
Abstract
Keywords
Introduction
About 12 million children under 5 years of age attend early care and education centers (ECEs) (U.S. Department of Commerce CB, 2016) where they consume a substantial number of meals, affecting their dietary quality and eating habits (Larson et al., 2011; Luecking et al., 2020). ECEs provide an estimated one-half to two-thirds of the food and drink preschool aged children consume in a day, yielding the remainder of food and drink coming from caregivers at home (Benjamin-Neelon, 2018). Dietary intake of preschool aged children within the home environment can be impacted by food insecurity which is higher among low income, rural, and racially diverse families (Tomayko et al., 2017; Boles et al., 2019). Examining the child's dietary intake at both the ECE and home environment is important for understanding the preschool aged child's overall dietary quality to effectively prevent and combat childhood obesity, cardiovascular disease, and other comorbidities.
Prevalence of obesity was 13.4% among children aged 2–5 years in the United States from 2017–2018 (Fryar et al., 2020). Obese children are three times more likely to have abnormal lipids than normal-weight peers (Nguyen et al., 2015). Childhood overweight and obesity is not only a strong predictor for obesity in adulthood (Janssen et al., 2005), but also presents a higher risk for comorbidities including metabolic syndrome, type 2 diabetes, and cardiovascular disease (CVD) (Weiss et al., 2004; Lloyd et al., 2012). Over one-fifth (21%) of children and adolescents 6–18 years have at least one abnormal serum cholesterol measure (Force et al., 2016; Nguyen et al., 2015). While national data on cardiometabolic disease risk factors is not available for preschool children since these measures are not routinely collected, research indicates obese adolescents have poor lipid profiles (higher total cholesterol, higher low-density lipoprotein, lower high-density lipoprotein, higher triglycerides), higher blood pressure, and higher blood glucose levels than non-obese peers, leading to increased CVD risk (Nathan and Moran, 2008; Sinaiko et al., 2005; Warnberg and Marcos, 2008). Approximately 91% of children and adolescents 5–19 years are estimated to having a poor cardiac diet; a diet characterized by meeting only one out of five criteria for a heart healthy diet (Lloyd-Jones et al., 2010). Diets higher in sugar, sodium, total fat, saturated fat, and cholesterol increase risk for childhood obesity and CVD (Kavey, 2010; Van Horn et al., 2003; Mikkila et al., 2009). Snack foods are high in sodium, energy-dense, nutrient-poor, and lead to childhood obesity (Blaine et al., 2017; Rudy et al., 2018; Pfisterer et al., 2010; O'halloran et al., 2018).
Consumption of adequate servings of fruits and vegetables in childhood is important for sufficient nutrient intake, weight control, decreasing disease risk, and enhancing vascular health in adulthood (Aatola et al., 2010; Juonala et al., 2010; Mcguire, 2011). Diets higher in plant-based foods are higher in fiber and important for reducing or controlling cholesterol to protect against CVD (Flight and Clifton, 2006). From 2015–2018, 90% of children aged 2–5 years consumed fruit on a given day and 91% consumed vegetables on a given day (Wambogo et al., 2020). Although most young children consume fruit and vegetables daily, most children do not meet vegetable intake recommendations despite meeting fruit intake recommendations (Kim et al., 2014). According to National Health and Nutrition Examination Surveys from 2002 to 2010, children aged 2–5 years on average met the total fruit target for Healthy People 2020 from 2009 to 2010; total vegetable intake was not met and intake did not change (Kim et al., 2014). Previous studies showed that preschoolers ate more fruits and vegetables at home when they were available and accessible and when their parents consumed fruit and vegetables (Wyse et al., 2011; Bassul et al., 2020). Children living in food insecure homes are less likely to have access to fruits and vegetables (Lorson et al., 2009) and are more likely to be overweight (Gundersen et al., 2008).
Previous research reported that preschool-aged children have healthier dietary intake within the ECE environment than at home (Sisson et al., 2017; Luecking et al., 2020). Specific nutrient or food groups have been examined in previous research (Sisson et al., 2017; Bollella et al., 1999). However, the dietary intake of children at ECEs and home has not been examined using a composite dietary score reflecting the degree to which intake conforms to guidelines for a diet beneficial for heart health. Studies among adolescent-aged children (11–12 years) reported that home availability of fruits and vegetables was associated with fruit and vegetable intake, irrespective of environment (e.g. home or school) (Koui and Jago, 2008). However, access to food at home has only been examined in relation to preschooler fruit and vegetable intake within the home, not primary environments such as ECEs (Wyse et al., 2011; Bassul et al., 2020). Evaluating home food access and children's dietary intake at home and ECEs in terms of a composite heart-healthy diet score is needed to understand the gaps and to effectively prevent CVD.
The purpose of this study was to determine whether greater access to fruits, vegetables, and snacks at home was associated with heart-healthy diet score at home and at ECEs in preschool-age children, and to determine whether there is a difference in heart-healthy diet score between home and ECEs. We hypothesized that greater access of fruit and vegetables at home would be associated with a more heart-healthy diet at home and ECEs, and that heart-healthy diet scores would be higher at ECEs than at home.
Methods
Study design and participants and recruitment
This was a secondary, cross-sectional study of families with 3-to-5-year-old children and ECEs across Oklahoma in 2011–2013. Sixteen ECEs and 88 children and their primary caregivers participated. ECE program eligibility included provision of a lunch meal. Centers were recruited as part of larger studies (Sisson et al., 2017; Rasbold et al., 2016). Recruitment included ECEs operated by Native American Tribes and Nations. Thirty-seven ECEs were contacted via telephone; 13 did not qualify, eight had scheduling conflicts, and 16 childcare centers participated. Caregivers whose 3-to-5-year-old children attended these 16 centers were invited to participate after providing informed consent. Participants provided information on the home environment and child demographics via telephone interview with trained researchers. A total of 252 caregivers provided consent; 90 participated in telephone interviews. Eighty-eight children had at least one observed lunch at the ECE and a caregiver who participated in the telephone interview. The University of Oklahoma Health Sciences Center Institutional Review Board and appropriate tribal review boards approved all study activities.
Dietary access at home
The Healthy Home Survey is a telephone survey to measure elements of the obesogenic home environment, including food access, of young children (Bryant et al., 2008). Questions from the survey that determined the home availability of fruits and vegetables were included. Family responses were recorded per food category. The Healthy Home Survey has reported a mean kappa value 84.4%-95.6% for reliability of food availability items. Test re-test reliability for food variety was high (substantial to almost perfect) for most items. Food environment assessment found that percent agreement for reliability (mean = 86%) and validity (mean = 71%) ranged from 58% to 98% (Bryant et al., 2008).
Home dinner dietary intake
Caregivers were asked to recall the previous three nights of dietary intake at dinner (3-Dinner Dietary Recall). Some caregivers could only recall one (n = 1) or two days (n = 10). If only one dinner was reported, this meal was used as the average for all three dinners. Dependent t-test analysis indicated no differences between intake on day one and intake on day two for children with two recalls. If only two dinners were reported, the average of the two reported dinners was used to represent the third dinner. Values for all three days were averaged for analyses. Trained researchers gave descriptive examples to obtain accurate serving sizes of foods consumed. Probing questions were asked regarding the food preparation and specifics, including brand names, ingredients in mixed dishes, and added condiments.
Dietary intake at early care and education lunch
Using the Dietary Observation for Child Care (DOCC) system (Ball et al., 2007), plate waste was used to assess all foods and beverages served to and eaten by children at ECEs during lunch. DOCC is an accurate method for estimating intake when compared with measured plate waste for determining children's intake (Pearson's r = 0.90–0.95) (Ball et al., 2007). Trained field observers had prior plate waste competency through plate waste training, passed a plate waste practical exam, and had a high reliability between observers across foods (Intraclass Correlation Coefficient = 0.968, P < 0.001). Each observer recorded the amount and type of all foods and beverages served to the children, any food spilled or given away, and additional servings for up to three children (Ball et al., 2007). The total food consumed by each child was found by calculating the difference between what was served and what was remaining.
Plate waste was obtained during two different lunch times for 65 children and during one lunch time for 23 children. Dependent t-test analysis indicated no differences between intake for days one and two. Thus, day one values were used instead of averaged two-day values for those 23 children with a single observation. Values for both days were averaged for analyses.
Nutrient analyses
Recipes were collected for mixed dishes. Trained researchers entered recipes into nutrient analysis software, FoodWorks® version 10, to obtain nutritional information on the specific nutrients (fiber, energy, total fat, saturated fat, protein, cholesterol, carbohydrate, and sodium). Total amounts of fish, fruit, vegetables, and total fruit and vegetables were calculated. High fat and high sugar foods, salty snacks, sugar drinks, fruit juice, and total of sugary drinks and fruit juice children consumed at home were calculated to comprise the snacks category. Energy, total fat, saturated fat, protein, fiber, cholesterol, carbohydrate, and sodium were determined using FoodWorks® (The Nutrition Co., Long Valley N.J.) and the United States Department of Agriculture food database. Evaluation of dietary intake included descriptive statistics (mean ± SD, frequencies) of macronutrients and food groups (energy, fat, saturated fat, protein, cholesterol, carbohydrate, sodium, fruit, vegetables, total fruit and vegetables, and snacks) at home and ECE centers.
Heart-healthy diet score
The six components of the heart-healthy diet score were consumption of fish, fruits, vegetables, fiber, and limited sodium and sugary drinks (e.g. fruit juice, sports drinks, and sugar sweetened beverages; Table 1). Heart-healthy diet scores ranged from zero to six. A score of six was considered ideal. Fiber and sodium were determined though nutrient analysis of the DOCC and 3-Day Dinner Recall. Remaining components from the DOCCs and 3-Day Dinner Recalls were recorded manually on data sheets; data were then transferred to Excel. A point for fish was given if any portion was consumed at a meal. A point was given for remaining heart-healthy diet score components if children met age- and sex-specific national references standards of the American Academy of Pediatrics (AAP) and American Heart Association (AHA) for dietary intake (Gidding et al., 2006; Pediatrics, 2018; National Academies of Sciences and Medicine, 2017).
Heart-Healthy Diet Score Components According to Sex and Age for Foods Consumed at One Meal.
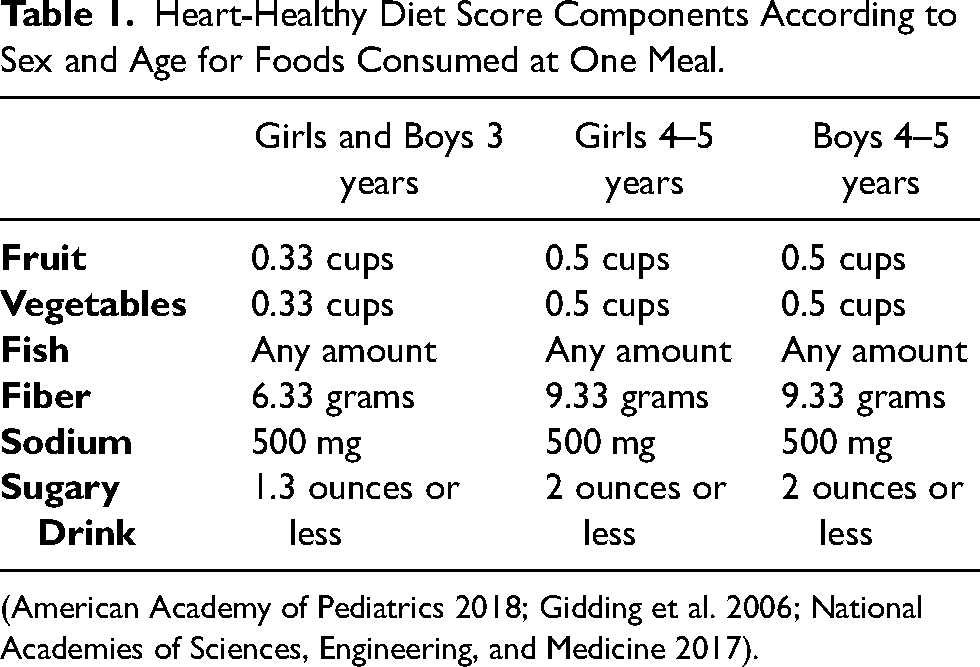
Heart-Healthy Diet Score Components According to Sex and Age for Foods Consumed at One Meal.
(American Academy of Pediatrics 2018; Gidding et al. 2006; National Academies of Sciences, Engineering, and Medicine 2017).
All heart-healthy diet score components from days 1–2 of ECE center DOCCs and days 1–3 of home 3-Day Dinner Recall were averaged for each child in Excel. In SAS, conditional “if-then” statements were utilized with appropriate formulas for the heart-healthy diet score standards for child sex and age to determine whether children met the 1/3 day cut-points for the heart-healthy diet score components (Table 1). Children were given a score of a “1” if they met the heart-healthy diet score criterion and a “0” if they did not meet the age- or sex-specific score standards (Table 1).
Descriptive statistics (mean ± SD, frequencies) were calculated for demographic characteristics and children's home access to fruits, vegetables, and energy-dense snacks. Paired samples t-tests were used to determine differences between nutrients and child mean heart-healthy diet score variables. Wilcoxon sign rank test was used to determine differences in heart-healthy diet score frequency at home and ECEs and within rural or urban environments. An independent Wilcoxon test was used to determine differences in heart-healthy diet scores across rural and urban environments.
A series of adjusted linear regression analyses were conducted to examine the relationship between the home food access and heart-healthy diet score at home and ECEs. Due to limited sample size and to protect model stability, possible covariates (e.g. age, sex) were included only if significantly correlated with predictor or outcome variables. Age was significantly correlated with the ECE heart-healthy diet score (r = -0.25, P = 0.0187) and therefore included in adjusted linear regression analyses. Kruskal-Wallis tests were used to determine a difference between heart-healthy diet scores at home and ECE with race, number of children at home, household income, and occupation of child's caregiver. All analyses were conducted using SAS (Statistical Analysis Software, 9.4). Due to multiple testing, the alpha was adjusted, using the Bonferroni method for significance (P = 0.0007).
Results
Demographics
The average child age (n = 88) was 3.8 ± 0.7 years; and relatively even distribution between females (52%) and males (48%) (Table 2). The sample was racially/ethnically diverse; 57% reported non-white race/ethnicity (Table 2). Most families (52%) reported an annual household income of $10,000-$50,000 and 71% of the child's primary caregivers worked full-time outside the home. Families reported various grocery shopping patterns, with the most common being a big trip every other week, with a few small trips during the week (33%). Eleven of the 16 participating ECEs were tribally-affiliated full-day ECEs located in rural Oklahoma, primarily enrolling American Indian children; the remaining 5 ECEs were in urban settings. There was no statistically significant difference between heart-healthy diet score at home and ECEs with race, household income, number of children within the home, or with child's primary caregiver occupation.
Descriptive Characteristics of Participating Families with 3-to-5-Year-Old Children in Early Care and Education Programs Across Oklahoma from 2011–2013 (n = 88).
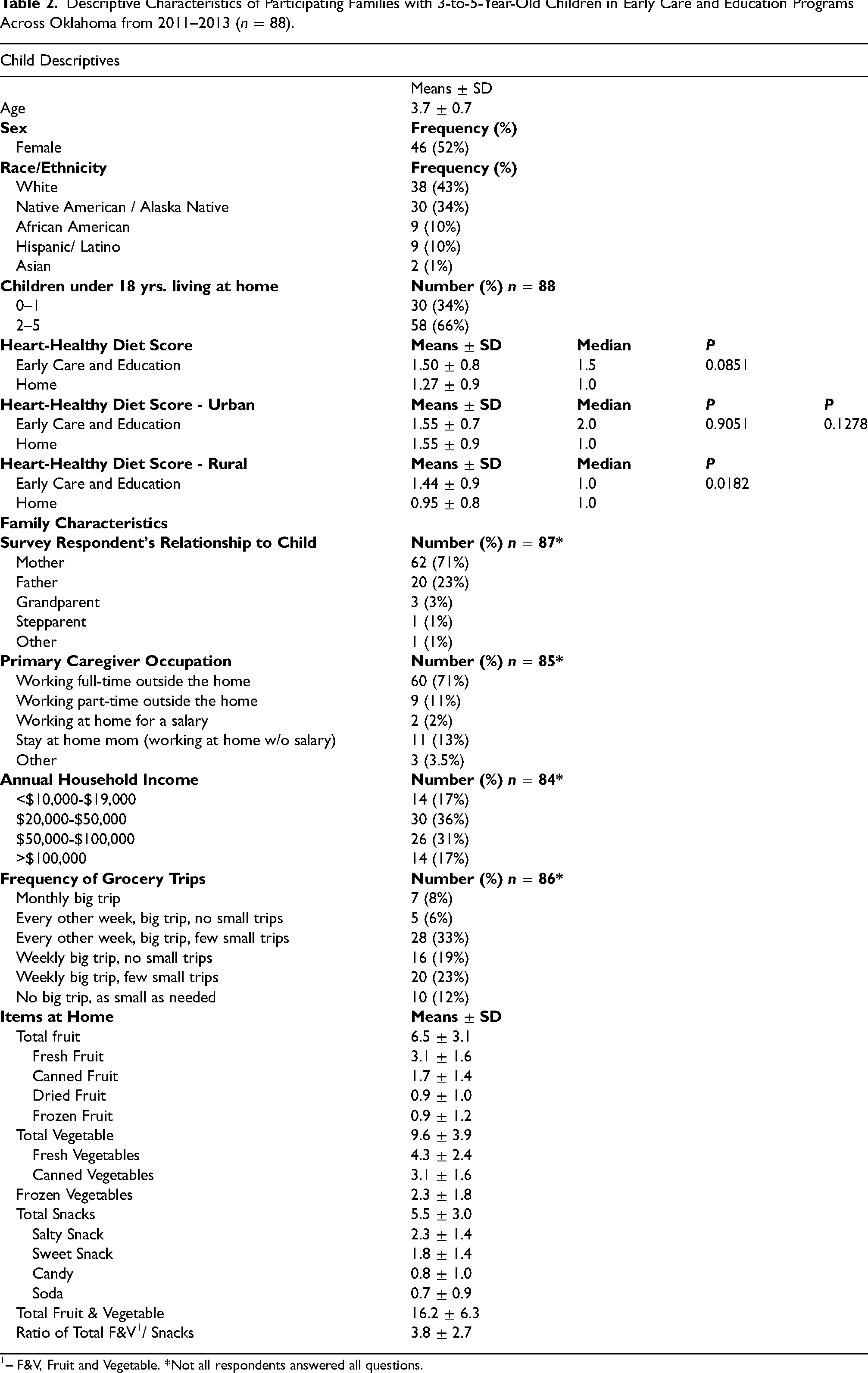
Descriptive Characteristics of Participating Families with 3-to-5-Year-Old Children in Early Care and Education Programs Across Oklahoma from 2011–2013 (n = 88).
– F&V, Fruit and Vegetable. *Not all respondents answered all questions.
Home access of total fruits and vegetables (16.2 ± 6.3) outnumbered snacks (5.5 ± 3.0) with the mean ratio of total home fruits and vegetables to snacks at 3.8 ± 2.7 (Table 2). Specific foods within the fruit, vegetables, and snack categories are shown in Table 2 and Figure 1.
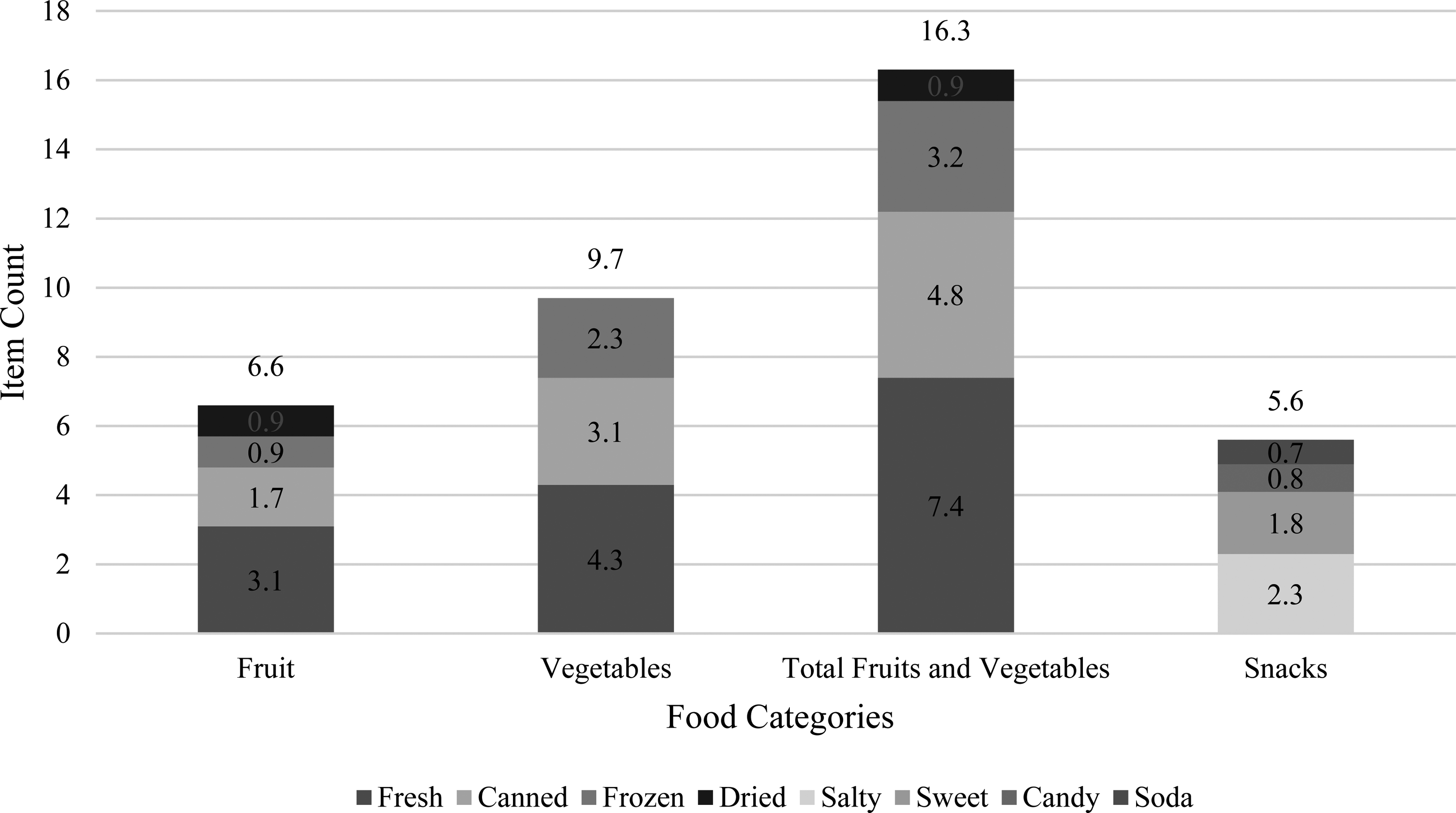
Average Counts of Home Food Access to Fruit, Vegetables, and Snacks in Oklahoma Families with 3-to-5-Year- Old Children Attending ECE Programs in 2011–2013 (n = 88).
Dietary intake at ECEs had lower kcals, protein, carbohydrates, total fat, saturated fat, cholesterol, and sodium than did dietary intake at home (Table 3). Protein (16.5 ± 9.8 at ECE; 20.9 ± 8.8 at home) and sugar (19.1 ± 11.1 at ECE; 16.8 ± 10.4 at home) were the only nutrients that were not different across ECEs and home. There was no difference in heart-healthy diet score between ECEs (1.50 ± 0.8) and home (1.27 ± 0.9, P = 0.0934) and based on urban (ECE 1.55 ± 0.7; home 1.55 ± 0.9; P = 0.9051) or rural sites (ECE 1.44 ± 0.9; home 0.95 ± 0.8; P = 0.0182). There was no difference in heart-healthy diet scores across rural and urban groups (P = 0.1278) (Table 2). Approximately 10% of children met at least three of the heart-healthy diet score criteria at ECEs, while 9% did at home (Table 3).
Nutrient Values and Heart-Healthy Diet Score
2
of Foods Consumed by 3-to-5-Year-Old Children in ECE Programs Across Oklahoma from 2011–2013 (n = 88).
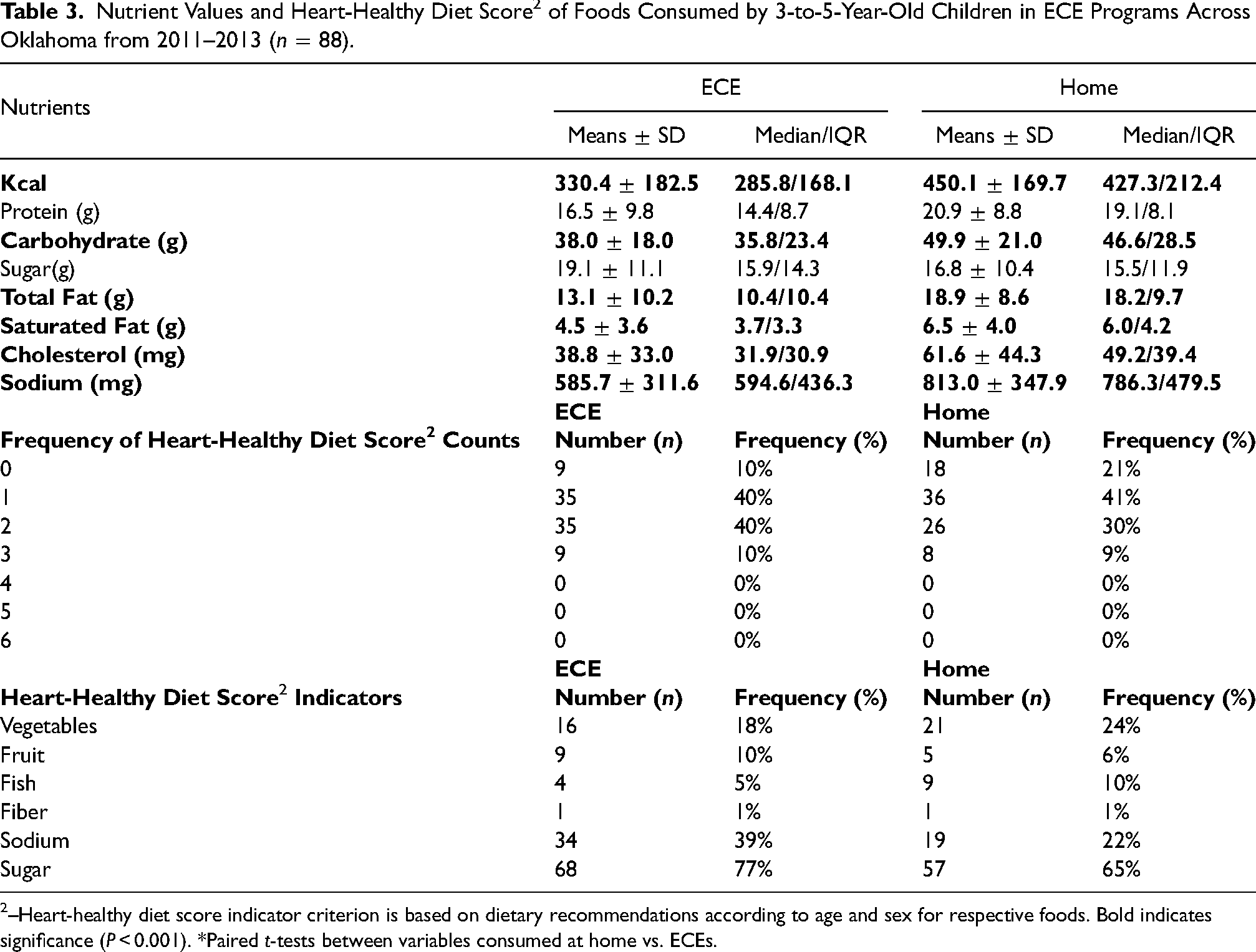
Nutrient Values and Heart-Healthy Diet Score 2 of Foods Consumed by 3-to-5-Year-Old Children in ECE Programs Across Oklahoma from 2011–2013 (n = 88).
–Heart-healthy diet score indicator criterion is based on dietary recommendations according to age and sex for respective foods. Bold indicates significance (P < 0.001). *Paired t-tests between variables consumed at home vs. ECEs.
A majority of children in the ECE and home environments met guidelines for sugars (77% at ECE vs. 65% at home; Table 3). Children did not meet intake recommendations for other variables (vegetables [18–24%], fruit [6–10%], fish [5–10%], fiber [1%], sodium [22–39%]; Table 3) at both environments.
There was no relationship between home food access variables of total fruits and vegetables and snacks and heart-healthy diet scores and nutrients, either at home or at ECEs (Table 4, Table 5).
Relationship of Home Availability of Total F&V
1
and Snacks Available in the Home and the Home and ECE Heart-Healthy Diet Score of 3-to-5-Year-Old Children in Oklahoma ECE Programs in 2011–2013 (n = 88).
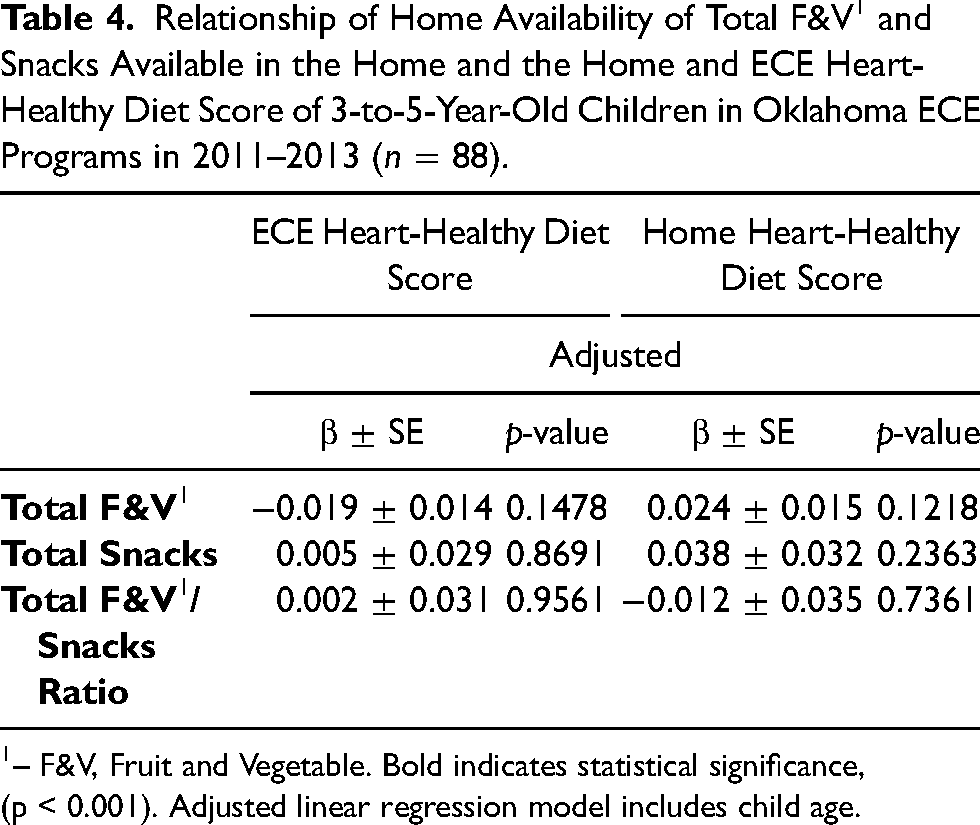
Relationship of Home Availability of Total F&V 1 and Snacks Available in the Home and the Home and ECE Heart-Healthy Diet Score of 3-to-5-Year-Old Children in Oklahoma ECE Programs in 2011–2013 (n = 88).
– F&V, Fruit and Vegetable. Bold indicates statistical significance, (p < 0.001). Adjusted linear regression model includes child age.
Relationship of Home Availability of Total F&V1 and Snacks and Nutrients Consumed at Home and ECE in 3-to-5-Year-Old Children in Oklahoma in 2011–2013 (n = 88).
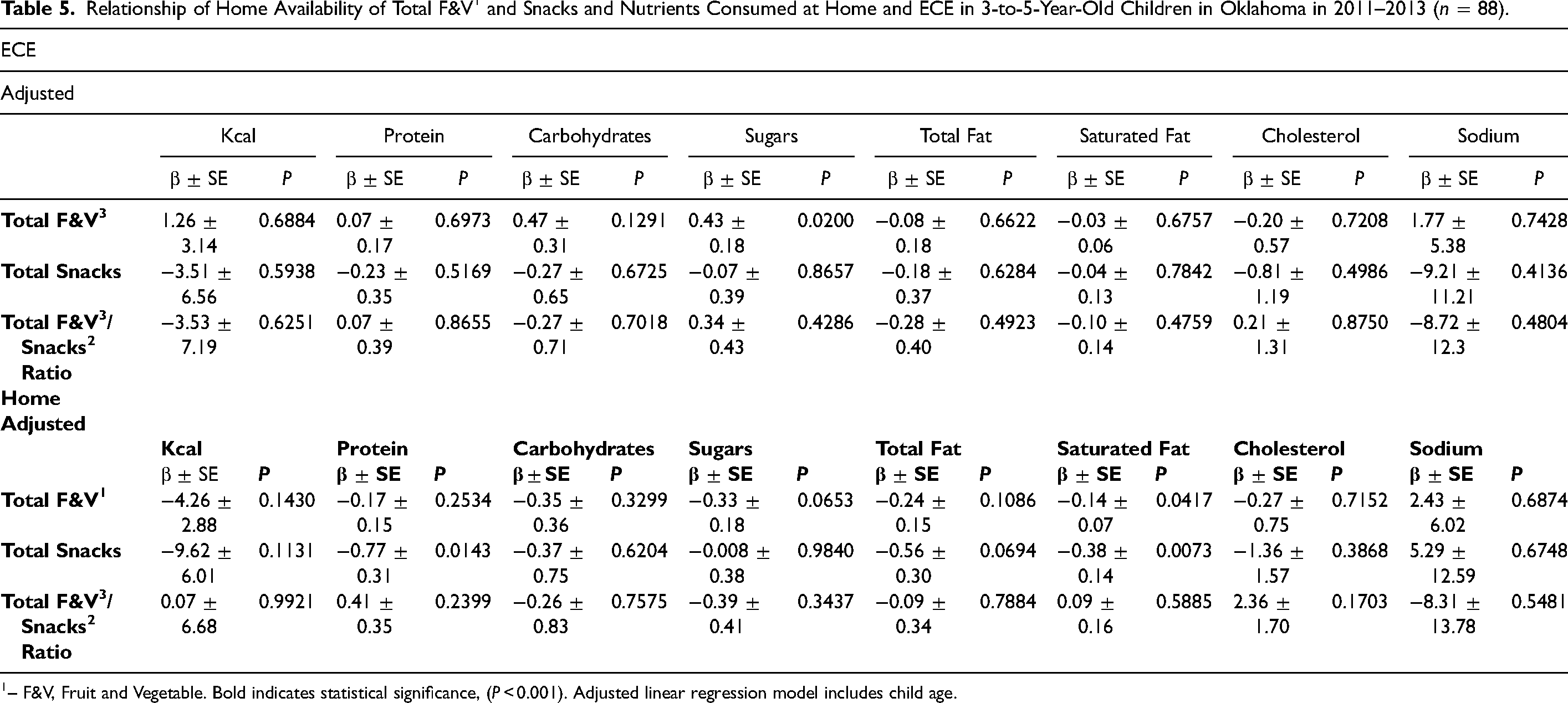
– F&V, Fruit and Vegetable. Bold indicates statistical significance, (P < 0.001). Adjusted linear regression model includes child age.
The findings showed low heart-healthy diet scores at home and ECEs with the lowest score at home within the rural environment. Contrary to our hypothesis, there was no difference in heart-healthy diet score between environments. There was also no difference in heart-healthy diet scores between ECEs and home based on urban or rural sites, race, household income, number of children within the home, or child's primary caregiver occupation. Home access to total fruits and vegetables and snacks was not associated with heart-healthy diet score at home or ECE. The heart-healthy diet score was contingent upon volume of healthy food group consumption and specific nutrient intake per meal. Although child mean nutrient intakes at ECEs were better than at home, age- and sex-specific cut points may not have been met for heart-healthy diet score components. The heart-healthy diet score may have been lowest within the rural home environment due to factors such as low income, caregivers working outside the home, and a substantial Native American population (Tomayko et al., 2017; Boles et al., 2019). During data collection, Child and Adult Care Food Program (CACFP) guidelines gave ECEs the option of offering a minimum of one serving of fruit or vegetables at lunch for preschoolers (Services, 2020), potentially affecting children's consumption of one of these food groups at lunchtime at ECEs. Current CACFP guidelines now require one serving of fruits and vegetables or two servings of different vegetables at lunchtime, supporting more healthy fruit and vegetable intake (Services, 2020). ECE center compliance with CACFP guidelines does not guarantee children will meet age- and sex-specific servings for healthy foods as recommended by the Dietary Guidelines for Americans (Hasnin et al., 2020). Both current and former CACFP guidelines need improvement, as they do not meet the heart-healthy diet score or Dietary Guidelines for Americans (U.S. Department of Agriculture, 2020).
The present study found home access to fruits and vegetables and snacks was not associated with heart-healthy diet score at ECE. Previous research has reported home food access to healthy foods equates to healthier daily intake, nonspecific to environment, the studies involved adolescents, not preschoolers (Koui and Jago, 2008; Cho and Kim, 2018). Research among adolescents utilized self-reported weekly intake (Koui and Jago, 2008; Cho and Kim, 2018), which may present social desirability bias. One such study had a small sample size and was conducted outside the United States, presenting limitations based on cultural differences (Koui and Jago, 2008). Child dietary intake at ECE may have been low, regardless of home food access due to abovementioned CACFP guidelines that were in effect during the data collection for this study.
The present study found home access to fruits and vegetables and snacks was not associated with heart-healthy diet score at home. This is contrary to previous research that has found positive associations between preschool aged children's fruit and vegetable intake at home based on availability at home (Wyse et al., 2011). Previous research has reported that healthy home food access with parental preparation and intake of fruit and vegetables is positively associated with higher fruit and vegetable intake in preschool-aged children at home (Bassul et al., 2020; Wyse et al., 2011). Parental involvement in consuming and preparing nutritious foods at the home may be key to healthy intake among children. Research also supports that preschool children from dual-parent households whose mothers work outside the home consume more unhealthy foods and less healthy foods (Wu, 2018). A majority (71%) of caregivers within this study, who were mothers, worked outside the home. About 52% of the households within this study had an annual household income of $10,000-$50,000 and 66% of households had 2–5 children under the age of 18 years at home. The monthly cost for a family of four to follow the MyPlate, based on the DGAs, is $1109 to $1249/month (Mulik and Haynes-Maslow, 2017). Therefore, barriers such as primary caregivers working outside the home and the cost of eating healthier with multiple children to support may have affected the dietary intake of children at home even as our study found no difference in heart-healthy diet scores between home and ECE based on these demographic factors.
At home and ECEs, the highest heart-healthy diet score was 3 out of 6 components, similar to other studies reporting 0 to 3 out of 5 components from the AHA Healthy Diet Score or similar measure (Pacor et al., 2016; Aatola et al., 2014; Ning et al., 2015; Alman et al., 2014; Shay et al., 2013; Steinberger et al., 2016; Ruiz et al., 2015; Lenhart et al., 2014). Of these previous studies, only two reported on similarly aged children and the age ranges extended into middle childhood (5–11 years and 2–19 years), (Ning et al., 2015; Steinberger et al., 2016) making it difficult to compare across studies (Pacor et al., 2016). Fiber and fish intake were the two lowest components at ECEs and home and may be due to low whole grain intake(Finn et al., 2019) and the greater expense of fish with limited budgets(Otten et al., 2017; Mulik and Haynes-Maslow, 2017). Similar to previous studies, the present study showed more calories, protein, carbohydrate, and fat were consumed at home than at the ECE (Sisson et al., 2017; Sepp et al., 2001). Sodium intake was also higher at home than at ECEs though above recommendations within the ECE environment (O'halloran et al., 2016). Menu analysis of both urban and rural ECEs has found them high in sodium (Frampton et al., 2014) and high intake of sodium at ECEs may be due to centers serving breads, cereals, processed meats, and packaged foods containing high sodium levels(Frampton et al., 2014; O'halloran et al., 2018; O'halloran et al., 2016). The combined higher intake of calories, total fat, saturated fat, and sodium at home within our study may be due to either full-service restaurant, fast-food, or ultraprocessed foods consumed at dinnertime (Powell and Nguyen, 2013; Wang et al., 2021). Daily snacking at home, common among preschoolers (Hutchinson et al., 2018), may have been an additional contributor to carbohydrate and calorie intake at home (Xue et al., 2019); the top three snacks within home food access were chips, crackers, and nuts, which are higher in carbohydrates, unsaturated fats, and sodium. The combined mean sodium intake of children at lunch at ECEs and dinner at home would be very close to exceeding daily sodium guidelines, as is common among children across the United States (Steinberger et al., 2016; Wang et al., 2021). Aligning CACFP guidelines with Dietary Guidelines for Americans, AHA, and AAP guidelines would help to ensure improved intake of healthy food groups and fiber, and reduce sodium and sugar consumption, among preschoolers (Gidding et al., 2006; Steinberger et al., 2016; Pediatrics, 2018).
Strengths of the present study include a diverse sample of children and families. All researchers completed detailed training and certification and all instruments were validated. ECE participation in the CACFP was not recorded, but ECE licensure within Oklahoma requires adherence to the CACFP meal pattern (Services, 2020). Participating ECE centers were located across Oklahoma in urban and rural settings. Limitations should also be discussed. First, social desirability bias could have influenced parents recording the 3-Day Dinner Recall. Second, the heart-healthy diet score measure has not been previously validated, but is based on national references standards for children from the AAP and AHA (Gidding et al., 2006; Pediatrics, 2018). A validated heart-healthy diet health measure for preschool aged children has not yet been developed, as barriers of limited cardiac data in early childhood (Pacor et al., 2016), metric simplicity, standardization, and age-appropriateness remain (Steinberger et al., 2016). The six heart-healthy diet score components mirrored the AHA Healthy Diet Score (Lloyd-Jones et al., 2010), which is part of AHA's Life's Simple 7 and used in adults and children, although only validated among adults (Folsom et al., 2011). The AHA Healthy Diet Score includes the following five dietary components: fruits and vegetables; fish, limited sodium, limited sugar-sweetened beverages, and whole grains (Lloyd-Jones et al., 2010). The difference with the AHA diet score and our score was “fiber” in place of “whole grains,” as dietary fiber is more strongly associated with reduced CVD risk factors in children (Steinberger et al., 2016; Fulgoni et al., 2020). As the heart-healthy diet score in the present study was dependent on volume of child intake at lunch or dinner, this may have led to an inaccurate characterization of overall daily intake, as breakfast meals and snacks were not included. Future research is needed to develop and validate an appropriate measure for heart-healthy diet health among preschoolers. Additionally, future directions should develop interventions for improving heart-healthy dietary intake among preschool aged children who live rurally, whose primary caregivers work outside the home, and whose families are low-income, and culturally diverse.
Due to multiple testing, the Bonferroni correction was used to protect against Type 1 statistical errors (Andrade, 2019). Our Bonferroni correction yielded a very low adjusted alpha level (P = 0.0007). A limitation of this measure is the potential for Type 2 statistical errors (Andrade, 2019). This low alpha level additionally limited the opportunity for statistical significance.
Conclusions
Our findings confirmed that the heart-healthy diet health of children at home and ECE does not meet recommendations, despite access to healthy foods at home. Future directions should include interventions supporting preschool aged children from families that are located rurally, low-income, racial minorities, and whose primary caregivers work outside the home. Additional implications include promoting policies that will even more closely align the CACFP guidelines with the DGAs, AHA, and AAP recommendations for cardiac health among preschool children. As young children depend on the provision of meals from their parents, heart healthy dietary interventions that target both parents and children might increase the likelihood of improved dietary intake at home.
Footnotes
Abbreviations
Acknowledgements
We would like to thank the Oklahoma ECE centers and families that participated and partnered together in this project. We also thank the tribal nations who participated in this project. We also thank the Behavioral Nutrition and Physical Activity Laboratory students who participated in data collection and management. Finally, we thank Kathy Kyler who conducted scientific editorial review of this manuscript.
Authors’ contributions statement page
Mrs. Rasmussen participated in study concept and design, data analysis, data interpretation, and writing and revision of the manuscript.
Dr Sisson assisted in study concept and design, interpreting analysis, writing, and revising the manuscript.
Dr Campbell contributed to study concept and design, interpreting analysis, and revising the manuscript.
Dr DeGrace contributed to study concept and design, interpreting analysis, and revising the manuscript.
Professor Baldwin provided guidance with study concept and design, data analyses, data interpretation, and revising the manuscript.
All authors have read and approved the final version of the manuscript.
Availability of data and materials
These data are not publicly available. Opportunity for collaborations can be considered given co-author and tribal approvals.
Consent for publication and ethical approval
We confirm that Ethical Committee approval was sought where necessary and is acknowledged within the text of the submitted manuscript. We confirm that guidelines on patient consent have been met and any details of informed consent obtained are indicated within the text of the submitted manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This project was supported by the Gretchen Swanson Center for Nutrition and the Stephenson Cancer Center at the University of Oklahoma Health Sciences Center, as well as the University of Oklahoma Health Sciences Center, Department of Nutritional Sciences.