
Abstract
Background:
Breakfast is considered the first and most important meal of the day. Missing the first meal may result in significant nutritional deficits, if not compensated in subsequent meals.
Aim:
To describe the nutrient intake through breakfast and to study its association with nutritional indicators among adolescent girls.
Methods:
A cross-sectional study among adolescent girls (n = 565) 16–18 years was carried out in urban slums of Pune, Maharashtra, India. Haemoglobin was assessed by cyanmethemoglobin method. Nutritional status was assessed through anthropometry and three 24-hours diet recall. Z scores, independent sample test, and linear logistic regression were used to assess undernutrition, to compare means of nutrient intake and to associate nutrient intake with nutritional status, respectively.
Results:
Almost 50% did not consume solid food for breakfast and 99% of the participants consumed inadequate breakfast (<610 kcal). Two types of breakfast emerged: I (bakery products + beverage) and II (traditional breakfast + beverage). Although the mean energy intake of type II breakfast (235±100.55 kcal) and the mean micronutrient intake was significantly higher than type I (micronutrients: vitamin C and folate (p = 0.001), iron (p = 0.01)) it did not meet the adequacy norms for breakfast. Among nutritional indicators breakfast intake was not directly associated with body mass index. However, mean intake of nutrients such as energy, protein and iron through the day were significantly lesser (p = 0.001, p = 0.01 and p = 0.01 respectively) among anaemic adolescents. Linear regression showed significant association between energy, fat intake and BAZ scores.
Conclusions:
Compensating dietary deficits that arise in the first meal would directly address the day’s nutrient deficit. The results highlight the need for a food-based approach to address undernutrition among adolescent girls in resource-poor settings.
Introduction
Breakfast is considered the first and most important meal of the day. It varies culturally, with the timing of the day and the foods consumed (O’Neil et al., 2014). Work carried out in Maharashtra, India, has defined breakfast as any food item, solid or liquid, consumed at the beginning of the day. Nutritionally adequate breakfast has been defined as one that provides one quarter of the nutrient requirement of the day (Sivaramakrishnan and Kamath, 2012). Benefits of consuming breakfast range from providing energy for the brain after an overnight fast, providing macro and micronutrients to meet the daily requirements, reduced risk of overweight and obesity (Blondin et al., 2016) , improved learning (Adolphus et al., 2013), to developing healthy food habits (Wurtman and Wurtman, 1977; Gajre et al., 2008; Gikas et al., 2003).
Adequacy of breakfast has been studied among various age groups in different settings. In developed countries, inadequate intake of breakfast is known to increase the risk of overweight and obesity (Thompson-McCormick et al., 2010). Children who skipped breakfast in these settings had increased waist circumference (Song et al., 2005). Similar observations were reported in developing countries among the higher socio-economic status (Arora et al., 2012; Kuriyan et al., 2012). On the contrary, in developing countries nutrient inadequacy in the first meal, followed by inability to compensate in the subsequent meals results in undernutrition (Sethi and Dangwal, 2001). The reasons may be food insecurity, cultural influences or restricted time for food preparation (Bartfeld and Ahn, 2011; Howden et al., 1993).
In India, data on breakfast consumption of school-going children is available through a few regional studies. However, national level data on dietary intake of adolescents and specifically breakfast intake are limited. Among the few regional studies available, work carried out in Andhra Pradesh showed that more than one-half of the schoolchildren skipped breakfast at least few times per week (Chitra and Reddy, 2007). However, adolescents who are school dropouts are least studied. Work done in rural areas about overall dietary intake reported that adolescents diet lacked diversity and were cereal based (Malhotra et al., 2007). Consequence of nutritional deficits among adolescent girls from the lower socioeconomic strata is of interest, in light of the high prevalence of maternal and child undernutrition. In India, iron deficiency anaemia (IDA) is also widespread among women of reproductive age (NFHS, 2016). Undernutrition in pregnancy has been documented as the major cause of poor pregnancy outcome such as low birth weight (LBW), stillbirth, perinatal morbidity and mortality in developing countries. Therefore, the present work was carried out to study the breakfast habits of adolescent girls 16–18 years of age from the urban slums of Pune city. This work aimed
to study the breakfast intake of adolescent girls; to assess the nutrient adequacy of breakfast consumed by the adolescent girls; to examine the association, if any, between adequacy of breakfast, body mass index (BMI) for age Z scores (BAZ) and haemoglobin levels.
Methods
Study design and sampling
The study design was a cross sectional survey. Seven slums from Pune Municipal Corporation (urban) and two from Pimpri Chinchwad Municipal Corporation (peri-urban) were chosen as the study locale. About 1200 households are distributed in each of these slums. Through the NGOs working in the slums a list of households with adolescent girls aged 16–18 years was obtained from the health workers in the selected slums. All the households with adolescent girls were contacted through individual home visits. Over 600 adolescent girls were contacted to participate in the study. Those girls who consented to participate and who were from free from chronic illness six months prior to or during the study period were excluded. Thus a sample of 565 (with response rate of 94%) adolescent girls was randomly recruited from urban and peri-urban slums of Pune city.
Socio-demographic and dietary data
A semi-structured questionnaire was used to collect information on socio-demographic data. Three, 24-hour diet recall was used to elicit information about breakfast and overall dietary intake per day. Of the three-days, one was a holiday and the other two were working days. Both type and quantity of food consumed were recorded. The recall was done through face to face interview. Standard measuring cups and spoons were used to record the quantity of foods consumed. Models of Indian bread (Chapattis of different sizes) and images of foods standardised were used to assess the portion size of foods consumed. The portions were back calculated to measures in grams using the nutritive value of Indian foods (ICMR, 2010). Both macro and micronutrient intake including iron, vitamin C and beta-carotene was calculated to assess the quantity and quality of diet consumed. The average intake of three days was used to calculate nutrient intake per day.
Anthropometric assessment
Height-for-age (HAZ) reflects the cumulative effects of nutritional exposure whereas BMI-for-age (BAZ) reflects acute changes in nutritional status. Measurements of height and weight were recorded in duplicates using standard equipment (portable Seca stadiometer, Model No 213; Omron digital, portable weighing scales). Measurements were recorded nearest to 0.1 cm. Technical error of measurement (TEM) that includes intra and inter observer variability was maintained within standard limits (0.1). Anthropometric data was analysed by using WHO Anthro software to determine the prevalence of underweight (weight-for-age), and stunting (height-for-age) based on reference data from the National Center for Health Statistics (NCHS)/World Health Organization (WHO) (De Onis et al., 2004; NHANES, 1999–2006). According to Z score categorisation, < −2 standard deviations (SDs) is used to classify undernourished children < −3 SDs to define severe undernutrition. Positive SDs greater than two and three indicate overnutrition.
Haematological data
A 5 ml blood sample was collected for haematological assessment. The results of haemoglobin estimation alone are described in this study. The samples were stored in ice packs until transported to the laboratory. Haemoglobin was estimated by the cyanmethemoglobin method in the haematology unit in King Edward Memorial Hospital, Pune, in Maharashtra, India. Haemoglobin concentrations were categorised as per the WHO criteria (WHO, 2011). As per the categorisation, mild anaemia is defined as haemoglobin levels from 11.00 to 11.9 g/dl, moderate anaemia from 8.00 to 10.9 g/dl and severe anaemia as <8 g/dl. This work was approved by the Inter System Biomedica Ethics Committee (ISBEC), Mumbai. The study was explained to the participants in local language and informed consent from parents and assent from adolescent girls were obtained before initiation of the project. Of the 565 recruited, 284 (50%) participants consented for haematological assessment.
Data analysis
At population level, breakfast intake is studied to assess adequacy of nutrient intake. Adequacy of breakfast has been categorised as follows: (a) breakfast skippers meeting 0% Recommended Dietary Allowance (RDA) for calories, (b) inadequate breakfast consumers I: <15% RDA, (c) inadequate breakfast consumers II: 15% to ≤25%, and (d) adequate breakfast consumers meeting >25% of RDA for energy (Sivaramakrishnan and Kamath, 2012). Average nutrient intake per day was calculated from the three days diet recall. Food items consumed for breakfast was used to calculate nutrient intake through breakfast. An average of three days was calculated to assess the nutrient intake per day through breakfast. Distribution of macro- and micronutrient intake per day through the day’s diet was calculated among breakfast takers and skippers. Distribution of undernutrition as per HAZ and BAZ scores among adolescent girls was studied. One-step linear regression was used to study the association between the dependent variable HAZ score and independent variables that included macronutrients and selected micronutrients. Mann Whitney U test was performed to study the difference in micronutrient intake among anaemic and non-anaemic participants.
Results
The age of participants ranged from a minimum of 16 years to maximum 18 years, with the mean age being 16.89±1.23 years. As the samples were recruited from urban slums who represent migrant population, more than three quarters of the participants (78.4%) were from the upper-lower socio-economic strata, according to the Kuppuswamy scale (Gururaj, 2014). The mean height of the participants was 151.8±5.72 cm and the mean weight of the participants was 44.9±6.33 kg. The mean BMI of the participants was found to be 19.44 kg/m2, which is well within the normal range (Table 1).
Description of socio-economic status and anthropometric indices of participants.
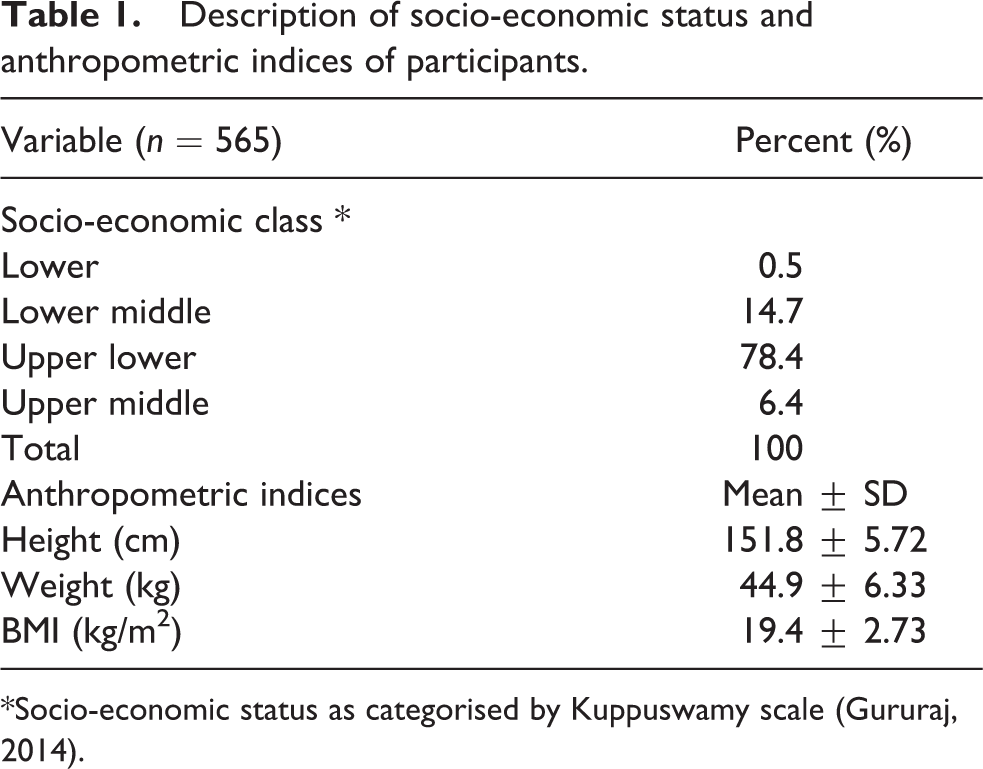
*Socio-economic status as categorised by Kuppuswamy scale (Gururaj, 2014).
Breakfast intake and types of breakfast
About 28% of the adolescent girls did not consume any breakfast. Foods taken by adolescent girls who consumed breakfast was consolidated and the following types of breakfasts emerged: (i) only tea; (ii) tea with biscuits; (iii) tea with khari (a puffed pastry without any filling, made of refined flour and vegetable fat); (iv) tea with chapatti (Indian bread); (v) chapatti with vegetable; (vi) upma/poha/sheera/kichidi (cereal preparations with semolina, rice flakes, rice and pulses, respectively). School supplementary meals provide a mixed preparation of cereal, pulse, vegetable and oil. This is provided for children up to eighth grade through the Government of India, Mid-Day Meal programme (MDM, GOI). This is a food-based approach to provide food (one meal) and nutrition security (one-third of nutrient requirement for the day) on a daily basis, to prevent undernutrition among children (MHRD, 2016). The school started at 7.30 am and the meal was served between 10.30 and 11 am. Therefore this meal was categorised as breakfast in this study. In this study, as per definition, foods consumed in the early part of the day that comprised the first meal were considered as breakfast. Also, for the purpose of quantitative estimation of nutrients taken, all foods consumed during this time were included and hence this categorisation was followed. The types of breakfast consumed by the adolescents, its distribution and macronutrient content are given in Table 2.
Distribution of participants according to the types of breakfast consumed and maximum and minimum macronutrient content of different types of breakfast.
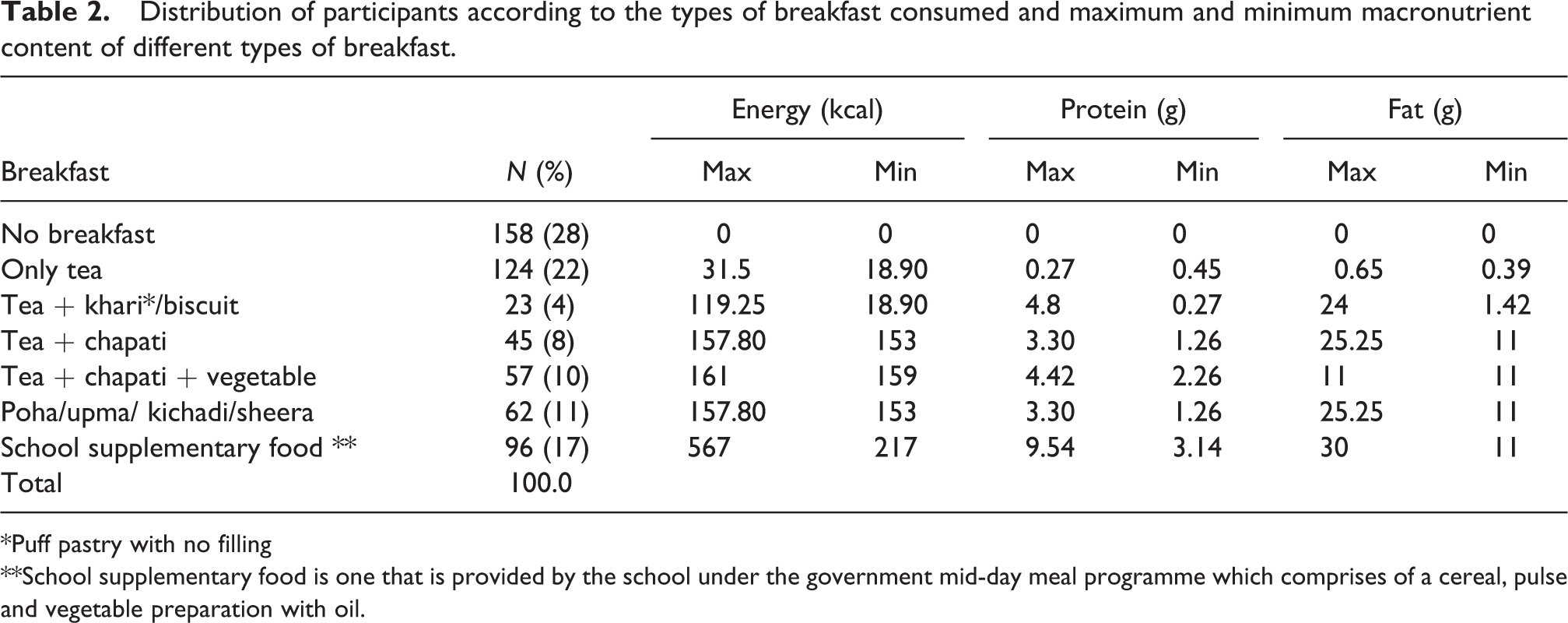
*Puff pastry with no filling
**School supplementary food is one that is provided by the school under the government mid-day meal programme which comprises of a cereal, pulse and vegetable preparation with oil.
More than a quarter of the participants (28%) skipped breakfast while another 22% consumed only tea. Thus, one half of the participants started their day without consuming any solid food. Maximum nutrient intake was observed among those who consumed (17%) the school supplementary food. The older children who participated included those who were detained or had discontinued due to migration and continued their education further by repeating the grade. These children were still eligible for MDM. Also, there is a percent of children who come for food although not eligible and they are usually not denied.
Adequacy of breakfast
Indian Council of Medical Research (ICMR) recommends the total nutrient requirement per day in the Recommended Dietary Allowance for Indians (ICMR, 2010). Adequate breakfast should essentially supply one fourth of the days nutrients required, i.e. 610 kcal (Sivaramakrishnan and Kamath, 2012). The distribution of breakfast intake among the girls as indicated by percent RDA for calories is shown in Table 3.
Distribution of adolescents according to percent RDA met through breakfast.
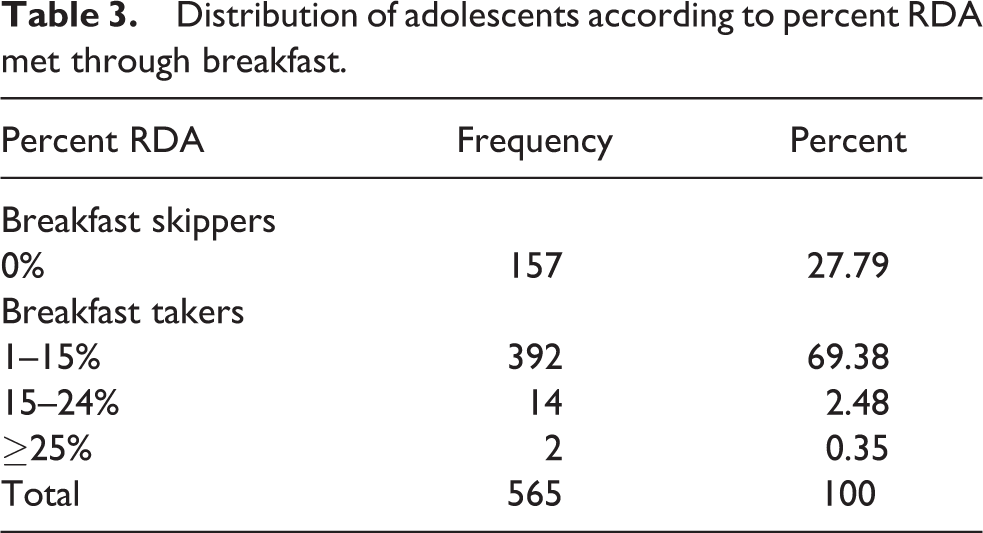
In the present study, breakfast that met 25% of RDA for calories was defined as adequate breakfast. As per the definition almost all the adolescent girls (99.6%) consumed inadequate breakfast. Among the 408 adolescent girls who consumed breakfast, about 69% met up to 15% RDA and about 0.35% met 15–24% RDA. Nutrient adequacy of breakfast when calculated showed 62% energy deficit, 71% protein and 11% fat deficit in foods consumed by adolescent girls. Micronutrients of interest especially iron and vitamin C were grossly deficient, i.e. by 97.5% and 90.1% respectively.
Macro and micronutrient intake through breakfast
For the purpose of analysis and comparison, breakfast taken by participants was categorised into two groups. Those who took tea, or tea with biscuits or khari were categorised into group I breakfast and the others who took a traditional breakfast, i.e. tea with chapatti, tea with chapatti and vegetable and who took a cereal preparation (sheera, poha or upma or school supplementary meal) were categorised into group II. Among the participants more than 50% consumed breakfast of the first category.
The mean macro- and micronutrient intake of breakfast takers who consumed a traditional cereal preparation for breakfast with a beverage was significantly higher than the first category. The mean energy intake was 235.08±101 kcal among group II and one fifth of these by group I. Energy intake of group I breakfast category was either from the sugar in the beverage, refined flour and or fat from bakery products. On the contrary, the cereal component from group II breakfast category included complex carbohydrates along with fat thereby contributing to the higher energy intake. Protein as well as fat intake of group II was three times higher than group I. However, the important observation in this study was that, even among those adolescents who consumed any breakfast the average intake did not meet one fourth of the RDA.
Breakfast intake, overall nutrient intake per day and anaemia
Results of haemoglobin estimation indicated 56% prevalence of any anaemia among the adolescent girls. As per WHO categorisation of severity, 11% were mild, 43% were moderate and 2% were severely anaemic. Dietary factors are implicated as the contributors to high prevalence of anaemia in India. The overall macronutrient and micronutrient intake in a day, between breakfast takers and breakfast skippers is shown in Table 4.
Mean overall intake macro- and micronutrients per day as compared between breakfast takers and breakfast skippers.
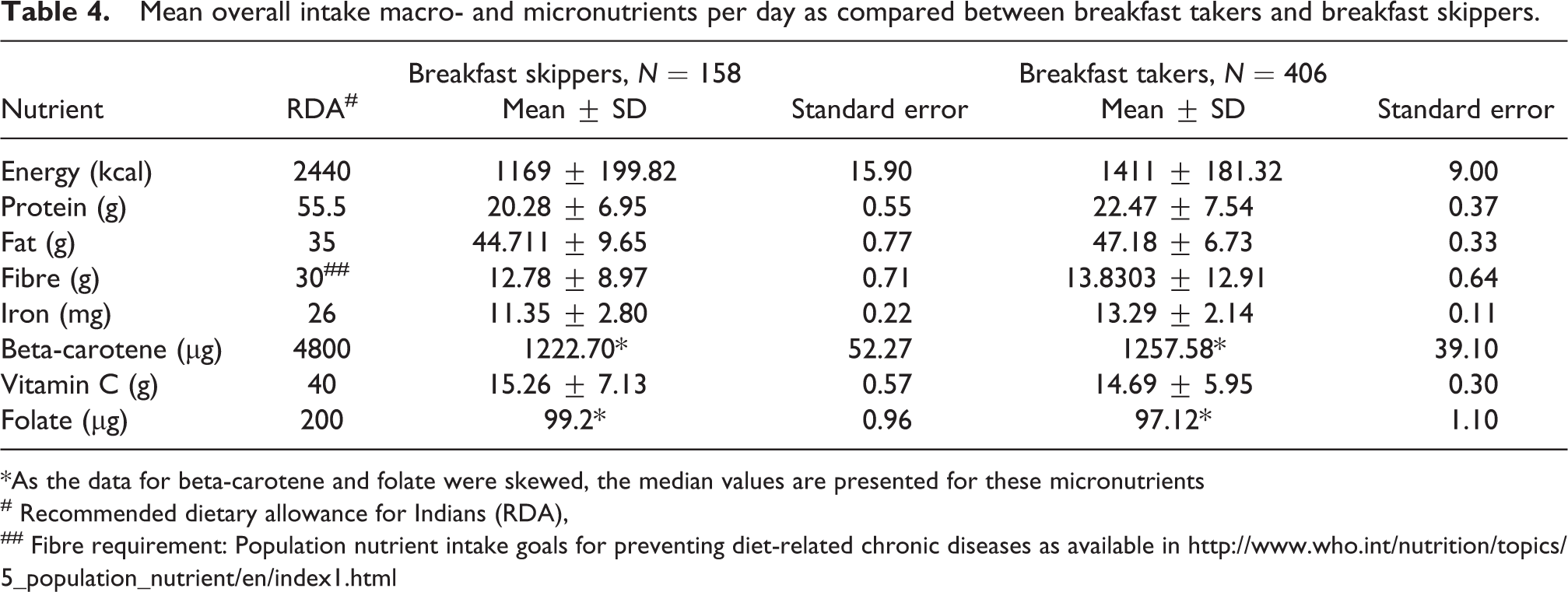
*As the data for beta-carotene and folate were skewed, the median values are presented for these micronutrients
# Recommended dietary allowance for Indians (RDA),
## Fibre requirement: Population nutrient intake goals for preventing diet-related chronic diseases as available in http://www.who.int/nutrition/topics/5_population_nutrient/en/index1.html
Comparison of macro- and micronutrient intake between anaemic and non-anaemic adolescents is shown in Tables 5 and 6, respectively.
Comparison of means of macronutrient intake though the entire days food intake between anaemic and non-anaemic adolescents.
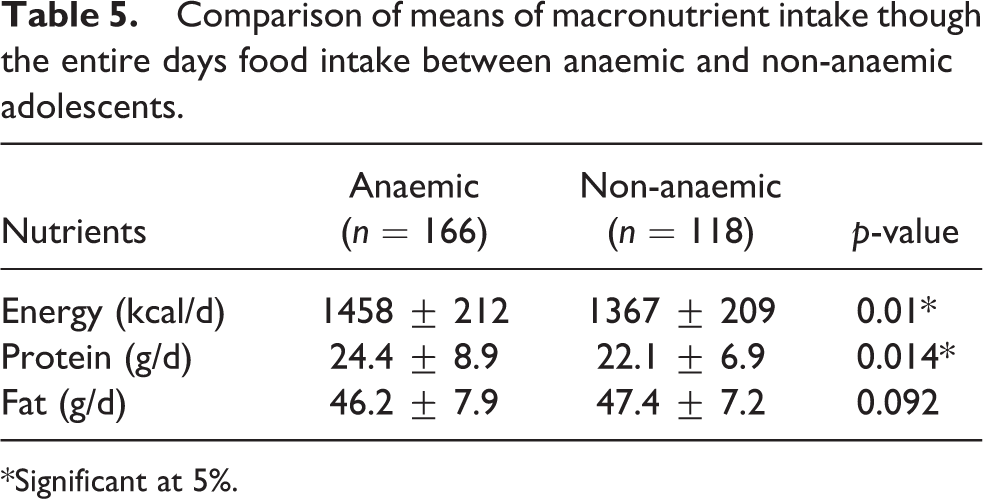
*Significant at 5%.
Comparison of means of micronutrient intake through the entire day’s food intake between anaemic and non-anaemic adolescents.
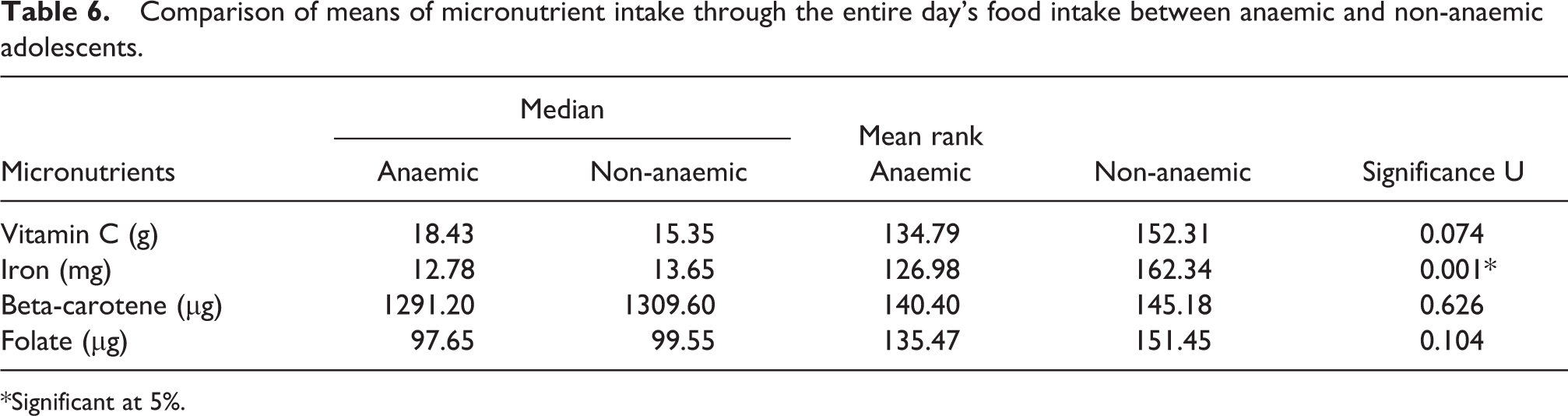
*Significant at 5%.
Among the nutrients taken, energy protein and iron intake were significantly lesser (p = 0.001, p = 0.01 and p = 0.001) among the adolescent girls who were anaemic. In this study, dietary deficits arising in breakfast was not compensated in the subsequent meals. Nutrient deficits in a day may therefore be corrected by improving the quality and quantity of the first meal consumed.
Breakfast, overall nutrient intake per day and BAZ
According to HAZ, which reflects stunting (a long-term indicator of nutritional status), >50% were undernourished. Of these, 43.5% were mild, 28% moderate and 5% severely stunted. The WHO report on regional consultation (WHO, 1998) showed a prevalence of 45% stunting among adolescents which is comparable to the present study findings.
The Z scores and classification of malnutrition of adolescent girls in this study are presented in Table 7.
Distribution of undernutrition as per HAZ and BAZ scores among adolescent girls.
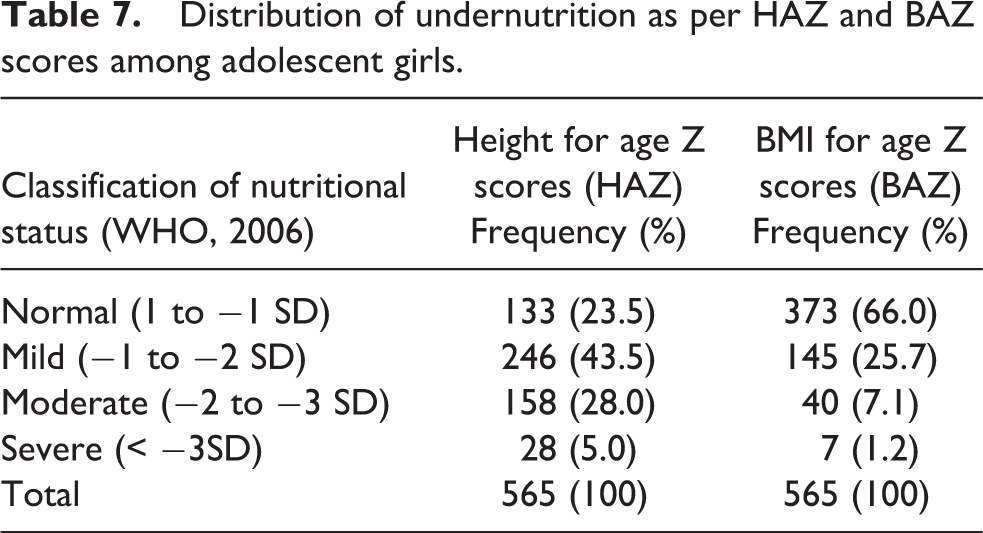
BAZ is a measure of relative weight adjusted for age and sex. According to BAZ, 34% were undernourished. Of these, 25% were mild, 7% moderate and 1% severely undernourished.
Linear regression of HAZ scores and macro and micronutrient intake is provided in Table 8. Results showed a positive association between the days’ overall energy and fat intake and HAZ scores.
Linear logistic regression of HAZ and macro and micronutrient intake through breakfast among adolescent girls.
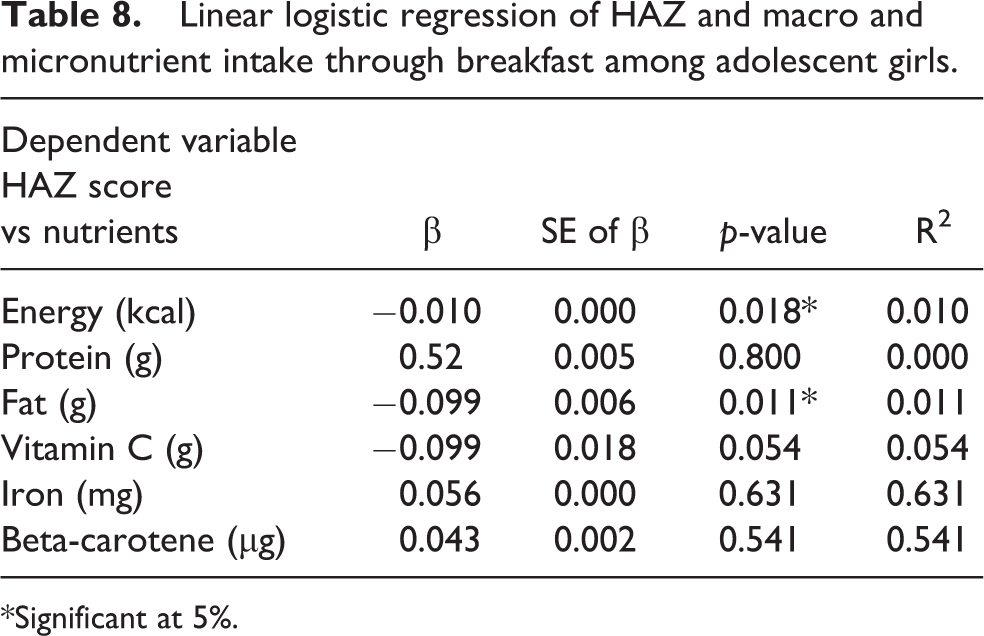
*Significant at 5%.
Discussion
The present study aimed to assess the breakfast intake of adolescent girls, its adequacy and is effect on nutritional indicators. The intake of breakfast among adolescent girls living in resource poor settings was comparatively lesser than other sections of the population as observed from other studies. The percent of adolescent girls who skipped breakfast was lesser compared to another study carried out in Andhra Pradesh, wherein more than 50% of the adolescents skipped breakfast a few times per week (Chitra and Reddy, 2007). However, observations among adolescents from higher and middle-income families in Mumbai showed that a lesser percent of adolescents (16%) skipped breakfast (Sivaramakrishnan and Kamath, 2012). Literature evidence also shows variations in breakfast consumption patterns in developed and developing nations. In the United States, analysis of National Health and Nutrition Examination Survey (NHANES) Survey (1999–2006) revealed that 35% of participants skipped breakfast (Deshmukh-Taskar et al., 2010). However in Ghana, frequent breakfast consumption was observed among adolescents from middle and higher income groups (Doku, 2013).
In this study, assessment of adequacy of breakfast indicated that nearly 69% met <15% of RDA. Work done by Sivaramakrishnan and Kamath (2012) in Mumbai, India, also showed similar results, where about 64% consumed ≤15 % RDA. Findings as these highlight the poor quality and quantity of breakfast, as otherwise it may mislead that breakfast takers have better nutrient intakes. More studies need to focus on nutritional adequacy of breakfast to plan appropriate interventions.
The present study revealed negligible intake of all micronutrients by the participants. In developed countries breakfast comprises of cereal, which may be fortified with micronutrients, or bread with butter, eggs, milk and or fruit juice (Song et al., 2006). The protein quality and micronutrient intake of such breakfasts is higher. In India, fruits are classified as income elastic foods and therefore not affordable by the lower income groups. Even among middle income groups in Hyderabad in India, fruit consumption was reported only among 2% of the school children (Gajre et al., 2008). With only cereals and very little milk in morning tea and with minimum or no inclusion of fruits and vegetables, protein and micronutrient intake is marginal in the urban slums in developing countries (Arora et al., 2012).
Epidemiologic transition has contributed to major lifestyle changes and dietary habits, both in developing and developed countries (Popkin, 2001). In developed countries, there is a trend toward increased consumption of high caloric fast foods and breakfast cereals. Literature evidence suggest that in developed countries adolescents who took ready to eat fortified breakfast cereals had better nutrient intake profile and favourable adiposity index compared to other breakfast consumers (WHO, 1998). Whereas in developing countries convenience foods like bakery products, which are high in calories and low in micronutrients, have replaced the traditional breakfast.
In a Belgian study, the intake of macro and micronutrients were proportionally higher among adolescents who consumed better quality breakfast (Matthys et al., 2007). In Denmark, adolescents who did not skip meals frequently included fruits with breakfast. Also irregular breakfast intake was associated with low fruit consumption (Pedersen et al., 2012). In resource-poor settings other than direct dietary factors, lack of time for preparation of breakfast (as the mothers leave for work early in the day) and availability of convenience food, which are nutritionally poor, affect both quantity and quality of breakfast. Poor intake of nutrients has been identified as a major risk factor for poor nutritional indicators. Among dietary risk factors of anaemia, low dietary iron intake, lower intake of foods that improve bioavailability, such as vitamin C and vitamin A, and the presence of inhibitors in the diet have been identified (Hallberg, 1992; Semba and Bloem, 2002; Stoltzfus et al., 1998). In this study, there was no direct association between breakfast adequacy and anaemia status. However, there was significant association between the days’ nutrient intake and haemoglobin status. According to Nair and Iyengar (2009), every 1000 kcal of an average Indian meal would contribute about 8-10mg of iron. Therefore, ensuring adolescents consume the first meal would enhance the nutrient intake through the day.
BAZ scores of adolescents indicated 34% undernutrition and haematological indicators showed 56% prevalence of anaemia. This underscores the poor nutritional indicators among adolescent girls. As the population was homogenous (i.e. 99% consuming inadequate breakfast) the association between nutritional status and breakfast intake was not significant. However, associations were significant when studied with the overall nutrient intake of the day. Hence, compensating the dietary deficits through an additional meal, i.e. breakfast, would ensure better nutrient intake and contribute to improvement of overall nutritional status.
In India the definition of poverty is based on the total calories consumed in a day, the expenditure for education and health. According to the Federation of India Chambers of Commerce and Industry (FICCI, 2015) survey, the poorest 10% of the Indian population consumed 1679 kcal, whereas intake of the rich is nearly 2518 kcal. The difference accounts to nearly 50%. With reference to expenditure, on an average the Indian household spends 30% of its income on food, the more developed the country, the less the expenditure on food (NSSO, 2014). In such a setting food security need to be viewed from the perspective of ‘food availability’ rather than ‘food preference’. In this study qualitative observation among the sample revealed ‘lack of time’ as they had to leave early for work or school. Work done by Kotecha et al. (2013) provides similar findings, where lack of time and body image have been identified as barriers to improving dietary practices among adolescents. The adolescent girls too, did not take the initiative to prepare breakfast for themselves or their families. With a deficit of one fourth of the RDA observed among this population and the inability to compensate either due to lack of time, financial restriction or poor available choices, it is unlikely to meet the nutrient requirements for the day.
Recommendations
Under the Ministry of Women and Child Development, the programmes for adolescent health focus on rendering services such as immunisation, reproductive health education, anaemia control through iron supplementation and nutrition and health education. The present study underscores the need for food-based approach to address the nutrient gap that arises due to missing a meal, in order to improve the nutritional status of adolescent girls. Stand-alone approaches such as supplementation of micronutrients may not address the energy and protein gap that aggravate micronutrient deficiencies.
The nutrient intake of those adolescents who participated in the school supplementary programme was higher compared to those who took breakfast at home. As this programme caters to children only up to eighth grade (primary and upper primary), older adolescents in and above ninth grade do not benefit from food-based interventions. Hence, there is a need to extend the programme for adolescents in higher grades. This would prepare them nutritionally for the reproductive phase. Creating awareness among the adolescents about these interventions and encouraging participation in the existing interventions would ensure better utilisation of services and improved nutritional benefits.
To meet the micronutrient needs of non-school going adolescents, fortification of bakery products (as this formed a major part of the breakfast foods) would ensure better intake, as taking a balanced meal for breakfast is economically and practically not feasible in this setting. Data on dietary intake of women and adolescents need to be studied regularly to plan intervention for women. Interventions for income generation are vital to improve the resources to purchase and prepare healthy food. Empowering adolescent girls with nutrition education and creating awareness on the importance of preparing food at home would encourage them to make healthy choices of food.
Footnotes
Acknowledgements
The authors wish to thank all the participants of the study and Dr Swapnil Gadhave for his support in statistical analysis
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.