
Abstract
Background:
A historical turning point occurred in the treatment of diarrhea when it was discovered that glucose could enhance intestinal sodium and water absorption. Adding glucose to salt water (oral rehydration solution, ORS) more efficiently replaced intestinal water and salt losses.
Aim:
Provide a novel hypothesis to explain why mainstream use of ORS has been strongly recommended, but weakly adopted.
Methods:
Traditional (absorptive) and novel (secretory) physiological functions of glucose in an ORS were reviewed.
Results:
Small amounts of glucose can stimulate both intestinal absorption and secretion. Glucose can exacerbate a net secretory state and may aggravate pathogen-induced diarrhea, particularly for pathogens that affect glucose transport.
Conclusion:
A hypothesis is made to explain why glucose-based ORS does not appreciably reduce diarrheal stool volume and why modern food science initiatives should focus on ORS formulations that replace water and electrolytes while also reducing stool volume and duration of diarrhea.
Introduction
A historical turning point in the treatment of diarrhea occurred in the 1960s with the discovery that glucose could enhance intestinal sodium and water absorption (Schultz and Zalusky, 1964; Anon., 1978). The mindful addition of glucose to saltwater solutions (oral rehydration solution, ORS) for the treatment of diarrhea (Nalin et al., 1968) was thereafter credited with the prevention of millions of cholera deaths (Nalin et al., 1968; Rao, 2004) and was heralded as one of the most important medical advances of the 20th century (Anon., 1978). The original formula has since been modified to equal parts glucose and sodium (1:1) with a reduced osmolality (Duggan et al., 2004). Despite the storied success of ORS and rational mainstream endorsement of its use (Patino et al., 2018), widespread adoption of ORS has waned worldwide (Pantenburg et al., 2012; Santosham et al., 2010; Wagner et al., 2015). ORS rehydrates by replacing water and salt losses, but it does not promote reabsorption of intestinal secretions (chloride, bicarbonate) or reduce stool volume. Failure to resolve common clinical endpoints (stool volume, diarrhea duration) may create the false impression that ORS does not rehydrate, leading to under-utilization (Wagner et al., 2015; Santosham et al., 2010; Pantenburg et al., 2012). Recent evidence suggests that even small amounts of glucose can stimulate intestinal chloride secretion (Yin et al., 2014) and exacerbate the secretory effects of infectious pathogens (Yin et al., 2017). A research priority of the World Health Organization (WHO) is to develop and improve ORS beyond its current capabilities (Rhoads et al., 1991). Modern food science initiatives could lead to ORS formulations that replace water and electrolytes while also reducing stool volume and duration of diarrhea.
Statement of the hypothesis
A hypothesis is made that commercial ORS formulations may not be optimally designed for treating diarrhea. The explanation provided describes how the traditional inclusion of glucose may exacerbate the net secretory state created by infectious pathogens, particularly for pathogens that also impair glucose transport. Promising innovative alternative formulations are discussed for their potential to optimize ORS for treating diarrhea.
Evaluation
Physiology of infectious diarrhea
The human intestine has both absorptive and secretory functions. Digestive secretions total c. 8 l/day, but more than 98% of those secretions are reabsorbed (Masyuk et al., 2002). Infectious diarrhea can increase intestinal fluid losses tenfold (from 200 ml/day to more than 2 l/day); cholera toxin can produce life threatening losses of > 20 l/day (Gennari and Weise, 2008). Intestinal inflammation, shortening of the villi and disruption of tight junctions (Hodges and Gill, 2010) are associated with malabsorption due to loss of mucosal surface area and brush border membrane (BBM) enzyme activity. However, mature epithelial cells are replaced by crypt epithelia, leaving secretory function intact. Therefore, structural changes in the gastrointestinal tract reduce absorption and increase secretion. Figure 1 depicts different absorptive and secretory apical and basolateral membrane proteins potentially affected by infectious pathogens (Hodges and Gill, 2010; Das et al., 2018).
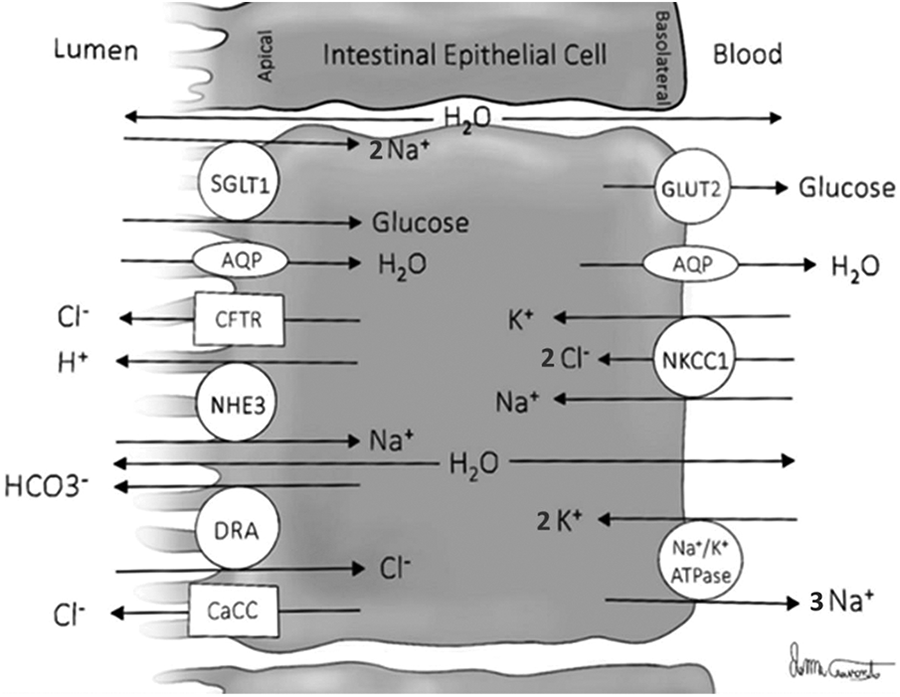
Mechanisms of water and electrolyte absorption and secretion at the apical and basolateral membranes of intestinal epithelial cells. NHE3, sodium/hydrogen exchanger-3; SGLT1, sodium/glucose cotransporter-1; DRA, down-regulated in adenoma; AQP, aquaporin water channel proteins; Na+/K+ ATPase, sodium/potassium adenosine triphosphatase; CaCC, calcium activated chloride channel; NKCC1, sodium/potassium/chloride cotransporter-1; CFTR, cystic fibrosis transmembrane conductance regulator; data compiled from Hodges and Gill (2010) and Das et al. (2018).
Understanding the roles of glucose in oral rehydration solutions ORS
The purpose of an ORS is to replace water and salt (sodium, chloride, potassium, bicarbonate) deficits incurred as a result of diarrhea. The inclusion of sugar (i.e. glucose) takes advantage of the coupled transport of sodium and glucose across the BBM (Chen et al., 1995), which enhances water absorption (Meinild et al., 1998) additively to other intestinal water transport avenues (Masyuk et al., 2002). The mechanism for this transport was identified in the 1980s as the sodium/glucose cotransport-1 protein (SGLT1) (Figure 1). In the treatment of cholera it is important to point out that the storied success (Nalin et al., 1968) of ORS may be attributable to the fact that while cholera creates enormous chloride secretion through cystic fibrosis transmembrane conductance regulator (CFTR) and calcium activated chloride channel (CaCC) activation (Figure 1), unlike some infectious pathogens it leaves SGLT1 functional (Das et al., 2018; Hodges and Gill, 2010).
The SGLT1 Km for glucose (i.e. the glucose concentration required to make SGLT1 active at half capacity) ranges experimentally from 0.6 to 30 mmol (Wright et al., 2011), which indicates a high affinity of SGLT1 for glucose. Therefore, the WHO ORS recommended concentration of glucose (75 mmol) (Table 1), as well as actual commercial ranges for glucose (99–222 mmol), is well above what is required for transport activation. The optimal ORS molar ratio of glucose to sodium ranges from 1:2 to 2:1 (Medicine, 1994), with 1:1 representing the current WHO ORS formulation (Duggan et al., 2004). Most commercial ORS also exceed the upper 2:1 ratio (Table 1). The addition of glucose to either water (Gisolfi et al., 1990; Meinild et al., 1998; Masyuk et al., 2002) or saline (Fordtran, 1975) enhances its absorption via SGLT1, by passive transport (Fordtran, 1975) and by upregulating sodium/hydrogen exchanger-3 (NHE3) expression (Donowitz et al., 2009) (Figure 1). Unlike cholera, many infectious diarrheal pathogens decrease NHE3 activity and many impair SGLT1 (Hodges and Gill, 2010; Das et al., 2018).
Glucose, sodium and osmolality characteristics of common beverages purchased to treat diarrhea.
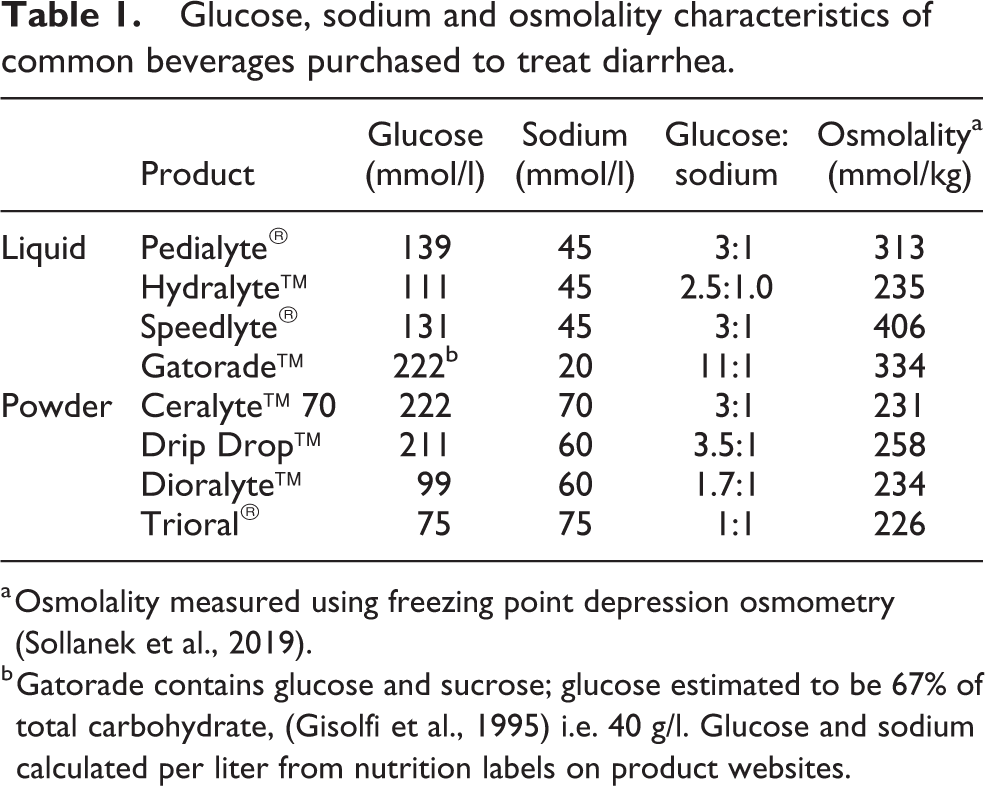
a Osmolality measured using freezing point depression osmometry (Sollanek et al., 2019).
b Gatorade contains glucose and sucrose; glucose estimated to be 67% of total carbohydrate, (Gisolfi et al., 1995) i.e. 40 g/l. Glucose and sodium calculated per liter from nutrition labels on product websites.
Glucose can also act paradoxically as an intestinal secretagogue at concentrations as low as the Km for SGLT1 (Yin et al., 2014). Glucose increases calcium activated chloride secretion in small intestinal cells (Yin et al., 2014). Yin et al. (2017) demonstrated that as little as 8 mmol glucose enhanced intestinal chloride secretion and failed to increase sodium absorption in the presence of rotavirus enterotoxin (NSP4). While some of this effect was likely due to a reduction in NHE3 expression (Figure 1), NSP4 also drastically increased the required Km for SGLT1 (Yin et al., 2017), which is consistent with rotavirus-induced carbohydrate malabsorption (Sack et al., 1982). This is especially important because rotavirus has long been a leading cause of community acquired diarrhea in children world-wide (Unger et al., 2014). E. coli is a common form of traveler’s diarrhea in adults and some strains of E. coli infection also inhibit SGLT1 in adults (Steffen, 2005). Glucose may therefore exacerbate pathogen-induced chloride secretion, particularly for pathogens that affect SGLT1. These important findings could help explain why reduced osmolality ORS, which contains less glucose, sometimes reduces stool output compared with traditional ORS (Duggan et al., 2004). However, historical efforts to redesign ORS to reduce stool output have been largely unsuccessful (Duggan et al., 2004).
The extent to which quantitative glucose-mediated chloride secretion in Ussing chamber cell preparations impact qualitative stool formation in vivo is an important consideration. As little as 50 to 60 ml of additional unabsorbed gastrointestinal secretions is enough to produce qualitatively ‘loose stools’ in accordance with a hypersecretory state (Corinaldesi et al., 2012). A significant correlation also exists between quantitative stool water content and qualitative stool type (Lewis and Heaton, 1997) with the water content difference between qualitative extremes on the order of only 20% (Blake et al., 2016). It is also important to note that the concentration of glucose used in cell studies (≤ 8 mmol) to stimulate CaCC secretion (Figure 1) is far below anything found in a commercial ORS (Table 1).
Osmolality also plays a key role in ORS efficacy (Thillainayagam et al., 1998). ORS osmolality, which is principally a function of glucose and electrolyte concentrations, determines the osmotic gradient for water movement and is one of the most important factors determining water flux in the small intestine. ORS sodium (and potassium and accompanying anions) concentrations must be made as high as possible to correct the substantial deficits incurred through diarrhea (e.g. 40–140 mmol/l sodium, 15–40 mmol/l potassium) (Gennari and Weise, 2008), but also must be kept low enough to remain palatable and hypotonic. The replacement of 75 mmol/l sodium and 20 mmol/l potassium, with accompanying anions, limits the amount of glucose to be added to < 90 mmol/l if osmolality is to remain below that of plasma (c. 280 mmol/kg). Although glucose and salt mixtures ranging in osmolality from 186 to 403 mmol/kg are made isotonic beyond the ligament of Trietz, a greater requirement for net water flux in hypertonic solutions results in faster net water absorption with hypotonic formulations (Medicine, 1994). The ranges of measured osmolality in commercial liquid ORS solutions are frequently hypertonic (Table 1).
Sports drinks were not designed for treating diarrhea and their use for this purpose is not advisable (Pantenburg et al., 2012). Sports drinks contain excessive amounts of glucose (and other sugars) and replace far too little sodium and potassium relative to diarrheal losses, thus they should not be viewed as an effective alternative to ORS. In fact, when large losses of water and salt are induced by diuretic to mimic deficits incurred with diarrhea, complete volume replacement with sports drink results in inefficient rehydration and may increase the risk for developing hyponatremia (Gennari and Weise, 2008; Cheuvront et al., 2018). The measured osmolality of liquid sports drinks is hypertonic and the glucose to sodium ratio is 10 times higher than what is recommended for an ORS (Duggan et al., 2004; Sollanek et al., 2019) (Table 1).
Novel approaches for improving ORS
Any approach to improving ORS must retain essential elements made possible by the addition of glucose, namely sodium-cotransport functions. Any novel ingredients must also keep osmolality below that of plasma. One way to achieve a lower osmolality while still maximizing the delivery of glucose as a carrier is to adopt the use of glucose polymers (e.g. maltodextrins, rice syrup). Glucose polymers exert less osmotic pressure in solution but may still pose a challenge as luminal osmolality will increase when the rate of starch hydrolysis exceeds absorption (Shi et al., 1994) leading to greater intestinal water efflux, reduced net water absorption, and possible worsening of diarrhea. Another creative solution involves the use of resistant starches, which have significantly improved water absorption in rats (Subramanya et al., 2006) and humans (Ramakrishna et al., 2000; Rabbani et al., 2004) with infectious diarrhea. Rice-based ORS performs equivalently to conventional ORS (Bhan et al., 1994) but no better. Importantly, none of these solutions would ameliorate the chloride secretory effects that glucose has as a natural digestive product of starch.
Amino acid–sodium cotransporters have also been known since the discovery of glucose–sodium cotransport (Schultz et al., 1967). The use of amino acids in ORS, whether in combination with or in isolation from glucose, have also largely performed equivalently to conventional ORS (Bhan et al., 1994; Gutierrez et al., 2007). However, the number and concentration of amino acids studied have been extremely limited. Some amino acids, such as glutamine, promote effective intestinal sodium and water absorption even in the presence of the very common rotavirus (Rhoads et al., 1991), which is known to impair SGLT1 activity and glucose absorption (Sack et al., 1982; Yin et al., 2017). Indeed, the potential benefits of glutamine in an ORS have been extensively considered (Bardhan, 2007). Further, there is increasing evidence of additional amino acid gut benefits. For example, a proprietary blend of five amino acids (threonine, valine, serine, tyrosine, tryptophan) has been demonstrated to increase NHE3 and decrease CFTR expression and functionality, reduce paracellular permeability and promote villi proliferation following radiation injury (Yin et al., 2016). Similar to radiation injury, intestinal proteins responsible for absorption (NHE3, SGLT1, down-regulated in adenoma (DRA), aquaporin water channel proteins (AQP), sodium/potassium adenosine triphosphatase (Na+/K+ ATPase)) are impaired and those responsible for secretion (CaCC, sodium/potassium/chloride cotransporter-1 (NKCC1), CFTR) (Figure 1) are enhanced in infectious diarrhea (Hodges and Gill, 2010; Das et al., 2018). Therefore, all four mechanisms improved in response to radiation injury might similarly counter the hypo-absorptive and hyper-secretory effects of many infectious diarrhea pathogens.
Other ORS ingredients may afford improvements in functional ORS outcomes as well. For example, a meta-analysis of more than 18,000 diarrhea cases indicated that zinc usage could significantly shorten the duration of diarrhea (Lamberti et al., 2013), possibly by blocking chloride secretion (Thiagarajah et al., 2015). Certain bacterial strains can decrease expression or function of DRA, CFTR and NKCC (Thiagarajah et al., 2015) (Figure 1) and can reduce the duration of diarrhea (Ahmadi et al., 2015), implicating probiotics for possible inclusion in ORS. Although some commercial products include both zinc and probiotics, we know of no commercial combination of these ingredients that has been demonstrated to be more effective than conventional ORS.
Implications
Despite the addition of glucose to ORS in amounts aimed at efficient sodium/glucose cotransport across the intestine, a pernicious secretory role of glucose in the small intestine (Yin et al., 2014; 2017) and the inhibitory effects of some infectious agents on SGLT1 activity (Hodges and Gill, 2010; Das et al., 2018) may contribute to low ORS adoption rates (Pantenburg et al., 2012; Santosham et al., 2010; Wagner et al., 2015). Innovative food science solutions incorporating alternate formulations of glucose, the addition or substitution of other ingredients such as amino acids, zinc or probiotics, may improve the current capabilities of ORS. Recent advances in understanding how diarrheal pathogens impact membrane protein expression represent an emergent approach to the development of both drug and natural diarrhea therapies (Thiagarajah et al., 2015). Ingredients that target transmembrane proteins may help optimize ORS formulations in the 21st century. Importantly, if improvements are to become widely adopted and effective, they must be achieved without compromising the cost for implementation in low-income or low-resource settings.
Footnotes
Acknowledgments
Authors’ contributions
SNC and SV were responsible for paper conceptualization; SNC and RWK were responsible for original draft preparation; LL, KMM, and SV were responsible for review and editing of paper.
Declaration of conflicting interests
SV is the Chief Science Officer and co-founder of Entrinsic Bioscience, LLC. All authors are employees of Entrinsic Bioscience, LLC., which manufactures medical hydration products.
Ethical statement
This paper involved no use of humans or animals and no new data were collected; thus, ethical approval was not required.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.