
Abstract
Background
A plant-based diet (PBD) has been associated with potential health benefits, but factors that may affect access to and consumption of a PBD are not well defined.
Aim
To determine the association between socioeconomic status and plant-based dietary consumption among participants enrolled in the National Health and Nutrition Examination Survey (NHANES).
Methods
This was a cross-sectional study using data obtained from the NHANES database. The following covariates were assessed: age, sex, race/ethnicity, educational level, marital status, smoking status, physical activity, alcohol use, history of diabetes, and hypertension. Socioeconomic status was categorized according to poverty-income ratio (PIR). Food frequency questionnaires were used to calculate previously validated plant-based diet index (PDI) and healthful plant-based diet index (hPDI). Multivariable-adjusted logistic regression was performed to determine the association between PIR, clinical, demographic, and plant-based diet indices.
Results
A total of 5037 participants were in the final analytic sample. Median age of participants was 51 ± 18.5 years. Overall PDI and hPDI were 50 [46–54] and 52 [47–57], respectively. Median PDI index was significantly different among PIR groups (PDI, p = 0.018; hPDI, p < 0.001). On multivariable analysis, participants in the poorest socioeconomic group (PIR ≤ 130%) were more likely to have lower consumption of a healthful PBD (hPDI).
Conclusion
Lower socioeconomic status (PIR ≤ 130%) was associated with decreased consumption of a healthful plant-based diet. These data suggest that socioeconomic disparities may limit consumption of healthier food and contribute to the high prevalence of adverse health conditions that exist in certain population groups.
Introduction
Racial and socioeconomic disparities that affect access to healthy food may contribute to the high prevalence of heart disease, diabetes, and cancer observed in underrepresented minority populations (Rehm et al., 2016). Disparities in the quality of various diets according to race/ethnicity, education level, and income have been reported (Thompson, 2003; Rehm et al., 2016; Wang et al., 2014). Age and racial/ethnic differences in dietary sources of protein have also been observed, implying that social and cultural factors play a role in food choices. For example, Hispanics were the only identified group to have plant-based protein in the top 10, and younger groups were less likely to obtain a large portion of protein from fish (Beasley et al., 2020). Furthermore, Black and poor communities have less access to healthy diet components (Zenk et al., 2006). Consumption of a plant-based diet (PBD), quantified by a higher healthful plant-based diet index (hPDI) score, is associated with a lower risk of all-cause mortality in U.S. adults (Kim et al., 2018). Intake of dark green vegetables and green leafy vegetables has been associated with lower risk of heart disease (Bhupathiraju et al., 2013). Barriers to adoption of a PBD may include differences in cultural habits, beliefs, or socioeconomic disparities (Wang et al., 2014; Råberg Kjøllesdal et al., 2010). In fact, the overall prevalence of overweight adolescents has been shown to be 50% higher in poor versus nonpoor families (Miech et al., 2006).
Determinants that may be associated with consumption of a PBD including race/ethnicity and socioeconomic status have not been fully investigated. PBD indices which register different scores for animal foods, healthy plant foods, and less-healthy plant foods have been constructed and validated to investigate the association between PBD and mortality (Kim et al., 2018). Consumption of a PBD index rich in healthier plant foods is associated with a significantly lower risk of coronary heart disease (Satija et al., 2017). Increased consumption of plant-based foods, however, can potentially decrease nutritional intake when substituted for certain nutrient-dense animal foods (Cifelli et al., 2016). We examined the relationship between socioeconomic status as measured by poverty-income ratio (PIR) and consumption of a PBD among participants in the National Health and Examination Survey (NHANES).
Methods
Data source
We obtained data from the publicly available continuous National Health and Nutrition Examination Survey (NHANES) from 2003–2006. The NHANES is a biannual survey that assesses the health of the United States population through demographic and lifestyle questionnaires as well as lab measurements and physical examinations with body measures. We selected the time period from 2003–2006 since these were the most recent years to assess the Food Frequency Questionnaire (FFQ). The FFQ is a 139-item survey administered by the NHANES that queries participants regarding their estimated frequency of intake of several different food items (Shim et al., 2014). All files were obtained and merged by participant ID using SAS Version 9.4 in accordance with NHANES recommendations. Data is publicly available and de-identified of all protected health information and potential identifiers; therefore, no Institutional Review Board approval was required to conduct this secondary data analysis.
Participant selection
After selecting males and females ≥ 18 years of age from the NHANES database, the following exclusion criteria were applied: incomplete plant base diet index information, incomplete family PIR information, missing clinical and demographic variables. Starting with 11,183 participants, 6146 were excluded, of those 3643 were excluded due to incomplete dietary information, 433 incomplete level of education, family PIR, household income or marital status, 110 unreported BMI, and 1960 due to unreported clinical variables such prevalence of HTN, DM, alcohol use, METs per week, or serum creatinine.
Clinical and demographic variables
Based on prior studies (Fan et al., 2015; Robbins et al., 2001), the following covariates reported by participants were considered for analysis: age (continuous), sex (male or female), race/ethnicity (non-Hispanic white, non-Hispanic black, Mexican American, other Hispanic, or other), educational level (less than high school, high school, some college, college graduate), marital status (married, widowed, separated or divorced, never married), smoking status (current, former, or never smoker), physical activity (as a continuous variable using metabolic equivalents), monthly alcohol use (questioned regarding number of occasions and quantity per month), history of diabetes mellitus (ever told by a doctor they had diabetes other than in pregnancy), hypertension (ever told by a doctor they had high blood pressure), and family PIR. Age, sex, race/ethnicity, education level, marital status, smoking status, alcohol use, physical activity, and history of diabetes mellitus and/or hypertension were assessed through questions administered by oral interviews in English and Spanish.
Family PIR is calculated by the NHANES team using the U.S. Department of Health and Human Services Poverty Guidelines that are updated annually. Family PIR is used to categorize income by poverty threshold and is utilized as an indicator of socioeconomic status. Poverty thresholds are adjusted for family size and inflation. A PIR under 1 (100%) indicates that a family is below the poverty line (Thompson, 2003; Freedman et al., 2007). PIR was stratified into 3 family income categories: low income (≤ 130% of the poverty line), middle income (131–350% of the poverty line), and high income (> 350% of the poverty line) (Alaimo et al., 2001).
To quantify physical activity, participants answered the number of times they participated in various activity categories such as walking, running, swimming, etc. and each activity was converted to weekly metabolic equivalents (MET) (Ainsworth et al., 2000). Total serum creatinine was measured with the use of previously described methods (Schmidt et al., 2015).
Plant-based diet Index
We quantified plant-based diet using the Plant-Based Diet Index (PDI) and healthful PDI (hPDI), which are validated indices for measuring the level of overall plant foods in the diet of a population. Detailed methods for construction of PDI and hPDI have been previously described (Satija et al., 2017). Briefly, daily serving sizes were calculated based on responses from the FFQ, a survey administered by the NHANES between 2003–2006, to assess consumption of various foods throughout the year. Serving sizes were then grouped from individual foods into 17 groups (Supplementary Table 1) and then assigned a score from 1 through 5 based on the quintile of consumption. For PDI, the highest quintile of consumption was assigned a 5 for all plant foods and a 1 for all animal foods. For hPDI, the highest quintile of consumption was only assigned for plant foods deemed to be healthy. Thus, after categorizing participants into quartiles based on PDI, those with lower and higher PDI and hPDI were categorized into the first (Q1) and fourth (Q4) quartiles, respectively.
Statistical analysis
Statistical analysis was performed with SPSS 24 software. Continuous variables were presented as medians and interquartile ranges [percentile: 25th-75th] or mean and standard deviation in accordance with data distribution. Comparison of continuous variables between PIR groups was performed with the Kruskal-Wallis or ANOVA test as required. Categorical variables were presented as absolute variables and frequencies and analysis was performed with the Chi-square test. Correlation analysis between PIR and dietary characteristics was performed with the Spearman test. Multivariable-adjusted logistic regression analysis was performed to determine the association between PIR ≤ 130% (dependent variable) and clinical, demographic, and PBD index percentile. A p-value < 0.05 was considered statistically significant.
Results
A total of 5037 participants consisting of 2545 (50.5%) males and 2492 (49.5%) females were in the final analytic sample (Table 1). The overall median age was 51 ± 18.5 years. The largest ethnic/racial group was White (58.3%), followed by Black (18.2%), and Mexican (17.7%). A total of 1446 (28.7%) participants had some college education and 3290 (65.3%) were married or living with a partner. A total of 1674 (33.2%) participants had an annual income of $35,000 - $74,999, and the overall family PIR was 258% [136% - 445%]. Analysis of clinical and demographic variables demonstrated that only gender distribution was similar between groups (p = 0.376). Age, race/ethnicity, level of education, marital status, BMI, comorbidities, weekly physical activity, and alcohol consumption were significantly different between PIR groups (p < 0.05). A full description of clinical and demographic characteristics of participants is shown in Table 1.
Clinical and demographic characteristics according to family poverty income ratio (PIR) groups.
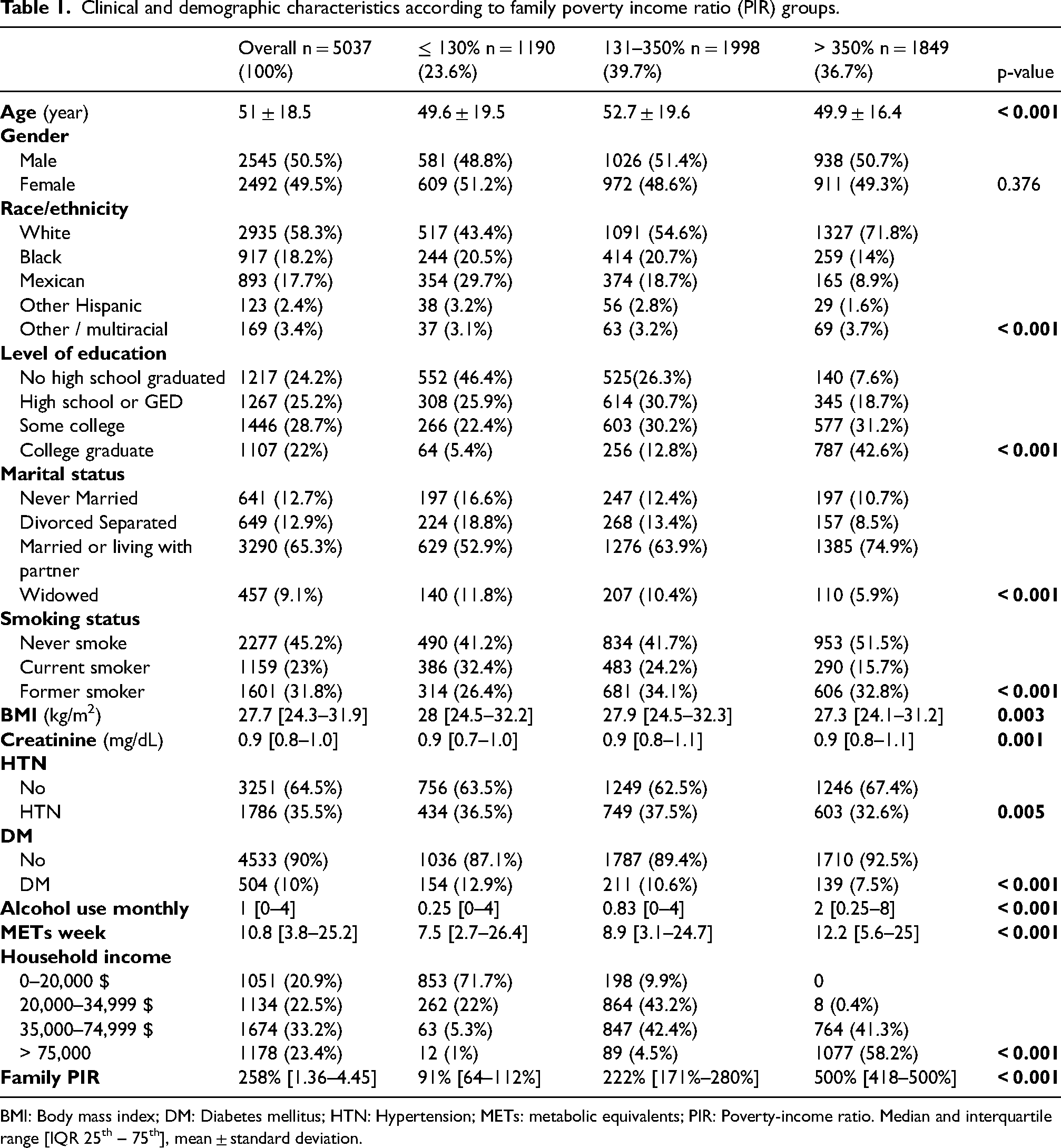
BMI: Body mass index; DM: Diabetes mellitus; HTN: Hypertension; METs: metabolic equivalents; PIR: Poverty-income ratio. Median and interquartile range [IQR 25th – 75th], mean ± standard deviation.
The overall PDI and hPDI among participants was 50 [46–54] and 52 [47–57], respectively (Table 2). After categorizing participants according to family PIR, a total of 1190 (23.6%) were in the poorest group with a PIR of ≤ 130%, followed by 1998 (39.7%) with a PIR of 131–350%, and 1849 (36.7%) with a PIR > 350%. Median PBD indices were different between PIR groups (PDI, p = 0.018; hPDI, p < 0.001). Analysis of PIR groups after stratification of PBD indices into quartiles from lowest (Q1) to highest (Q4) demonstrated that PBD consumption was different between PIR groups (PDI, p = 0.013; hPDI, p < 0.001).
Dietary characteristics of family PIR groups according to plant-based diet index (PDI) and healthful plant-based diet index (hPDI) quartiles.
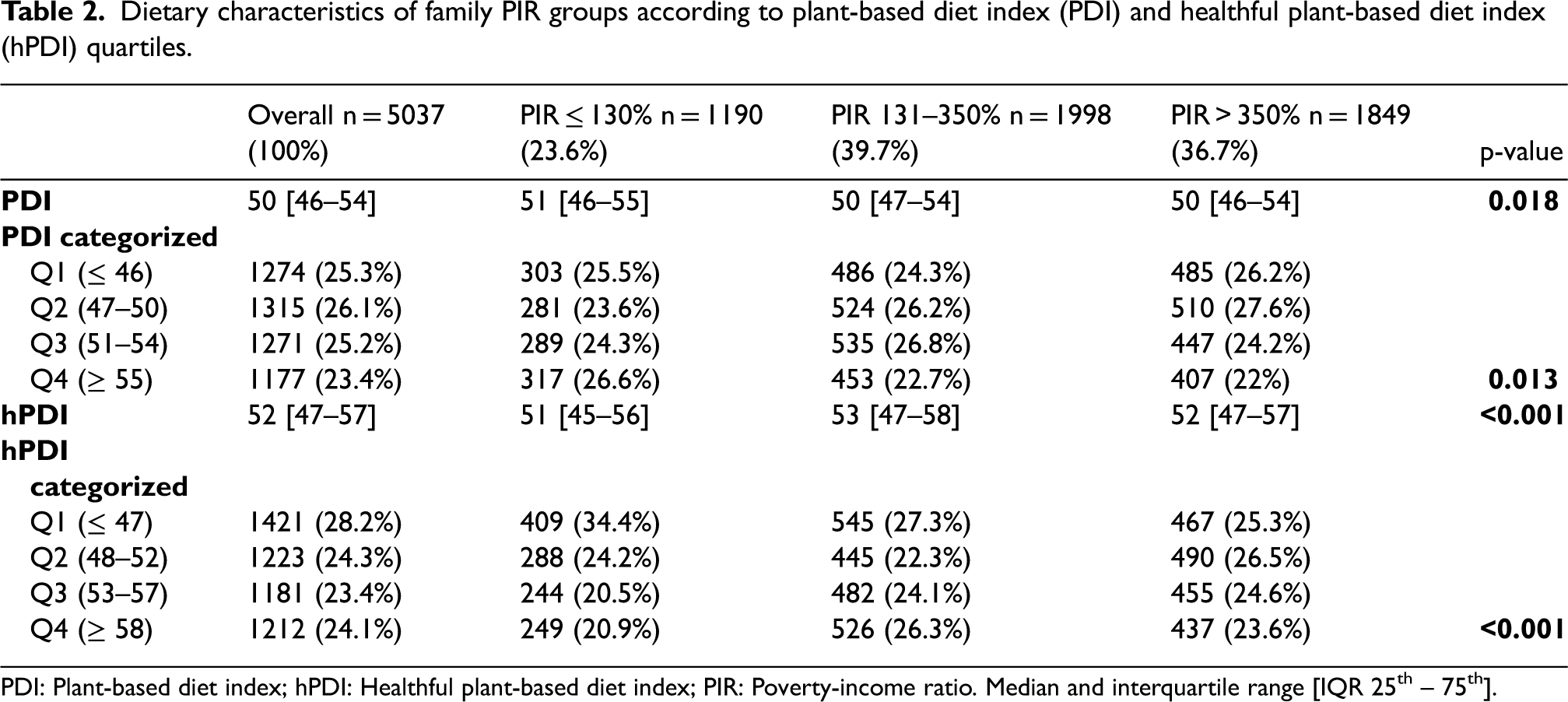
PDI: Plant-based diet index; hPDI: Healthful plant-based diet index; PIR: Poverty-income ratio. Median and interquartile range [IQR 25th – 75th].
Multivariable-adjusted logistic regression analysis was performed to determine the relationship between PIR ≤ 130% (lowest socioeconomic group) and clinical/demographic characteristics (Table 3). Mexican ethnicity and current smokers were significantly associated with PIR ≤ 130% (p < 0.001). In both models (PDI and hPDI) age, race/ethnicity, level of education, marital status, and alcohol consumption were significantly associated with PIR ≤ 130% (p < 0.05). A significantly lower likelihood of consuming a healthful PBD was observed among participants in the poorest socioeconomic group (PIR ≤ 130%). Participants in Q3 had an OR = 0.706 (95% CI: 0.578–0.863; p = 0.001) and participants in Q4 had an OR = 0.663 (95% CI: 0.540–0.814; p < 0.001). These data indicate that participants with higher healthful PBD consumption are less likely to be part of the PIR ≤ 130% group.
Multivariable-adjusted analysis between participants with family PIR ≤ 130%, clinical, demographic, and dietary characteristics.
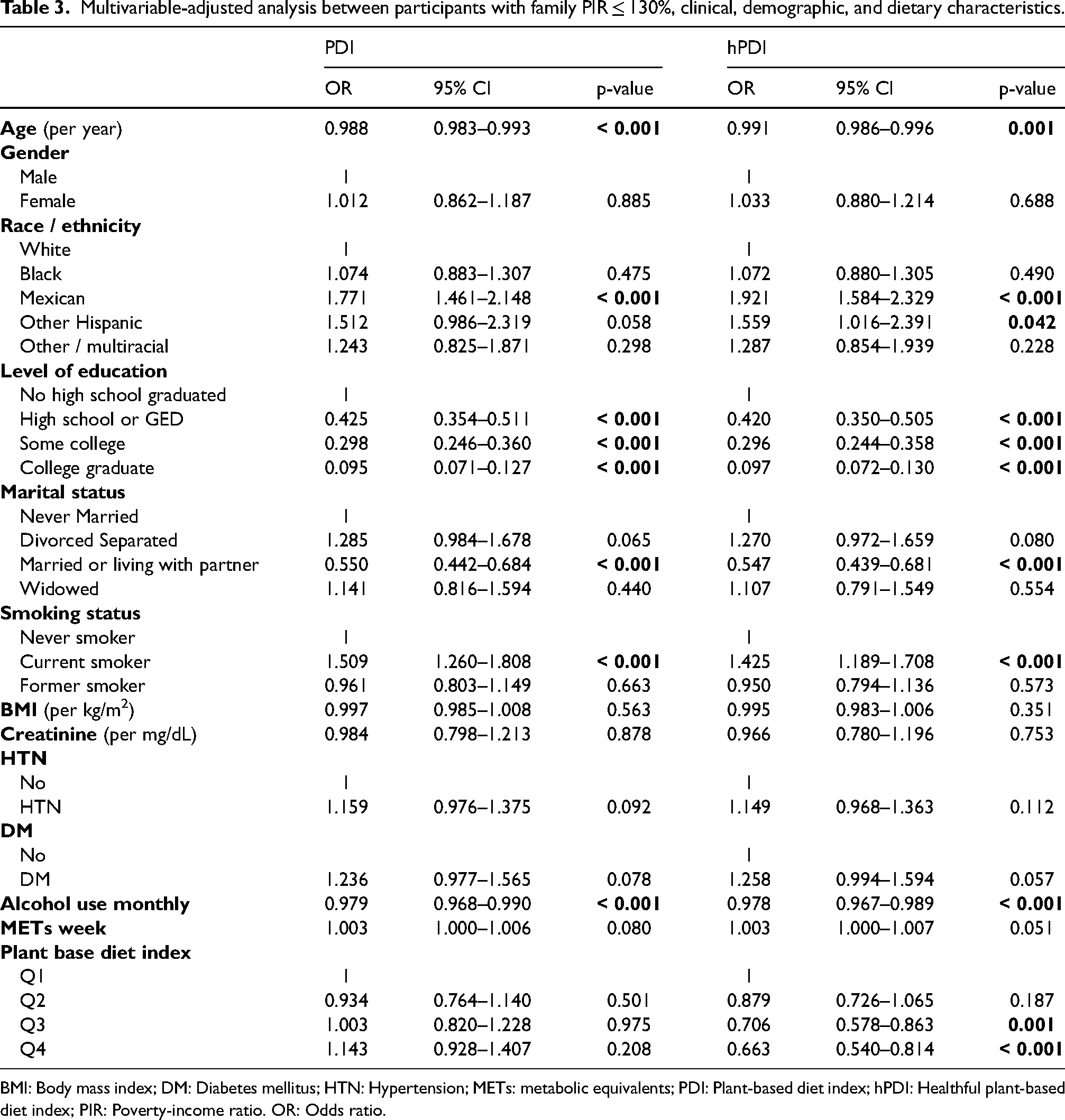
BMI: Body mass index; DM: Diabetes mellitus; HTN: Hypertension; METs: metabolic equivalents; PDI: Plant-based diet index; hPDI: Healthful plant-based diet index; PIR: Poverty-income ratio. OR: Odds ratio.
Discussion
There is growing evidence that suggests restriction of animal-based food is associated with improved environmental health effects (Aleksandrowicz et al., 2016). Consumption of a PBD has been associated with decreased risk of obesity, cardiovascular disease, type 2 diabetes mellitus, and mortality (Barnard et al., 2006). However, PBD may be less accessible to populations with lower socioeconomic status. Therefore, we sought to determine the association between socioeconomic status according to PIR and consumption of a PBD among participants in the NHANES database.
Mexican ethnicity and current smokers were significantly associated with PIR ≤ 130%. This is in line with the finding of Hitchman et al. that reported participants of the International Tobacco Control Project in the lower socioeconomic status recorded a higher number of smoking friends (Hitchman et al., 2014). In contrast, older age, higher education, being married or living with a partner, and alcohol consumption were less likely to be associated with poverty (PIR ≤ 130%) on multivariable-adjusted analysis.
High consumption of a healthful PBD (hPDI) was less likely to be observed among participants with the lowest socioeconomic status (PIR ≤ 130%). Our findings are consistent with a previous report that showed access to core components of a healthy diet varied by race and socioeconomic status, and negatively affected Black and poor communities (Zenk et al., 2006). The authors of this study suggested that food insecurity could potentially be a barrier to a healthier diet resulting in consumption of lower quality, unhealthy, and inexpensive food. Time scarcity, in which parents are working multiple jobs to support their family, may also encourage intake of fast food or pre-cooked processed meals, leading to unhealthy lifestyle choices in low socioeconomic communities (Popkin and Hawkes, 2016). Moreover, it has been shown that lower socioeconomic status is associated with poor diet quality, and that dietary improvement in the U.S. from 1999–2010 was mainly driven by communities with higher socioeconomic status (Wang et al., 2014).
The U.S. government publishes “Dietary Guidelines” to promote health and prevent illnesses. However, 6 out of 10 adults are living with a diet-related chronic disease (McGuire, 2011). This statistic underscores the need for further interventions and education to promote a shift toward consumption of a healthful PBD, which may improve overall public health. Such strategies should incorporate economically and socially appropriate interventions to achieve success.
We found that participants in the poorest socioeconomic group (PIR ≤ 130%) had decreased consumption of a healthful plant-based diet, but our research is not without limitations. This study is cross-sectional, and no cause-effect relationship can be established. Furthermore, NHANES lacks data regarding change in dietary behaviour or lifestyle modifications over time, which can result in significant confounding factors. Moreover, FFQ is subject to both recall and self-serving bias. The complex interaction between clinical, demographic, socioeconomic, cultural, and dietary characteristics of different populations should also be considered when studying this prospective research cohort. Despite these limitations, our study highlights a potentially significant barrier to consumption of a healthful PBD that should be addressed as part of future public health strategies.
Conclusion
Lower socioeconomic status is associated with decreased consumption of a healthful plant-based diet. Socioeconomic disparities may limit access of certain populations to healthy food and contribute to a higher prevalence of adverse medical conditions. Additional studies are needed to characterize social and economic barriers that prevent access to healthy food to establish policies that can better address the needs of vulnerable populations.
Supplemental Material
sj-docx-1-nah-10.1177_02601060221109669 - Supplemental material for Socioeconomic differences associated with consumption of a plant-based diet: Results from the national health and nutrition examination survey
Supplemental material, sj-docx-1-nah-10.1177_02601060221109669 for Socioeconomic differences associated with consumption of a plant-based diet: Results from the national health and nutrition examination survey by Mia R. Gonzalgo, Sirpi Nackeeran, Ali Mouzannar and Ruben Blachman-Braun in Nutrition and Health
Footnotes
Availability of data and materials
NHANES data is publicly available.
Authors’ contributions
Gonzalgo: conceived, designed, analysed data, wrote manuscript; Nackeeran: designed, collected data, analysed data, edited, and reviewed manuscript; Mouzannar: analysed data, edited, and wrote manuscript; Blachman-Braun: designed, performed statistical analyses, analysed data, wrote manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the content in this manuscript.
Ethical statement
All authors have been personally and actively involved in substantive work leading to this manuscript and will hold themselves jointly and individually responsible for its content.
Consent for publication
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.