
Abstract
Background
The timing, route, and amount of nutrition for surgical patients with substantial caloric deficits remain active areas of study. Current guidelines are based on in-hospital days NPO after admission to the hospital. This historic process neglects the multiple days of caloric deficit patients experience prior to hospital admission.
Aim
To determine the impact of pre-hospital caloric deficit (PHCD) for surgical patients on their outcomes.
Methods
313 patients admitted with a diagnosis of small bowel obstruction, pancreatitis, or diverticulitis were analyzed for their PHCD's. PHCD's were estimated using patient-reported days with significant emesis, and absent oral intake. Patients with PHCD's were compared to patients with no PHCD for length of stay, status on discharge, disposition, and 30-day readmission rate.
Results
There were 313 patients and 42% of the patients were male. The median age was 65 years. Median number of days sick prior to hospital admission was 1 (IQR: 1 to 2). Median PHCD was 1882 kcal (IQR: 1355 to 3650). Median number of days NPO while in-hospital was 3 (IQR: 2 to 5). Median in-hospital caloric deficit was 4268 kcal (IQR: 2825 to 6610). No significant association was observed between discharge disposition, complication rate, ambulatory status, 30-day readmission rate and PHCD. In-hospital caloric deficit was associated with complications after surgery (p < 0.0001).
Conclusion
Small PHCD's in patients with SBO's, pancreatitis, or diverticulitis do not negatively affect their outcomes. Further research of patients with large PHCD's is needed to best treat surgical patients at risk for malnutrition.
Keywords
Introduction
The timing, route, and amount of nutrition for surgical patients with substantial caloric deficits remain active areas of study. Early (within 24 to 48 h of hospital or ICU admission) enteral nutrition (EN) leads to reduced infections, complications, length of stay, and mortality (Marik and Zaloga, 2001: 2264–2270). EN is preferred to parenteral nutrition (PN) because it reduces infectious complications such as pneumonia, central line infections, and intra-abdominal abscess formation (McClave et al., 2016: 159–211). Data is limited for surgical patients with compromised intestinal tracts, but there is a trend that supports early enteral nutrition (Pupelis et al., 2001: 91–94; Singh et al., 1998: 142–146). Gastrointestinal (GI) surgical patients prove to be a special population; they frequently present to the hospital with many days of nausea, vomiting, decrease oral intake and once admitted are kept nil per os (NPO) for many days. This is especially true of patients with small-bowel obstructions, pancreatitis, and diverticulitis. When patients have not achieved adequate nutritional intake for 7–10 days or when EN is not feasible, they are considered for PN. While starting EN early is beneficial, the same is not necessarily true for PN. Early PN (within 2 days admission to ICU) leads to increased mortality and infectious complications (see Casaer et al., 2001: 506–517; Sax et al., 1987: 117–124) while later PN (>14 days) leads to increased morality (see Sandstrom et al., 1993: 185–195). There is limited data addressing the nutritional status at admission for GI surgical patients. The data, and current guidelines, only account for time admitted to the hospital and apply to patients at low nutritional risk. Current research does not account for pre-hospital caloric deficits (PHCD's). We hypothesized that patients presenting to the hospital with the diagnosis of small-bowel obstruction, pancreatitis, or diverticulitis, that have large PHCD's have poor outcome measures including length of stay, functional status, and 30-day readmission rates.
Methods
We performed a retrospective review of 313 surgical patients from 2017–2019 admitted to two metropolitan teaching surgical hospitals. Pre-hospital deficits were estimated using patient-reported days with significant nausea, emesis, and absent oral intake. Inpatient deficits were estimated using total days kept NPO. The number of days NPO or with significant symptoms were converted to caloric deficits using ideal body weights and a 25KCal/Kg/d expected daily intake. All patients were made NPO upon admission to the hospital though some patients quickly recovered from their illness and were advanced to a regular diet and discharged within a day. Inclusion criteria for the study were: Age 18 and older, primary admitting diagnosis of small bowel obstruction, acute pancreatitis, or diverticulitis. Patients were excluded if they were immune-compromised, taking immune-modulators at the time of admission, had malignant small bowel obstructions, or carried a diagnosis of ulcerative colitis or Crohn's disease. Causes for pancreatitis included gallstones, alcohol, hypertriglyceridemia, and idiopathic. Causes for SBO included adhesions, hernias (which included ventral, incisional, inguinal, and internal hernias), and primary (SBO in a patient with no prior surgery). Smoking history and co-morbidities such as hypertension, hyperlipidemia, diabetes mellitus, coronary artery disease, cerebrovascular accident, cancer, dementia, and COPD were recorded for each patient. The Charlson Co-morbidity index was used to give a morbidity score and risk of death within 5 years for each patient and a means to give weight to sicker patients. Surgery for patients who required an operation was performed on an urgent or emergent basis. The days from admission to surgery was also captured. Discharge ambulatory status was classified into categories: Independent – not limited, Independent – limited, rolling walker, wheelchair, and bedbound. Disposition was analyzed as three categories: home without assistance, skilled needs, which included home with assistance and rehabilitation center, or deceased. Length of hospital stay was defined as the number of days from admission to discharge. Readmission within 30 days was binary and recorded for any readmission reason. Patients with pre-hospital deficits were compared to patients with no pre-hospital deficit for length of stay, status on discharge as measured by ambulatory status and disposition, and 30-day readmission rate.
Statistical methods
Descriptive statistics were reported for each variable for the overall cohort and by diagnosis. Continuous variables were reported as means and standard deviations, or as medians and interquartile ranges (IQR: 25th percentile to 75th percentile), as appropriate. Categorical variables were reported as frequencies and percentages. To examine differences in explanatory variables by diagnosis, Wilcoxon rank sum tests were used to test for differences in continuous variables, and Chi-square tests or Fisher's exact tests were used to test for differences.
All outcomes were analyzed using logistic regression. Univariable logistic regression was used to test for association of each of the outcomes (discharge disposition, ambulatory status, functional status, and 30-day readmission) with PHCD. Multivariable logistic regression was used to test for association between each of the outcomes with PHCD while adjusting for the covariates: diagnosis, surgery, and in-hospital caloric deficit in the model when feasible. Backwards elimination was used to retain only those covariates that were statistically significant while forcing the model to include PHCD - the primary variable of interest A p-value < 0.05 was considered statistically significant. All analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC).
Results
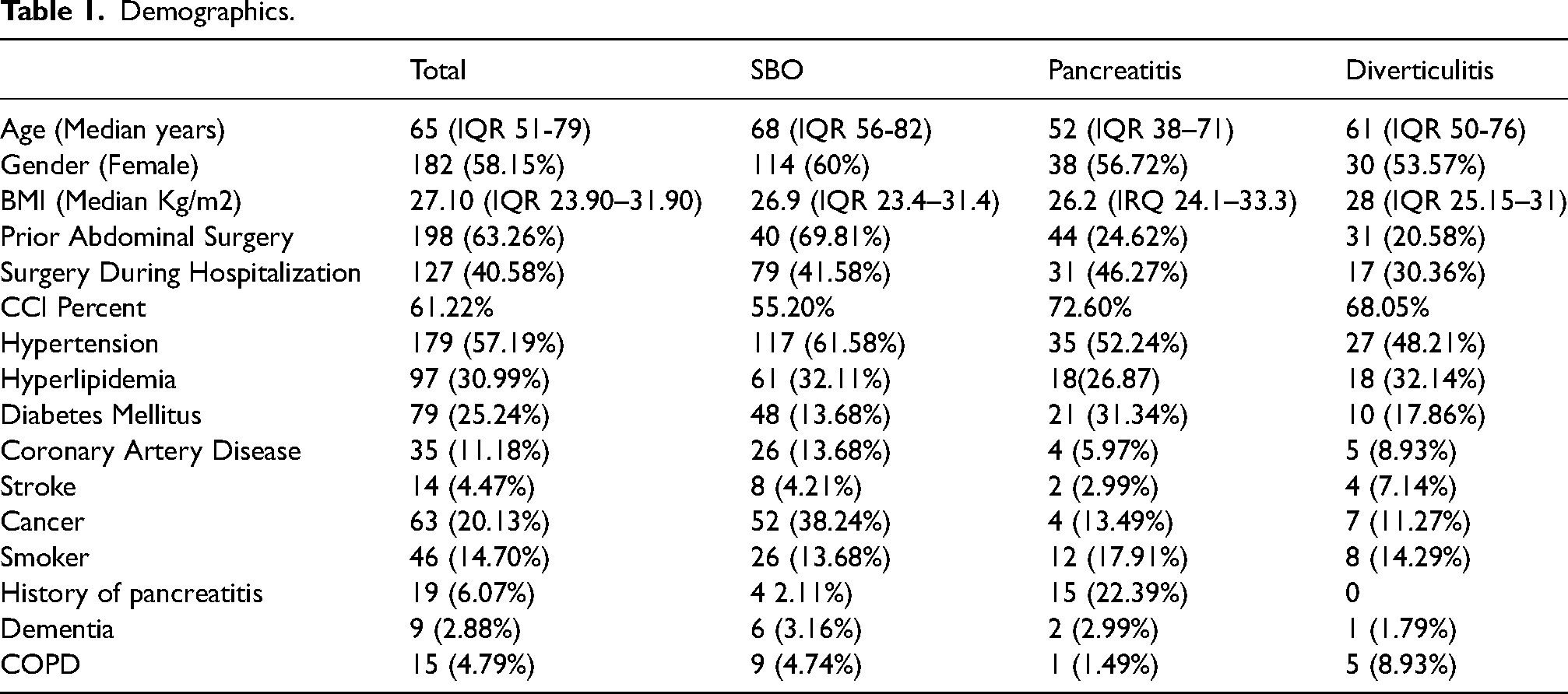
Records from 313 patients were included in the study. 61% (n = 190), had a diagnosis of SBO, 21% (n = 67) had a diagnosis of pancreatitis, and 18% (n = 56) had a diagnosis of diverticulitis. Forty-two percent (n = 131) of the patients were male. The median patient age was 65 years (IQR: 51 to 79). A summary of the demographics including comorbidities are depicted in Table 1. There were not any significant differences in comorbidities across the three diagnoses though the age of the SBO patients tended to be higher than the ages of the pancreatitis and diverticulitis patients.
Demographics.
Median number of days sick prior to hospital admission was 1 (IQR: 1 to 2). Median PHCD was 1882 kcal (IQR: 1355 to 3650). Median number of days NPO while in-hospital was 3 (IQR: 2 to 5). Median in-hospital caloric deficit was 4268 kcal (IQR: 2825 to 6610). Four patients were NPO during their entire hospital stay, two of these four patients were discharged after 1 day (ie they were advanced to a regular diet within 24 h of admission), and two died in the hospital. Most patients were NPO and removed from NPO once (95% (n = 296)), with the remaining patients having been cycle on/off NPO between two and four times. Forty-one percent (n = 127) of patients had surgery.
Results by outcome
Two percent (6 of 313) of patients expired while in the hospital. No significant association was observed between discharge disposition and PHCD. Only univariable analysis was performed because of the small number of events.
Fourteen percent (45 of 311) of patients experienced a complication due to their diagnosis as classified on the Clavien-Dindo scale. Of these 45 patients, 25 were SBO patients, 14 were pancreatitis patients, and 6 were diverticulitis patients. There was no significant association between PHCD and complication rate. For the multivariable analysis, although PHCD was not significantly associated with complications, in-hospital caloric deficit was associated with complications after surgery and diagnosis were removed during backward elimination (p < 0.0001).
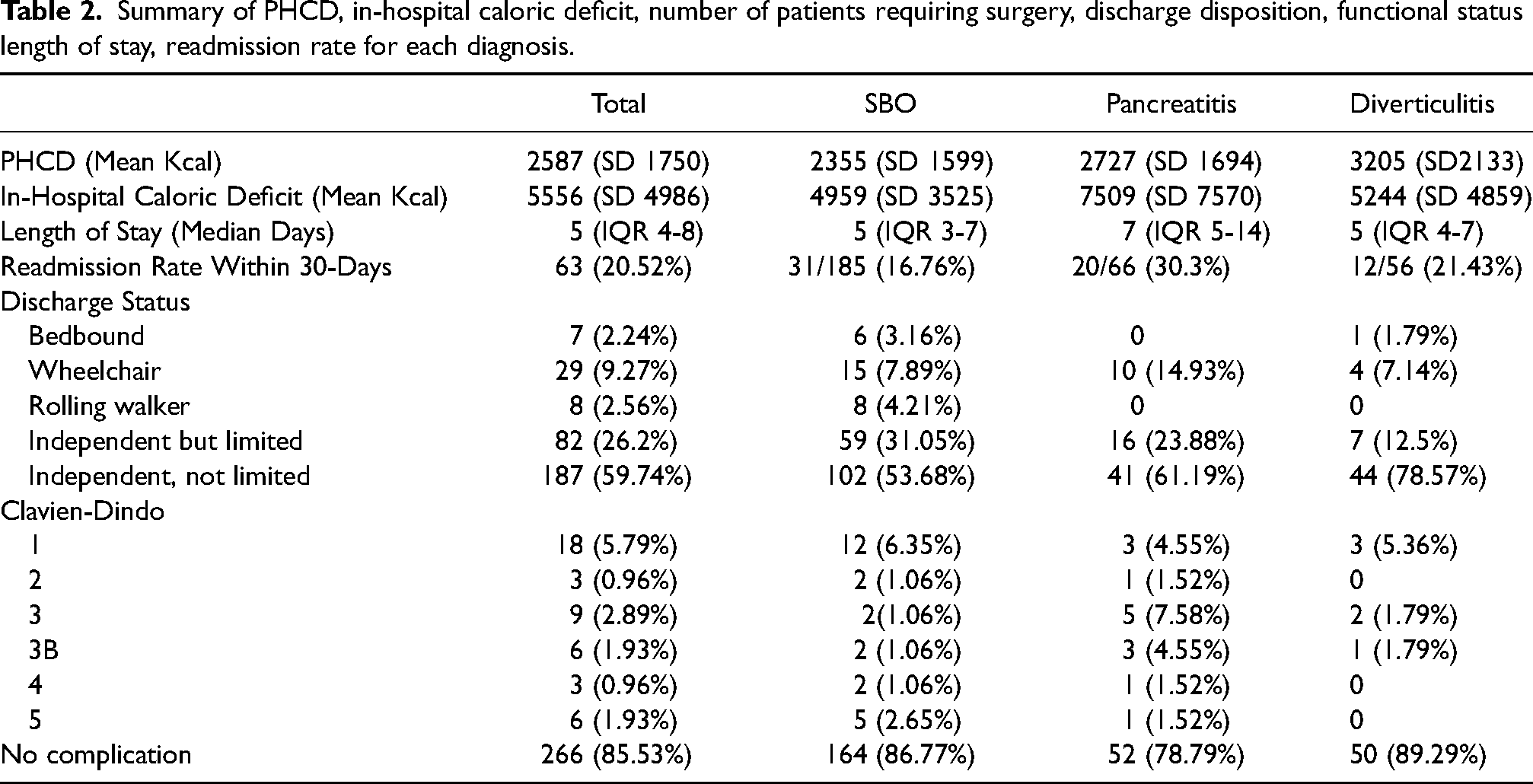
Of the 307 patients who were discharged alive, thirteen percent (n = 39) had an ambulatory status of being bedbound, needing a wheelchair, or needing a rolling walker. There was no significant association between ambulatory status and PHCD for the univariable or the multivariable analyses. Twenty-one percent of patients (63 of 311) were readmitted within 30 days. No significant association was observed between 30-day readmission and PHCD in the univariable or the multivariable analysis (Table 2).
Summary of PHCD, in-hospital caloric deficit, number of patients requiring surgery, discharge disposition, functional status length of stay, readmission rate for each diagnosis.
Results by diagnosis
Median number of days sick prior to hospital admission was 1 (IQR: 1 to 2) for SBO patients, 1 (IQR: 1 to 3) for pancreatitis patients, and 2 (IQR: 1 to 3) for diverticulitis patients. Median PHCD was 1768 kcal (IQR: 1355 to 3075) for SBO patients, 1940 kcal (IQR: 1355 to 3893) for pancreatitis patients, and 3014 kcal (IQR: 1470 to 4254) for diverticulitis patients. Median number of days NPO while in-hospital was 3 (IQR: 2 to 4) for SBO patients, 4 (IQR: 3 to 5) for pancreatitis patients, and 2.5 (IQR: 2 to 4) for diverticulitis patients. Median in-hospital caloric deficit was 3892 kcal (IQR: 2712 to 6200) for SBO patients, 5184 kcal (IQR: 3720 to 8262) for pancreatitis patients, and 3880 kcal (IQR: 2652 to 5821) for diverticulitis patients. There was no significant association observed between discharge disposition and PHCD for SBO patients with univariable analysis. No multivariable analysis was performed for discharge disposition because of the small number of events. No significant association was observed between functional status and PHCD in patients with SBO for univariable or multivariable analyses, although in-hospital caloric deficit was statistically significant (p < 0.0001). No significant association was observed between ambulatory status and PHCD for SBO patients in univariable or multivariable analyses, although in-hospital caloric deficit was statistically significant (p < 0.011). No significant association was observed between 30-day readmission and PHCD in patients with SBO who were alive at discharge for univariable or multivariable analyses.
Because of the small number of patients with pancreatitis and with diverticulitis, and the small number of events for each of these diagnoses for the outcomes discharge disposition, functional status, ambulatory status, and 30-day readmission, no univariable or multivariable analyses were performed on these diagnosis subgroups.
Discussion
Current guidelines set forth by leaders in nutrition for critically ill patients are based on in-hospital data for patients. Malnutrition is associated with poorer outcomes for surgical patients. Malnutrition is also associated with increased lengths of stay, increased admissions to ICU's, delayed wound healing, cancer recurrence, reoperations, and increased infectious complications (Enomoto et al., 2013: 1181–1200). Limited data on the PHCD exists especially for patients with surgical conditions such as SBO, pancreatitis, and diverticulitis. While nutrition scoring tools have been validated to predict morbidity for GI surgery patients they do not consider the acute malnutrition caused by the patients’ conditions leading up to and during hospital admission (Schiesser et al., 2009: 519–526). Furthermore, protein and caloric deficits in critically ill patients has been shown to lead to a higher likelihood of being discharge to a rehabilitation center or skilled nursing facility rather than home (Yeh et al., 2016: 37–44). Patients with these conditions have varying degrees of decreased PO intake prior to admission to the hospital. We found that while patients typically presented to the hospital soon after developing significant retractable nausea and vomiting, but that also some patients arrived malnourished. We set out to investigate the effect of pre-hospital malnutrition on patients with surgical conditions.
We found that having a PHCD did not cause worse outcomes when controlled for baseline characteristics. This conclusion is based on patients whose median number of days NPO prior to arrival was low. It is unclear if the same conclusion can be drawn for patients with a larger PHCD or who are at baseline malnourished. The severity of disease was not characterized in this study and likely interfered with length of stay. It is possible that more severe conditions led to longer hospital stays but it is not clear if more severe conditions led to larger PHCDs. Furthermore, the severity of condition likely affected the other outcomes such as the rate of discharge home, functional status on discharge, and readmission rate.
There were many limitations to the study. The biggest limitation was the heterogeneity in patient population. Patient care differed because of diagnosis and physician. In particular, the course of treatment, e.g., when to take patient off NPO, and whether to have surgery or when to have surgery varied by physician. Furthermore, the amount of decreased pre-hospital intake was not routinely characterized which excluded a substantial number of patients from the study. Lastly, the additional examination of the relationship of PHCD for each diagnosis was hindered by the limited sample size.
Limited data exists partly due to the nature of the data – it is a subjective reporting from patients. Patients do not precisely describe their intake over many preceding days in the light of illness unless prompted. Many times, the history did not include a detailed description of the patient's oral intake. It was rare that the nutrition status prior to the onset of the patients’ conditions was clearly documented. Significant nausea or vomiting was used as a proxy for poor caloric intake, though it is possible some patients were still eating despite their symptoms. The charts lacking descriptions of symptomology and decrease oral intake were excluded and charts with unclear pre-hospital deficits were resolved through second party review and discussion. To homogenize the characterization of PHCD, we included all patients admitted to the surgical services with the said diagnoses with clearly documented symptoms, and pre-hospital deficit was recorded prior to recording of outcomes to minimize risk of bias.
Pre-operative nutrition supplementation has been shown to be beneficial particularly in elective surgical cases (Jie et al., 2012: 1022–1027). Optimizing a patients’ nutrition status prior to a surgical operation with calorie and protein rich formulas promote maintenance of a perioperative anabolic state, improving healing, reducing complications, and shortening the time to recovery of bowel function and hospital discharge (Evans et al., 2014: 10). In this study, we concluded that acute malnourishment in patients with SBO, pancreatitis, and diverticulitis presenting to the hospital does not affect outcomes such as length of stay, hospital readmission rate, functional status, and discharge disposition. Nevertheless, we conclude that PHCD should be routinely considered both in determining timing of supplemental nutrition and implementing a more aggressive nutrition for surgical patients.
Conclusion
Small PHCD's in patients with SBO's, pancreatitis, or diverticulitis do not negatively affect their outcomes. It is established that larger the caloric deficit for surgical patients lead to a larger risk for complications related to malnutrition for surgical patients in the hospital. Further research of patients with large PHCD's is needed to best treat surgical patients at risk for malnutrition and establish a guideline pertaining to PHCD's.
Footnotes
Acknowledgements
None to declare.
Availability of data and materials
All data is de-identified and stored in an encrypted database that is not available to the public.
Authors’ contributions
All authors have made considerable contributions to this project and have given consent for publication.
Consent for publication
Informed consent for the project was waived through approval from the IRB.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This project was approved by the Northwell Health Institutional Review Board. Study # 18-0557.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.