
Abstract
Keywords
Introduction
Fruits and vegetables are among the fundamental pillars of healthy eating and considered one of the key factors in preventing non-communicable diseases (NCDs) and death worldwide (Micha et al., 2017). A systematic analysis of the Global Burden of Disease study identified an optimal intake of 250 grams of fruit and 360 grams of vegetable per day in preventing NCDs (GBD 2017 Diet Collaborators, 2019) and the World Health Organization recommends the consumption of at least 400 grams or five servings of fruit and vegetable per day (World Health Organization, 2003).
Self-reported health (SRH) is an extensively used instrument for measuring health at the individual level (Bombak, 2013; Bowling, 2005). The instrument's popularity is mainly due to its simplicity, easy administration, and ability to predict future health status and mortality (Bamia et al., 2017; DeSalvo et al., 2006; Idler and Benyamini, 1997; Mossey and Shapiro, 1982). Previous research has identified several factors that can influence SRH, including objective health status, socioeconomic status (Bobak et al., 2000; Dowd and Zajacova, 2007; Huisman et al., 2007), psychosocial factors (Molarius et al., 2007;), and lifestyle factors such as physical activity (Abu-Omar et al., 2004; Han, 2021), smoking (Chen et al., 2007), or alcohol consumption (Gémes et al., 2019; Lindström et al., 2020; Zhao et al., 2020).
The association of fruit and vegetable intake with SRH has also been investigated by previous research. Several cross-sectional studies have described the positive association between fruit and vegetable intake and SRH (Abuladze et al., 2017; Kim et al., 2008; Lengyel et al., 2009; Södergren et al., 2012; Takaoka and Kawakami, 2013). Additionally, the relationship between fruit and vegetable intake and SRH has also been analysed in prospective studies, emphasizing the positive effect of vegetables on SRH (Mood, 2013).
Literature regarding nutrition or fruit and vegetable intake and their relationship with health remains sparse in Central and Eastern Europe, and no previous study in the region examined the association with SRH in a longitudinal manner. According to the European Health Interview Survey (EHIS), only 5% Czech men and 12% women between the age of 45 and 64 consume five or more servings of fruits and vegetables a day, and almost half of the population in this age group does not consume fruits or vegetables at all on a daily basis (EUROSTAT, 2020a). Simultaneously, the Czech Republic was found to be one of the countries with a highest rate of poor SRH, with 9.5% men and 9.6% women aged 45–64 reporting SRH as bad or very bad (EUROSTAT, 2020b).
The primary goal of this analysis was to examine fruit and vegetable intake and its relationship with SRH in the Czech part of the Health, Alcohol and Psychosocial Factors in Eastern Europe (HAPIEE) study.
Materials and methods
The HAPIEE study is an international prospective cohort study focusing on social, psychosocial, and lifestyle factors and the health of the urban population in Central and Eastern Europe. The first wave of data collection in the study’s Czech arm took place between 2002 and 2005, and a total of 8856 persons aged 45–69 years were recruited in seven cities (Hradec Králové, Jihlava, Havířov, Karviná, Kroměříž, Liberec and Ústí nad Labem). All participant completed a questionnaire survey and underwent a detailed medical examination, including blood sampling (Peasey et al., 2006). The second wave took place between 2006 and 2008, with the participation of 5210 individuals from the original sample.
Only individuals who participated in both waves were included in this analysis. From them, we excluded those with missing data on SRH from both waves (n = 36), those with poor and very poor SRH from wave 1 (n = 474), and those with missing data on fruit and vegetable intake (n = 445). Data on a total of 4255 individuals were included in the analysis. Informed consent was obtained from all participants, and the study was approved by the University College London Ethics Committee and The National Institute of Public Health in the Czech Republic.
Measures
The collection of nutritional data in the HAPIEE study is described in detail previously (Boylan et al., 2009). Daily fruit and vegetable intake was measured using the Food Frequency Questionnaire (FFQ). Participants reported how often they consumed selected foods and beverages on a nine-point frequency scale from never or less than once a month to six or more times a day. The FFQ consists of 136 items, 23 and 29 items in the fruit and vegetable group, respectively (Supplementary material, Table S1). Daily consumption of individual fruits and vegetables was calculated by multiplying the number of servings per day by the average portion size. The total daily consumption of each participant was then calculated by adding up the individual items. As a result, we obtained continuous variables of daily consumption of fruit and daily vegetable consumption. Estimating total intake using FFQ may not be accurate, especially for fruits and vegetables. There is particularly a risk of overestimating actual consumption due to social desirability bias (Miller et al., 2008). The FFQ used in HAPIEE was thus validated on a randomly selected smaller sample of participants (Stefler et al., 2014), estimating the correlation between consumption of fruit and vegetable and plasma biomarkers (vitamin C and beta carotene).
The primary outcome, SRH, was measured by the question: "In the last 12 months, would you say that your health was: very good, good, average, poor, and very poor?" Other sociodemographic and lifestyle variables were also considered in the analysis, including education (primary or less, vocational, secondary, university), economic activity (employed, entrepreneur, pensioner still employed, a pensioner not employed, housewife/unemployed), marital status (married or cohabiting, single, divorced, widowed), material deprivation measured by the availability of enough money for food, clothing, and paying bills (each question with answers on Likert scale 0–4, with overall maximum deprivation score of 12 categorized as, without problems: score 0, few problems: score 1 to 2, with problems: score 3 and more), smoking status (non-, ex-, current smokers), binge drinking of alcohol (60 g of ethanol more than once a month), and physical activity (number of hours a week engage in sports, games or hiking categorized as, no activity: 0 h per week, low: 1 to 2 h per week, mild: 3 to 5 h per week, intensive: more than 6 h per week). Finally, the health status was measured by questions on self-reported doctor diagnosed high blood pressure (yes, no), diabetes mellitus (yes, no), as well as questions on previous heart attack (HA)/acute myocardial infarction (MI), angina (A)/ischemic heart disease (IHD), stroke, cancer), and long-term health problems that needed medical treatment.
Statistical analysis
Ordinal regression models were used to examine longitudinal associations between fruit and vegetable intake from wave 1 and response to the SRH question from wave 2. We classified fruit, vegetable and combined fruit and vegetable intakes into quartiles (Q), and the ordinal regression models were adjusted for other independent variables. Model 1 looked at the relationship between the SRH, the main exposure variables, adjusted for age and sex. We further adjusted for education, economic activity, marital status, material deprivation, smoking status, binge drinking of alcohol, and physical activity, and the variables related to health status in wave 1 in Model 2. Finally, in Model 3, we added the total energy intake in megajoule (MJ), and SRH from wave 1.
To determine the possible effect of sex as a moderator of our hypothesized effect, we tested possible interactions between the nutritional variables and sex. There was no evidence for statistically significant interaction (for fruit intake, vegetable intake; the homogeneity p-values were 0.365, 0.167, respectively). Thus, men and women were assessed together in all models. Statistical analysis was calculated using IBM SPSS Statistics 25 with a selected significance level of 0.05.
Results
Sociodemographic characteristic and SRH
Data on SRH and fruit and vegetable consumption were available from a total of 4255 men and women. Most participants rated their health as average (34.9%) and good (51.8%) while 204 individuals (4.8%) rated their health as poor and 14 (0.3%) as very poor. Table 1 shows the distribution of the individuaĺs characteristics across fruit and vegetable intake quartiles. Increased fruit and vegetable intake were positively associated with being female, primary or less and secondary education, being widowed, and employed/not employed pensioners. Furthermore, it was positively associated with non-smokers, non-drinkers, and individuals with medium and intensive physical activity.
Distribution of the individuals across fruit and vegetable intake quartiles.
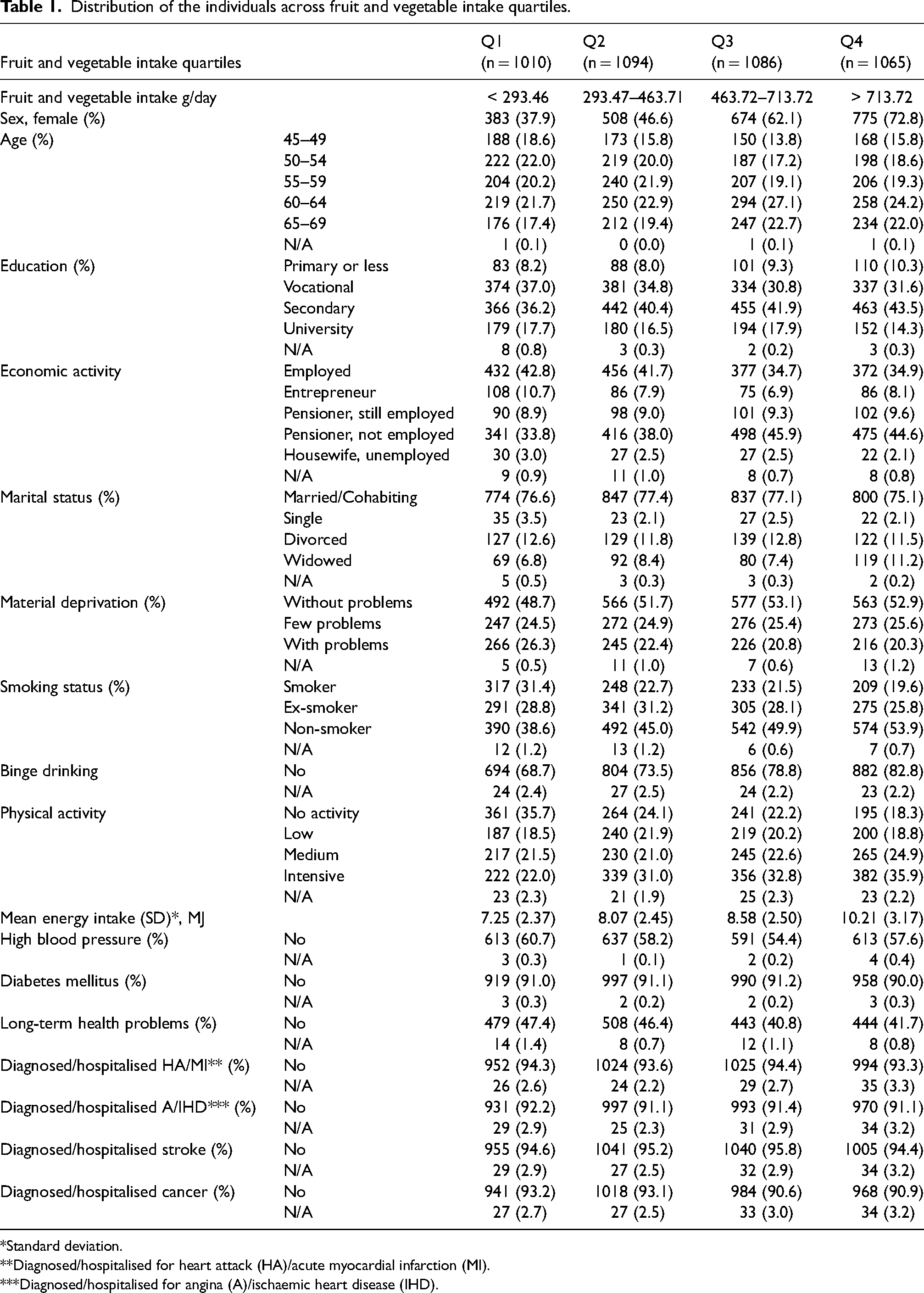
*Standard deviation.
**Diagnosed/hospitalised for heart attack (HA)/acute myocardial infarction (MI).
***Diagnosed/hospitalised for angina (A)/ischaemic heart disease (IHD).
Regression analysis of SRH and fruit and vegetable intake
Table 2 shows the odds ratios for all three models, exposure variables, and p-value for a trend in fruit and vegetable consumption categories. We chose Q4 as the reference category, and thus with decreasing consumption of fruit and vegetable, there were higher odds of worse SRH. We also observed increasing odds of worse health across decreasing consumption of combined fruit and vegetable intake in the fully adjusted model (Model 3). Those who consumed the least fruits and vegetables had significantly higher odds of worse SRH compared to those who consumed the most (OR = 1.24, CI: 1.01–1.52). Similarly, vegetable intake predicted worse SRH for individuals with less consumption (OR = 1.25, CI: 1.03–1.51). After controlling for all confounders, there was no effect of fruit intake on SRH (p value for trend 0.239).
Results of ordinal regression analysis of SRH and fruit and vegetable intake (models 1–3).
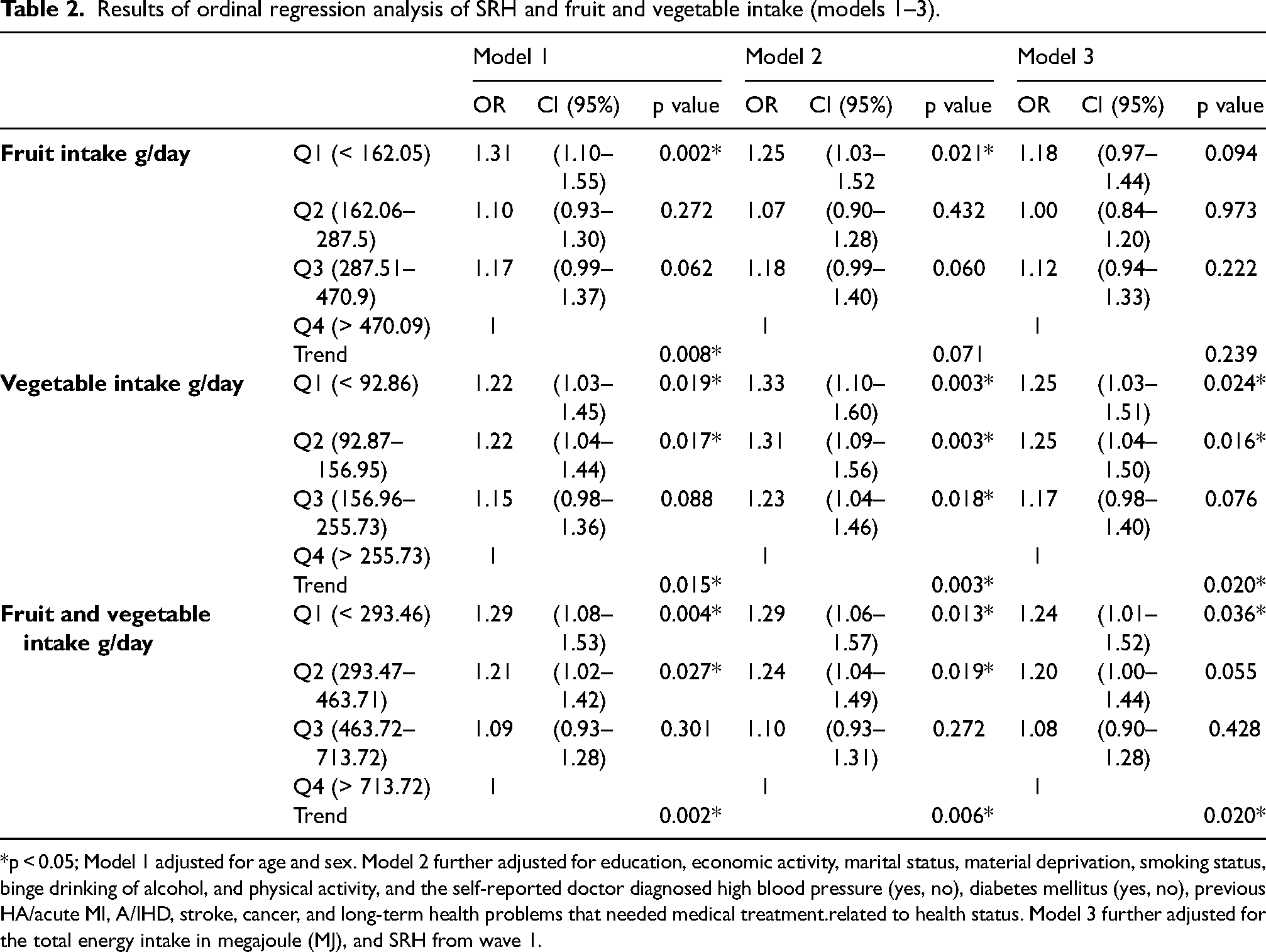
*p < 0.05; Model 1 adjusted for age and sex. Model 2 further adjusted for education, economic activity, marital status, material deprivation, smoking status, binge drinking of alcohol, and physical activity, and the self-reported doctor diagnosed high blood pressure (yes, no), diabetes mellitus (yes, no), previous HA/acute MI, A/IHD, stroke, cancer, and long-term health problems that needed medical treatment.related to health status. Model 3 further adjusted for the total energy intake in megajoule (MJ), and SRH from wave 1.
The associations with other covariates were similar for fruit and vegetable separately, as for the merged category. For combined fruit and vegetable intake (Supplementary materials, Table S2) in a fully adjusted Model 3, odds for worse SRH were negatively associated with primary or less education (OR = 1.36), non-working pensioner (OR = 1.39), with problems in the area of material deprivation (OR = 1.25), no physical activity (OR = 1.19) and with high blood pressure, diabetes and long-term health problems (OR = 1.36, OR = 1.59, OR = 1.47). Unsurprisingly, we saw an adverse association SRH from wave 1, in the good and very good category (OR = 0.25, OR = 0.04) compared to average SRH. There was no association between age, sex, smoking status, total energy intake, and variables asking individuals about diagnose and hospitalization for health conditions.
Discussion
Main findings
In this study, we analysed the longitudinal relationship of fruit and vegetable intake with SRH in an urban general population sample in the Czech Republic. We found that lower consumption of fruits and vegetables was associated with worse SRH. The association was statistically significant for vegetable intake and when fruit and vegetable intakes were merged, but not when fruit intake was assessed separately, although the direction of the effect was consistent with the other two outcomes. Poor SRH was also associated with primary or less education, non-working pensioner, materially deprived, not physically active, with high blood pressure, diabetes, and long-term health problems.
Interpretation of findings
Findings for the relationship between SRH and fruit and vegetable intake are consistent with previous literature, where generally higher risk of worse SRH with lower fruit and vegetable intakes were observed in cross-sectional (Abuladze et al., 2017; Södergren et al., 2012) as well as in longitudinal studies (Lengyel et al., 2009; Mood, 2013; Takaoka and Kawakami, 2013). A randomized control trial in Germany examined the association between several risk factors, including low fruit and vegetable intake, and SRH in a specific population group, and found that low consumption (less than five servings of fruits and vegetables per day) was significantly associated with poor SRH, but only for women (Freyer-Adam et al., 2011).
Individuals possibly assess their health based on health status and their own health behaviour (Jylhä, 2009). Taking into account high fruit and vegetable intake can affect both pathways. Fruits and vegetables are sources of beneficial substances such as vitamins, minerals, other bioactive substances, or fibre. All of these are biologically active components and may play a role in preventing the development of cardiovascular and other chronic diseases (Wang, 2014). The SRH may also reflect the awareness of an individual's health behaviour (Bombak, 2013). Eating fruits and vegetables is considered beneficial for one's perception of own health; thus, higher consumption of fruits and vegetables may lead to a better SRH. Many other factors are reflected in SRH, so characteristics, such as primary or less education, non-working pensioner, materially deprived with no physical activity, high blood pressure, diabetes mellitus, and long-term health problems, were also associated with poor SRH. However, nutrition is a modifiable risk factor for chronic health conditions, and a healthy diet should be emphasized. According to WHO, the recommended daily intake of fruits and vegetables is more than 400 grams as a part of a healthy diet (World Health Organization, 2003), and the Czech dietary guidelines are even higher (600 grams of fruits and vegetables a day) (The Czech Society for Nutrition, 2012). Almost half of our sample did not meet the threshold set by the WHO recommendation, and only a small minority consumed more than 600 grams a day. Therefore, we should promote and encourage higher consumption of fruits and vegetables, especially in mid and older age groups. Our results suggest that higher intakes could lead to better self-perceived health in the population and could potentially contribute to improved population health in the Czech Republic.
Our results are also consistent with previous studies that showed strong relationships of fruit and vegetable intake with socioeconomic factors or other lifestyle habits (Amini et al., 2021; De Irala-Estévez et al., 2000; Estaquio et al., 2008) which may confound the association with SRH. Low education or unemployment, for example, can lead to lower fruit and vegetable intake due to financial constraints, while these factors are also often predictors of low SRH (Lindholm et al., 2001). Taking into account these relationships with multivariable adjusted models is important for the validity of the findings.
Limitations and strengths
The presented study has several limitations. We used data from FFQ, which is a retrospective method, and the estimated quantity may be imprecise and over/underestimated. In fact, overestimation of fruit intake with FFQ could be up to 40% compared to 24-h recall (Kristal et al., 2005; Michels et al., 2005). However, FFQ offers a detailed record of an individuaĺs diet, and future analysis could follow the relationship of specific fruits and vegetables on SRH.
Another possible limitation is a reduction of the study sample in the second wave. Due to the drop-out, exclusion of individuals with poor and very poor SRH from wave 1, and missing data on fruit and vegetable intake, we analyse the effect on only half of the original sample. We have compared those included in the analysis and those who did not participate in the second wave. Non-participants were younger, had a higher proportion of less-educated individuals, unemployed pensioners, and more materially deprived individuals. Similarly, individuals with poor or very poor SRH in wave 1, and therefore excluded from the main analysis, were less educated, more likely to be unemployed pensioners, and more deprived. In addition, they have the highest proportion of no physically active participants. These groups are more difficult to keep participating in prospective studies (Cheung et al., 2017; Jooste et al., 1990). Considering the fact that participants were recruited only from mid-sized towns, the findings may not be entirely representative of the Czech population as a whole. To avoid residual confounding, we adjusted for a large number of possible confounders such as socioeconomic and individuaĺs health status characteristics, but we cannot exclude potential effect of some unmeasured variables.
Apart from the methodological issues and limitations discussed above, our study added new longitudinal findings to strengthen the available evidence on associations between fruit and vegetable intake and SRH. Furthermore, the HAPIEE study is the most extensive study of its kind in the Czech Republic and Eastern Europe. It collects and is a source of detailed data about dietary habits and all socioeconomic factors and creates a reliable and information-rich database for the population's long-term study.
Conclusion
In conclusion, we examined the longitudinal relationship between SRH and fruit and vegetable intake. The observed association suggests that low consumption of fruits and vegetables may lead to worse SRH. Considering the previous evidence regarding low intake of fruits and vegetables in the Czech Republic and other Eastern European countries, public health nutritional interventions that aim to increase dietary intakes of these foods have the potential to improve population health in this region.
Supplemental Material
sj-docx-1-nah-10.1177_02601060211069209 - Supplemental material for Low fruit and vegetable intake is associated with poor self-rated health in the Czech part of the HAPIEE study
Supplemental material, sj-docx-1-nah-10.1177_02601060211069209 for Low fruit and vegetable intake is associated with poor self-rated health in the Czech part of the HAPIEE study by Eliska Hrezova, Martin Bobak, Nadezda Capkova, Denes Stefler and Hynek Pikhart in Nutrition and Health
Footnotes
List of abbreviations
Acknowledgements
We would like to thank all the participants for their long-term support and Tomas Prusa for his help in the paper preparation.
Author’s contributions
EH and HP conceived the analytical design for this manuscript. MB, NC, and HP conceived the overall study design for the HAPIEE study and oversaw data collection. EH carried out data analysis, HP and DS advised on data analysis. EH drafted the initial version of the manuscript. All authors were involved in writing the paper and had final approval of the submitted manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
Informed consent was obtained from all participants, and the study was approved by the University College London Ethics Committee and The National Institute of Public Health in the Czech Republic.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The HAPIEE study was supported by the Wellcome Trust (grant numbers WT064947, WT081081); the US National Institute of Aging (grant number 1RO1AG23522) and the MacArthur Foundation Initiative on Social Upheaval and Health; CETOCOEN EXCELLENCE Teaming 2 project supported by Horizon2020 (grant number 857560) and the Czech Ministry of Education, Youth and Sports (grant number CZ.02.1.01/0.0/0.0/18_046/0015975), R-Exposome Chair project supporter by Horizon2020 (grant number 857487). The funders of the study had no role in study design, data collection, analysis, and interpretation, or writing of the manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.