings like juvenile detention centers. Despite the shortcomings, the DASS-Y has made its place in clinical settings for the assessment of depression, anxiety, and stress among adolescents due to its strong psychometric properties3,4,11 and therefore, this tool was utilized for conducting this study. However, the lack of documented evidence of the internal reliability and factorial validity of the DASS-Y in the Indian context creates a significant geographical and cultural gap, limiting its applicability to India’s multilingual, culturally diverse population.4,10,13 This also raises concerns about whether the original DASS-Y can be used among the Hindi-speaking juvenile delinquents amidst the rising rate of juvenile delinquency.12,15
Rationale for the Study
There is a substantial growth in adolescent-led offenses that raises concerns about delinquency. 19 Such individuals are at an increased risk of developing mental health disorders when compared to the community population19,20 further contributing to the onset and perpetuation of several externalizing behaviors. 21 This suggests an urgent need for a valid assessment tool to assess broader mental health problems like depression, anxiety, and stress among Indian adolescents. This study included only male participants from detention centers, as these centers are overrepresented by male adolescents both globally and in India.7,9,11 Even though higher levels of internalizing problems are reported among female counterparts, the proportion of male juvenile delinquents outweighs the former, which further necessitates a valid assessment tool to assess depression, anxiety and stress among Indian adolescents.7,9,11 Earlier versions of DASS, with 21 and 42 items, did not perform well at capturing and differentiating among emotional states in adolescents.3,19 Keeping this in mind, DASS-Y was designed to be in simplified language and address the problems related to the comprehension of its items among adolescents.3,11 Although DASS-Y has been an indispensable aid in early identification of symptoms of mental health disorders since its inception in the clinical field, there is no validated Hindi-translated DASS-Y 21-item scale in existence. Thus, the authors in the current study translated the DASS-Y into Hindi and evaluated its psychometric properties, that is, reliability, factorial validity, and item-level functioning of the Hindi DASS-Y 21-item scale, among Hindi-speaking male juvenile delinquents from Northern India, to address current gaps in mental health assessment tools available in this context. Providing a valid tool in this line will help clinicians detect internalizing problems early, differentiate between negative emotional states contributing to delinquent behavior among adolescents, and thereby provide policymakers with an aid in formulating tailored management guidelines to address issues related to delinquency.5,7
Hypotheses
H1: The Hindi-translated DASS-Y 21-item scale shows satisfactory reliability and factorial validity.
H2: All 21 items of translated DASS-Y significantly load on their respective latent factors, supporting the original factor structure of DASS-Y.
H3: All items based on Thurstone thresholds and Tau thresholds analyses demonstrate good fit with satisfactory performance.
Aim
By keeping the above facts in mind, the present study aimed to translate and validate the DASS-Y into Hindi among Hindi-speaking juvenile delinquents in India and evaluate the psychometric properties of the DASS-Y-21-item scale.4,11,13,19,22
Objectives
The objectives were: (a) To conduct cross-cultural adaptation by translating the DASS-Y into Hindi using the forward-backward translation method for juvenile delinquents.3,4,12,15,18 (b) To evaluate the internal consistency reliability of translated DASS-Y among juvenile delinquents.3,13,16,18,22,23 (c) To evaluate factorial validity and confirm whether the theoretical three-factor structure (depression, anxiety, and stress) of the original DASS-Y holds good for data collected from juvenile delinquents from detention centers using confirmatory factor analysis (CFA).3,12,16,19,22 (d) To evaluate item-level validity and scale functioning among juvenile delinquents with the help of polytomous Rasch analysis to ensure that the participants correctly understand the items of the scale.3,18,24,25
Methods
Ethical Considerations
The Institutional Ethics Committee approved the study. Written informed consent/assent was obtained from all participants and their legal guardians, with a verbal explanation of the aim and procedure of this study. Participants were informed that any information collected during the interview would be kept confidential, and their refusal to participate would not affect the status of juvenile court proceedings or their stay in the detention center.
Study Design
The study complied with COnsensus-based Standards for the selection of health Measurement Instruments (COSMIN) guidelines 26 for designing and reporting the properties of the DASS-Y 21-item scale, and with the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE)27 checklist for cross-sectional observational studies. For compliance, completed COSMIN and STROBE checklists are documented as Supplementary Online Material. This is a cross-sectional study using purposive sampling to evaluate the psychometric properties, reliability, and factorial validity of the Hindi translation of the DASS-Y 21-item scale. Purposive sampling allowed the researchers to adhere to the inclusion and exclusion criteria while balancing accessibility in recruiting participants aligned with the study’s objectives.3,12
Study Participants and Settings
The study enrolled only Hindi-speaking male juvenile delinquents (n = 351) within the age range of 10–19 years 4 from two detention centers or observation homes across Delhi, India7,11 who could comprehend Hindi-translated items on the questionnaires and were willing to provide their assent or consent for participation. Individuals with a formal diagnosis of intellectual or psychiatric impairments revealed from their case files were considered for exclusion from the data collection process. On identification, they were referred to the administration for further referral to mental health services available within the facility.
Sample Size Calculation
The sample size was calculated by using the “Population Sample Size Formula” mentioned below.
where n = sample size; Z = z-value (the number of standard deviations from the mean, based on the confidence level, for example, 1.96 for 95% confidence); P = Estimated proportion of the population (0.5 for maximum variability); and E = Margin of error (often set at 0.05). In accordance with the determined sample size of 384 participants, a total of 384 responses were collected. However, 33 out of 384 responses contained incomplete details, missing entries, or lacked both assent and consent. These responses were excluded from the final dataset for data analysis, comprising 351 participants.
Tools
The DASS-Y is a 21-item scale with three sub-scales: (a) depression, (b) anxiety, and (c) stress, each containing seven items. The authors translated the DASS-Y 21-item scale into Hindi, which was administered to the study sample to assess depression, anxiety, and stress using simplified, age-appropriate language. This scale was originally published by Szabo and Lovibond in April 2022. 11 The scale uses a 4-point Likert response format based on the original DASS-Y, ranging from 0 (Not True) to 3 (Very True). DASS-Y is based on the tripartite model, eliciting both “Depression” and “Anxiety” as latent factors sharing a common core component of negative affect called general distress; however, they differ from each other in Anhedonia (low positive affect), specific to depression only, and physiological hyperarousal, specific to anxiety only.4,16 For non-specific arousal, Lovibond and Lovibond proposed “Stress” as a third latent factor exhibited in the form of inability to relax, overreacting, tension, impatience, and irritability. 16 This scale is an extension of the adult form-DASS-21, reworded to adapt to adolescents. It was developed to assess negative emotional states among children aged 7–18 years. 11 Participants rate their experiences over the past week (the last 7 days). Each domain gives a score of 21, and the total score ranges from 0 to 63.11,16 The mean score for depression was 8.889 ± 6.356, for anxiety 8.293 ± 5.549, for stress 6.567 ± 5.633, and the mean score for the overall DASS-Y-score was 23.749 ± 15.955 for the current study sample. There are five severity levels as per the overall scores in each sub-scale, ranging from normal to extremely severe.11,16,17 DASS-Y has shown high reliability and validity across different cultural settings with values of both Cronbach’s alpha (α) and McDonald’s omega (ω) exceeding 0.80 in its three dimensions, indicating that it effectively differentiates between depression, anxiety, and stress.3,4,16,18,22
Translation Procedure
The Hindi translation and adaptation of DASS-Y used the forward-backwards method to ensure semantic equivalence with the original version.4, 11 Two independent bilingual experts conducted the forward translation from English to Hindi. An independent third party from the institute conducted the back-translation into English by retaining the original meaning of each item in the Hindi version of the DASS-Y 21-item scale. The revised version of the scale was sent to experts, including clinical psychologists, in the department for reviewing cultural suitability across Hindi-language dialects.4 This exercise helped in identifying and removing any inconsistencies in the translated items. It ensured ease of interpretation and maintained semantic equivalence by adapting translated items that resonate with the lived experiences of Hindi-speaking adolescents in India.4 The final Hindi-translated version of the scale was initially administered to ten random juvenile delinquents (n = 10) from the pool belonging to the spectrum of the age 10–19 years for checking the clarity, readability, and comprehension of translated items of the scale.3,16,18,22 During the administration of the items, participants were asked to verbalize any difficulty in understanding their meanings. Based on participants’ feedback, items were reworded to make the language more understandable by making minor syntactic corrections. Comments from departmental experts were sought for final correction. The final Hindi-translated scale was included in the data collection process. However, the results of this pilot testing were not published due to insufficient statistical power to evaluate the scale’s psychometric characteristics.3,4,12,16
Data Collection
The authors used pen-and-paper questionnaires. A response sheet was prepared to record participants’ responses, which was then transferred to a data sheet for analysis.
Statistical Analysis
All statistical analyses were performed using Jamovi (v. 2.7.18.0). To achieve the study objectives, analyses were conducted in four stages: (a) Descriptive statistics & normality testing, (b) reliability testing, (c) CFA, and (d) polytomous Rasch analysis. The first step included calculating descriptive statistics, including mean, standard deviations, skewness, kurtosis, and the Shapiro–Wilk normality test, to analyze the data distribution and normality. The second step included reliability testing using Cronbach’s alpha (α) and McDonald’s omega (ω) coefficients. These coefficients predicted the scale’s consistency in Hindi before examining its internal structure. In the third step, the authors performed a CFA to test the fit of the original three-factor structure of the scale (depression, anxiety, and stress as latent factors). Finally, polytomous Rasch analysis was performed in Jamovi using the SnowIRT module to apply the rating scale method (RSM) and the partial credit model (PCM).25,28 These two tests explain the item fit and monotonic functioning of response categories of the scale. This confirms whether the participant correctly understood and differentiated among levels of distress based on hierarchical responses on a 4-point Likert scale.
It is worth noting that past studies often relied on classical test theory (CTT) to address factorial inconsistencies, assuming that all items contribute equally to the total score.24,25,29 Nonetheless, to ensure the precise item-level contribution to the Hindi-translated version of DASS-Y, to identify misfit items and to verify response level distinction by the participants (e.g., “Not True” vs. “A Little True”), authors in this study relied on CFA and polytomous Rasch analysis.24,25,28
Bias and Study Size
Juvenile delinquents represent a heterogeneous population in terms of literacy levels. 20 Therefore, to maintain data collection homogeneity and remove measurement bias, items were read aloud to study participants, with relevant standardized instructions provided and any items requiring further clarification explained. A sample size of 351 provided sufficient statistical power, exceeding the recommended baseline of 10:1 respondent-to-item ratio for CFA and Rasch modeling.12,13,16
Procedure
The study followed all guidelines in the Declaration of Helsinki. 30 Hindi translation of DASS-Y relied on the forward-backward method, using the original English version of the scale. 11 The final version was used to conduct the pilot testing. After making minor corrections to the Hindi translation of DASS-Y to maintain cultural suitability and semantic equivalence, the authors proceeded to data collection. Written informed consent or assent was obtained from all participants and their legal guardians. Completed questionnaires were entered into LibreOffice Calc and Jamovi for final statistical validation.
Results
Descriptive Statistics and Normality Tests
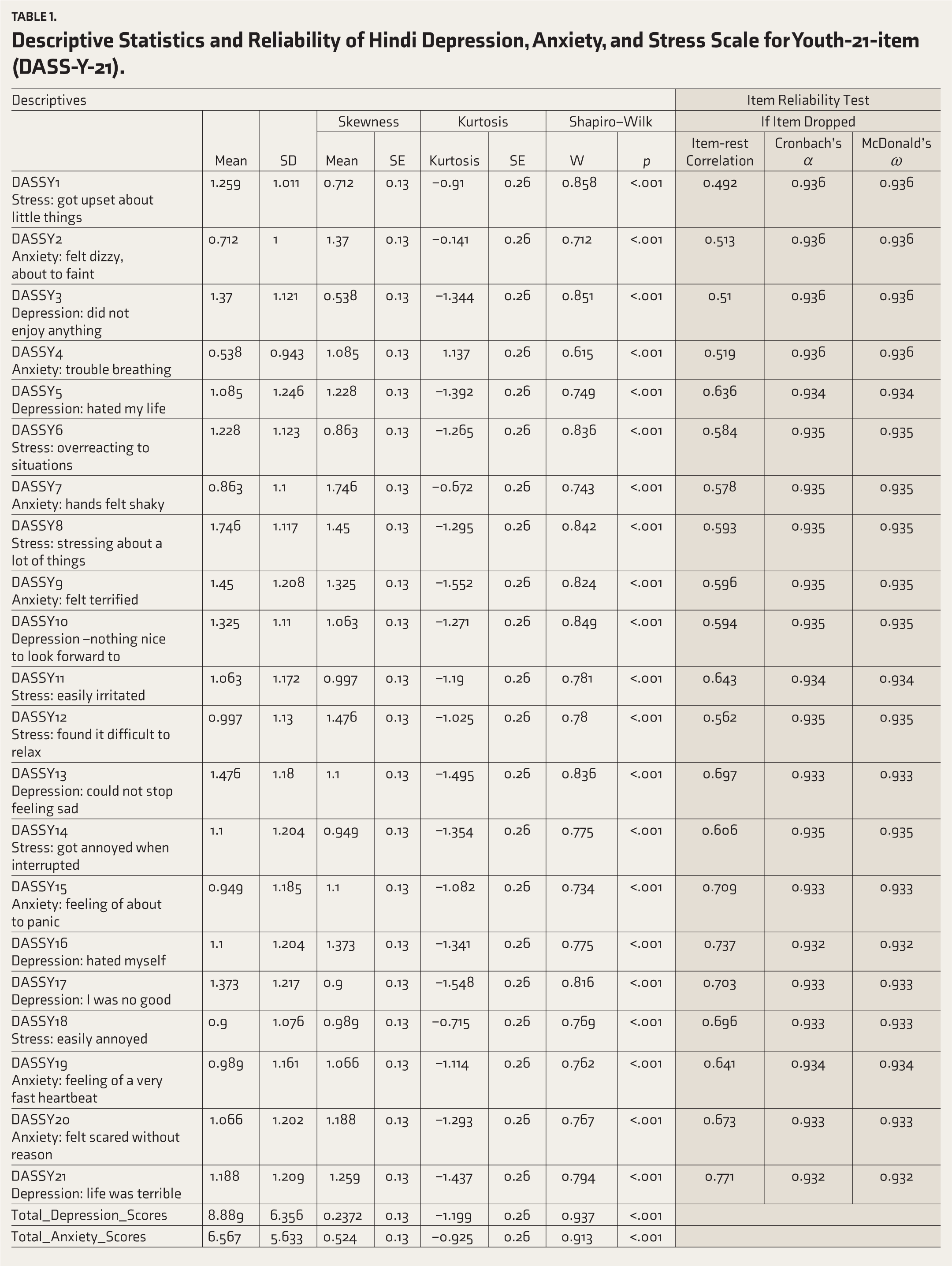
There are no missing values in the data. All recruited participants were male juvenile delinquents aged 12–19 years, with an average of 16.3 (±1.18) years. The majority of participants (n = 237, 67.5%) belonged to the upper-lower socio-economic status category, followed by lower-middle (n = 77, 21.9%). The mean values of translated DASS-Y items ranged from DASSY4 anxiety (0.538) to DASSY8 stress (1.746), with standard deviations ranging from ±0.943 to ±1.246, suggesting greater variability in the data. Many variables exhibit slight to moderate skewness and kurtosis, indicating non-normal distributions. The Shapiro–Wilk test (W) with p values <.001 for all items confirms the rejection of the null hypothesis of normality for the data (Table 1).
Descriptive Statistics and Reliability of Hindi Depression, Anxiety, and Stress Scale for Youth-21-item (DASS-Y-21).
Item Reliability Statistics
The item-rest correlations range from moderate to high, that is, from 0.492 (DASSY1Stress) to 0.771 (DASSY21Depression), and are nearly incremental, suggesting that each item contributes to the scale in a meaningful way. Item drop test consisting of Cronbach’s alpha (α) and McDonald’s omega (ω) values > 0.90, suggesting that none of the items, when dropped from the scale, significantly affects the reliability of DASS-Y, and it has a stable internal consistency. This further confirms the scale’s homogeneity and suggests that none of the items is a misfit on the scale (Table 1).
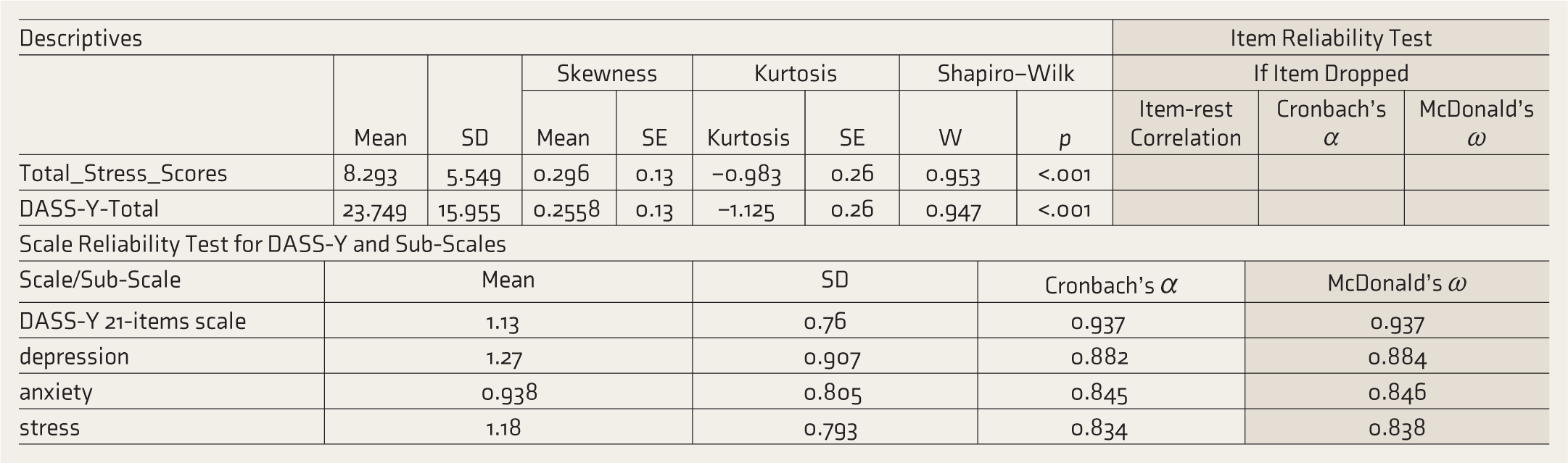
Scale and Sub-scale Reliability Statistics
The scale reliability statistics indicate high internal consistency. The mean score of the scale is 1.13 (±0.76). The values of both Cronbach’s α and McDonald’s ω are 0.937, which exceed the threshold of 0.70, suggesting interrelations among items, high consistency among them, and common underlying constructs. Furthermore, the values of Cronbach’s α for subscales depression, anxiety, and stress were 0.882, 0.845, and 0.834, respectively. Also, the values for McDonald’s ω for depression, anxiety, and stress were 0.884, 0.846, and 0.838, respectively. This further indicates the robustness of the translated scale in measuring the underlying constructs, that is, depression, anxiety, and stress (Table 1).
Confirmatory Factor Analysis
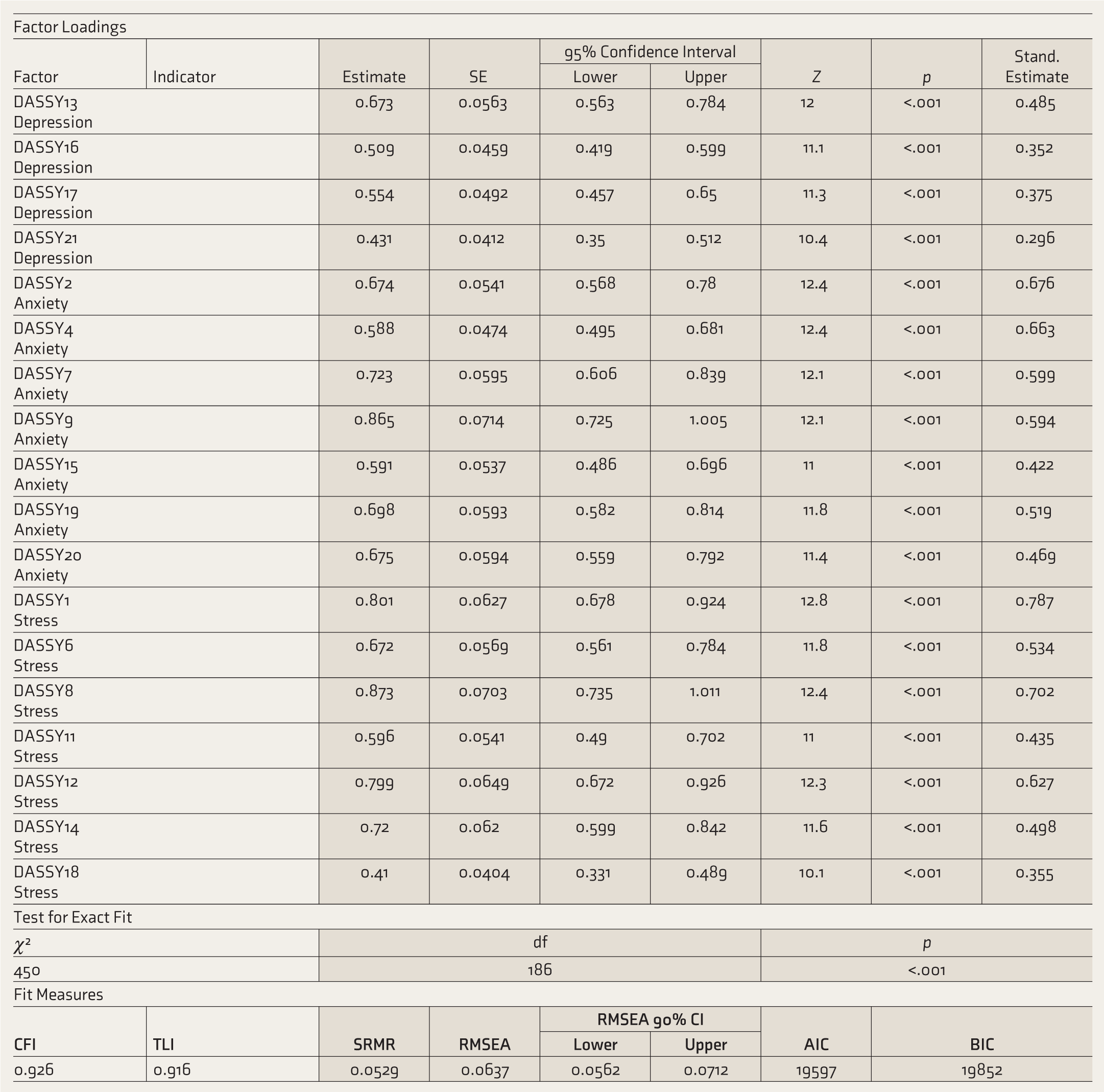
Estimates of factor loadings provide information about the degree of association between each item of the scale and the targeted or designated latent factor to which it is assigned. Here, the minimum threshold for estimation coefficients for factor loadings was set at ≥0.40. 4 All 21 DASS-Y items loaded significantly on their designated factors, further confirming that the model fits the data well (Figure 1 and Table 2).
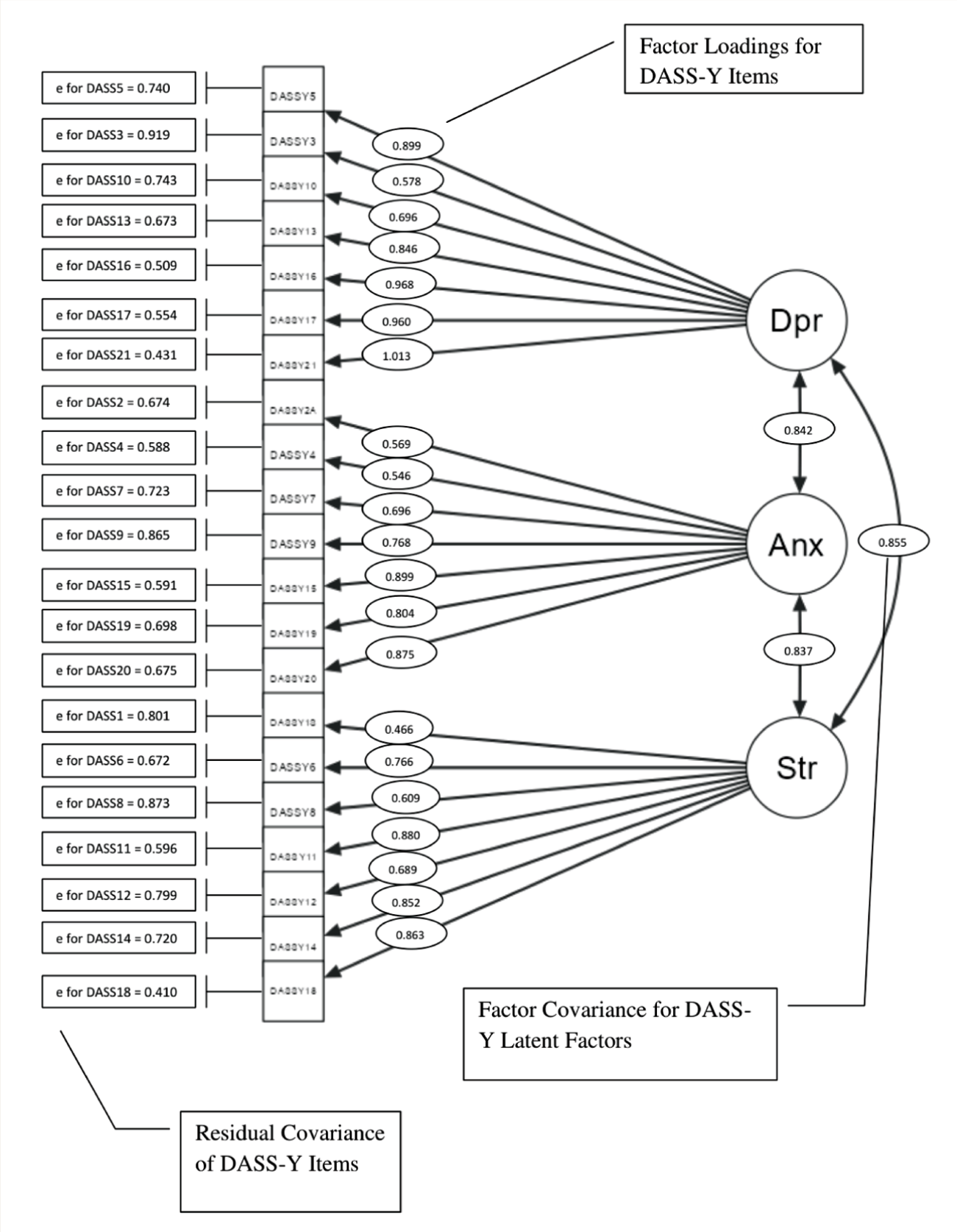
Dpr: Depression as a Latent Factor, Anx: Anxiety as a Latent Factor, Str: Stress as a Latent Factor, e = Residual Covariance for individual items.
Factor Loadings, Factor Covariance and Residual Covariance of Hindi Depression, Anxiety, and Stress Scale for Youth-21 (DASS-Y-21) Items.
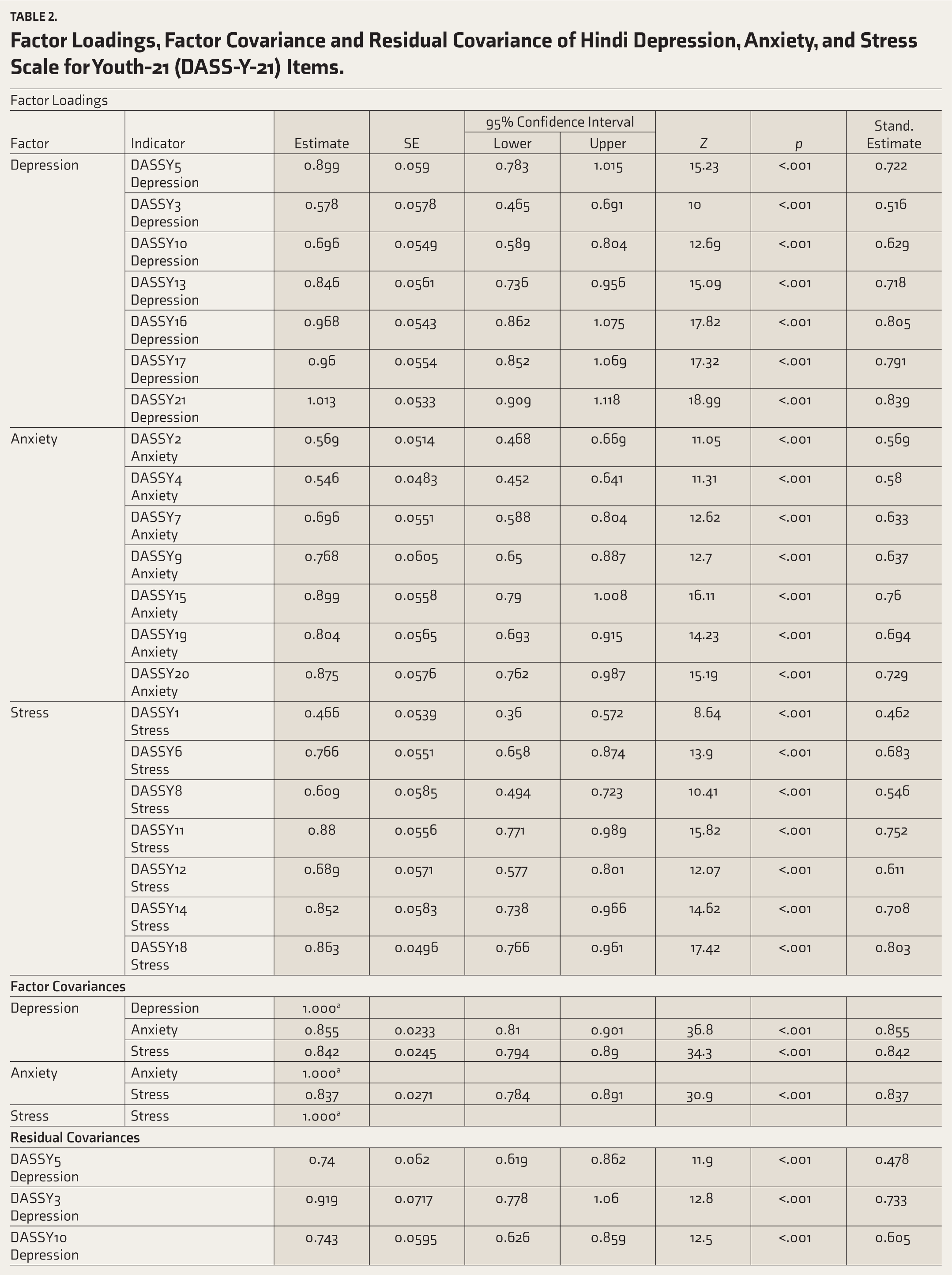
On the other hand, factor covariance reflects the strength of relationships among latent factors, suggesting common underlying constructs such as genetic preloadings. 13 The acceptable values for the estimates of the factor covariances among depression, anxiety, and stress as latent factors were set below 0.85 to ensure non-redundant inter-factor correlations. 13 Positive values for depression anxiety (0.855), depression-stress (0.842), and anxiety-stress (0.837) suggest existing stronger relationships.
The standard estimate of residual variance in CFA explains the proportion of unexplained variance in each DASS-Y item attributable to the latent factors and accounts for the contribution of these factors to the overall variation in the data. DASSY3Depression has the highest residual variance (e = 0.919) for factor depression, and DASSY18stress has the lowest residual variance (e = 0.410) for factor stress. All standard estimates attained the significant levels of unexplained variance (p < .001).
Although comparative fit index (CFI) and Tucker-Lewis index (TLI) (acceptable fit values >0.90 or ≥0.90), 19 standardized root mean square residual (SRMR) (acceptable fit values <0.10 or <0.08) 19 and root mean square error of approximation (RMSEA) (acceptable fit ≤ 0.08) 19 confirm the model’s good fit to the data.
Polytomous Rasch Analysis
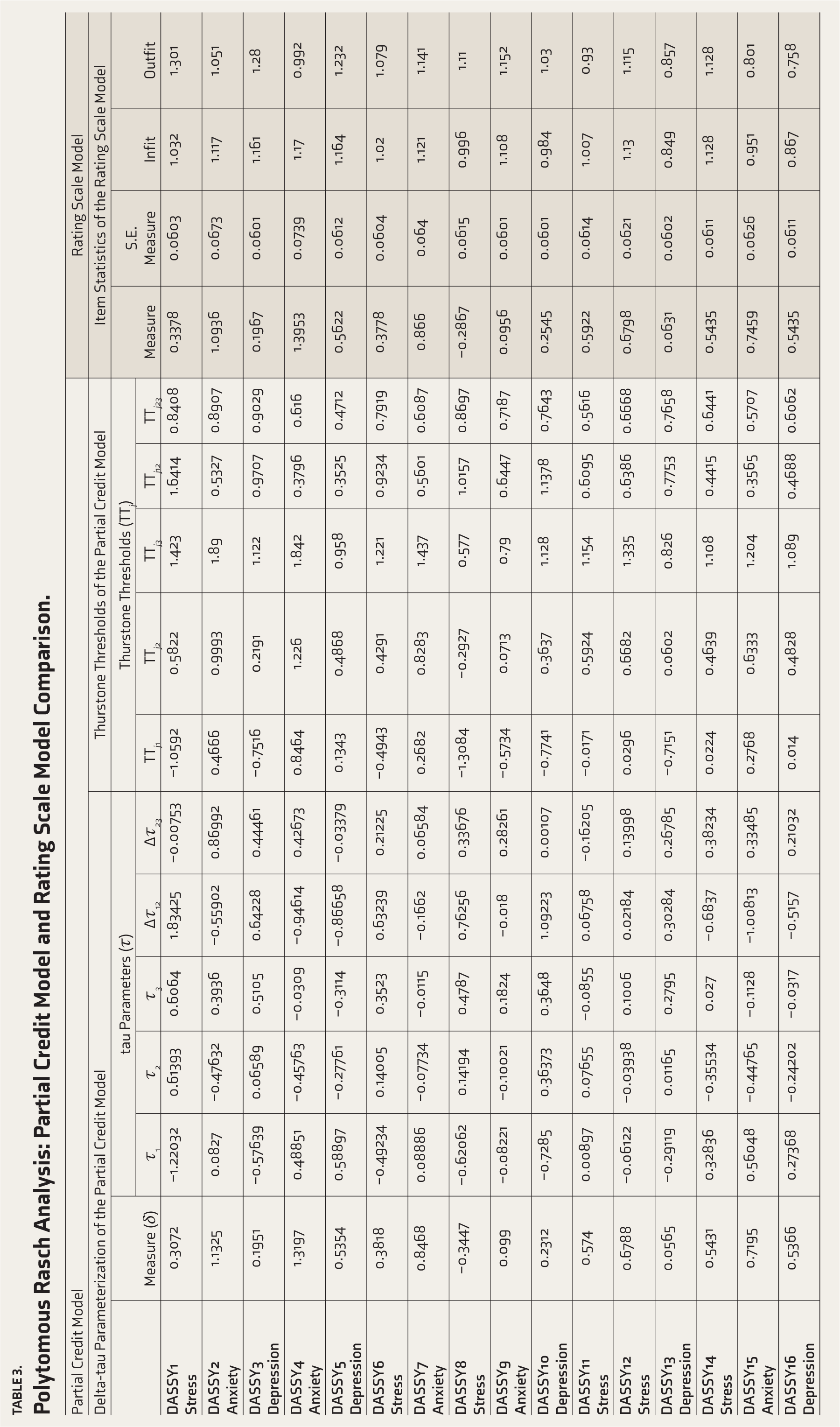
Table 3 contains information about the PCM, the RSM, and their comparison. In the PCM, measure (δ) ranges from −0.3447 (DASSY8) (item with lowest difficulty) to 1.3197 (DASSY4Anxiety) (item with greatest difficulty). Most items oscillate between 0.0 and 0.8, suggesting moderate difficulty levels. In the dataset, most Δτ values are moderate (Table 3).
The DASSY17Depression is an outlier (Δτ23 ~0.0004). This may indicate overlap between the second and third response levels for the item. DASSY3Depression (Δτ12 = 0.64228, Δτ23 = 0.44461) indicated clear boundaries within responses. For DASSY5Depression (Δτ12 = −0.86658, Δτ23 = −0.03379), the third response level underperforms the threshold levels, indicating difficulty in moving from “A Little True” to “Very True.” For both DASSY16Depression (Δτ12 = −0.5157, Δτ23 = 0.21032) and DASSY21Depression (Δτ12 = −0.30841, Δτ23 = 0.19469), the second response level underperforms, that is, difficulty in moving from “Not True” to “Fairly True.” For DASSY10Depression (Δτ12 = 1.09223, Δτ23 = 0.00107), the first response level “Not True” underperforms and may be perceived as fairly easy to be neglected by the respondent.
Polytomous Rasch Analysis: Partial Credit Model and Rating Scale Model Comparison.
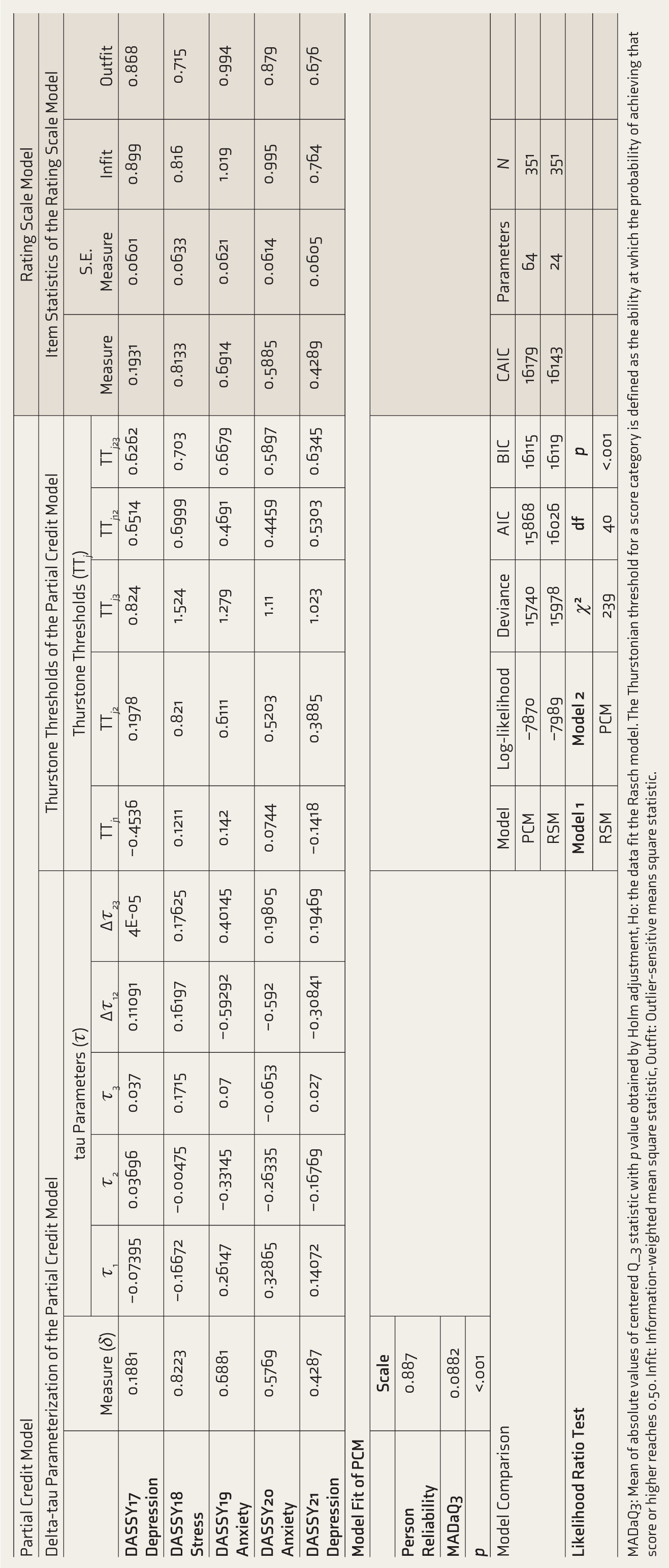
MADaQ3: Mean of absolute values of centered Q_3 statistic with p value obtained by Holm adjustment, Ho: the data fit the Rasch model. The Thurstonian threshold for a score category is defined as the ability at which the probability of achieving that score or higher reaches 0.50. Infit: Information-weighted mean square statistic, Outfit: Outlier-sensitive means square statistic.
DASSY15Anxiety is the outlier due to the extreme negative Δτ12 (−1.00813), indicating that respondents rarely reach the second response level (“Fairly True”) in the data set, suggesting the item’s poor construct. DASSY4Anxiety has a high Δτ12 (−0.94614), indicating difficulty in transitioning from “Not True” to “Fairly True.” DASSY2Anxiety has a negative Δτ12 (−0.55902), suggesting a problem in transitioning from “Not True” to “Fairly True” response.
DASSY8Stress shows a slightly higher Δτ12 (0.76256), suggesting underperformance on lower responses and difficulty choosing the “Fairly True” response. DASSY11Stress shows minimal Δτ12 (0.06758) but a higher negative value for Δτ23 (−0.16205), suggesting a smooth transition from “Not True” to “Fairly True” and difficulty while moving from “A Little True” to “Very True.” DASSY12Stress has Δτ12 (0.02184) and Δτ13 (0.13998), suggesting a smooth transition despite varied underlying thresholds across response categories.
Overall, the depression domain has three problematic items (DASSY17, DASSY5, DASSY10); the anxiety domain has three problematic items (DASSY15, DASSY4, DASSY2); and the stress domain has two problematic items (DASSY8, DASSY11).
Thurstone thresholds (TTj1, TTj2, TTj3) indicate relative response difficulty levels.25,28 Tau thresholds are defined as step-deviation parameters, while Thurstone thresholds are absolute step difficulties.25,28 In the dataset, most TTj1 values are negative, indicating that the item is lower on the construct. Step deviations (TTj2 − TTj1) are within the range of ~0.3 to 1.6, suggesting some problems with transitions. Also, (TTj3 − TTj2) falls within the range of ~0.4 to 0.8, suggesting an incremental increase in underlying severity across the response levels.
For the RSM, higher values of measure indicate a higher location on the response category. The higher the value, the greater the difficulty in marking the response, and thereby requires higher levels of latent trait. 24 Information-weighted fit (infit) is the measure of the underlying pattern of consistency 24 and Outlier-sensitive fit (Outfit) is the measure of outlying responses of the participant in picking the relevant response as per the item. 24 The acceptable range of infit and outfit is generally within 0.5–1.53,25 and any deviation beyond these values indicates randomness in responses.3,25 For instance, the item difficulty measure for DASSY1Stress is 0.3378 beyond the average values of 0.0 18 indicating that this item is slightly more difficult than the average item in the scale and therefore, requires higher levels of the underlying trait like depressive symptoms for choosing the higher categorical response. 24 In addition, values of infit (1.032) and outfit mnsq (1.301) for DASSY1Stress lies within the range of 0.5–1.5 18 suggesting that the item performs as per the expectations of the proposed three-factor model. 11 As per RSM, all 21 items of DASS-Y demonstrated good fit; however, they lie on a continuum of varied difficulty levels, for example, items with high infit but low outfit (e.g., DASSY4Anxiety: 1.17, 0.992 & DASSY11Stress: 1.007, 0.93), suggesting systematic variations in the item across the scale.
Furthermore, both PCM and RSM have comparable values of the Akaike Information Criterion (AIC) (15,868, 16,026), the Bayesian Information Criterion (BIC) (16,115, 16,119), and the Consistent Akaike Information Criterion (CAIC) (16,179, 16,143), suggesting comparable goodness-of-fit. However, RSM has a lower log-likelihood (−7,989), indicating a poorer fit than PCM (−7,870).
Discussion
The present study aimed to translate and validate the DASS-Y into Hindi among Hindi-speaking juvenile delinquents (n = 351) in India and evaluate the psychometric properties of the DASS-Y-21-item scale. Keeping the aim and hypotheses in the vision, descriptive tests were performed first. Previous studies reported variability in items and total scores for the sub-scales, that is, depression, anxiety, and stress.5,11,25,31 This variability can be attributed to various factors, including developmental stage, the DASS-Y’s structural design, and participants’ latent clinical features.5,11,25,31 For instance, in the Turkish Version of the DASS-Y, significant differences existed among psychiatric and non-psychiatric samples for scores on sub-scales, that is, depression (mean score = 10.73 for psychiatric and 3.24 for non-psychiatric sample), anxiety (mean score = 9.45 for psychiatric and 2.93 for non-psychiatric sample), and stress (mean score = 13.25 for psychiatric and 6.77 for non-psychiatric sample). 16 In the present study, mean scores of items (ranged from 0.538 to 1.746 with standard deviations of ±0.943 to ±1.246), sub-scales: depression (8.889 ± 6.356), anxiety (6.567 ± 5.633), and stress (8.293 ± 5.549), and overall DASS-Y (23.749 ± 15.955) were higher than the reported scores for the non-psychiatric population and lower than the psychiatric population. 16 There could be several reasons for such variations in the scores: (a) DASS-Y readily captures subthreshold symptoms because of graded severity levels, keeping scores of respondents oscillating around the mean values or in between non-psychiatric and psychiatric populations.5,11 (b). Individuals with a history of mental health problems exhibit higher levels of variance in mean scores. 31 (c) With developmental transitions, mean scores show a natural shift from normal to subsyndromal thresholds. 12
Next, the scale’s reliability was checked, and its factor structure was confirmed by loading the scale items onto pre-specified latent factors proposed in earlier studies.11,32 Item-rest correlations exhibit a nearly incremental nature, suggesting that each item contributes to the scale in a meaningful way. In addition, the item drop test suggests that the scale has stable internal consistency and confirms that the items are homogeneous rather than redundant or multidimensional. These findings are consistent with previous findings.12,33 Furthermore, as per the CFA findings, the significant chi-square value (χ² = 0.450, p < .001) indicates poor model fit, rejecting the null hypothesis of a perfect fit. The rejection is likely due to the large sample size or the model’s complexity.23,33 Conversely, other indices, including CFI, TLI (acceptable fit values >0.90 or ≥0.90), (SRMR) (acceptable fit values <0.10 or <0.08), and RMSEA (acceptable fit ≤0.08), confirmed the good fit of the model to the data. Similar results were reported in previous studies.4,16,18
As of our current knowledge, only three studies have performed Rasch analysis to confirm item fitness and categorical thresholds for their responses.3,18,34 Out of these, one study reported its findings in pre-prints during the synthesis of this report. 34 To achieve the objective of testing item-level validity and scale functioning, the authors performed a polytomous Rasch analysis. They compared the PCM and the RSM to clarify further. Polytomous Rasch analysis is used to analyze items in which more than two response levels or categories exist, for example, a 4-point Likert scale used in DASS-Y.11,24
The Delta-tau parameterization in PCM helps decompose the difficulty of scale items into two components. 28 Delta (δ) is one of the item location parameters in PCM, indicating the difficulty level of each item relative to the overall items. 28 Positive values of δ indicate greater difficulty. 28 Tau (τ), on the other hand, is the threshold parameter while moving from response levels. 28 Positive values of Δτ indicate ease of moving progressively from one response to another while distinguishing among different levels of response categories. Conversely, negative values of Δτ indicate that the respondent has difficulty distinguishing among the response categories.3,18,24 For this data set, measure (δ) ranges from −0.3447 (DASSY8) (item with lowest difficulty) to 1.3197 (DASSY4) (item with greatest difficulty). Most items oscillate between 0.0 and 0.8, suggesting moderate difficulty levels. Items with low and high values of δ may need revision to capture the construct’s scale fully. On the other hand, values of Δτ near zero indicate a well-defined item construct; however, large values indicate unclear boundaries within the response set. 28 In the data set, most Δτ values are moderate, and similar results have been reported in previous studies.18,28
Previous studies reported DASSY5, 18 DASSY10, 18 and DASSY173,18 as problematic items. These results are in accordance with previous studies.3,18 For instance, Cao et al. (2023) in Chinese participants and Kurnianto et al. (2025) in Indonesian participants reported differential item functioning (DIF) (also known as demographic-bias, like age or education-bias, like education level). Different meanings are assigned by the participant to the item as per age, education, and socio-cultural aspects) during the reporting of responses.3,18 Such items were removed from parsimonious versions of DASS-Y, suggesting that fewer items, that is, their removal from the scales, do not affect the psychometric properties of the scale in such settings.4,23,31 Similarly, DASSY15 (anxiety, feeling of about to panic), DASSY4 (anxiety, trouble breathing ), DASSY2 (anxiety, felt dizzy, about to faint) showed problems in the anxiety domain in the current study. Previous findings supported these findings. For DASSY2Anxiety, DIF was held responsible. 18 In addition, studies reported category disordering (difficulty in differentiating between incremental nature of response levels for given item) 3 for DASSY15 (Felt like about to panic), and poor positive factor loading for DASSY4Anxiety (trouble breathing) 32 among Chinese and Indonesian children.
Stress also includes two problematic items in this study: DASSY8Stress (Stressing about a lot of things) and DASSY11Stress (Easily irritated). Previous studies attributed this primarily to category disordering, 3 among 7–12-year-old Chinese participants and demographic bias 18 among Indonesian participants. In this study, the sample population consisted of juvenile delinquents aged 12–19 years (±16.3 years). The major reasons for these problematic items in the data set could be attributed to their socio-cultural aspects, prior encounters with the law (recidivism), low socio-economic status, and early school dropouts, which limit their psychosocial growth.3,7,18
Thurstrone thresholds (TT j ) are absolute step difficulties.25,28 In the dataset, most TTj1 values are negative, indicating that the item is lower on the construct. Step deviations (TTj2 − TTj1) are within the range of ~0.3–1.6, suggesting some problems with transitions. Also, (TTj3 − TTj2) falls within the range of ~0.4–0.8, suggesting an incremental increase in underlying severity across the response categories. Previous studies reported mixed outcomes for Thurstone threshold levels. One study reported a steady increase in threshold estimates, 18 and another reported disordered levels. 25
Outcomes of the RSM, on the other hand, suggest all 21 items of DASS-Y demonstrated good fit; however, they lie on a continuum of varied difficulty levels. Kurnianto et al. (2025) also reported similar findings. 18 However, other studies either rejected the RSM in favor of more flexible methods or multidimensional rating approaches. 3
Compared to PCM, RSM showed comparable goodness-of-fit. However, RSM had a lower log-likelihood (−7,989), indicating a poorer fit than PCM (−7,870). This is further supported by a higher deviance value (15,978) for RSM. Cao et al. (2023) reported similar findings. 3
Limitations
The analytical findings of this study include several limitations in the study design, measurement procedures, and the unique intersections between cultural and forensic settings to which juvenile delinquents belong. For instance, purposive sampling may hinder the generalizability of findings to the entire population of juvenile delinquents across India. As this study employed a cross-sectional study design, this may limit the study’s ability to explain and predict causal relationships between juvenile delinquency and mental health problems prevalent among the sample. This design also prevents establishing the temporal stability of the Hindi-translated version of the DASS-Y 21-item scale, which future studies may overcome by employing longitudinal study designs.
In the context of measurement tools, this study relied only on self-reported measures among juvenile delinquents. Such measures are susceptible to social desirability bias in forensic settings due to a fear of prolonging detention or to underlying individual traits. Future studies may overcome this by ensuring confidentiality and anonymity, using indirect questioning, conducting preparatory cognitive interviews, conducting interviews in private settings in the absence of security personnel (if possible), or relying on mixed-method approaches to reduce bias. This study also did not include a gold-standard structured clinical interview alongside the DASS-Y 21-item scale. As a result, DASS-Y’s ability to provide a formal diagnosis remains unverified in the current sample.
In the context of analytical procedures, this study relied on CFA and polytomous Rasch analysis. CFA is highly sensitive to sample size, as shown by the chi-square (χ²) test, resulting in a poor-fitting model. In addition, CFA relies on assumptions of pre-existing theoretical models and multivariate normality. This was overcome by including polytomous Rasch analysis in the statistical procedure. However, Rasch analysis has its own downfalls. Rasch analysis relies on assumptions of unidimensionality within sub-scales, which may affect the precision of item-level estimates in the measure. Future studies may improve the functioning of this test by reducing the number of items, collapsing response levels, and making the model either more comprehensive or simpler.
This study only included male juvenile delinquents as the study sample. The cultural norms and notions linked to masculinity may differ from those in Western countries, which may further prevent participants from disclosing their mental states in forensic settings. This may lead to underreporting of mental health problems like depression, anxiety, and stress. A thorough critical examination of cultural norms and notions in the context of juvenile delinquents is suggested to overcome such limitations in future studies.
Conclusions
The study aimed to translate and validate the DASS-Y into Hindi for Indian juvenile delinquents, and to evaluate its psychometric properties and item-level validity using polytomous Rasch analysis. Reliability tests confirm good internal consistency but also suggest modifications to some items to improve the scale’s sensitivity. Both PCM and RSM models demonstrated adequate fit with slight differences in log-likelihood values. Overall, this study contributes to the validation of DASS-Y and understanding related mental health problems among Hindi-speaking Indian juvenile delinquents.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
Not applicable.
Reporting Guideline
Name: COSMIN Study Design Checklist for Patient-Reported Outcome Measurement Instruments
Citation: Mokkink LB, Terwee CB, Patrick DL et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an International Delphi study. Qual Life Res 2010; 19(4): 539–549. DOI:
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethical Approval
Institutional Ethics Committee of the School of Behavioural Sciences (SBSC), Department of Clinical Psychology, Shree Guru Gobind Singh Tricentenary University, Gurugram, India
Approval Reference No.: SGTU/FBS/ECC/20245/01
Date of Approval: September 28, 2024.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent/Assent
Written informed consent or assent was obtained from all participants and their legal guardians, with a verbal explanation of the aim and procedure of this study.
Prospective Registration (for interventional studies: WHO-approved public trials registry,e.g.,CTRI)
Registry name: Not applicable
URL of the registry record: Not applicable
Registration number: Not applicable
Date of registration: Not applicable
Citation Diversity Statement
We are committed to equitable citation practices and have made conscious efforts to include work from authors of diverse genders, geographic regions (including the Global South), career stages, and historically marginalized groups. We aim to support a more inclusive and representative scholarly record.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.