
Abstract
Background:
Sepsis and septic shock are severe medical conditions that can damage multiple organs with a higher risk of mortality. Recently, the combination of hydrocortisone, ascorbic acid and thiamine (HAT) was hypothesized to work synergistically to reverse septic shock and reduce mortality.
Aim:
To ascertain the efficacy of HAT therapy and compare whether HAT therapy is more beneficial compared to the standard of care in sepsis and septic shock patients.
Methods:
PubMed, Clinicaltrials.gov, Scopus, Web of Science, Cochrane and Embase are databases that were used to identify trials that conducted a study of the combination of HAT in sepsis or septic shock.
Results:
There were 134 articles identified through a database search and 16 from other sources, which were subsequently reduced to 11 trials (six randomized trials and five non-randomized trials) that were deemed appropriate for inclusion in this review. Most of the outcomes from these studies focused on mortality, the need for renal replacement therapy, duration of vasopressor use, changes in Sequential Organ Failure Assessment score, procalcitonin clearance and lengths of intensive care unit stay.
Conclusion:
Due to inconsistent results from clinical studies, the benefits of HAT therapy cannot be confirmed at this point in sepsis and septic shock. Currently, there are at least 20 randomized controlled trials testing HAT in various combinations and dosages in patients with severe sepsis and septic shock. The results of these studies are required before definitive conclusions can be made regarding the impact of this novel treatment strategy on the morbidity and mortality of patients with sepsis.
Key points
Eleven clinical studies (six randomized and five non-randomized control trials) have evaluated the clinical benefits of hydrocortisone, ascorbic acid and thiamine (HAT) combo therapy in sepsis or septic shock.
The systematic review of available clinical studies could not confirm the clinical benefits of HAT combo therapy for sepsis or septic shock.
Based on the studies analyzed, the combination treatment protocol did not lead to patient side effects or increased mortality.
Introduction
Sepsis is a dysregulated systemic inflammatory response to an infection that can damage multiple organs, while septic shock is a critical condition of sepsis with severe hypotension and a higher risk of mortality (Pendleton, 2018). In the USA, the incidence of severe sepsis is estimated to be 3 cases per 1000 population and 2.26 cases per 100 hospital discharges (Angus et al., 2001). The average costs per case were US$22,100, with annual total costs of US$16.7 billion nationally (Angus et al., 2001; Mayr et al., 2014). According to the World Health Organization (2018), the global epidemiological burden of sepsis is difficult to ascertain, and difficulties related to sepsis is most likely highest in low- and middle-income countries. It is estimated to affect more than 30 million people worldwide every year (World Health Organization, 2018). In order to reduce the burden of sepsis worldwide, sepsis treatment interventions should be sufficient, inexpensive, safe and readily available (Marik et al., 2017). Recently, the combination of HAT has been used as a new therapeutic approach to sepsis in several trials. These three agents are thought to work synergistically with one another to reduce mortality, duration of vasopressor use and incidence of renal replacement in sepsis and septic shock patients. Plasma levels of vitamin C are significantly wasted in critically ailing patients, and this can contribute to hypotension, exaggerated inflammation, microcirculatory compromise, oxidative organ injury and immune defense (Litwak et al., 2019). Besides that, vitamin C also demonstrates its role in restoring glucocorticoid receptors function once they get oxidized (Marik et al., 2017). Hydrocortisone is an anti-inflammatory agent that can help to mitigate the inflammatory response during septic shock. Glucocorticoids can amplify the effects of catecholamines via glucocorticoid receptors on vascular smooth muscle cells to suppress the production of prostacyclin and nitric oxide, which are the essential factors of vasodilator (Litwak et al., 2019). In addition, glucocorticoids can also increase the expression of the sodium-vitamin C transporter-2, which mediated the transport of vitamin C into the cells (Marik et al., 2017). Accordingly, vitamin C can aid in glucocorticoid receptor renewal, while hydrocortisone can enhance the cellular absorption of vitamin C. Another study also showed that a high dose of intravenous vitamin C could cause calcium oxalate nephropathy; thus, thiamine can be used to prevent this reaction by decreasing the conversion of glyoxylate to oxalate (Kim et al., 2018). Based on the mechanism of action on the three agents, they theoretically work synergistically together to reduce endothelial barrier changes caused by septic shock and prevent nephropathy caused by overproduction of oxalate (Litwak et al., 2019). This review aims to assess those studies to ascertain the potential benefits of the combination therapy of HAT on mortality, the need for renal replacement therapy, duration of vasopressor use, changes in Sequential Organ Failure Assessment (SOFA) score, procalcitonin clearance and length of stay for patients with sepsis/septic shock.
Methods
Database search
These databases were referenced for the research in question: PubMed (1996–April 2021), Clinicaltrials (2000–April 2021), Scopus (2004–April 2021), Web of Science (1900–April 2021), Cochrane (1996–April 2021) and Embase (1947–April 2021). The following terms were used for potential study identification: “vitamin C, hydrocortisone, thiamine, sepsis” and “vitamin C AND hydrocortisone AND thiamine AND sepsis.”
Study selection
Articles reviewed were not restricted to those written in English; however, there were no foreign language studies included. Articles were not included if the following applied: labeled review article; did not combine the three medications; did not reference sepsis or septic shock as the primary diagnosis; did not use human participants. If the study was controlled, at least one standard therapy should be a combination of HAT. Three independent researchers reviewed articles to identify relevant information referencing mortality rates, vasopressor-free days and length of intensive care unit (ICU) stay in clinically diagnosed sepsis or septic shock patients.
The following information was collected for the systematic review: study purpose; study design; whether the setting was hospital versus ICU; time frame of the study performance; drug duration/route/dose; predominant type of infection; score of severity (utilizing SOFA [Acute Physiology and Chronic Health Evaluation] APACHE II, PaO2/FiO2 and EUROSCORE II); inclusion and exclusion criteria; primary and secondary results; population size; hospital mortality index; vasopressor-free days; ventilator-free days; ICU length of stay; changes in lactate level; change in radiologic score at day 7; requirement for renal replacement therapy (with acute kidney injury [AKI] diagnosis); and procalcitonin level.
Risk of bias was evaluated by examining the randomization method, blind method, adverse effects, treatment withdrawals, missing data or any “as-treated” analysis. The risk of bias table was made by one author utilizing the Cochrane Handbook for Systematic Reviews of Interventions and evaluated by two other authors for accuracy (The Cochrane Collaboration, 2011).
Results
Initially, 134 articles were identified, with 16 others from different sources (which includes six articles provided by Nutrition and Health editors), but following a review utilizing the Preferred Reporting Item for Systematic Reviews and Meta-Analyses (PRISMA) statement, that number was reduced to 11 studies (six randomized and five non-randomized trials) (see Figure 1) (Moher et al., 2009). All 11 trials were published between the years of 2017 and 2021. A detailed accounting of the outcomes in each of those trials can be found in Table 1. The following is a discourse on the cumulative results of the major outcomes assessed by this review, such as mortality, renal replacement therapy, duration of vasopressor use, changes in SOFA scores, procalcitonin clearance, lengths of stay and a risk of bias assessment. Common sites of infection included throughout the trials were respiratory, intra-abdominal, urinary tract, pulmonary, gastrointestinal, skin/soft tissue, blood, central nervous system (CNS) and bone/joint (Coloretti et al., 2020; Fujii et al., 2020; Hwang et al., 2020; Kim et al., 2018; Litwak et al., 2019; Marik et al., 2017; Moskowitz et al., 2020; Sevransky et al., 2020; Vail et al., 2020).
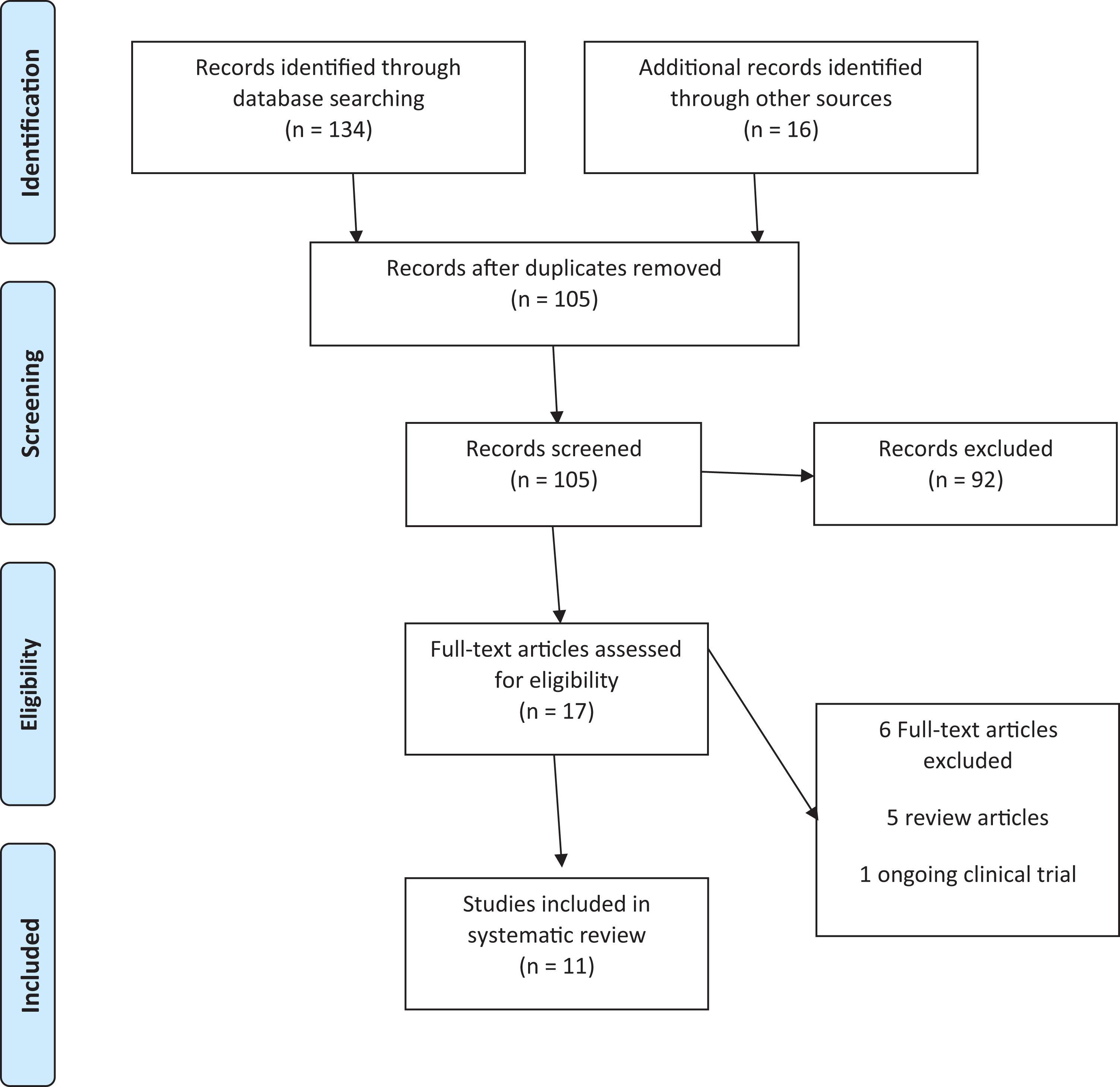
Preferred Reporting Item for Systematic Reviews and Meta-Analyses 2009 flow diagram.
Summary of all studies (Balakrishnan et al., 2018; Coloretti et al., 2020; Fujii et al., 2020; Hwang et al., 2020; Iglesias et al., 2020; Kim et al., 2018; Litwak et al., 2019; Marik et al., 2017; Moskowitz et al., 2020; Sevransky et al., 2020; Vail et al., 2020).

TG: treatment group; CG: control group; CRP: C-Reactive Protein; SOFA: Sequential Organ Failure Assessment; KDIGO: Kidney Disease: Improving Global Outcomes; UTI: urinary tract infection; ICU: intensive care unit; DNR: do not resuscitate; DNI: do not intubate; G6PD: glucose-6-phosphate-dehydrogenase; ED: emergency department; CNS: central nervous system; PCT-c: procalcitonin clearance; HAT: hydrocortisone, ascorbic acid and thiamine; HF: heart failure; COPD: chronic obstructive pulmonary disease; PCT: procalcitonin; LOS: length of stay; AKI: acute kidney injury; Δ: changes; ARDS: acute respiratory distress syndrome; PC: propensity score; GI: Gastrointestinal; IQR: Interquartile Range.
Mortality
All 11 trials examined in this review evaluated the effects that combination HAT therapy had on mortality in patients with sepsis, with four trials displaying beneficial results. The experiments by Marik et al. (2017), Kim et al. (2018), Coloretti et al. (2020) and Iglesias et al. (2020) showed decreased hospital mortality in sepsis patients who received the combination treatment of HAT. On the other hand, the studies by Litwak et al. (2019), Sevransky et al. (2020), \Moskowitz et al. (2020), Vail et al. (2020), Hwang et al. (2020) and Fujii et al. (2020) displayed no improvement in in-hospital mortality between the treatment group and the control group (Balakrishnan et al., 2018).
Renal replacement therapy
In total, nine trials (Coloretti et al., 2020; Fujii et al., 2020; Hwang et al., 2020; Iglesias et al., 2020; Litwak et al., 2019; Marik et al., 2017; Moskowitz et al., 2020; Sevransky et al., 2020; Vail et al., 2020 ) assessed in this review evaluated the effects of HAT therapy on the need for renal replacement therapy. The studies by Marik et al. (2017), Litwak et al. (2019) and Iglesias et al. (2020) all displayed a reduction in renal replacement therapy for sepsis patients who received HAT therapy compared to the control group, who only received standard care. In contrast, the other studies showed no significant difference in the requirement of renal replacement therapy between the treatment group and the control group (Coloretti et al., 2020; Fujii et al., 2020; Hwang et al., 2020; Moskowitz et al., 2020; Sevransky et al., 2020; Vail et al., 2020).
Duration of vasopressor use
All nine trials assessed in this review evaluated the effects of HAT on the duration of vasopressor(s). Six of the nine trials by Marik et al. (2017), Balakrishnan et al. (2018), Kim et al. (2018), Coloretti et al. (2020), Fujii et al. (2020) and Iglesias et al. (2020) showed beneficial results with less time to vasopressor dependence in the treatment group who received the combination therapy of HAT compared to the control group, who only received the standard care. Nevertheless, the other three studies displayed no significant difference in time to vasopressor dependence in both groups (Hwang et al., 2020; Litwak et al., 2019; Vail et al., 2020).
Changes in SOFA scores
Eight out of the 11 trials in this review evaluated the benefits of HAT on changes in SOFA scores within the first 72 hours of sepsis admission. The studies by Moskowitz et al. (2020) and Fujii et al. (2020) are the only two that showed decreased SOFA scores in patients receiving the combination therapy of HAT. Still, the other six trials displayed no significant difference in changes in SOFA scores between the treatment group and the control group (Balakrishnan et al., 2018; Hwang et al., 2020; Iglesias et al., 2020; Litwak et al., 2019; Marik et al., 2017; Sevransky et al., 2020).
Procalcitonin clearance
Out of the 11 trials, six trials in this review assessed the effects of HAT on the clearance of procalcitonin within 72 hours of sepsis administration. Studies by Marik et al. (2017), Balakrishnan et al. (2018), Hwang et al. (2020) and Iglesias et al. (2020) displayed an increase in procalcitonin clearance of the patients who received the combination therapy with a statistically significant difference in both groups. The other two trials by Coloretti et al. (2020) and Litwak et al. (2019) showed no statistically significant difference in procalcitonin clearance between the treatment group and the control group.
Lengths of stay
Of the 11 studies, eight studies in this review evaluated the benefits of the combination therapy of HAT on lengths of ICU stay in sepsis patients.
Three studies by Kim et al. (2018), Coloretti et al. (2020) and Hwang et al. (2020) exhibited statistically significant decreases in ICU length of stay between the treatment group and the control group. The other five trials did not have such an impact (Fujii et al., 2020; Iglesias et al., 2020; Litwak et al., 2019; Sevransky et al., 2020; Vail et al., 2020).
Risk of bias in randomized controlled trial
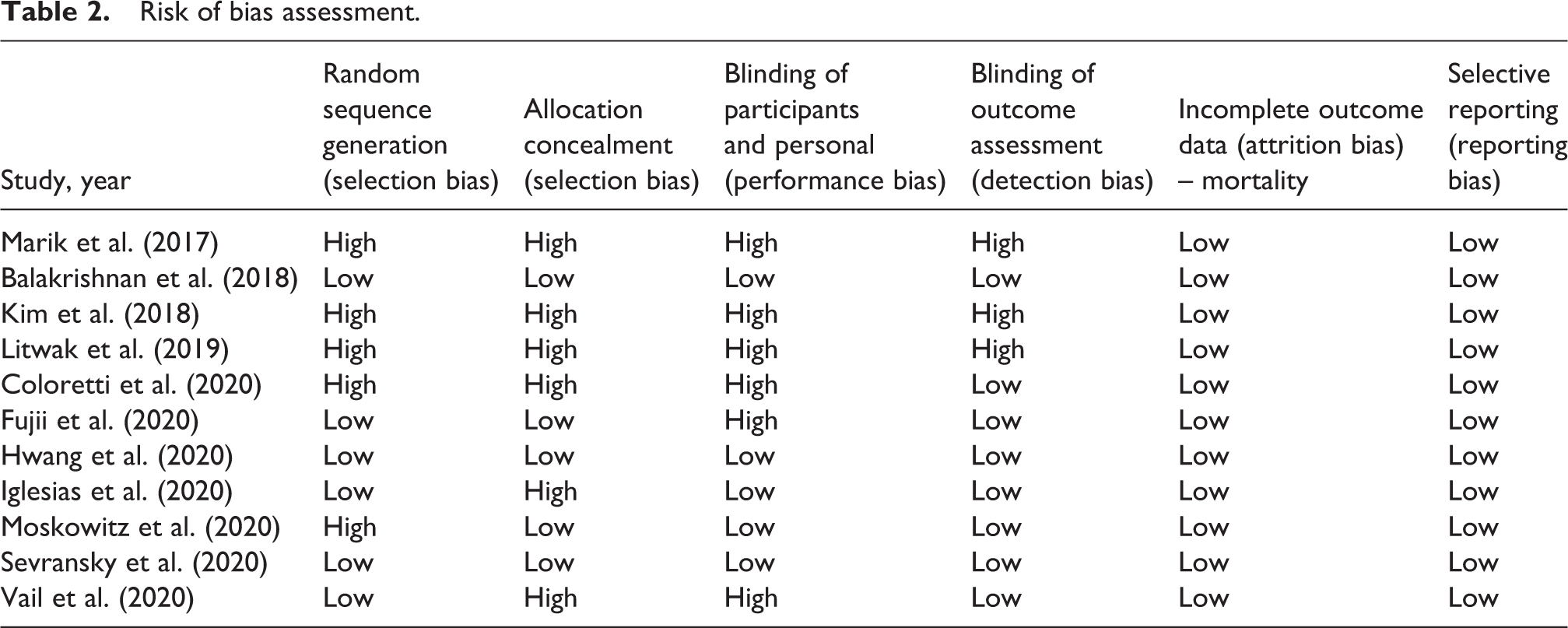
There are six randomized studies, Balakrishnan et al. (2018), Moskowitz et al. (2020), Hwang et al. (2020), Fujii et al. (2020), Iglesias et al. (2020) and Sevransky et al. (2020), while the others are non-randomized. After evaluating random sequence generation, allocation concealment, blinding of outcome assessment, blinding of outcome data addressed, incomplete outcome data addressed and selective reporting, there is no risk for bias with Balakrishnan et al. (2018), Hwang et al. (2020) or Sevransky et al. (2020). However, it is minimal in Fujii et al. (2020), Moskowitz et al. (2020), Iglesias et al. (2020) and Vail et al. (2020). All other studies revealed high selection bias, performance bias and detection bias. Table 2 provides a summary of the risk of bias assessment (Balakrishnan et al., 2018; Coloretti et al., 2020; Fujii et al., 2020; Hwang et al., 2020; Iglesias et al., 2020; Kim et al., 2018; Litwak et al., 2019; Marik et al., 2017; Moskowitz et al., 2020; Sevransky et al., 2020; Vail et al., 2020).
Risk of bias assessment.
Discussion
This systematic review evaluated all published studies with HAT therapy. Although all 11 studies assessed the clinical outcomes in sepsis or septic shock patients, the findings were inconsistent from these trials due to the variations in study design, the severity of diseases, infection types, triple regimen (consistent dose and duration) and the sample size among the studies.
Of the 11 studies, five studies were not randomized, which could increase the risk of selection and reporting bias. Although experiments by Marik et al. (2017), Kim et al. (2018) and Coloretti et al. (2020) showed the benefits of HAT therapy on mortality, these studies have some limitations, such as retrospectively non-randomized controlled, small sample size within a single-center design and the participation of nonconcurrent control participants. In this review, a total of six randomized control studies were the experiments by Balakrishnan et al. (2018), Hwang et al. (2020), Fujii et al. (2020), Iglesias et al. (2020), Moskowitz et al. (2020) and Sevransky et al. (2020). However, the Balakrishnan et al. (2018) trial only enrolled patients with sepsis and septic shock following cardiac operations, with a limited sample size that was inadequate for evaluating the difference in the mortality parameter.
Based on the baseline sepsis severity, differences arise in APACHE II and APACHE IV scores among the studies, which could be a factor that impacts the consistency in outcomes across the experiments. For instance, between the trials by Balakrishnan et al. (2018) and by Marik et al. (2017), the baseline sepsis severity from the Balakrishnan et al. (2018) trial was less severe compared to the trial by Marik et al. (2017). Due to the differences between the APACHE IV scores, the study by Balakrishnan et al. (2018) detected no statistically significant difference in mortality, whereas the study by Marik et al. (2017) displayed a reduction in mortality in the group of patients who were treated with the HAT therapy. In addition, the mortality data is not presented in the published Balakrishnan et al. (2018) trial. This is a significant limitation.
Another variation among the studies is infection types. The frequent infections that lead to sepsis and septic shock were diverse across all studies. One trial only enrolled septic shock patients from cardiac surgery, yet other trials included patients with pneumonia or other types of infections disproportionately. The Balakrishnan et al. (2018) trial did not report the site(s) of infection. The dissimilarity in types of infection may influence the treatment outcomes that lead to inconsistency about the study findings.
Dosage and duration of the triple regimen is another element that is not consistent among the trials. Some studies used the HAT therapy for four days, whereas other studies decided to extend the use of hydrocortisone for seven days or until ICU discharge. The dosage of the three agents was similar across the studies, except the dosage of hydrocortisone from the study by Litwak et al. (2019). In addition, there are several limitations in the study by Litwak et al. (2019) because the combination of HAT regimen was not protocolized.
Although the study by Litwak et al. (2019) tried to replicate the study by Marik et al. (2017), the outcomes were in conflict with one another. The inclusion criteria in the Litwak et al. (2019) study were not provided, while Marik et al. (2017) included sequential patients meeting the inclusion criteria. It is likely that there was a severe selection bias in which patients received HAT. In the study by Litwak et al. (2019), the decision to initiate and the timing of discontinuation of HAT therapy was solely based upon provider preference. About 57% of the patients in the treatment group did not complete the full four-day treatment duration due to late HAT therapy initiation, therapy discontinuation by the primary team and patient death. HAT therapy was initiated at median 13.8 h (7.5–36.8 h) from vasopressor initiation. Due to the lack of treatment protocol and interruption of therapy, the study by Litwak et al. (2019) did not detect any beneficial outcomes from the HAT therapy in sepsis or septic shock patients.
The population sample size is another limitation among these trials. In this review, the sample size ranged from 24 to 99 in four trials. With a limited sample size, some studies did not have enough power to detect the differences in clinical outcomes. Therefore, it is difficult to draw a concrete conclusion about the benefit of HAT therapy in sepsis and septic shock patients at this point. In addition, another essential clinical question has arisen in that whether the clinical benefit is from the HAT therapy or from the steroid itself.
Corticosteroids have been used as an adjunct therapy in septic shock patients for a while (Rochwerg et al., 2018). Rochwerg et al. (2018) and Fang et al. (2019) performed two systematic reviews and meta-analyses that primarily focus on the effects of corticosteroids in sepsis patients compared to the standard of care therapy. There was a small reduction in 28-day mortality with the relative risk (RR) of 0.93 and 0.90 from the studies by Rochwerg et al. (2018) and Fang et al. (2019), respectively. After examining all 11 trials, seven studies in this systematic review included patients who received hydrocortisone in both the control group and treatment group after a septic shock. There were 59.6%, 90%, 40.4% and 98.1% of patients who received hydrocortisone in the control arm in the studies by Marik et al. (2017), Kim et al. (2018), Litwak et al. (2019) and Fujii et al. (2020), respectively, while Iglesias et al. (2020), Hwang et al. (2020) and Coloretti et al. (2020) all had 100%. Four out of 11 studies (Coloretti et al., 2020; Iglesias et al., 2020; Kim et al., 2018; Marik et al., 2017) exhibited the benefit in mortality reduction significantly. By examining the control group population, the study by Kim et al. (2018) consisted of more patients who were on hydrocortisone in the control group as compared to the study by Marik et al. (2017): 59.6% and 90%, respectively. Although there were more patients who received hydrocortisone in the control group from the study by Kim et al. (2018) than the study by Marik et al. (2017), there was not much of difference in mortality reduction when comparing these two control groups from both studies. The mortality rate in the control group from Marik et al. (2017) study was 40.4%, while it was 39% in the control group from the study by Kim et al. (2018). By comparing these studies, the monotherapy of hydrocortisone may not be beneficial on mortality in septic shock. Besides that, the study by Kim et al. (2018) detected that the control group and the treatment group showed similar declines in vasopressor requirements, and it was thought that the use of hydrocortisone might help control patients with shock reversal. However, when the researchers performed subgroup analysis, for which they divided the control group into who did receive the steroid and who did not receive the steroid, they found that there was no difference in terms of hospital mortality and superinfection rates. Again, this could reinstate that the combination of HAT could work synergistically in reducing mortality rates in sepsis/septic shock patients.
Although treatment is inexpensive and devoid of side effects/complications at the recommended dose, there were neither statistically or clinically significant differences in mortality, renal replacement therapy, duration of vasopressor, changes in SOFA score, procalcitonin clearance and length of stay outcomes. However, in weighing the risks versus benefits of this treatment, there is no harm in using it despite the lack of a strong recommendation for its use. Without significant adverse effects, HAT therapy could be considered by providers when evaluating patient sepsis severity, while the clinical benefits remain controversial.
At this moment, there are only 11 trials that examined the benefits of combination therapy of HAT in sepsis and septic shock patients; however, the study outcomes were inconsistent, which makes it difficult for clinicians to apply the results in clinical practice. Fortunately, more ongoing trials are focusing on the benefits of HAT therapy in sepsis and septic shock patients. Seven ongoing trials were identified, with four dates anticipated to conclude as follows: NCT03649633 in September 2021 (still recruiting); NCT03913468 in January 2022 (active, not recruiting); NCT03592693 in September 2021 (recruiting); NCT03872011 in September 2021 (recruiting) (Kory, 2019; Mentzelopoulos and Kotanidou, 2018; Mentzelopoulos and Zakynthinos, 2020; Qingquan, 2019). There are two ongoing trials with an unknown status: NCT03540628 in February 2020 (unknown, was recruiting) and NCT03380507 in April 2019 (unknown, was recruiting) (Abdelaty and Mohamed, 2019; Haines, 2018). There is only one study, NCT03335124, that was terminated on 1 December 2018, due to insufficient recruitment (Stefanovic, 2017). The study populations are not identical among all clinical trials; however, their inclusion and exclusion criteria are comparatively similar. Most clinical trials have inclusion criteria of 18 years of age or older, diagnosis of sepsis or septic shock within 12 hours of admission in ICU and all sexes. Exclusion criteria among trials mostly include healthy volunteers, less than 18 years of age, pregnancy, underlying fatal conditions, glucose-6-phosphate-dehydrogenase (G6PD) deficiency, immunocompromised patients and patients who received steroids for other indications other than septic shock, more than 24 hours of septic shock, do not resuscitate (DNR) or do not intubate (DNI) order on admission, terminal end-stage disease and transferred from another hospital. In addition, every study has the same dosage of vitamin C, 1.5 g Q6 H, hydrocortisone, 50 mg Q6 H, and thiamine, 200 mg Q12 H, except for study NCT03872011, which used 2 g of vitamin C for their treatment group instead of the commonly used 1.5 g. As more studies arise on the benefits of HAT therapy for septic shock, a further comprehensive systematic review is needed to be undertaken once the above ongoing clinical trials have been finalized.
Conclusion
In conclusion, the clinical benefits from the combination of HAT for severe sepsis/septic shock cannot be confirmed at this time. The 11 main studies highlighted in this review did not consistently show a significant change in mortality, procalcitonin levels, duration of vasopressor use, renal replacement requirement or SOFA score to indicate infection improvement. The results of ongoing randomized controlled studies testing HAT therapy in various combinations and dosages are required to make definitive conclusions regarding the impact of this novel treatment strategy on the morbidity and mortality of patients with sepsis.
Footnotes
Authors’ contributions
Young R Lee, Kandace Vo and Jincy T Varughese contributed to the design and implementation of the research, to the analysis of the results and to the writing of the manuscript. All authors read and approved the final manuscript.
Availability of data and materials
The authors confirm that the data supporting the findings of this systematic review are available within the manuscript.
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Ethical approval
Institutional ethics approval was not applicable in this type of systematic review.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.