
Abstract
Background:
In the United States in 2014 approximately 1.7 million adults were hospitalized with sepsis, resulting in about 270,000 deaths. Malnutrition in hospitalized patients contributes to increased morbidity, mortality, and costs, especially in the critically ill population.
Aim:
Our goal was to investigate the prevalence of malnutrition in sepsis and the impact it has on clinical and financial outcomes in our most critically ill patients.
Methods:
We implemented nutritional screening by a registered dietitian of 1000 patients admitted with sepsis to specialized care units. We calculated the prevalence of malnutrition, and compared outcomes including mortality, length of stay, and financial costs.
Results:
About 10% of patients with sepsis admitted to our specialized care units were diagnosed with malnutrition on admission after implementation of mandatory assessment.
Conclusions:
Although mortality did not reach statistical significance, these patients had more comorbidities, longer hospital stays, and higher total costs.
Introduction
Sepsis is associated with high morbidity, mortality, and financial costs. In 2014, approximately 1.7 million adults were hospitalized with sepsis, resulting in about 270,000 deaths in the United States (US) with in-hospital mortality as high as 16% (Rhee et al., 2017). Costs are estimated to be over US$20 billion annually (Manaktala and Claypool, 2017). After discharge, 50–70% of sepsis survivors continue to have increased mortality, with many facing critical illness myopathy, neuropathy, and post-intensive care syndrome, which contribute to high morbidity and financial burden (Myers et al., 2016). Malnutrition, common in hospitalized patients with a prevalence between 20% and 50%, is often underdiagnosed (White et al., 2012; Naber et al., 1997). Malnutrition in hospitalized patients further contributes to increased morbidity, mortality, and costs (Correia, 2003; Barker et al., 2011), most significantly in the critically ill population, where it is even more prevalent (Barker et al., 2011; Lew et al., 2017). Early sepsis is characterized by a massive catabolic response, which can overwhelm the metabolism especially during initial critical illness. In patients with pre-existing malnutrition, this leads to higher morbidity and mortality.
During critical illness, initiation of enteral nutrition maintains the structural and functional integrity of the gastrointestinal (GI) tract, something that parenteral nutrition does not match (McClave and Heyland, 2009). Initiating enteral nutrition increases contractility of the GI tract, which moves the luminal bacteria downstream, simulating normal physiologic action during an intense time of catabolic demand (McClave and Heyland, 2009). Enteral nutrition improves blood flow to the gut and this cascade of events propagates the release of anti-inflammatory cells from the GI tract into the systemic circulation (McClave and Heyland, 2009). Without enteral nutrition, there is limited gut mobility, which in turn increases the risk of bacterial overgrowth (McClave and Heyland, 2009). These bacteria can become virulent and increase cytokine release, which promotes cell apoptosis and puts the luminal epithelium at risk of further breakdown (Alverdy et al., 2005). Reduced blood flow to the gut induces ischemia and perfusion injury. Septic patients appear to be particularly vulnerable to these detrimental consequences of malnutrition.
In this study, by implementing mandatory nutritional assessments by registered dieticians (RD) on admission, we investigate the prevalence of malnutrition in sepsis and the impact it has on clinical and financial outcomes in the most critically ill patients. Patients diagnosed with moderate or severe malnutrition are compared to patients without malnutrition, looking at factors such as hospital length of stay, morbidity, mortality, and overall costs.
Methods
Our institution is a 900-plus-bed tertiary care hospital that serves the community of greater Northern Virginia. During the fourth quarter of 2016, we implemented mandatory nutrition assessments by an RD of all patients admitted to the Intermediate Care Unit (IMC) and Medical-Surgical Intensive Care Unit (ICU). The option of a nutrition consultation at the discretion of the physician continued to be available, allowing treatment teams to prioritize patients with the perception of more immediate nutritional needs. For all patients diagnosed with malnutrition, appropriate evidence-based nutritional treatment plans were prescribed. After the initial 3-month implementation of the universally RD-led malnutrition assessment program, we collected data on 1000 consecutive patients admitted to IMC or ICU from February 2017 through November 2017 with the primary or secondary diagnosis of sepsis (diagnosis ICD 10 DRG 871). Patients with the diagnosis of moderate or severe malnutrition were compared with patients without malnutrition (control group). The method used to diagnose malnutrition was based on the American Society for Parenteral and Enteral Nutrition (APSEN) and the Academy of Nutrition and Dietetics (AND) criteria per the 2012 consensus paper. Patients were required to meet at least two out of the six criteria to be diagnosed with malnutrition, which included decreased energy/poor oral intake, significant weight loss, subjective muscle wasting, subjective subcutaneous fat wasting, fluid accumulation, and decreased functional status. This information was collected, depending on the circumstances, from the patient, the patient’s family, and/or via chart review by the RD.
We report demographics, clinical characteristics, and variation in insurance providers in patients with sepsis with moderate or severe malnutrition compared to the patients with sepsis without malnutrition (Table 1). The outcomes of interest are hospital mortality, length of stay (LOS), and total cost that includes direct and indirect costs (Table 2). We also compare patients who were diagnosed with malnutrition after a physician (MD) referral for a malnutrition assessment to the patients screened by an RD and diagnosed with malnutrition with no referral from a physician (table not shown). Analysis of variance tests were conducted for finance and outcome numeric components, the Chi-squared test or Fisher’s exact tests were used for comparison of proportion of a categorical outcome, such as mortality, according to different independent groups. All analysis were two-tailed tests and significance level was determined by p < 0.05. Statistical analysis was performed using SAS 9.4 (SAS institute, Cary, NC).
Characteristics in malnourished vs non-malnourished patients with sepsis.
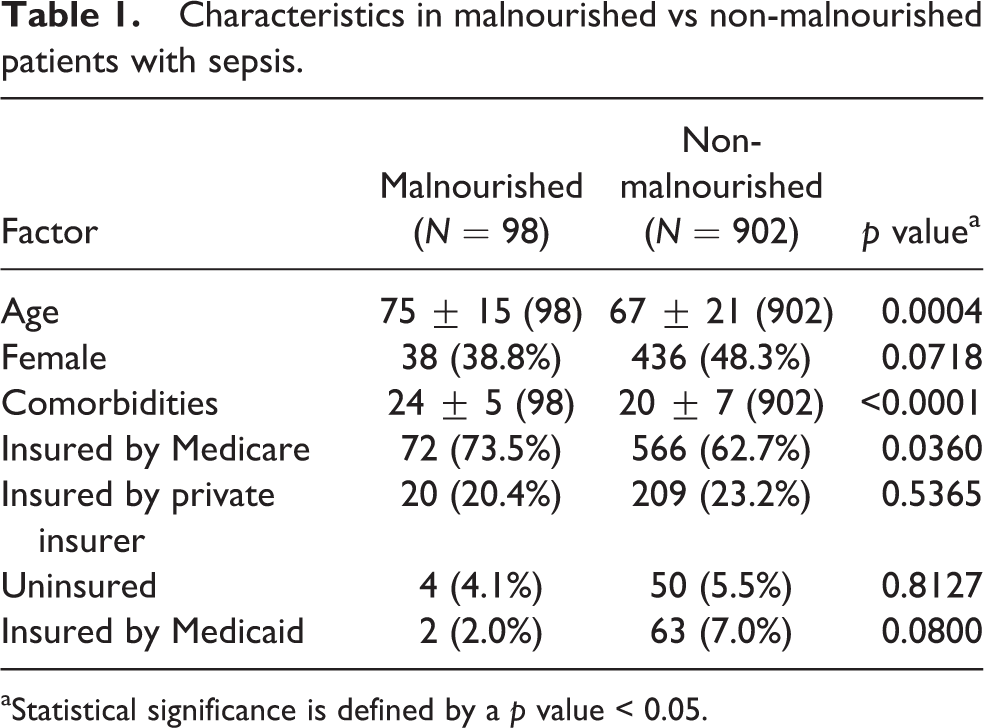
aStatistical significance is defined by a p value < 0.05.
Outcomes in non-malnourished versus malnourished patients with sepsis.
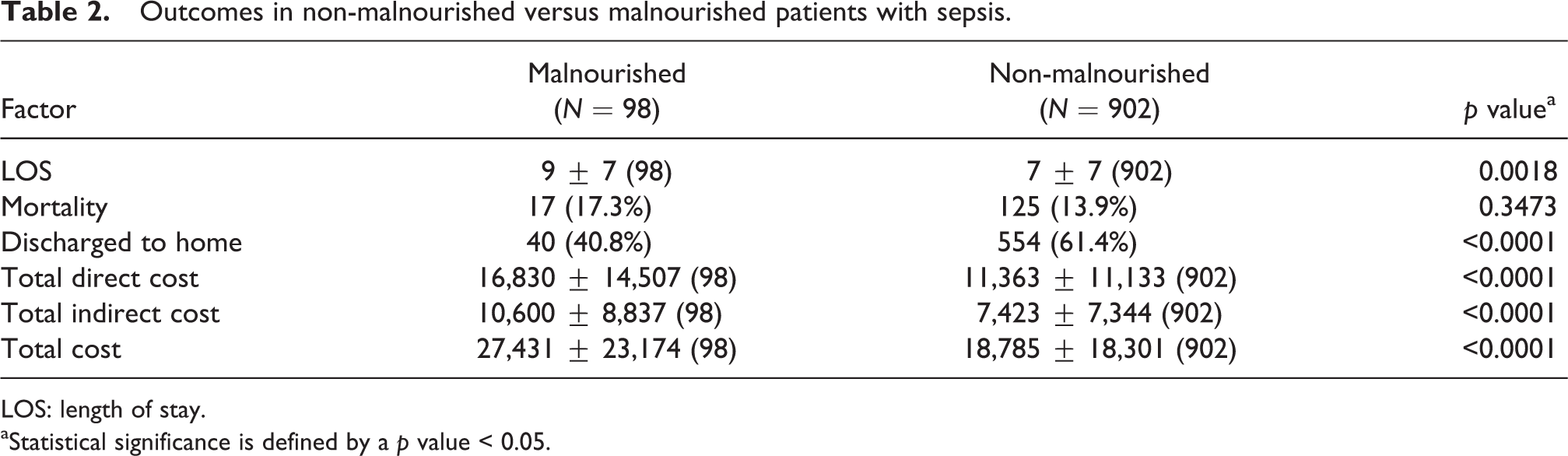
LOS: length of stay.
aStatistical significance is defined by a p value < 0.05.
Results
Of 1000 consecutive patients, 9.8% were diagnosed with malnutrition (Table 1). Of those patients, 54% had severe malnutrition based on ASPEN/AND criteria. Patients with malnutrition were older (75 years +/-15 years vs 67 years +/- 21 years, p < 0.001), and therefore were more likely to be insured by Medicare (73.5% vs 62.7%, Table 1). They also had more comorbidities (24 +/-5 vs 20 +/- 7, p < 0.001). Patients with malnutrition had a longer LOS (average 9 vs 7 days, p = 0.0018) and higher total cost (US$27,431 vs US$18,785, p < 0.0001, Table 2). Mortality in the malnourished cohort was not statistically higher (17.3% vs 13.9%, p = 0.34, Table 2). Patients without malnutrition were more likely to be discharged home compared to those with malnutrition (61.4% vs 40.8%, p < 0.001, Table 2). Only 32.6% of patients diagnosed with either moderate or severe malnutrition were referred to a dietitian by a physician, the remaining 67.3% were all diagnosed based on mandatory RD-led assessments (data not shown).
Discussion
After implementing a universal RD assessment for malnutrition, moderate or severe malnutrition was diagnosed in about 10% of patients admitted with sepsis. Referral by physician accounted for only one-third of the patients diagnosed. The remaining two-thirds of patients with malnutrition were diagnosed based on newly implemented mandatory nutrition consults. Patients with malnutrition were older with more comorbidities, and their hospital LOS was on average 2 days longer. In addition, hospital costs were almost 45% higher and they were more likely to be discharged to a location other than home. All three of these outcomes were significantly worse in patients with malnutrition and there was a trend towards increased mortality in patients diagnosed with sepsis and malnutrition compared to patients with sepsis who were not malnourished on admission.
Malnutrition is associated with increased risk of re-admission to ICU and a higher percentage of discharge to nursing facilities (Lew et al., 2017). Despite severe consequences of malnutrition in the critically ill, it frequently goes undiagnosed and not adequately treated (Alberda et al., 2009; Rice et al., 2005). For example, despite multidisciplinary rounds with an intensivist, bedside nurse, and nutritionist, on average only 50% of enterally fed patients meet a successful intake goal after 5 days of enteral feeding while in the ICU (Binnekade et al., 2005). Implementation of mandatory nutritional assessments of all patients in our ICU and IMC sought to identify and treat patients with pre-existing malnutrition early in their hospital course to theoretically prevent further nutritional decline during times of significant catabolic stress. New strategies aiming for early recognition and aggressive treatment of malnutrition with universal RD-led assessments and standardized administration volume-based feeds are feasible in critically ill patients and can lead to more effective treatment of pre-existing malnutrition and prevent further nutritional decline.
The exact mechanism by which malnutrition negatively impacts outcomes in critically ill patients is not completely understood. It is likely multifactorial including altered immunity, inflammatory pathways, enteropathy, and microbiomes, among others (Bourke et al., 2016). Patient factors that affect risk of malnutrition include age, preexisting co-morbidities, psychiatric diseases, functional status, sensory loss, and drug therapy (Barker et al., 2011). Sepsis may further worsen nutritional status by severe catabolic response during acute illness, compounded by an exacerbated pro-inflammatory state, decreased gut motility, malabsorption, and prolonged immobilization (Casaer and Van den Berghe, 2014). Known consequences of malnutrition include loss of lean body mass, the inability to mount an effective immune response, increased secondary infection, pressure ulcer risks, impairment in thermoregulation, and impairment in renal function (Barker et al., 2011). Malnutrition is associated with poor immune system function, which poses a greater risk for infectious complications (Rubinson et al., 2004). A study of 138 patients at Johns Hopkins University proved the risk of bloodstream infection was highest in patients receiving <25% of American College of Chest Physicians recommended calories compared with all other patients (Rubinson et al., 2004).
Our study has several limitations. This is a single-center study, and diagnosis of sepsis was based on administrative coding. Our newly implemented nutritional assessment did not include mild malnutrition. Rates of malnutrition in our study are lower than in some other studies in the critically ill population. Multiple explanations are possible, including that our hospital admits patients mostly from northern Virginia and sub-urban Washington, DC, an area with a highly educated population and among the highest per-household income in the nation. The assessments are reliant on subjectively reported data from the patient or family, which were difficult to collect in some of our most critically ill patients either due to the patient’s clinical status or the inability to reach family members for an interview. These patients were included in the analysis as having normal nutritional status, so it is possible that malnutrition prevalence was under-reported. As we did not perform adjustments to account for differences in demographic factors and severity of disease, it is not possible to attribute the increased mortality in septic patients to malnutrition. We studied only patients who were malnourished on admission and did not include those who developed malnutrition during their hospital stay. The large majority of patients were diagnosed with malnutrition based on mandatory RD assessments, and only a minority based on physician referral; it is possible that treatment teams were aware of the universal nutrition consult policy during the implementation phase and relied on it for diagnosis, rather than making their own assessment.
Although it is well known that malnutrition and sepsis are independent causes of high mortality and morbidity associated with high societal and financial costs, this is one of a few studies evaluating the impact of early assessment and diagnosis of malnutrition in patients with sepsis. Further studies are needed to expand on our findings. In particular, it would be important to study the consequences of malnutrition on outcomes in patients with sepsis in diverse patient populations and diverse socioeconomic environments. It is unclear if early nutritional support in the critically ill patient improves outcomes. Although early diagnosis of malnutrition with timely and aggressive nutritional interventions may improve outcomes, we did not collect data on the impact of universal nutrition assessment on patient outcomes.
In summary, about one in 10 patients admitted to our hospital with sepsis were diagnosed with severe or moderate malnutrition on admission after implementation of universal RD-led nutrition consult. These patients were older, had more comorbidities, had longer LOS, higher total hospital costs, and were less likely to be discharged home.
Footnotes
Author Contributions
Jessica McLaughlin: Interpretation of results, drafting, review and editing of manuscript
Nibras Chowdhury: Drafting, review and editing of manuscript
Svetolik Djurkovic: Design, data collection, interpretation of results, review and editing of manuscript
Omer Shahab: Data collection, review and interpretation of results
Mehmet Sayiner: Data collection, review and interpretation of results
Ruth Kennedy: Data collection, review and interpretation of results
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. This study is IRB exempt.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.