
Abstract
Introduction
Cardiovascular disease (CVD) remains the leading cause of morbidity and mortality worldwide (Wong, 2014). Coronary artery disease (CAD) accounts for the greatest proportion of CVD and atherosclerosis has a major role in the pathogenesis of CAD. Dyslipidemia is a major risk factor for CAD and its treatment can reduce coronary lesions progression and cardiovascular mortality. The change in serum level of low-density lipoprotein-cholesterol (LDL-C), as well as, total cholesterol (TC) to high-density lipoprotein-cholesterol (HDL-C) (TC/HDL-C) can predict CAD outcomes (Goff et al., 2006). In addition to the classic CVD risk factors such as plasma lipids and lipoproteins concentrations, measuring inflammatory biomarkers is useful for cardiovascular risk assessment and predicting cardiovascular risk (Enriquez and de Lemos, 2010, Zakynthinos and Pappa, 2009). Lipoprotein-associated phospholipase A2 (Lp-PLA2), as a member of the phospholipase A2 family, is produced by inflammatory cells and correlated with cardiovascular risk (Thompson et al., 2010). Lp-PLA2 activity has been associated with a worse prognosis of CAD, ischemic stroke, and vascular mortality (Zalewski and Macphee, 2005). A higher level of Lp-PLA2 activity may imply a worse cardiovascular prognosis in high-risk patients referred to coronary angiography (Maiolino et al., 2012).
It is believed that most of the burden of CVD can be prevented through a healthy lifestyle, including a healthy dietary pattern (Martinez-Gonzalez and Bes-Rastrollo, 2014). The knowledge that atherosclerosis is an inflammatory disease, has stimulated research on the effects of functional foods and diets with potential anti-inflammatory properties to reduce CAD risk. Dietary supplementation with functional foods such as flaxseed may provide more beneficial effects regarding cardiovascular risk factors. Flaxseed (Linum usitassimum) is the richest plant source of alpha-linolenic acid (ALA) and lignans and the results of interventional studies have shown some favorable effects of flaxseed consumption on CVD risk factors (Edel et al., 2015, Khandouzi et al., 2019, Djousse et al., 2003).
Dietary changes are considered to be the main shaper of the intestinal microbiota composition (David et al., 2014). However, few studies have evaluated the impact of flaxseed consumption on gut microbiota composition (Lampe et al., 2019). In addition to their effect on gastrointestinal health, the gut microbiota has been linked to physiological processes that affect several health conditions and diseases, including cardiovascular disease (Jie et al., 2017).
Some of the previous studies have shown some effects on plasma lipids and lipoproteins following flaxseed consumption (Mandasescu et al., 2005, Khalatbari Soltani et al., 2013, Saxena and Katare, 2014), but the effect on Lp-PLA2 activity has not been studied. Furthermore, the effects of dietary flaxseed on plasma levels of lipids and lipoproteins in patients with cardiovascular disease, already on lipid-lowering medication may be different from the response observed in healthy subjects or those only presenting with risk factors. In our previous study (IRCT2017040328742N2), consumption of dietary flaxseed in a patient population with CAD was associated with improved endothelial function and plasma inflammatory markers (Khandouzi et al., 2019). As a secondary analysis of the same trial, in this study, the effects of dietary flaxseed on plasma lipids and lipoprotein, as well as the relative abundance of some gut microbiota were examined.
Methods
Study design, subjects, and treatments
The current report is a follow-up to a previously conducted trial (IRCT2017040328742N2). The details for the study design were previously described (Khandouzi et al., 2019). Herein, outcomes related to the effects of flaxseed consumption on plasma lipids and the gut bacteria were assessed. Briefly, this was a randomized, controlled, two-arm clinical trial. Study subjects were selected from patients who underwent percutaneous coronary intervention. Participants were randomly assigned to one of the two groups. To achieve a balanced distribution in terms of the age of patients as well as the number of diabetic patients in each of the study groups, stratified block randomization was used (stratification based on age and history of diabetes). The study duration was 12 weeks. The inclusion criteria were BMI<30 kg/m2; aged 20–75 years; non-smoker, not suffering from advanced renal disease. None of the subjects had taken antibiotics, dietary antioxidant supplements, flaxseed, or omega-3 supplements during the previous 1 month before the start of the study. Exclusion criteria were consuming <80% of flaxseed delivered to the patients, any changes in the disease treatment plan, including type or dose of lipid-lowering medications, any use of antioxidants supplements, and any allergic reaction to flaxseed consumption. The control group received dietary advice to include at least five servings of fruits and vegetables in their daily diet and to choose foods containing lower saturated fats and cholesterol. The flaxseed group, in addition to the above dietary recommendation, was supplemented with 30 gr of flaxseed daily. Flaxseed was purchased from the local market and was delivered to the subjects. The participants were asked to powder flaxseed before use and store it in closed packages in the refrigerator after powdering. The study was in adherence to the 1964 Declaration of Helsinki. The study was approved by the National Nutrition and Food Technology Research Institute Ethics Committee and written informed consent was obtained from all patients before the study. Dietary intake and physical activity level were monitored during the study.
Biochemical assays
Venous blood was obtained from each patient, after 12 h overnight fasting and collected into heparinized tubes at the beginning and the end of the study. The platelet-free plasma was separated by centrifugation (4000 rpm for 20 min) and stored at −80°C for later biochemical analysis. Lipid profile was analyzed with the colorimetry method by auto-analyzer Selectra 2 (Vital Scientific, Spankeren, The Netherlands), using commercial kits (Pars Azmoon, Iran). Measurement of small dense (sd) Low-Density Lipoprotein cholesterol (sd-LDL-C) consists of two steps: first, to precipitate the lipoproteins of density <1.044 g/mL using heparin-magnesium; and second, to measure LDL-C in the supernatant by an enzymatic assay (Hirano et al., 2003). Plasma Lp-PLA2 activity was analyzed by a commercial colorimetric assay kit (Cayman Chemical, Ann Arbor, MI, USA).
Fecal sample collection and analysis
Fecal samples were collected at baseline and after 12 weeks of dietary intervention periods and stored at − 20°C until extraction. For DNA extraction, each frozen stool sample was pulverized and homogenized by using a small blade grinder, and a 200 mg pulverized sample was used for DNA extraction. The grinder was cleaned using water and ethanol after each fecal sample was processed. Total microbial DNA was extracted from all stool specimens using the QIAamp DNA Stool Mini Kit (QIAGEN, Hilden, Germany) according to the manufactureŕs protocol. DNA quality and concentration were determined by Nanodrop (Nanodrop Technologies, USA). After extraction, extracted DNAs were immediately frozen at − 20°C until analysis.
For each sample, the levels of total bacteria and Lactobacillus, Bifidobacteria, Bacteroidetes, Firmicutes were estimated from fecal DNA by quantitative real-time polymerase chain reaction (qPCR) by using primers targeting 16S ribosomal DNA of bacteria. The primers used in the present study have been tested previously (Gorzelak et al., 2015) (Table 1). The amplification reactions were carried out with template DNA, the corresponding forward and reverse primer (1 µL of each), and 10 µL SYBR green mix (Ampliqon; Odense, Denmark) in a total volume of 20 µL. Parallel analysis of non-template controls (water) was also included. All reactions were performed on a Step-one plus system (Applied Biosystems, Inc., Foster City, CA) followed by melt curve generation for assessing amplicon specificity. The relative abundances of the 4 different bacterial genera were obtained by normalizing the Ct values of each bacteria for the Ct values of total bacterial (ΔCt values = Ct target bacteria − Ct total bacteria).
List of primers used in this study.
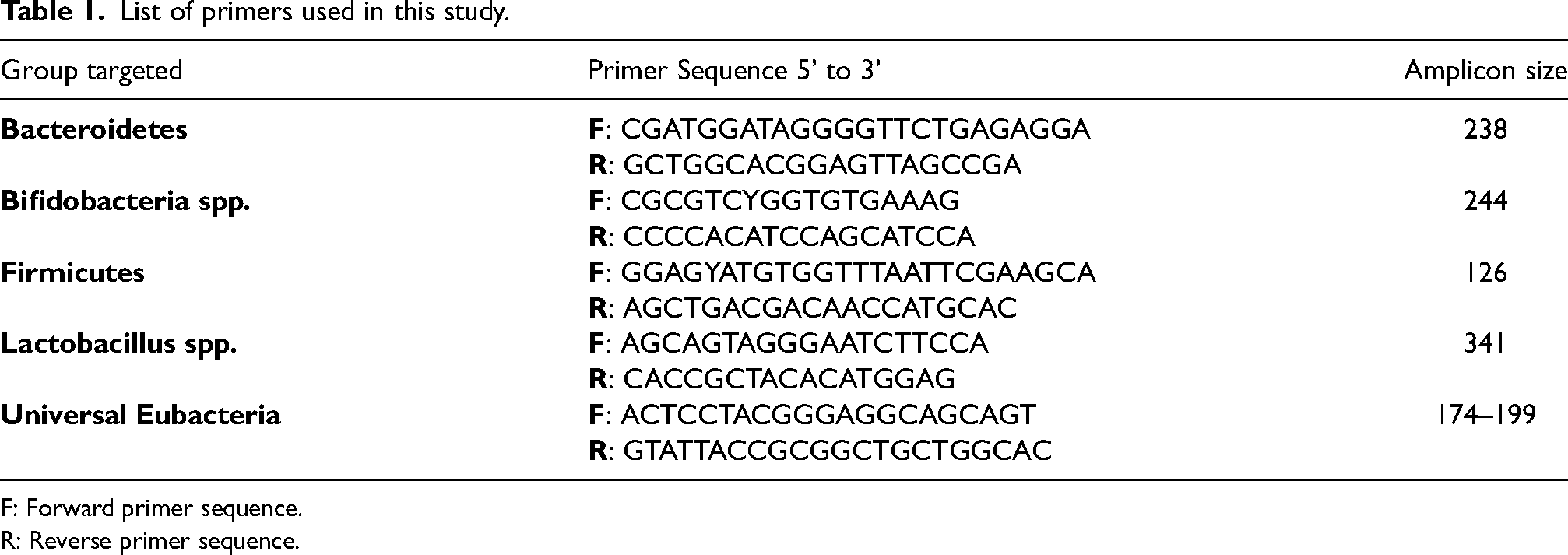
F: Forward primer sequence.
R: Reverse primer sequence.
Statistical analysis
In the original study, the sample size was determined based upon flow-mediated dilation as the primary outcome variable, considering type I error (α) of 0.05, an independent t-test indicated that enrolment of 23 subjects will provide 80% power (1–β = 0.80) to detect 5% difference of magnitude between the two groups, which was increased to n = 25/group to account for a 10% dropout rate. Data were analyzed with SPSS for Windows (version 21.0, SPSS Inc., Chicago, IL). The per-protocol analysis was performed (i.e. only those who completed the study were included in the analyses). Data normality was determined by Shapiro–Wilk test All values were reported as Mean ± SD unless otherwise mentioned. When the variables were not normally distributed, raw values were log-transformed. Analysis of covariance (ANCOVA) was used to compare the 12-week values between the groups using the baseline measures and body weight as the covariates. Paired samples t–test was used for comparing the measurements in the beginning and at the end of the intervention within the study groups. The statistical significance level was set at p < 0.05 (two tails).
Results
Fifty patients were randomized to each of the two groups of intervention and control (n = 25 in each group). The 21 subjects in the flaxseed and 23 in the control group completed the study (Figure 1). Participants’ baseline characteristics were similar between the two groups. The mean age and BMI were 56.67 ± 7.44 and 56.22 ± 9.02 years, and 26.55 ± 2.58 and 26.75 ± 2.37 kg/m2 in flaxseed and control groups, respectively. In the flaxseed group, 16 participants, and in the control group, 21 participants were male. Statins, aspirin, angiotensin-converting enzyme inhibitors (ACEIs) / Angiotensin receptor blockers (ARBs), and clopidogrel were prescribed to all patients. Eight patients in the flaxseed group and 9 patients in the control group had type 2 diabetes. All diabetic patients were treated with oral hypoglycemic drugs and none received exogenous insulin. Baseline body weight was 77.04 ± 10.09 and 75.26 ± 8.35 kg in flaxseed and control groups, respectively. There were no significant differences between the two groups in body weight and physical activity after 12 weeks of study. There were no differences in daily dietary intakes (energy and macronutrients) between the two groups at the baseline. After 12 weeks, calorie intake in the flaxseed group (1938.85 ± 173.80) was higher than in the control group (1764.43 ± 170.75) (p < 0.05). Furthermore, the percentage of calorie intake from carbohydrates was lower in the flaxseed group than the control group (p < 0.05) (51.91 ± 1.01% and 54.52 ± 1.57% in the flaxseed and control groups, respectively), whereas, the percentage of calorie intake from total fat, as well as monounsaturated fat and polyunsaturated fat, was higher in the flaxseed group than in the control group. At the end of the study, omega-3 intake was increased in the flaxseed group (153.05 ± 97.35 mg/day at baseline to 6098.09 ± 75.75 mg/day) compared to the control group (175.74 ± 124.44 mg/day at baseline to 136.87 ± 111.70 g/day). Total fiber intake was increased in the flaxseed group after 12 weeks (17.81 ± 2.63 at baseline to 26.09 ± 3.36 g/day, and 17.26 ± 2.32 at baseline to 16.87 ± 2.75 g/day in the flaxseed and control groups, respectively) (Khandouzi et al., 2019).
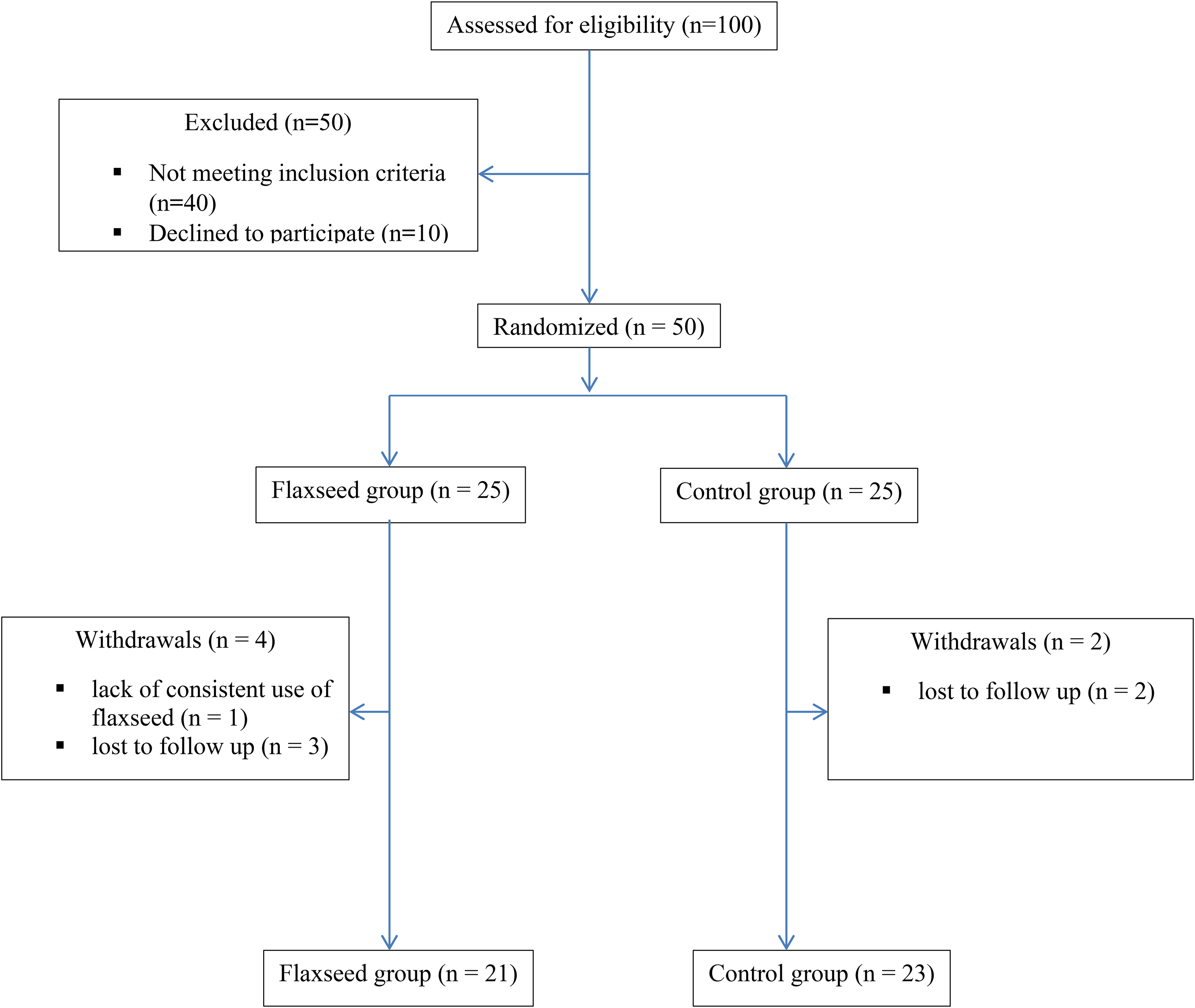
The consort flowchart of the study.
There were no significant differences in plasma levels of TG, TC, HDL-C, LDL-C, sd-LDL-C, or TC/HDL-C between the two groups at the baseline and after 12-week. Of the 44 patients who completed the study, only 3 patients had the baseline LDL-C >100 mg/dL whereas 20 patients had TG> 150 mg/dL. Sub-analysis among patients with TG>150 mg/dL did not show a significant difference between the two groups at the end of the study.
Comparison of Lp-PLA2 activity between the two groups showed that in the group consuming flaxseed, Lp-PLA2 activity was significantly lower than the control group. (p = 0.04) (Table 2).
Measures of biochemical variables by intervention groups a .
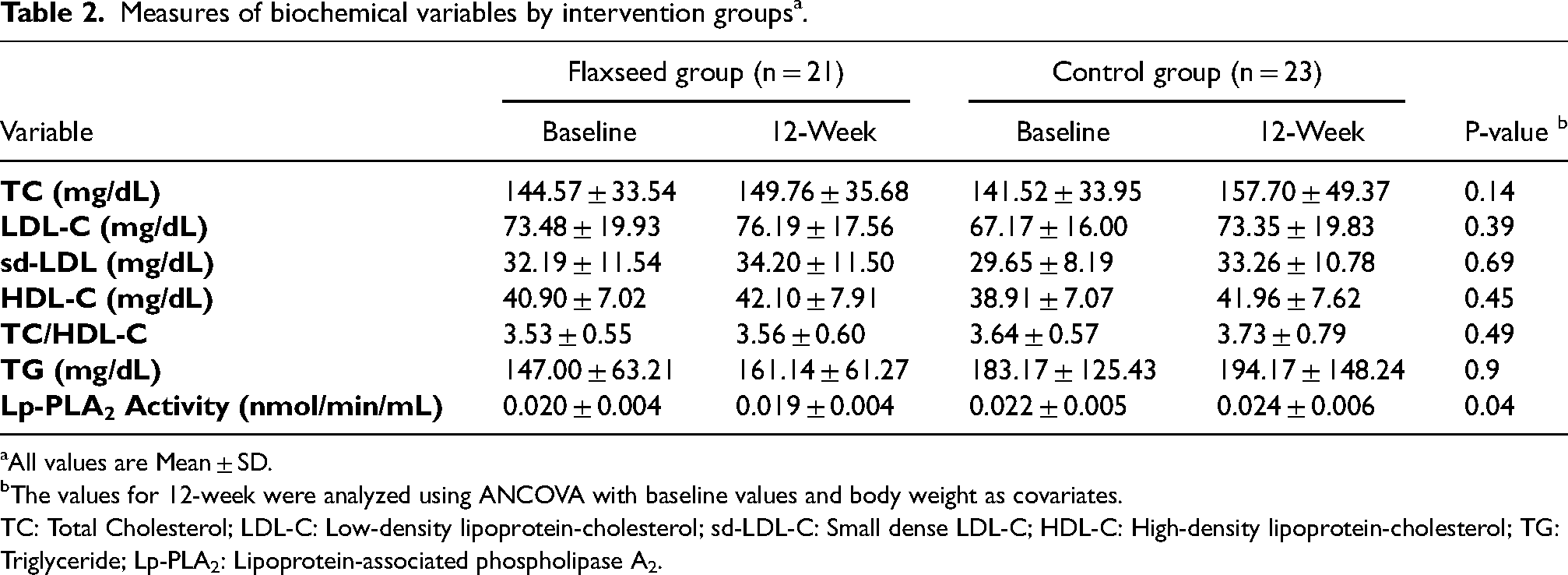
All values are Mean ± SD.
The values for 12-week were analyzed using ANCOVA with baseline values and body weight as covariates.
TC: Total Cholesterol; LDL-C: Low-density lipoprotein-cholesterol; sd-LDL-C: Small dense LDL-C; HDL-C: High-density lipoprotein-cholesterol; TG: Triglyceride; Lp-PLA2: Lipoprotein-associated phospholipase A2.
Flaxseed consumption had no significant effect on gut microbial composition and no statistically significant differences were found in the fecal abundance of the Lactobacillus, Bifidobacteria, Bacteroidetes, Firmicutes between the groups (Figure 2). Despite the apparent difference in the ratio of Firmicutes/Bacteroidetes between the two groups (−0.035 ± 1.54 vs. −1.53 ± 5.10 in the intervention and control groups, respectively), this difference was not statistically significant (p = 0.11).
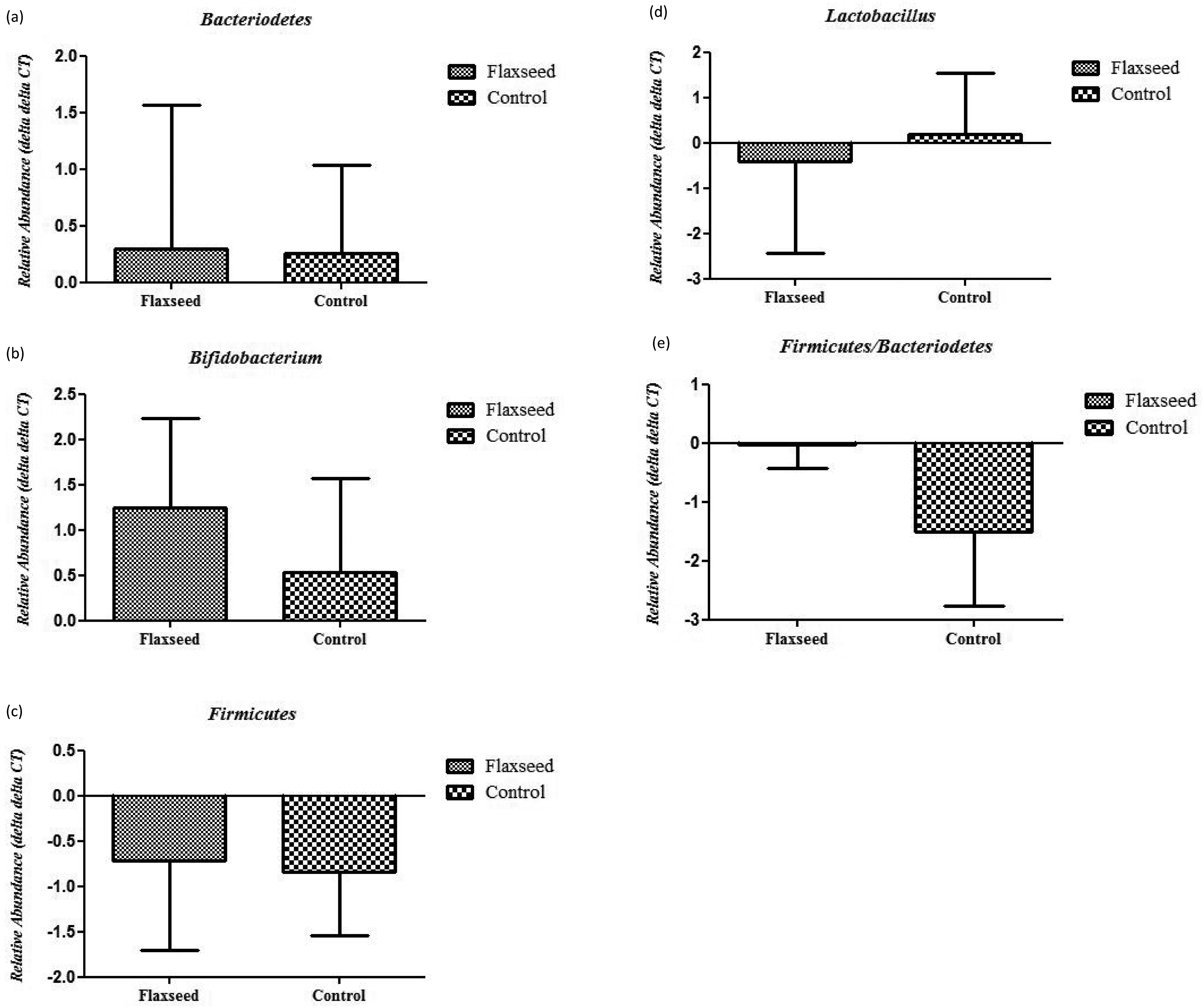
Changes in relative abundances of Bacteroidetes (a), Bifidobacterium (b), Firmicutes (c), Lactobacillus (d), or Firmicutes /Bacteroidetes ratio (e) in stool isolated from study subjects. Data are mean ± standard error. The relative abundances were calculated normalizing the Ct values of each bacterium for the Ct values of total bacterial (ΔCt values = Ct target bacteria − Ct total bacteria). Fold changes in the abundance of bacteria were calculated as the differences between ΔCts values at baseline and ΔCts values at 12-week. Higher values indicate a higher abundance.
Discussion
In the present study, the effects of dietary flaxseed supplementation were evaluated in CAD patients. The results of the current study on patients with CAD on stable medications showed that flaxseed supplementation for 12 weeks reduces plasma Lp-PLA2 activity but was not effective in improving plasma lipids and has no effect on the relative abundance of the studied fecal microbial community.
Lp-PLA2 belongs to the family of structurally diverse phospholipase A2 enzymes, also known as platelet-activating factor acetylhydrolase (PAF-AH). The higher Lp-PLA2 activity has been associated with an increased CVD risk in individuals with or without baseline subclinical CVD (Garg et al., 2015). In the current study, the observed decrease in Lp-PLA2 activity level following flaxseed consumption may be related to the flaxseed n-3 fatty acid content. Flaxseed is a good source of the plant-derived n-3 fatty acid ALA, as the major component (Bloedon and Szapary, 2004, Prasad, 2009, Rahimlou et al., 2019). No previous study has investigated the effect of flaxseed on Lp-PLA2 activity in patients with CAD. However, in participants of the Multi-Ethnic Study of Atherosclerosis, plasma Lp-PLA2 activity was significantly lower in those with the higher plasma eicosapentaenoic acid and docosahexaenoic acid (Steffen et al., 2013). The evidence from intervention trials for the influence of n-3 polyunsaturated fatty acids (PUFAs) on the Lp-PLA2 activity level is equivocal. Nelson et al. showed that supplementation with n-3 fatty acids capsules (11 g/day of flaxseed oil or 2 g/day of fish oil) over 8 weeks had no significant effect on plasma Lp-PLA2 activity in healthy adults (Nelson et al., 2011). In contrast, Gajos et al. reported that administration of omega-3 PUFA (1 g/day) for 4 weeks decreased Lp-PLA2 activity in stable CAD patients undergoing percutaneous coronary intervention (Gajos et al., 2014). This discrepancy may be related to different study populations since, in the study by Gajos et al., high-risk patients with severe atherosclerosis were included. In addition to the possible effects of omega-3 fatty acids of flaxseed, its lignans may have also contributed to reducing the activity of Lp-PLA2. Oral administration of lignans (from sesame) has reduced the plasma PAF-AH activity in rabbits (Nakamura et al., 2020).
The lack of significant change in LDC-C or TC / HDL-C concentration in the current study could be due to the low baseline plasma LDL-C levels of the study subjects. Participants of the present study had an optimum level of LDL-C due to statin therapy. The beneficial effects of flaxseed on plasma lipid profile may be more evident in patients whose plasma lipids are high at baseline. In patients treated with statins, or in those with normal baseline lipid levels, flaxseed had no significant or a limited effect on the levels of plasma lipids (Dodin et al., 2008, Faintuch et al., 2011). However, in dyslipidemic patients, or those with cardiovascular risk factors that have not been treated with lipid-lowering medications, flaxseed has been shown to reduce plasma lipid levels (Mandasescu et al., 2005, Saxena and Katare, 2014, Khalatbari Soltani et al., 2013). In addition, the amount of flaxseed supplementation required to reduce plasma lipid levels may be more than 30 g/d. Daily consumption of 40 g/d of ground whole flaxseed has been suggested to reduce blood cholesterol (Liperoti et al., 2017).
There is very little documentation on the influence of flaxseed consumption on the fecal microbial community. In the present study, flaxseed consumption did not have an effect on the fecal microbial composition. In healthy adults, flaxseed lignan supplementation (50 mg/d) had no significant effect on fecal microbial community composition as well as on individual genera (14). Furthermore, the addition of extruded flaxseed to the feed of pigs over 51 days had no measurable impact on the fecal bacterial community (36). In contrast to our finding, some animal studies have shown that the addition of flaxseed or the ingredients present in flaxseed to the animal's diet has favorable effects on gut microbial composition (Badger et al., 2021, Zhu et al., 2020, Yang et al., 2020). Oral administration of synthetic lignan naturally present in flaxseed has decreased Firmicutes/Bacteroidetes ratio, which is generally associated with lower intestinal and systemic inflammation, and also decreased abundance of Bifidobacterium, which is considered to be both anti-inflammatory and probiotic (Badger et al., 2021). Further, administration of flaxseed polysaccharides to mice fed with a high-fat diet did not affect the relative abundance of Bacteroidetes, but it significantly reduced the relative abundance of Firmicutes, thus significantly decreasing the Firmicutes/Bacteroidetes ratio and increased abundance of Bifidobacterium (Yang et al., 2020). High-fat extra-virgin olive oil or high-fat flaxseed oil-fed mice showed a lower abundance of the Firmicutes phylum in comparison with high-fat-fed mice (Millman and Okamoto, 2020). Moreover, 6 weeks treatment of alcoholic liver disease model of mice with flaxseed oil had a limited effect on Bacteriodetes and Firmicutes (Wang et al., 2017).
The present study had some limitations. The study population was relatively small. Furthermore, there was also no blinding of participants. Moreover, the abundance of a limited number of gut microbiota components was examined and the diversity of bacteria was not determined. This study also had some strengths, including good compliance with supplemental flaxseed.
In conclusion, the present study showed that in patients with CAD, flaxseed supplementation reduced plasma Lp-PLA2 activity but had no effect on plasma lipids and the composition of some intestinal bacteria. Since plasma Lp-PLA2 activity is an independent predictor of cardiovascular events (Zalewski and Macphee, 2005), its improvement may be effective in reducing the risk in CAD patients.
Footnotes
Acknowledgements
The study was supported by the National Nutrition and Food Technology Research Institute, Shahid Beheshti University of Medical Sciences, Tehran, Iran. We are grateful to the volunteers who participated in the study.
Availability of data and materials
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Authors’ Contribution
Nafiseh Khandouzi was responsible for designing the research protocol, writing the protocol, conducting the research, screening potentially eligible studies, conducting biochemical tests, extracting and analyzing data, interpreting results, and writing the paper.
Javad Nasrollahzadeh was responsible for designing and writing the research protocol and screening potentially eligible studies. He contributed to extracting and analyzing data, interpreting results, and writing the paper.
Ali Zahedmehr & Ata Firoozi assisted in conducting the research, especially in medical consultation & material support, and study supervision.
Consent for publication
The authors declare that any person named as co-author of the contribution is aware of the fact and has agreed to be so named. All of the authors give their consent for the publication of details within the text to be published in the above journal and article. Authors provide formal signed written consent to publish before the publication of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the National Nutrition and Food Technology Research Institute Ethics Committee and written informed consent was obtained from all patients before the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Nutrition and Food Technology Research Institute, (grant number 652).