
Abstract
Background:
The use of nutrigenomics and lifestyle genomics in clinical practice has the potential to optimize weight-related outcomes for patients.
Aim:
A scoping review was conducted to summarize and evaluate the current body of knowledge related to the effectiveness of providing DNA-based lifestyle advice on weight-related outcomes, with the aim of providing direction for future research.
Method:
Primary studies were included if they were written in English, evaluated weight-related and/or body mass index and/or body composition outcomes, and provided participants with an actionable genetic-based lifestyle intervention; interventions that only provided information on genetic risk for diseases/conditions were excluded. Data was extracted from each article meeting inclusion criteria (N=3) and the studies were critically appraised for methodological limitations.
Results:
Research in this area is promising, but limited. Specific limitations relate to study designs, the nature of the recommendations provided to participants, small (underpowered) sample sizes, the use of self-reported weight/BMI data and lack of consideration of important confounding factors.
Conclusions:
Therefore, the effectiveness of nutrigenomics and lifestyle genomics interventions for weight management in clinical practice cannot yet be conclusively determined. Recommendations for future research are detailed in the present manuscript.
Background
Consumers have expressed substantial interest in nutrigenomics (Nielsen et al., 2014; Vallée Marcotte et al., 2019). As a result, many companies are offering personalized DNA-based lifestyle advice, most of which provide specific recommendations to optimize weight management practices (23andMe, 2019; myDNA, 2019; DNAfit, 2019 Nutrigenomix Inc., 2019; Pathway Genomics, 2019). With increasing epidemiological and interventional research demonstrating relationships between genetics, nutrition and physical activity, and weight-related outcomes (Casas-Agustench et al., 2014; Corella et al., 2009; Garaulet et al., 2011; Phillips et al., 2012; Zhang et al., 2012), personalized lifestyle recommendations based on genetics are becoming established. For example, evidence from a two-year randomized controlled trial (RCT) reported that variation in the fat mass and obesity associated (FTO) gene at rs9939609 can predict weight loss response to a lower versus higher protein diet (Zhang et al., 2012).
Weight loss continues to be a priority for the general public (Sui et al., 2019). As such, nutrigenomics and lifestyle genomics testing for weight management are attractive tools, as they promote more personalized strategies for individuals to optimize their weight loss response to particular dietary plans. Nutrigenomics refers to gene–diet–health outcome interactions while lifestyle genomics is more broad and refers to interactions between genetics, various lifestyle factors (e.g. nutrition, physical activity, sleep, smoking, etc.) and health outcomes (Gibney and Walsh, 2013; Horne et al., 2018). While the scientific evidence for personalized weight management strategies continues to grow, long-term behavior change and weight management remain a challenge and weight loss outcomes in clinical practice often do not satisfy the wants or needs of patients (Field et al., 2013; Rogerson et al., 2016; Soleymani et al., 2016). Weight loss is often followed by weight regain above and beyond baseline weight; research has demonstrated that such weight yo-yoing (the constant and recurring decrease and increase in weight over time) can be more harmful to health than weight maintenance (Rhee, 2017).
Current evidence demonstrates that individual responses to nutrition plans for weight management differ based on genetic variation (Casas-Agustench et al., 2014; Corella et al., 2009; Garaulet et al., 2011; Phillips et al., 2012; Zhang et al., 2012). Some research has also shown that individuals are more motivated to follow nutrition advice when it is based on their genetics (Horne et al., 2018; Kaufman et al., 2012; Nielsen and El-Sohemy, 2014). Because of this, it is possible that the provision of nutrigenomics and lifestyle genomics interventions could be used as tools to support weight management. However, multiple factors beyond genetics, nutrition and physical activity contribute to the development and management of obesity, including the social determinants of health, built environment, food access and availability, medications, certain diseases/conditions such as polycystic ovarian syndrome, sleep, stress and others (Finkelstein et al., 2005; Geiker et al., 2018; Gilliland et al., 2012; Maina et al., 2004; Moore et al., 2010; Naderpoor et al., 2015; Seabrook and Avison, 2010). Thus, managing overweight and obesity is multi-factorial. Nutrigenomics and lifestyle genomics are not the only considerations of weight management, but they remain important components of the overall picture, alongside other factors.
The objectives of the present review include: summarizing the literature, critically appraising the literature and determining directions for future research related to the pragmatic application of actionable nutrigenomics and lifestyle genomics interventions for weight management. Despite the robust and growing research foundation on the science of nutrigenomics, lifestyle genomics and differing weight loss responses to the same nutrition plans, we hypothesize that minimal research exists assessing the pragmatic impact (effectiveness) of genetic-based lifestyle interventions for weight management.
Methods
A scoping review was conducted in July–August 2019 with guidance from Arksey and O’Malley’s (2005) methodological framework. This process included identifying the research question, finding relevant studies, selecting studies meeting inclusion criteria, charting relevant data and, finally, collating, summarizing and reporting the results (Arksey and O’Malley, 2005). Each study was also critically appraised for methodological concerns and considerations. The overall purpose of this review was to identify, summarize and critically appraise the existing literature on the effectiveness of using actionable genetic-based lifestyle interventions in clinical practice to enhance weight loss and/or improve body composition. Furthermore, we aimed to use these results to provide direction for future research. The first author (JH) conducted title and abstract screening, followed by full-text screening to find studies meeting inclusion criteria. English articles assessing the impact of providing genetic-based lifestyle advice on weight-related, body mass index (BMI) and/or body composition outcomes were included. Articles assessing the impact of providing information on genetic risk (i.e. without actionable lifestyle advice) were excluded. To capture only studies assessing the pragmatic use of genetic-based lifestyle interventions, articles were also excluded if they aimed to identify or replicate gene–nutrient–health outcome/weight interactions. PubMed and Google Scholar were searched for relevant studies using different combinations of the following search terms: nutrigenomics, nutrigenetics, nutritional genomics, lifestyle genomics, weight, BMI, body composition, intervention, nutrition, lifestyle, and/or physical activity. Reference lists of included articles were reviewed for relevant articles.
The following data from each study was charted: author(s), year of publication, intervention type and comparator, duration of intervention, study population, methods, relevant outcome measures, single nucleotide polymorphisms (SNPs) included in genetic reports, genetic testing company (where applicable) and relevant results related to the effectiveness of genetic-based weight management interventions. Each article was critically appraised for key limitations of the employed scientific methods, focusing on the data extracted and charted, to determine gaps in the existing literature and provide direction for future research.
Results
A summary of studies meeting the inclusion criteria (N=3) is presented in Table 1. This review found that overall research in this area is minimal, with only three studies assessing the practical impact of providing actionable genetic-based lifestyle information on weight, BMI and/or body composition. While two RCTs have been conducted, one was a feasibility study (Frankwich et al., 2015), which has not yet been followed up with a larger, adequately powered trial, and in the other (Celis-Morales et al., 2017), change in a weight-related outcome was not the predetermined primary outcome of interest (Newcastle University, 2016).
Summary of studies meeting inclusion criteria.
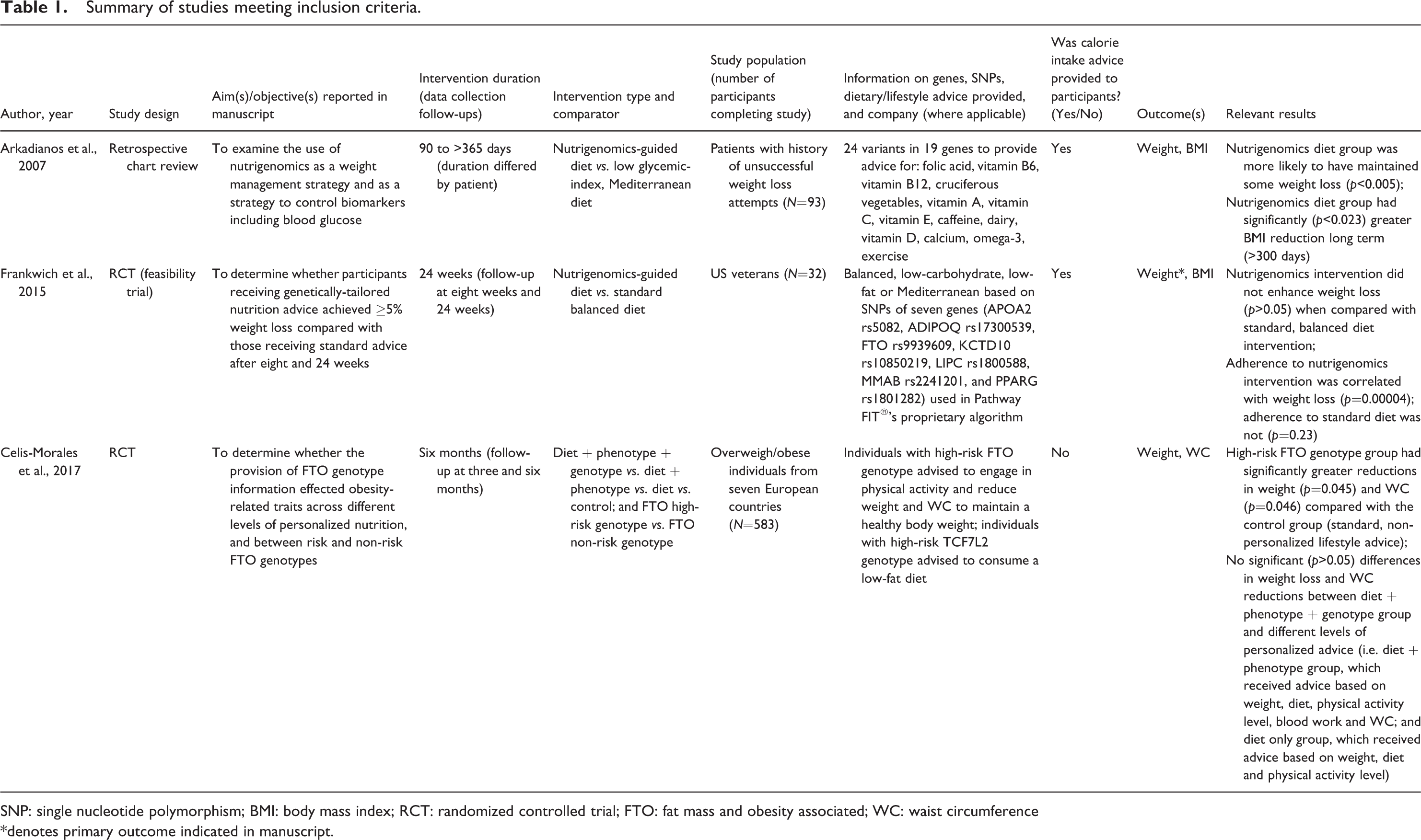
SNP: single nucleotide polymorphism; BMI: body mass index; RCT: randomized controlled trial; FTO: fat mass and obesity associated; WC: waist circumference
*denotes primary outcome indicated in manuscript.
The retrospective chart review by Arkadianos et al. (2007) was an informative first step for this body of knowledge. This study compared patient charts from individuals who attended a weight management clinic and received nutrition advice based on genetics, or based on standard/population-based information. Participants in each group were matched for age, sex, starting BMI and number of clinic visits. The authors concluded that individuals receiving the nutrigenomics intervention were more likely to maintain weight loss and experienced significantly greater BMI reductions over the long term. However, several methodological limitations should be noted. First, due to the nature of the study methods (retrospective chart review), cause and effect relationships cannot be drawn. Furthermore, the nutrition recommendations provided to participants were not specific to weight management; rather, they provided recommendations for general health and wellbeing. For example, SNPs in tumor necrosis factor alpha, interleukin-6 and nitric oxide synthase 3 were tested to provide nutrient recommendations such as ‘Add supplement Omega 3 (700–1400 mg). Make sure weekly diet contains portions of oily fish’ (Arkadianos et al., 2007). Additionally, intervention durations were not standardized and therefore varied substantially in both total length and the amount of follow-up. Of note, income was not considered as a confounding factor; given that patients either purchased or did not purchase a nutrigenomics test in this study, it is likely that income levels would differ significantly between groups. This is an important confounding factor to consider given that income is a well-established social determinant of health (Government of Canada, 2019). The authors noted several other limitations including the lack of placebo, modest sample size and a sample consisting of Caucasian individuals from Greece with a history of difficulty in losing weight, thus limiting generalizability (Arkadianos et al., 2007).
Frankwich and colleagues conducted the first RCT in this area (Frankwich et al., 2015). This was a feasibility RCT. Feasibility trials are distinguished by their focus on assessing the viability or capability of conducting a larger trial, rather than assessing effectiveness or efficacy of an intervention with adequate power (Eldridge et al., 2016). The percentage of participants achieving 5% weight loss was the primary outcome, and this study found that there was no significant difference between groups in the percentage of participants achieving 5% weight loss (Frankwich et al., 2015). However, typically, estimates of participant outcomes such as weight loss would be reported as estimates with 95% confidence intervals (without p-values) given that feasibility trials are not adequately powered to assess the effectiveness of an intervention (Eldridge et al., 2016). In fact, the authors noted limitations related to the small sample size (N=32), and determined that a sufficiently powered trial would require 336 participants per group using a sample size calculation with 80% power and an alpha-level of 0.05 (Frankwich et al., 2015).
Finally, Celis-Morales et al. conducted the second RCT on this topic (Celis-Morales et al., 2017), which was a sub-study within the larger Food4Me RCT (Celis-Morales et al., 2014). This was a significant contribution to the body of knowledge in this area. In total, participants were provided with information and advice related to five gene–lifestyle–health outcome interactions (FTO, physical activity and weight; FADS1 omega-3 and cardiovascular health; TCF7L2 dietary fat and weight; ApoE(e4), saturated fat and cholesterol/cardiovascular health; MTHFR, folate and cardiovascular health). This study compared weight and waist circumference outcomes between a control group and different levels of personalized advice (as outlined in Table 1) and further compared risk and non-risk FTO genotype groups (Celis-Morales et al., 2017). Participants randomized to receive genetic information/advice were informed that ‘A specific variation of this gene is associated with a greater need to maintain a healthy body weight and engage in physical activity. A healthy weight combined with exercise may provide added health benefits for these individuals.’ Carriers of the high-risk FTO allele were further advised to ‘[reduce their] body weight and waist circumference to a healthy normal range because [they] have a genetic variation that can benefit by reducing these 2 obesity-related markers.’ Furthermore, participants randomized to receive genetic-based advice were provided with weight-related information and advice according to a variant within the TCF7L2 gene. They were informed that ‘a specific variation of this gene is associated with improved weight loss when consuming a low-fat diet compared with the effect of other weight-loss diets’ and that ‘reducing dietary fat may enhance weight loss in these individuals’ (Celis-Morales et al., 2017). While the overall RCT was well-designed and is reflective of direct-to-consumer lifestyle genomics testing, there are some considerable limitations to note. First, the height, weight and waist circumference data were all self-reported. While the authors point out that these measures are reliable (Celis-Morales et al., 2015), certainly measured data would still have improved validity and reliability. Perhaps the greatest limitation of this study was that the FTO-related advice provided to participants was borderline actionable. Given the complexity of weight management (Finkelstein et al., 2005; Geiker et al., 2018; Gilliland et al., 2012; Maina et al., 2004; Moore et al., 2010; Naderpoor et al., 2015; Seabrook and Avison, 2010), simply advising individuals to ‘maintain a healthy body weight’ does not provide specific direction on how to achieve this aside from a broad statement advising individuals to exercise. While the TCF7L2-related advice to consume a low-fat diet was actionable, the exact amount of dietary fat was not well-defined and only individuals with the high-risk genotype of TCF7L2 received an actionable recommendation. Therefore, it is not surprising that individuals provided with genetic-based information/advice did not reduce their weight or waist circumference to a greater extent than those receiving other forms of personalized advice (Table 1). However, the genetic group experienced significantly greater reductions in weight and waist circumference compared with the control group, receiving non-personalized standard healthy eating guidelines. The authors do touch on the nature of the intervention as a limitation, stating that the feedback was ‘only a positive reinforcement’ (Celis-Morales et al., 2017). Last, a weight-related outcome was not the predetermined primary outcome of this study and therefore it is possible that the statistical power for this study was inadequate, which is also noted by the authors (Celis-Morales et al., 2017).
Overall, study limitations in the current body of knowledge are related to study design, the nature of the recommendations provided to participants, small (underpowered) sample sizes, the use of self-reported weight/BMI data and lack of consideration of important confounding factors.
Discussion
Overall, weight management remains a challenging area of clinical practice. Research evaluating the effectiveness of genetic-based weight management interventions has been minimal, and results have been variable thus far. While there were some promising findings by Arkadianos et al. (2007), this study had significant methodological flaws. Similarly, while Frankwich et al. (2015) completed the first RCT in this area, this was a feasibility RCT, which has not yet been followed up with a larger, adequately powered clinical trial. Lastly, Celis-Morales (2017) completed a second RCT, but the genetic-based advice provided to participants was minimal, and borderline actionable, and the study may not have been adequately powered statistically.
Based on this review, future research should seek to use evidence-based nutrigenomics interventions, employ an RCT methodology, be adequately powered to detect significant differences for a predetermined weight-related primary outcome, consider important confounding factors, be at least 12 months in duration, and follow established processes for clinical trials such as the SPIRIT and CONSORT guidelines (CONSORT, 2019; SPIRIT, 2019). Furthermore, this future work should aim to provide a genetic-based intervention that is likely to facilitate behavior change; a quality assessment tool for genetic-based interventions has been developed and should be used to help researchers design appropriate interventions (Horne et al., 2018). This work should also use previously developed study quality assessment tools to inform study design in order to reduce any risk of bias (National Heart, Lung, and Blood Institute, 2019).
Critically analyzing the level of evidence available to support the genes tested and subsequent dietary advice provided was beyond the scope of this review. However, it should be noted that the lack of regulation in the genetic testing industry allows for tests to go to market without any accountability to base such tests on robust or any level of scientific evidence (Horne et al., 2020). It is interesting to note that one of the three recently conducted studies provided genetic-based recommendations for following low-carbohydrate nutrition plans for weight loss (Frankwich et al., 2015). Recent research assessing whether or not genetic-based alignment to low-carbohydrate nutrition plans is effective for predicting weight loss outcomes concluded that dietary alignment to the particular genetic profiles included in these studies did not correlate with greater weight loss outcomes (Coletta et al., 2018; Gardner et al., 2018). This simply demonstrates that the few SNPs tested in these studies (which did not include a number of SNPs that have been strongly associated with individualized weight-loss responses such as FTO rs9939609 (Merritt et al., 2018; Zhang et al., 2012)) and genetic-based nutrition advice provided were not based on robust evidence. It should be stressed that the results of these studies do not imply that all nutrigenomics interventions will be ineffective at reducing weight and/or improving body composition. The intricate details of the interventions and SNPs will undoubtedly play a role in the study outcomes. While we work on improving knowledge related to genetically-determined weight loss responses to low-carbohydrate nutrition plans, perhaps interventions providing genetically-tailored weight management advice should be focused on other nutrients such as protein and saturated fat (Casas-Agustench et al., 2014; Corella et al., 2009; Zhang et al., 2012). Furthermore, the development of clinical practice guidelines (CPGs) in nutrigenomics would help to provide guidance to researchers and clinicians for incorporating evidence-based nutrigenomics advice into research and clinical practice (Horne et al., 2020). These CPGs would provide summaries of the level of evidence available to support various specific gene–nutrient–health outcome interactions (e.g. interactions can be classified as: convincing vs. probable vs. possible vs. not demonstrated); indeed, guidelines have been published to evaluate the scientific validity of nutrigenomics interactions and the development of CPGs will be an important step for the field of nutrigenomics (Grimaldi et al., 2017). Ultimately, this would help to enhance the potential for nutrigenomics to improve health outcomes for the general public.
Conclusion
Research in this area has been promising, but limited to date. Specific limitations relate to study designs, the nature of the recommendations provided to participants, small (underpowered) sample sizes, the use of self-reported weight/BMI data and lack of consideration of important confounding factors. As such, future research should seek to address the abovementioned limitations before we can thoroughly answer the important research question: Can the use of nutrigenomics and lifestyle genomics interventions enhance weight-related outcomes in clinical practice? Results from the Nutrigenomics, Overweight/Obesity and Weight Management trial should soon provide further insights into this important research question while addressing gaps in the current body of knowledge (Horne et al., 2019).
Footnotes
Authors' note
Janet Madill is also affiliated with Lawson Health Research Institute, London, ON, Canada.
Author contribution
JH conceptualized the manuscript, conducted the research and wrote the first draft of the manuscript. JM and JG revised the manuscript. All authors reviewed and approved the final draft of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
Ethics approval was not required as this was a review article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author was supported by a CIHR Frederick Banting and Charles Best Doctoral Research Award.