
Abstract
Keywords
Introduction
In the grand scheme of things, micronutrients assist in bringing a positive outcome of pregnancy. When there is a deficient intake of specific nutrients, pregnancy is under the risk of complications (Gernand et al., 2016). A micronutrient deficiency could be the result of imbalanced diets, limited dietary intake, or reduced intestinal absorption. A range of complications that could arise from a restricted micronutrient intake includes pre-eclampsia, gestational hypertension, anemia, intrauterine growth restriction (IUGR), and preterm birth, which can predict morbidity and mortality for mother and child (Hovdenak and Haram, 2012). Both inadequate intake and excessive intake have a negative impact on pregnancy. Both the consequences of overnutrition and undernutrition affect mothers and their children in the short-term and long-term (Villar et al., 2006).
The manner of nutrient consumption as well as an obesogenic environment can alter fetus development in terms of metabolic changes permanently. These changes increase the likelihood of metabolism-related diseases during childhood and adulthood. While it may be difficult to identify the underlying cause of many of these diseases, numerous researches is drawing a connection between pregnancy complications and the likelihood of developing diseases throughout childhood and adulthood (Neiger, 2017). Dietary intake of poor quality results in an inadequate intake of several micro and macronutrients and in turn having a drastic impact on the pregnancy, its outcomes, and the health of the fetus. While the best approach to a sufficient intake of vitamins and minerals is a balanced diet, it remains difficult to cover all vitamin and mineral requirements. When it becomes notably challenging for pregnant women to achieve an adequate intake of micronutrients, it may be necessary to introduce vitamin supplements to meet the increased nutritional requirements of pregnancy (Mousa et al., 2019).
Macronutrients
Macronutrients refer to nutrients that the body requires in large amounts in order to carry out basic functions and obtain calories or energy. Macronutrients include carbohydrates, proteins, and fat (Solon-Biet et al., 2014).
Carbohydrate and fibers
During pregnancy, carbohydrate and fiber intake become a critical source of energy and their intake is typically amplified during this period. The carbohydrate content that women need during pregnancy is 175 g/day, where 28 g/day of this content constitutes fiber (Pretorius and Palmer, 2021).
Protein
The fetus unit utilizes around 1000 grams of protein during pregnancy in the last two trimesters. According to the National Academy of Medicine, it is recommended for pregnant women to increase their protein intake to 1.1 g/kg/day to meet the requirements of the pregnant body (Kominiarek and Rajan, 2016). This intake limit is 0.3 g/kg/day more than the expected requirements for non-pregnant women. While protein is essential, higher intake typically from supplements can have adverse effects on the pregnancy (Mark et al., 1990).
Fat
Intake of varying types of fat and quantities of those fats consumed during pregnancy has been linked to birth weight small for gestational age (SGA), and neurodevelopment variations. For instance, high intake of dietary fat in early pregnancy is associated with increased birth weight and reduced risk of SGA (Abu-Saad and Fraser, 2010)
Micronutrients
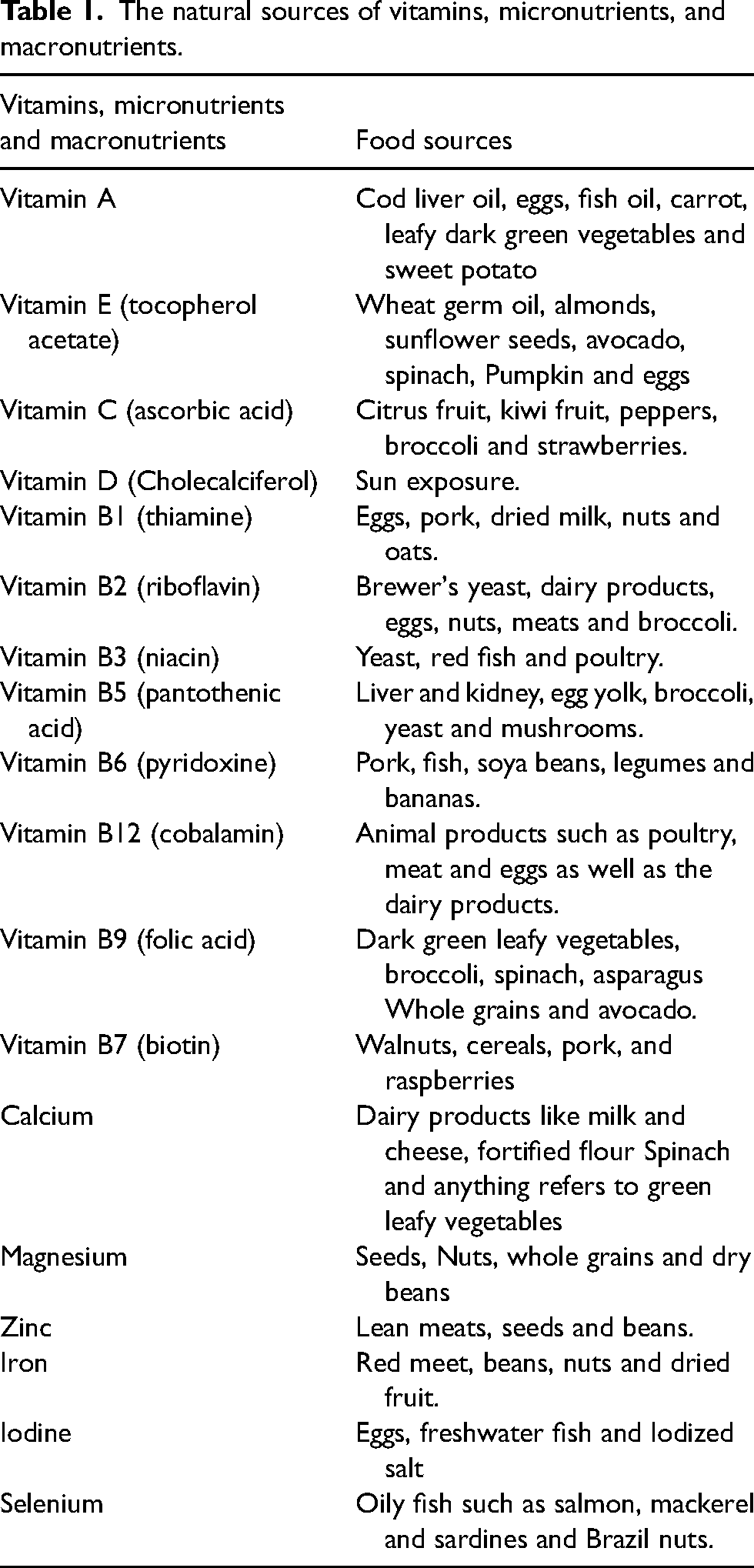
Micronutrients are dietary elements that the body needs in small amounts to function properly. Micronutrients are a category that includes vitamins and minerals. Table 1 summarizes the food sources that these vitamins could be collected from.
The natural sources of vitamins, micronutrients, and macronutrients.
Calcium
Because of its role in developing the fetus's bone structure, it is recommended for pregnant women to meet the requirements for their calcium intake and for the body to utilize calcium, vitamin D is essential. For pregnant women between the ages of 19 to 50 or lactating women, the elemental calcium Recommended Dietary Allowance (RDA) is 1000 mg/day and 1300 mg for girls between the ages of 14 to 18 (Garner and Post, 2017). For healthy pregnant women who meet the dietary calcium intake, the use of calcium supplementation will not reduce any potential neonatal risks (Buppasiri et al., 2015). However, there may be benefits to using calcium supplements in populations at high risk of pre-eclampsia. But this statement requires further study to support it provided present evidence is extracted from study populations that are small and diverse (Hofmeyr et al., 2003). Although calcium is important for fetus development, exceeding the limit of intake will have adverse complications such as constipation, kidney stones, impaired absorption of other minerals such as iron and zinc, irregular cardiac rhythm, and low calcium rates in the fetus (Pravina et al., 2013).
Vitamin D
The fat-soluble prohormone vitamin D takes part in fetus development by regulating and encouraging healthy bone mineralization, disease prevention, and immune functions (Basit, 2013). Additionally, vitamin D regulates other micronutrients and their use such as calcium and phosphate. There are many forms of vitamin D, but only two are required by the human body for development: ergocalciferol (D2) and cholecalciferol (D3). Sun exposure is the most important and natural source of vitamin D, since the skin synthesizes the derivate of the steroid cholesterol into cholecalciferol or D3 (Nair and Maseeh, 2012).
The RDA for vitamin D is 600 international units for all women of reproductive age, including pregnant and lactating women, according to the Institute of Medicine (IOM) (Mark et al., 1990). During pregnancy, the use of vitamin D supplements enhances the vitamin D status of pregnant women which in turn suppresses the risks of pre-eclampsia, low birth weight, and preterm birth (Holick, 2012). However, there is inadequate availability of studies and research conducted to evaluate the benefits and risks of using vitamin D supplements during pregnancy on the health of the mother and the infant. From the evidence available, it has been shown that vitamin D reduces the risk of offspring wheezing by the age of 3 (RR 0.81; 95% CI 0.67–0.98) (Maretzke et al., 2020). Furthermore, low maternal serum vitamin D concentrations are correlated with low levels of the vitamin in infants increasing the risk of several health complications such as detrimental effects on offspring bone and teeth development, and risk of infectious diseases. Although vitamin D is essential for a healthy pregnancy, in excess, it increases the risk of hypercalcemia in the fetus (Larqué et al., 2018).
Folic acid
The body converts vitamin B9, otherwise known as folic acid, to a more usable version referred to as folate. It is highly recommended for women wanting to conceive to begin increasing their intake of folic acid in preparation for conception. Likewise, women are advised to increase their intake of vitamin B9 during gestation. Known to suppress the risks of malformations in fetuses’ primarily neural tube defects, folic acid is critical to the steady growth of the fetus (Czeizel and Bánhidy, 2011). Megaloblastic anemia typically imitates the onset of several symptoms that include fatigue, and gastrointestinal disturbances such as diarrhea, nausea, and vomiting. During the first weeks of embryonic formation, folic acid plays a significant role in the healthy development of the neural tube, as well as the development of the brain and spinal cord. Furthermore, folic acid is a critical factor in the formation process of the heart and circulatory system. According to research, folic acid intake pre-gestation and in the early weeks during pregnancy can drastically suppress the risk of neural tube defect (NTD) (Risk Ratio (RR) 0.31; 95% confidence interval (CI) 0.17–0.58) (Allen, 2000).
As a result, it is advised that women meet the folic acid RDA of 0.6 mg to ensure a healthy development process for both the placenta and the fetus. It is recommended for pregnant women to resume the consumption of folic acid supplements post the first trimester as the termination of its use has been associated with a decrease in serum folate and a contrasting increase in homocysteine concentrations (Gindler et al., 2001). It should be noted that despite being beneficial in moderation, excess concentrations of folic acid increase the risk of insulin resistance and impaired brain development in the fetus (McNulty et al., 2013).
Iron
Iron is an element that is demanded by proteins relevant to cellular functions including transportation of oxygen, DNA synthesis, and anti-oxidant defenses. To achieve a healthy pregnancy, intake of iron supplements becomes critical to governing essential health-related processes. Where a reduced consumption of iron has been associated with adverse pregnancy outcomes, and a rise in perinatal mortality and morbidity (Kempenaar and Darwent, 2013). According to the evidence obtained from numerous studies, it is highly advisable for pregnant women to meet their iron intake requirements for healthy fetus development. Iron supplementation has been found to reduce the risk of low birth weight and anemia (Mahomed, 2000). Clinicians should also ensure that all pregnant women are tested for their ferritin and hemoglobin. According to experts, pregnant women should raise their consumption of iron by around 15 mg/day, thus increasing the total consumption of iron to about 30 mg/day as recommended by the Centers for Disease Control (CDC) (CDC, 1998). This limit is set to ensure that upon its fulfillment, several iron-related complications during pregnancy such as anemia subsided. A vast majority of vitamin supplements meet this limit making them ideal for non-anemic women (National Diabetes Data Group, 1979). While iron consumption is in fact necessary, overdosing on iron initiates the onset of several complications, such as glucose intolerance and Gestational diabetes mellitus (GDM) (Keen and Gershwin, 1990).
Zinc
In the body, zinc is found in exceptionally scarce amounts hence referred to as a trace element. Despite being available in sparse amounts, zinc plays a monumental factor in cellular processes and general tissue physiology. Abundant research indicates that drastic deficiencies of the zinc element are prone to initiating growth restriction (Jameson, 1993). Observational studies found that ideal consumption of the element of zinc had a direct link to increasing birth weight (CDC, 1998). A systematic review, namely one established in 2015, of 21 randomized trials concluded that zinc supplementation or the lack of it during pregnancy had, aside from a 14% decline in preterm birth among low-income women, little to no impact on the outcome of the pregnancy. It is essential however to avoid excessive consumption of zinc as it could lead to vomiting, nausea, diarrhea, or stomach aches (Ota et al., 2015).
Vitamin C
Ascorbic acid, otherwise known as vitamin C, is an essential component in the formation of fetus connective tissue and collagen, as well as enhancing the performance of the immune system (Walingo, 2005). However, it has little to no effect on reducing the risk of stillbirth, preeclampsia, and low birth weight. Moderation is key when consuming vitamin C for pregnant women. Although it has several benefits for the mother and fetus, excess vitamin C can cause several side effects, including an increased risk of preterm birth and gastrointestinal disturbances during pregnancy (Kiondo et al., 2014).
Vitamin E
Vitamin E is the most important lipophilic, radical-scavenging antioxidant, protecting humans from oxidative stress caused by active oxygen and nitrogen species (Niki and Noguchi, 2004). Oxidative damage that affects the DNA, proteins, and lipids is linked to low birth weight, preeclampsia, and preterm delivery. Whereas its role in the reduction of adverse complications such as stillbirths, preterm birth, preeclampsia, or low birth weight is little to none (Rumbold et al., 2015). Excessive intake of vitamin E by pregnant women is linked to a decline in birth weight.
Vitamin A
Functions of vitamin A are associated with regulation of the cell cycle, development and growth of fetus organs and skeletal system, and supporting the immune system as well as the healthy development of fetus vision besides preserving the health of maternal vision (WHO, 2012). Pregnant women must fulfill the slight increase in vitamin A requirements post conception. Non-pregnant women should typically consume the RDA of 2640 international units, but after conceiving, it is ideal to raise the limit to 3300 international units. Excessive amounts of vitamin A give a teratogen trait, causing it to adversely impact the development of the fetus (LASCHINSKI and SPIELMANN, 1988) Despite the toxic effects of vitamin A on the fetus, it is still essential for pregnant women to take the right amounts daily. In the case of a drastic absence of vitamin A in the body, it is important for pregnant women to steer away from formulations that contain 5000 international units of the vitamin. On the other hand, formulations with more than 10,000 international units of vitamin A are very averse to the development of the fetus as the element appears to have teratogenicity tendencies at the given concentration (Dibley and Jeacocke, 2001).
Iodine
Iodine is an element that plays a critical role in developing a set of organs and functions in the body and these include the thyroid and neurological functions. The absence of iodine in the body in concentrations that meet the requirements of a deficiency has extremely adverse effects on fetus development, where it could increase the risk of both maternal and fetus hypothyroidism (Sahay and Nagesh, 2012).
According to the National Academy of Medicine, it is advisable for pregnant women to consume no less than 0.21 mg of iodine, and breastfeeding women to increase their intake of iodine to 0.29 mg. Whereas The World Health Organization (WHO) advises that both pregnant and breastfeeding women should keep their iron intake at 0.25 mg (WHO, 2016). Because iodine influences the development of the thyroid, having it in excess could lead to fetus goiter. The occurrence of fetus hypothyroidism has been seen in women consuming around 12.5 mg, 3.2 mg, and 2.3 mg of iodine per day (Nishiyama et al., 2004).
Use of multivitamins in pregnancy
During pregnancy, it becomes critically essential for women to consume adequate amounts of minerals and vitamins for their health and the health of the embryo and its development. However, and despite the imperative role of sufficient vitamin intake during pregnancy, not all women are capable of following a balanced diet during these times. As an attempt to resolve the issue of micronutrient deficiencies, many women resort to the use of multivitamins, ones often made for pregnant women. However, despite the widespread belief that the consumption of vitamins pre or during pregnancy is beneficial for the health of the mother or the embryo, there is a jarring lack of evidence established to support the benefits of using multivitamin supplements during this period (Sullivan et al., 2009). While supplementing may prevent micronutrient deficiencies, they tend to provide minerals and vitamins in amounts that exceed the necessary. Recommending the use of multivitamin supplements for women who are pregnant or considering getting pregnant varies from one source to another (Hemminger and Wills, 2020). For instance, the IOM and WHO suggest that multivitamin supplements are best recommended for expecting mothers with poor diets, vegetarians, cigarette smokers, and those who consume alcohol. Whereas other sources recommend that multi-vitamin supplements should be used by all women of childbearing age (Picciano and McGuire, 2009)
The review aims to compare the Daily Recommended Dietary Allowance of each vitamin, micronutrient, and macronutrient with the doses available in a sample of products found in Turkish markets, whether imported or manufactured in Turkey.
Risks of excess micronutrient intake from prenatal vitamins
Excessive micronutrient consumption has a number of negative health impacts, depending on the amount and duration. These negative consequences vary from modest occurrences to poisoning. The majority of high-dose vitamin ingestion may be kept under control if reported quickly. However, for several micronutrients, such as vitamin A and zinc, a limited margin exists between the RDA and the tolerated upper intake level (UL), which may result in significant deleterious effects, as previously described (Pike and Zlotkin, 2019). Despite some vitamin brands providing higher doses of select vitamins than the Recommended Dietary Allowance that is ideally recommended, they don't exceed the tolerable upper intake level (UL) making them safe for use. The upper intake level is the maximum dose at which no adverse effects occur. By exceeding the upper intake level (UL) pregnant women usually suffer from adverse effects having a negative impact on the mother and her baby's health (Sullivan et al., 2009).
Materials and methods
When it becomes notably challenging for pregnant women to achieve an adequate intake of micronutrients, it may be necessary to introduce vitamin supplements to meet the increased nutritional requirements of pregnancy. Detailed information about the recommended doses and the natural dose of these sources has been discussed. The review has built on comparing the Daily Recommended Dietary Allowance of each vitamin, Micronutrient, and Macronutrient provided by the CDC, WHO and IOM with the doses available in a sample of the products found in the Turkish markets. The active ingredients available in each product and their amounts were obtained by using the database provided by the Turkish pharmacist association “Tebrp” as well as RxMediaPharma which is one of the common drug information resources used in the Turkish pharmacies. Elevit® and decavit® were chosen as they are the only two pregnancy vitamins approved by the Turkish ministry of health and covered by social security. A sample of the other products was selected randomly using a computer program as it's difficult to collect and mention all the products available in the Turkish market.
Results
A daily prenatal multivitamin is generally recommended during pregnancy. Table 2 displays the recommended daily intake of vitamin supplements as suggested by the Institute of Medicine for pregnant women.
Daily recommended dietary allowance for vitamins, micronutrients and macronutrients for pregnancy per day.
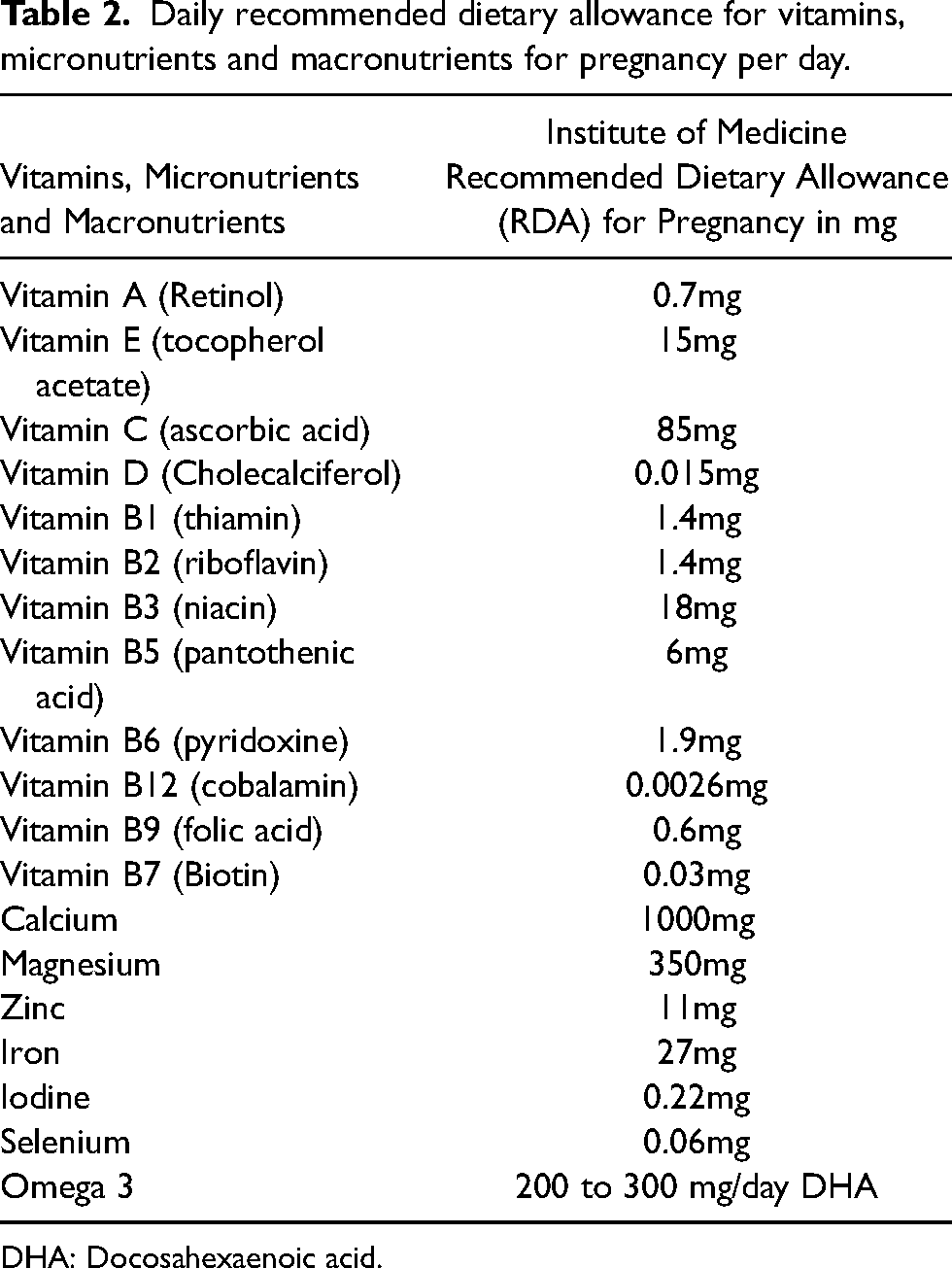
DHA: Docosahexaenoic acid.
The upper intake level is the maximum dose at which no adverse effects occur. Table 3 summarizes the upper intake level of the vitamins according to the US guidelines.
The upper tolerable limit (safety limit) of vitamins, micronutrients and macronutrients in pregnancy per day.
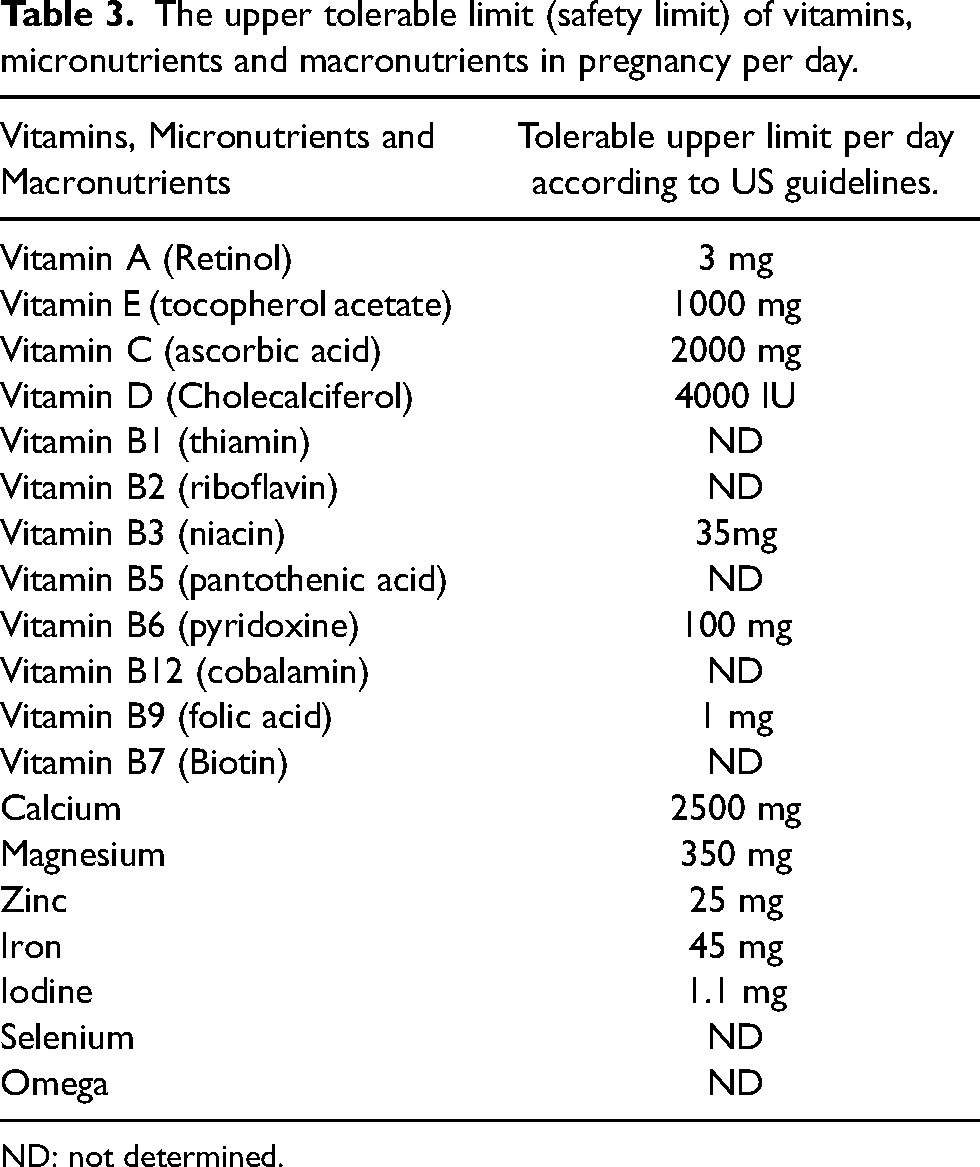
ND: not determined.
The availability of pregnancy multivitamin formulations has sparked an interest in evaluating their efficacy in contributing to a safe pregnancy as well as defining the proper dose value. Table 4 shows the doses of the multivitamin supplements used in this study as it's available in the Turkish markets.
Key micronutrient content of six leading pregnancy multivitamins available in Turkey.
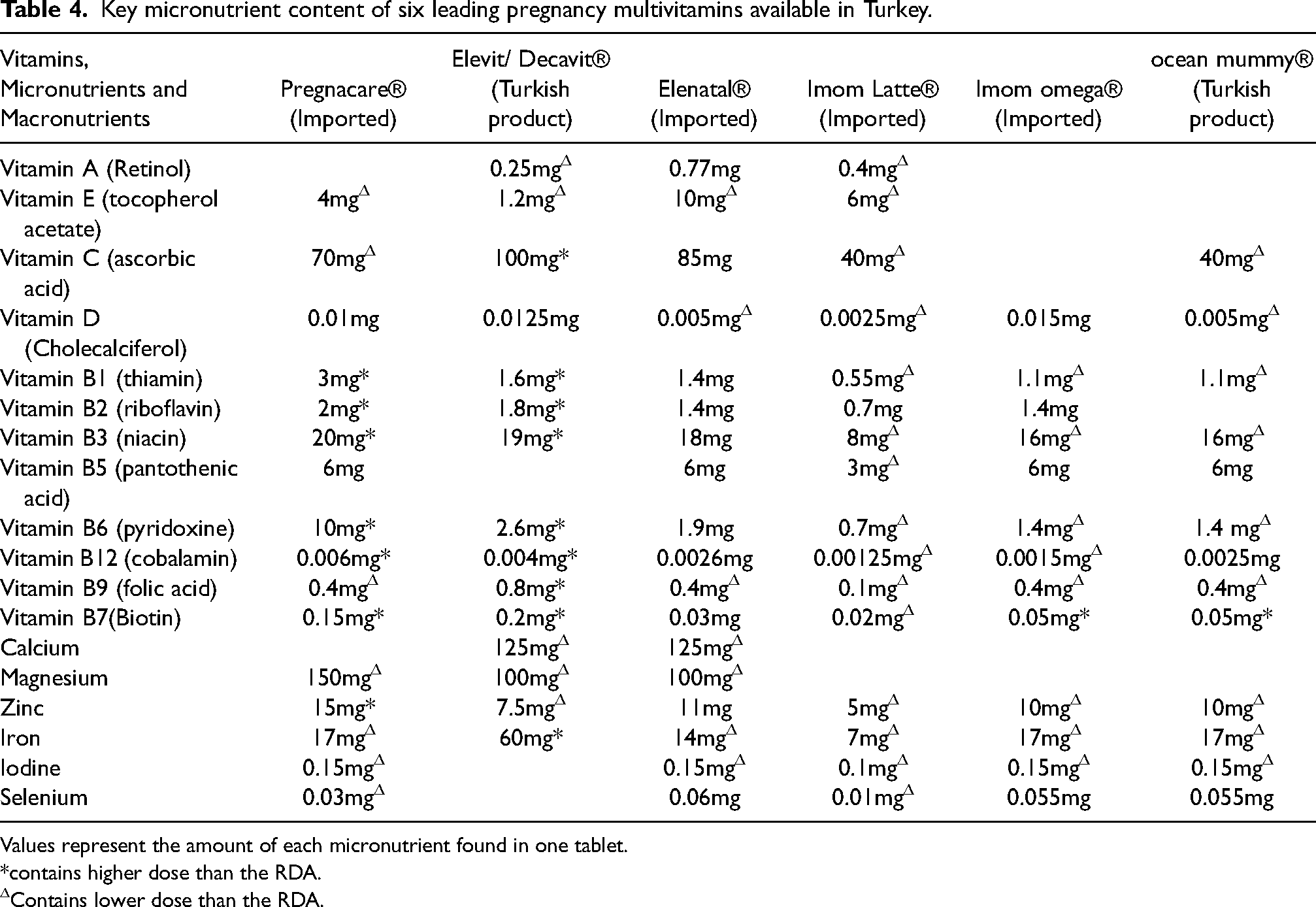
Values represent the amount of each micronutrient found in one tablet.
*contains higher dose than the RDA.
Contains lower dose than the RDA.
Discussion
The IOM and the Centers for Disease Control and Prevention recommend multiple micronutrient supplements, more commonly referred to as multivitamin supplements, for selected pregnant women.
Typically, those recommended to use multivitamins are with iron-deficiency anemia or those who follow poor-quality diets, are vegetarians, cigarette smokers, and those who consume alcohol. The lowest daily doses of supplements could be concentrations of vitamins and minerals that are typically hard to achieve through diet alone during pregnancy. These include the following (Kominiarek and Rajan, 2016):
Iron – 27 mg Folate – at least 0.4 mg (0.6 mg in the second and third trimesters) Calcium – at least 250 mg (elemental calcium 1000 mg/day) Iodine – 0.15 mg (preferably in the form of potassium iodide) Vitamin D – 200 to 600 international units (the exact amount is controversial)
This review mentioned several formulations display higher or lower daily contents of vitamins and minerals than is normally ideal for expecting women as specified by the Recommended Dietary Allowance (RDA). While high doses may have major adverse effects, smaller doses do not always indicate that they will induce a definitive deficiency because a well-balanced diet may be sufficient to meet the daily demands of pregnant women. Formulations that exceed the recommended RDA while remaining underneath the UL range for specific vitamins include Pregnacare®, Decavit®, and Elevit®. The aforementioned formulations incorporate concentrations of vitamin B that exceed the RDA. Yet, despite breaking the RDA, the aforementioned brands remain under the UL range marking them as safe for use. The body would typically deal with the excess of vitamin B by absorbing the necessary concentrations and then excreting the additional concentrations through urine. However, some individuals may show signs of side effects that come in the form of nerve pain in response to the intake of high levels of B6 (Raghavan et al., 2019). As for the role of vitamin B in pregnancy, several randomized studies indicate its benefits in suppressing nausea in expecting women. As a rule of thumb, vitamins and minerals in any given formulation are still safe to use if they exceed the RDA range while remaining underneath the UL. Both formulations by Elevit® and Decavit® indicated the presence of vitamin C in ranges beyond the RDA but far beneath the UL limit. While vitamin C is essential for human development, consuming the vitamin in amounts beyond the UL will have negative impacts such as diarrhea and gastrointestinal disturbances symptoms (Ghaedrahmati et al., 2017).
Other vitamins that if in excess could initiate potential fetus or maternal harm include vitamin A. Being a teratogen, vitamin A doses should be measured carefully and their consumption controlled in pregnant women since the intake of high doses of the vitamin increase the risk of congenital malformations (Pearce et al., 2016). During pregnancy, some vitamins play a more important role in maintaining a healthy fetus development than others. For instance, folic acid has an imperative role in preventing birth defects. The average recommended doses of folic acid that pregnant women should take ranges between 0.4 mg/day to 0.8 mg/day for the first trimester with women at a higher risk of fetus neural tube defects recommended to consume over 4 mg/day (Bortolus et al., 2014).
The American Thyroid Association recommends that women consume multivitamins consisting of 0.15 mg of iodine pre-conception, during pregnancy, and when breastfeeding in the form of potassium iodide. Despite iodine being an essential vitamin during pregnancy, numerous formulations such as Elevit® and Decavit® don't have it in their formula. Much like other vitamins, iodine intake should be monitored during pregnancy as excess intake increase the risk of fetus goiter (Breymann et al., 2010). As for iron, the CDC recommends women to increase or nearly double their iron intake from 15 mg/day to 30 mg/day to prevent anemia. Most of the available prenatal vitamin supplements meet this range and provide sufficient amounts of iron, whereas Elevit® and Decavit® have much more iron amount than the RDA. This high dose may be explained by the World Health Organization (WHO) recommendations that advise the pregnant women to take an elemental iron dose up to 60mg, especially in the countries where anemia is a public health problem. Turkey has a moderate public health problem regarding the prevalence of anemia (Pektaş et al., 2015).
As for vitamin D and calcium, a systemic review indicates that calcium supplements have low to no impact on reducing incidents of low birth weight or spontaneous preterm birth (Buppasiri et al., 2015). However, the studies do display a faint connection between intake of calcium supplements during birth and preeclampsia prevention among populations at high risk. Further studies need to be conducted to confirm the statements. In regard to vitamin D, it has been established that it plays an imperative role in pregnancy, where its intake during pregnancy reduces risks of autism, preeclampsia, and asthma (Agarwal et al., 2018).
In terms of fish oil, which some prenatal vitamin supplements such as Imom Omega® and Ocean Mummy® include, numerous randomized studies show that it decreases the incidents of preterm birth, asthma, and breathing problems in infants. No evidence of harm or side effects associated with the use of marine omega-3 either as supplements or dietary additions has been recorded. DHA, a type of omega-3 fatty acid has been shown to play an essential role in the brain's development and retina in the last trimester of pregnancy. Hence why it's important for expecting mothers to increase their daily intake of omega-3 fatty acids to be between 200 and 300 mg/day (Coletta et al., 2010).
Several formulations display higher or lower daily contents of vitamins and minerals than is normally ideal for expecting women as specified by the Recommended Dietary Allowance (RDA). Formulations that exceed the recommended RDA while remaining underneath the UL range for specific vitamins include Pregnacare®, Decavit®, and Elevit®.
Conclusion
Women should be educated on the benefits of eating a balanced diet consisting of all the essential vitamins and the role of supplements during pregnancy. Everything from fruits to vegetables, proteins, whole grains, and dairy helps expecting mothers to balance their intake of nutrients. Since every pregnant woman will need varying amounts of micronutrients based on age, activity level, weight, and height, it is best for expecting mothers to consult clinicians on their dietary needs during pregnancy to monitor their intake of vitamins. All of these variances in multivitamin content must be considered by physicians and clinical pharmacists when selecting the appropriate multivitamin for pregnant women, taking into account all of the hazards and benefits that vitamin supplements may bring for fetus health and development. Clinical pharmacists should have a role in reducing the hazards of irrational use of prenatal vitamins in pregnancy by providing pregnant women with up-to-date information and addressing their concerns.
Footnotes
Acknowledgements
The authors have no acknowledgment
Data availability
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Authors’ contributions
Conceptualization: [Nilay Aksoy, Nur Ozturk]; Methodology: [Nilay Aksoy, Nur Ozturk]; Formal analysis and investigation: [Nilay Aksoy, Nur Ozturk]; Writing - original draft preparation: [Nilay Aksoy, Nur Ozturk]; Writing - review and editing: [Nilay Aksoy, Nur Ozturk]; Funding acquisition: [Nilay Aksoy, Nur Ozturk]; Supervision: [Nilay Aksoy, Nur Ozturk].
Ethics approval
No need.
Declaration of conflicting interests
The authors have no conflicts of interest to declare. All co-authors have seen and agree with the contents of the manuscript and there is no financial interest to report. We certify that the submission is original work and is not under review at any other publication.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.