
Abstract
Introduction
Malnutrition is a major public health problem worldwide, particularly among children under the age of five and mothers (Dadi and Desyibelew, 2019). Malnutrition refers to both over-nutrition (overweight) and under-nutrition (wasting, stunting, underweight). Low weight-for-height is referred to as wasting, and it typically suggests recent and significant weight loss as a result of a lack of food and/or an infectious condition. Whereas, stunting is defined as having a low height-for-age which is caused by chronic or recurring malnutrition, associated with low socioeconomic status, poor maternal health and nutrition, frequent sickness, and/or unsuitable feeding and care of a child in early life (World Health Organization, 2021). Malnutrition among children and mothers has a negative impact on national and international economic development, as well as health and sustainable development (National Institute of Population Research and Training (NIPORT) et al., 2016).
Poor nutrition during childhood can hinder children's physical and mental development, increasing their risk of contracting infectious diseases or other important infections and burdening society (Bardosono et al., 2007). Under-nutrition causes half of all child deaths under five, increases the frequency and severity of common diseases, and delays recovery (Unicef, 2021). In 2011, 3.1 million children died from under-nutrition, 45% of all under five deaths (Bhutta et al., 2013). Previous research studies identified children's age group, sex, parents’ educational status, type of food used for starting complementary feeding, and mothers’ financial decision-making ability as some significant determinants of undernutrition among under five years children (Alemayehu et al., 2015).
Overnutrition, like undernutrition, harms children. According to a recent estimate, 41 million children under five were overweight or obese, with another 92 million at risk (WHO, 2020). Nearly two-thirds of overweight/obese children live in developing nations, mainly Asia (∼50%) (Abarca-Gómez et al., 2017). Overweight children are at a higher risk of developing various health problems, such as heart disease, respiratory sickness, and type 2 diabetes (Ebbeling et al., 2002). Furthermore, overnutrition has a severe impact on children's social and emotional well-being, as well as their self-esteem, resulting in delayed social development (Mia et al., 2018). Mothers’ education status, place of residence, wealth index and mother's age at first birth were found to be as significant associated factors for overnutrition among under-five children (Mia et al., 2018).
Malnutrition harms mothers and their newborns, making it even more devastating (Hasan et al., 2017). Despite global economic growth, most South-Central and Southeast Asian countries have high maternal undernutrition rates (Tang et al., 2016). Maternal undernutrition (BMI less than 18.5 kg/m2) ranges from 10% to 19% in most countries (Tang et al., 2016). Undernutrition can cause suffering from a combination of chronic energy deficiency that leads to low birth weight (LBW), preterm and unsuccessful birth outcomes among mothers (Hasan et al., 2017). Previous research has shown that children born to teenage and malnourished mothers had a higher risk of neonatal mortality, LBW, nutritional deficiency, and delayed growth in Bangladesh and worldwide (Chen et al., 2007; Uddin et al., 2019). Therefore, the consequence of undernutrition in mothers can pass to the next generation, creating intergenerational cycles of malnutrition, illness, and death (Khatun et al., 2019). Prior research identified younger age, dietary diversity score, antenatal care (ANC) visit, and wealth index as associated factors for maternal undernutrition (Boke et al., 2021). Moreover, being overweight remains another public health issue among mothers since it increases their chance of gestational diabetes, type 2 diabetes, and cardiovascular disease, as well as having a negative impact on perinatal, neonatal, baby, and infant outcomes (Catalano et al., 2012).
Despite almost a decade of effort and significant socio-economic progress, poor maternal and child nutrition in the form of undernutrition and rising rates of overweight and obesity is still highly prevalent in Bangladesh (Hasan et al., 2020). In 2014, the prevalence of stunting, wasting and being overweight among children under five years was estimated at 36%, 14%, and 2%, respectively (National Institute of Population Research and Training (NIPORT) et al., 2016; Mia et al., 2018). Not only children but also women in Bangladesh often suffer underweight, exacerbated by poverty, food shortages, and illiteracy (Ruel et al., 2013). It was estimated that one-fifth of adult females are underweight in Bangladesh (UNICEF, 2019). Additionally, Bangladesh's motherhood obesity rate rose from 3% in 1996 to 24% in 2014 (National Institute of Population Research and Training, 2018). Thus, investigating undernutrition and overnutrition among children and mothers has become essential for public health researchers in Bangladesh.
Moreover, understanding the prevalence and determinants of undernutrition and overnutrition in children and mothers is crucial to improving their health by allocating resources. This study was carried out to identify the most recent prevalence and determinants of maternal and child malnutrition. No prior study was carried out this analysis using the most recent (2017–18) Bangladesh Demographic and Health Survey (BDHS), which is nationally representative. Therefore, this study aimed to estimate the prevalence of malnutrition among Bangladeshi children (stunting, wasting, and overweight) and mothers (underweight and overweight) and examine the contribution of various factors using a nationally representative data set.
Methods
Data source
We used the most recent (2017–18) BDHS data, which is the eighth nationally representative cross-sectional surveys in the series implemented by the collaborative efforts of the National Institute of Population Research and Training (NIPORT), and Mitra and Associates.
Study design
A two-stage stratified sample of households was used in BDHS to generate a representative sample of Bangladesh. The survey employed a list of enumeration areas (EAs), the primary units of sampling/cluster, provided by the Bangladesh Bureau of Statistics (BBS) as a sampling frame, with an average of roughly 120 households. During the first stage, 675 EAs were picked with a probability proportional to EA size, which ensured that 250 EA were selected in urban areas and 425 EA were selected in rural areas. Second-stage sampling included a systematic selection of 30 households per cluster or primary sampling unit to provide statistically reliable estimates of the health indicators for the country as a whole, for urban and rural areas specific and for each of the eight divisions.
Participants
The survey sampled 20,376 ever-married women of childbearing age and interviewed 20,127 of them. Eleven thousand eight hundred six of them did not have children under the age of five and thus, were excluded from the analysis. Additionally, 521 women who had given birth two months before the survey were excluded. The analysis included 8321 children aged 0–59 months and 7800 mothers aged 15–49 years. The data extraction steps are depicted in the schematic diagram (Figure 1).
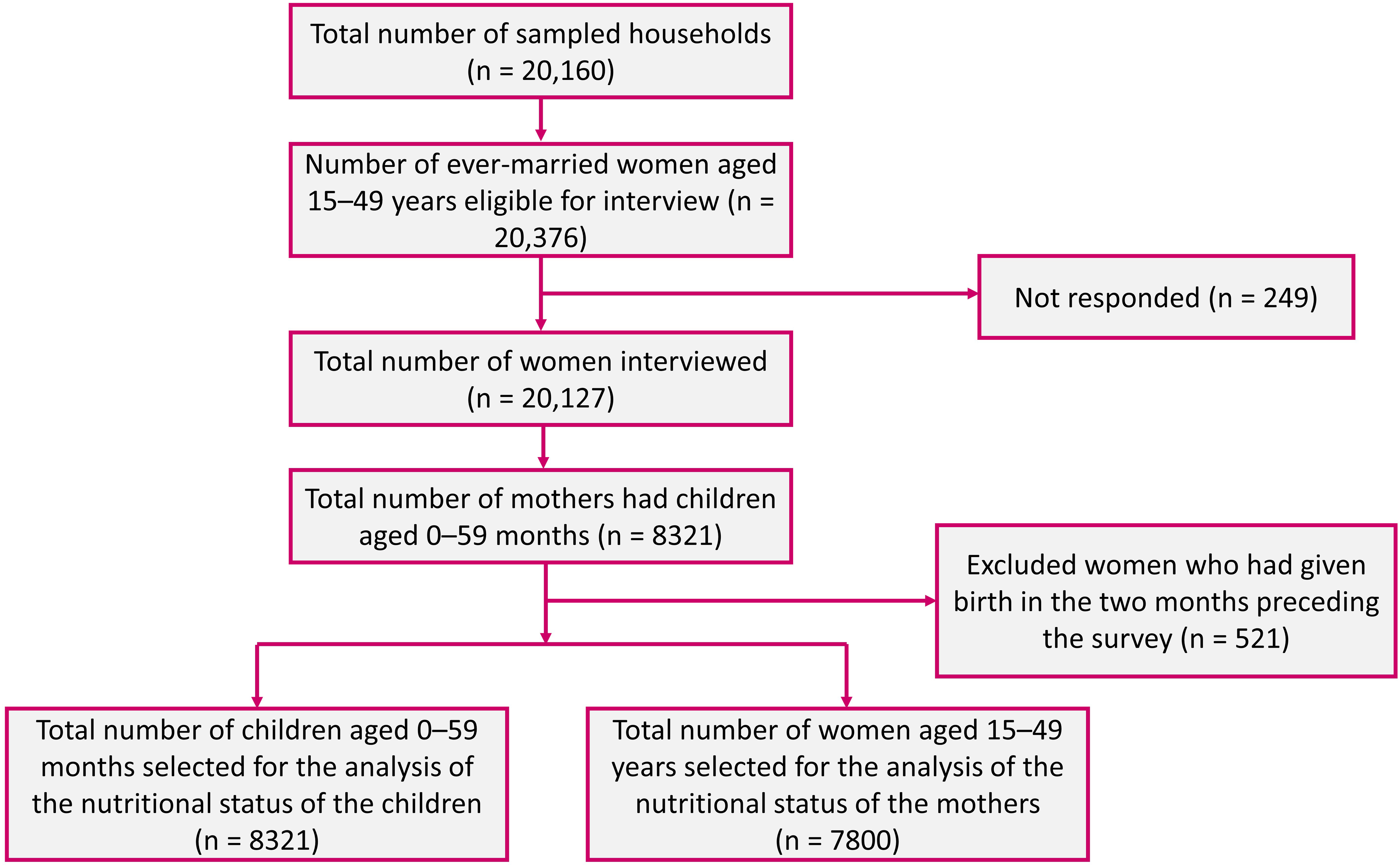
Sampling flowchart for the selection of participants.
Key outcome variables
Using WHO 2006 child growth standards, we computed three anthropometric indicators - stunting (height-for-age <−2 SD), wasting (weight-for-height <−2 SD) and overweight (weight-for-height >+2SD) as the response/outcome variables for children (World Health Organization, 2009). For women, we used underweight (BMI < 18·5 kg/m2) and overweight (BMI ≥25·0 kg/m2) (Status, 1995).
Predictor variables
The socio-economic and demographic information of the children and women were considered as independent variables. These included age, sex, birth order, mother's education (no or primary, secondary or higher), father's education (no or primary, secondary or higher), mother's BMI (underweight if BMI < 18·5 kg/m2), residence (rural, urban), division and wealth index (poor, middle, and rich). The wealth index was created using principal component analysis (PCA) based on selected household assets. The score was divided into three equal parts, with the first representing the poorest 33% of the population and the third representing the wealthiest 33%.
Statistical analyses
We used the statistical software package STATA version 15.0 to perform the data analysis. Sampling weights were applied in the analysis to obtain the nationally representative estimates. Due to the non-proportional allocation of the sample to different divisions and their urban and rural areas, sampling weights are required for any analysis employing BDHS data to ensure the actual representativeness of the survey results at both the national and domain levels. In addition, when analysing specific subpopulations within the BDHS sample, such as different age groups, weights enable accurate estimates for those subgroups by taking their proportional representation in the population into consideration. We used frequency distribution to determine the characteristics of the study participants, and percentage distribution with a 95% confidence interval (CI) to report the prevalence of nutritional status for both children (stunting, wasting, and overweight) and mothers (underweight and overweight) by background characteristics. We performed the chi-square test to explore the relationship between nutritional status and background characteristics of the participants. We reported the p-value from the chi-square test. We explored the overlapping of the nutritional status of the children using a Venn diagram. Three different multiple logistic regression models for three different outcomes of children and two different multiple logistic regression models for two different outcomes of mothers were performed to determine the factors associated with each nutritional status. We reported adjusted odds ratio (AOR) and its corresponding 95% CI from the multiple logistic regressions. The concentration curve was employed in this study to determine if any inequality exists in the area of nutritional status. If the concentration curve is located above the diagonal (line of equality at 45 degrees), this indicates that malnutrition is disproportionately concentrated among the poor, whereas if the curve is located below the line of equality, this indicates that the opposite is true.
Results
The overall prevalence of stunting, wasting, and overweight among children aged less than five years was 30.72%, 8.44%, and 2.21%, respectively (Table 1).
Percentage (%) of undernutrition (stunting and wasting) and overnutrition (overweight) by sociodemographic variables among children aged 0–59 months (n = 8321), Bangladesh, 2017–18.
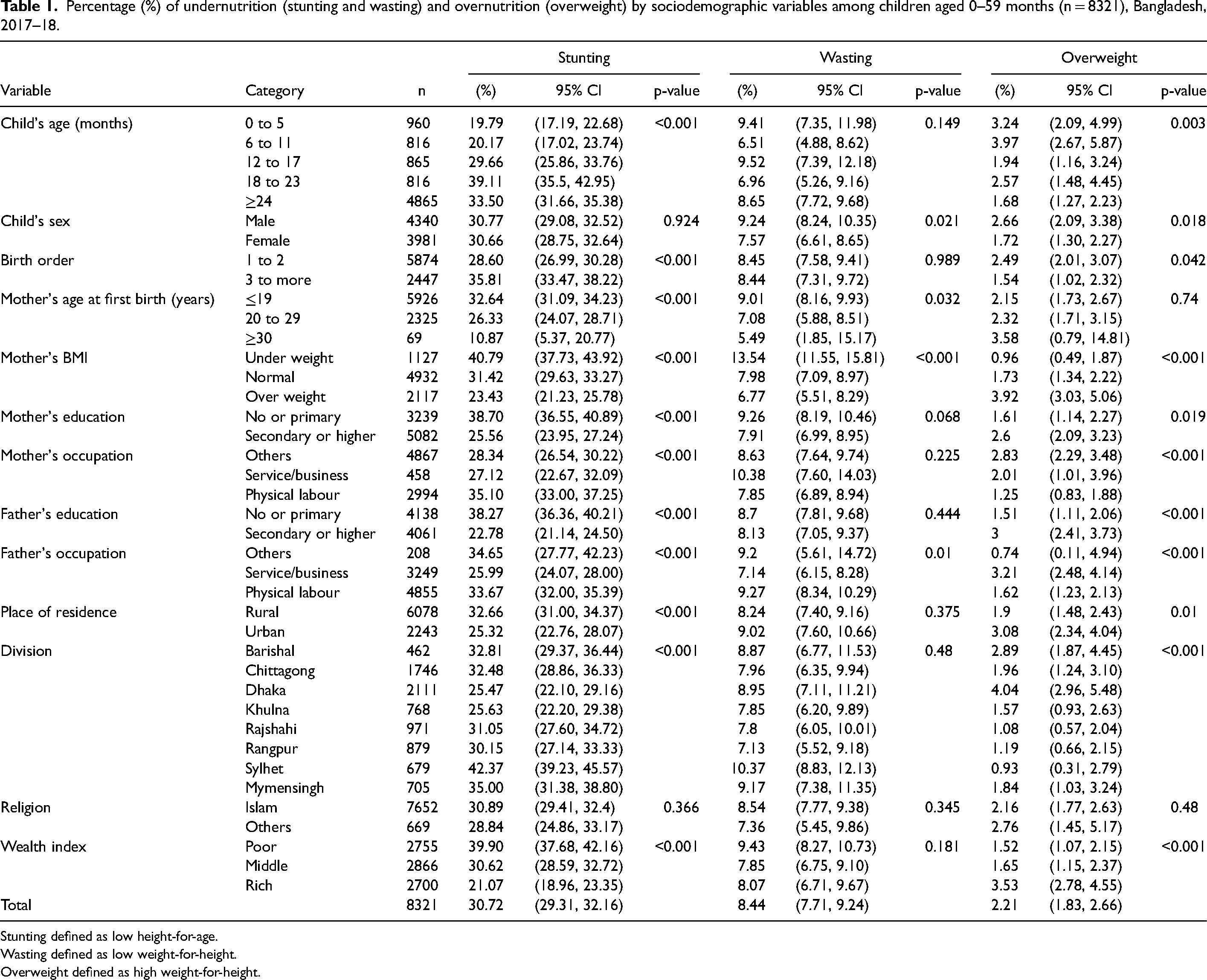
Stunting defined as low height-for-age.
Wasting defined as low weight-for-height.
Overweight defined as high weight-for-height.
Stunting was highly prevalent among children aged 18–23 months (39.11%). Male children were more affected by stunting, wasting and overweight than female children. Overweight children were reported to be higher among the overweight mothers (3.92%), mothers whose age was 30 or above at first birth (3.58%), secondary or higher educated mothers (2.6%), secondary or higher educated fathers (3%), urban area (3.08%), Dhaka division (4.04%) and rich wealth status (3.53%).
The percentages of being underweight and overweight, considering mothers aged 15–49 years were 14.09% (95% CI, 13.14–15.10) and 26.35% (95% CI, 24.92–27.82), respectively (Table 2). Adolescent mothers aged 15–19 years contributed more to being underweight (22.73%), and mothers aged 30–39 years were overweight (36.83%). A higher percentage of being underweight (15.52%) was found among the mothers whose age was 19 years or below at first birth and of being overweight (58%) for the mothers whose age was 30 years or above at first birth. Undernourished mothers (20.81%) were more prevalent in families with poor wealth status, and overweight mothers (42.89%) were more prevalent in families with rich wealth status.
Percentage (%) of underweight and overweight by sociodemographic variables among mothers aged 15–49 years (n = 7800), Bangladesh, 2017–18.
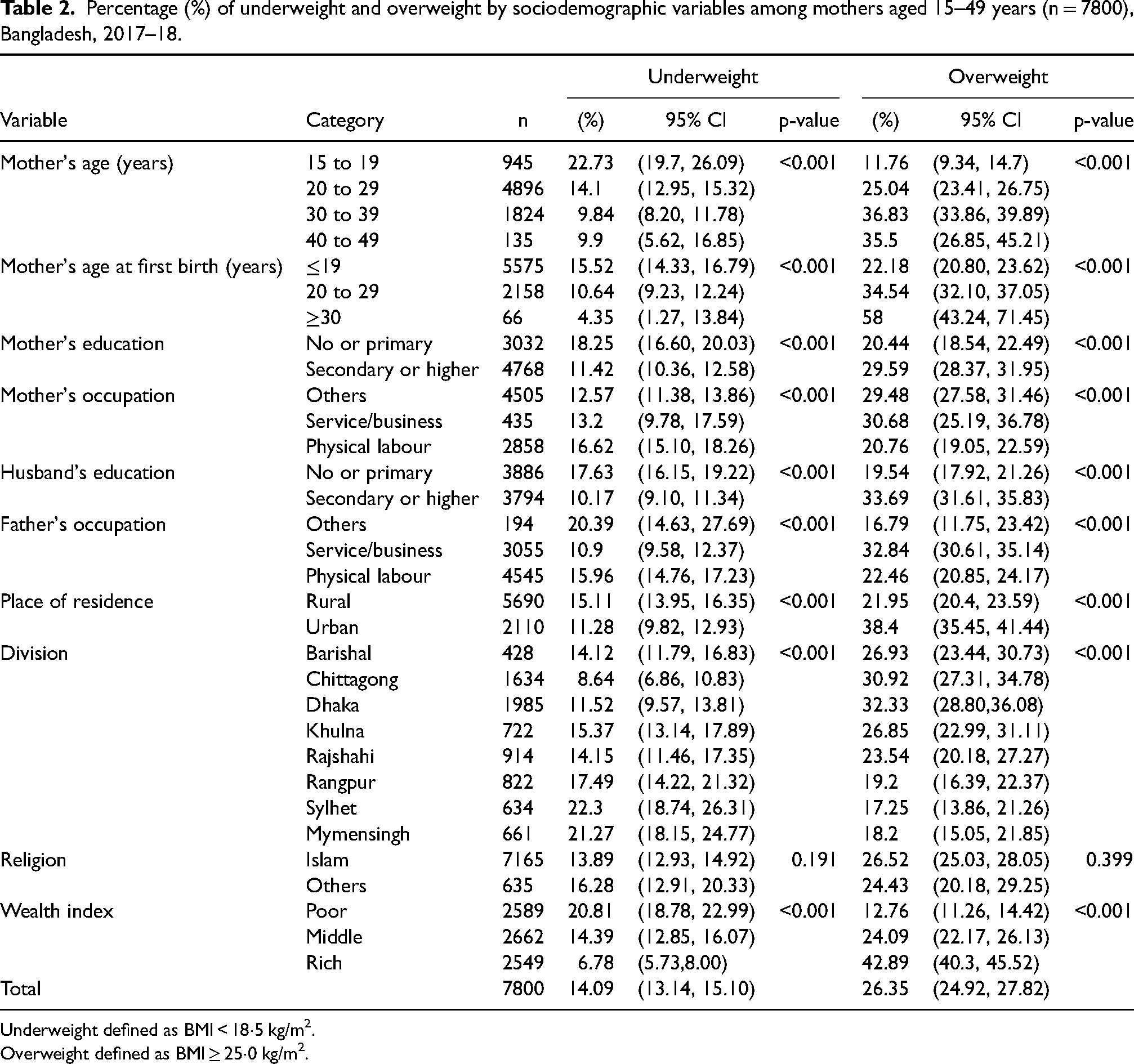
Underweight defined as BMI < 18·5 kg/m2.
Overweight defined as BMI ≥ 25·0 kg/m2.
Table 3 shows that mothers’ BMI status, education, fathers’ education and wealth index are associated with children being stunted, whereas child's sex and mothers’ BMI status are associated with wasting. On the other hand, a child's sex and birth order are associated with children being overweight.
Adjusted associations between undernutrition (stunting and wasting) and overnutrition (overweight) and sociodemographic variables among children aged 0–59 months, Bangladesh, 2017–18.
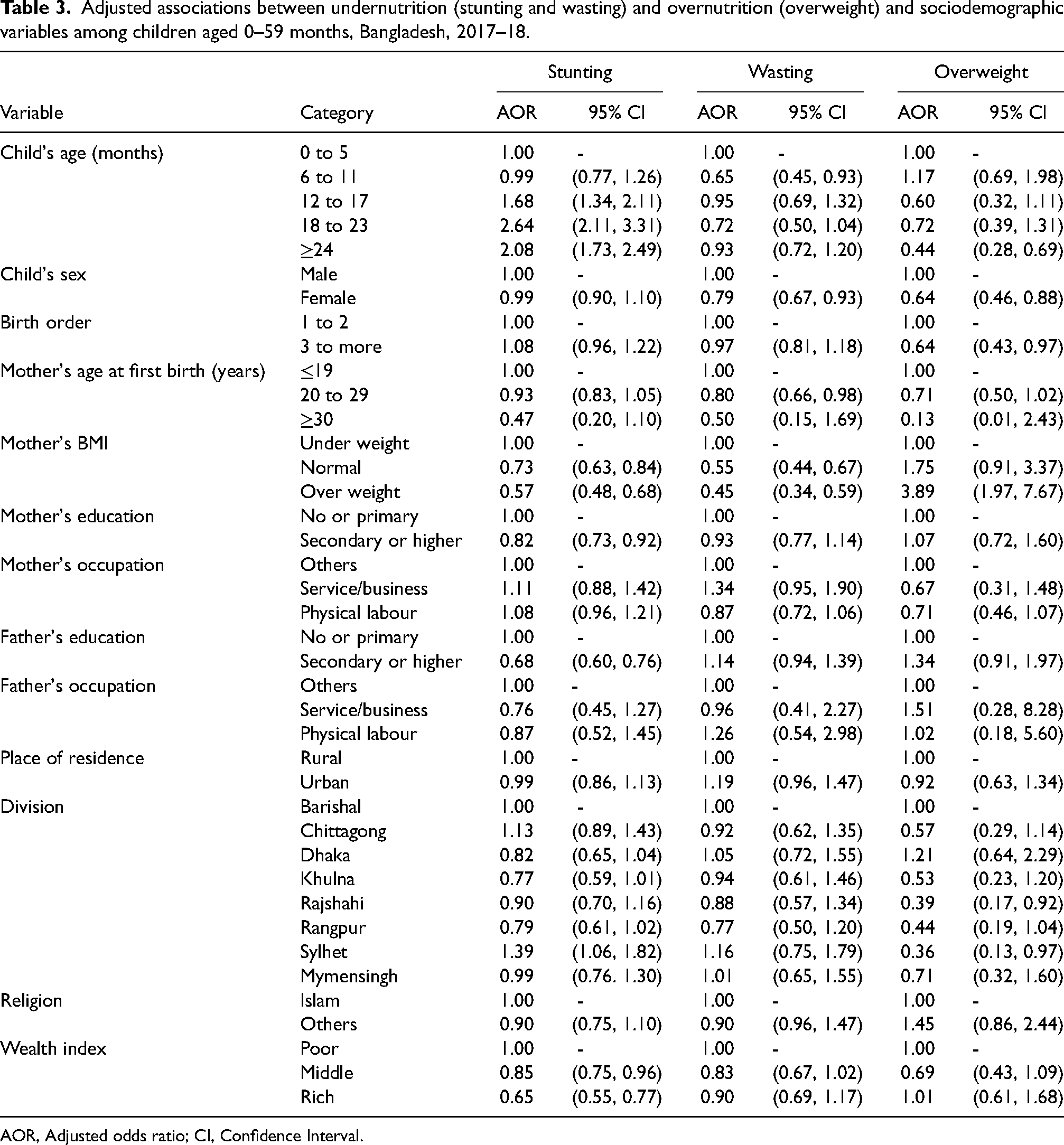
AOR, Adjusted odds ratio; CI, Confidence Interval.
Children aged 18–23 months were 2.64 times (95% CI: 2.11–3.31) more likely to be stunted compared to children aged 0–5 months. Female children were less likely to be stunted (AOR: 0.99, 95% CI: 0.90–1.10), wasted (AOR: 0.79, 95% CI: 0.67–0.93), and overweight (AOR: 0.64, 95% CI: 0.46–0.88) than male children. Children with birth order three or more were less likely to be overweight (AOR: 0.64, 95% CI: 0.43–0.97) than the children with birth order two or below. For the children below five years, the less likelihood of being stunted, wasted and overweight were found in mothers whose age were 20–29 years as well as 30 years or more at first birth compared to mothers whose age were 19 years or below at first birth. The less likelihood of being stunted (AOR: 0.57, 95% CI: 0.48–0.68) and wasted (AOR: 0.45, 95% CI: 0.34–0.59) was observed for children with overweight mothers compared to underweight mothers, whereas a higher likelihood of being overweight (AOR: 3.89, 95% CI: 1.97–7.67) were found. Children with secondary or higher educated mothers and fathers were less likely to be stunted compared to children with no or primary educated mothers and fathers. Children from the Sylhet division were more likely to be stunted (AOR: 1.39, 95% CI: 1.06–1.82) as well as wasted (AOR: 1.16, 95% CI: 0.75–1.79), whereas children from Dhaka division were more likely to be overweight (AOR: 1.21, 95% CI: 0.64–2.29) compared to Barishal division. Children with rich class families were less likely to be stunted (AOR: 0.65, 95% CI: 0.55–0.77) and wasted (AOR: 0.90, 95% CI: 0.69–1.17), whereas were more likely to be overweight (AOR: 1.01, 95% CI: 0.61–1.68) compared to children from poor class families.
Table 4 indicates that mothers’ age, mothers’ education, fathers’ education, place of residence and wealth index are significant determinants for mothers being underweight, whereas mothers’ age, mother's occupation, father's education, father's occupation, place of residence and wealth index are significant determinants for mothers being overweight.
Adjusted associations between undernutrition and overweight and sociodemographic variables among mothers aged 15–49 years, Bangladesh, 2017–18.
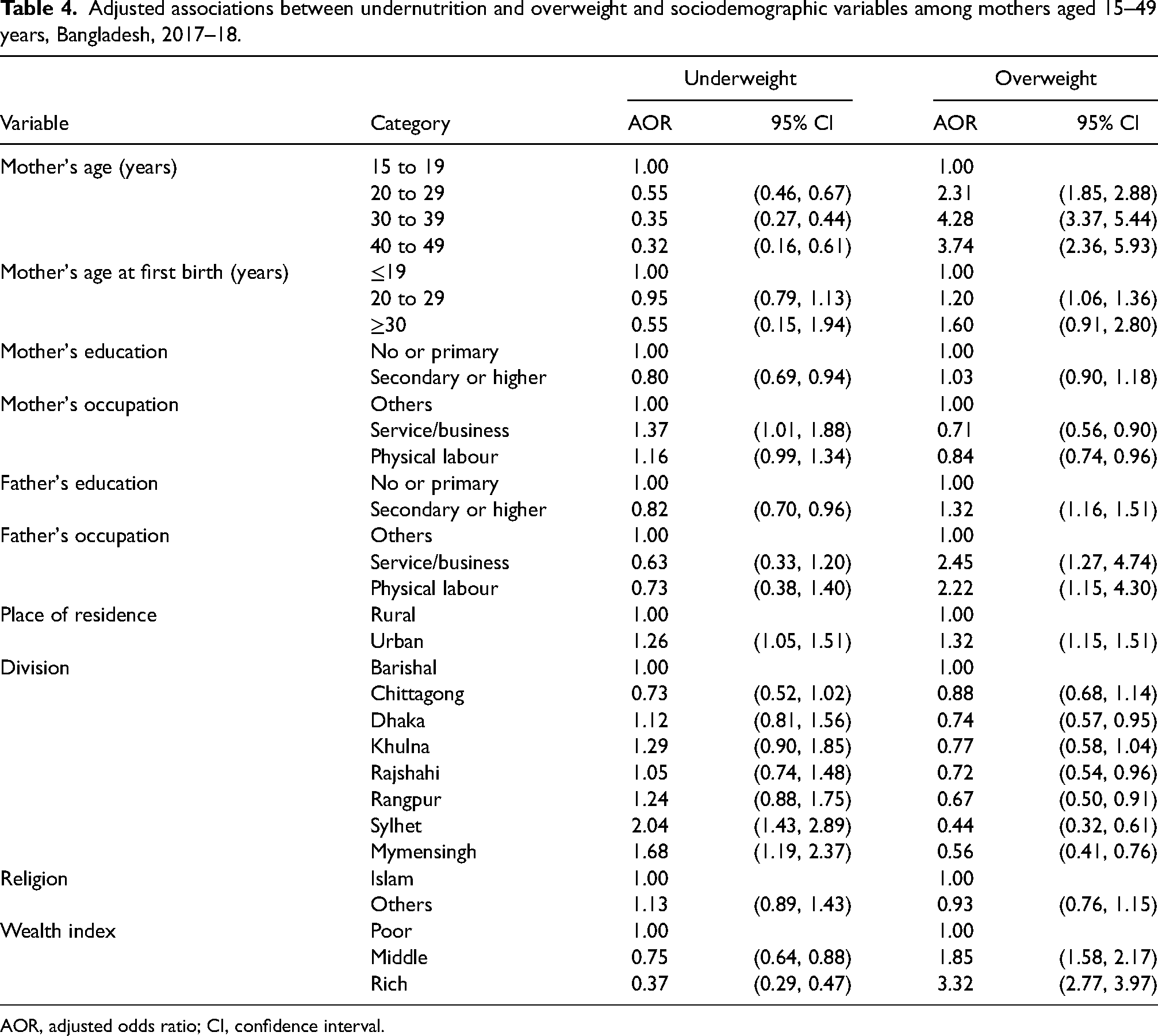
AOR, adjusted odds ratio; CI, confidence interval.
The likelihood of being underweight was decreasing as mothers’ age increased. Mothers aged 40–49 years were less likely to be underweight (AOR: 0.32, 95% CI: 0.16–0.61) and more likely to be overweight (AOR: 3.74, 95% CI: 2.36–5.93) compared to mothers aged 15–19 years. Mothers with secondary or higher education were less likely to be underweight (AOR: 0.80, 95% CI: 0.69–0.94) compared to mothers with no or primary education. Mothers were less likely to be underweight whose husbands were with secondary or higher education compared to no or primary education and more likely to be overweight. Mothers were less likely to be overweight whose occupation was physical labour (AOR: 0.84, 95% CI: 0.74–0.96) than the mothers from others categories. On the other way around, mothers were more likely to be overweight whose husband's occupations as physical labour (AOR: 2.22, 95% CI: 1.15–4.30) than the husbands from others categories. Mothers from urban areas were more likely to be both underweight and overweight than the mothers from rural areas. Mothers from the Sylhet division were more likely to be underweight (AOR: 2.04, 95% CI: 1.43–2.89) compared to the mothers from the Barishal division. Mothers from rich-class families were less likely to be underweight (AOR: 0.37, 95% CI: 0.29–0.47) and more likely to be overweight (AOR: 3.32, 95% CI: 2.77–3.97) compared to the mothers from poor class families.
Supplementary Figure 1 shows that no children had a combination of three indicators (stunting, wasting and overweight). The percentage of being only stunted, wasted and overweight were 27.31, 5.56 and 1.64, respectively. About 2.74% of the children were both stunted and wasted, while 0.56% of the children were both stunted and overweight.
Economic inequality in maternal and child malnutrition
The concentration curves for each of the malnutrition indicators (stunting, wasting for children and underweight for mothers) are all placed over the line of equality indicating that a disproportionately high prevalence of malnutrition exists among the poor segment of the population (Figure 2(a)). On the other hand, the curve for overweight is below the line of equality, which indicates that those with the most wealth have a significant high prevalence of overweight (Supplementary Table 1).

Concentration curves for nutritional status of children (a) and mother (b).
In consideration of the nutritional status of the mother, the concentration curve for the underweight indication is above the line of equality, whereas it is below the line of equality for the overweight indicator (Figure 2(b)). The poor have a disproportionately significant high prevalence of being underweight, whereas a significant high prevalence of being overweight is concentrated among the rich (Supplementary Table 2).
Discussion
Child's malnutrition
In developing countries like Bangladesh, maternal and child malnutrition is considered a paramount public health issue. This study explored the prevalence of maternal and child malnutrition using the recent BDHS 2017–18 data. The findings revealed that in 2017–18, 31% of children under the age of five were stunted, 8% were wasted, and 2% were overweight. The prevalence rate of stunting (36%) and wasting (14%) was considerably lower, but the prevalence rate of overweight (1.5%) was slightly higher than the previous study conducted in Bangladesh in 2014 (Mia et al., 2018). The findings also showed that in 2017–18, 14% and 26% of mothers were under- and over-weight, respectively. The prevalence of underweight (22%) was higher, and the prevalence of overweight (18%) was lower in 2014 (Mia et al., 2018). Our findings suggest that the prevalence of overweight and obesity is rising among Bangladeshi mothers and children, and similar findings were also reported in a previously published review article (Banik and Rahman, 2018). In this study, the gender and birth order of children, BMI status of the mother, educational status of parents, place of residence, and wealth index have a significant association with child's nutritional status. Whereas mothers’ age, mother's education and occupation, father's education and occupation, place of residence and wealth have a significant association with maternal nutritional status.
In the analysis, stunting of children was significantly associated with increased age of them, underweighted mother, no/primary school educated mother, no/primary school educated father, living in Sylhet, and poor wealth index; wasting was correlated with lower age of children, being male, mother first birth ≤19 years, and underweighted mother; whereas, overweight was associated with male gender, and having birth order between 1–2, as well as children living in Sylhet Division, were less likely to have overweight.
Among mothers, underweight was associated with lower age (15–19 years), no/primary educated mother, mother occupation (service/business), no/primary educated father, living in the urban area, and poor wealth index; whereas overweight was correlated with increased age, having mother occupation (others), father education (secondary or higher), father occupation (service/business and Physical labour), living in urban areas, living in Barishal, and wealth index (middle and rich).
Stunting was positively increased with children's age in the present study, which is concurrent with the previous studies conducted in Bangladesh (Das and Gulshan, 2017; Sultana et al., 2019; Talukder, 2017) and it's neighbouring counties (e.g., India, Nepal, China) (Meshram et al., 2012, Ruwali, 2018) as well as Sierra Leone (Sserwanja et al., 2021). A possible reason could be the discontinuation of breastfeeding and the provision of additional foods. After six months, the children are fed additional foods along with breast milk, increasing the likelihood of contaminated food intake and increasing communicable diseases among children by age (Hong et al., 2006). Thus, the policymakers should focus on children's age to design any specific interventions to reduce stunting among under-five children.
In the present study, male children were more likely to have dual malnutrition (e.g., wasting, overweight) than female children, which is consistent with the previous studies (Das and Gulshan, 2017; Meshram et al., 2012). Stunting was not associated with gender in the present study, which is in line with an earlier Bangladeshi study (Sultana et al., 2019). The children with secondary or higher education were less likely to have stunting compared to those with no/ primary education. This finding is similar to the previous studies in Bangladesh and other regions (Jesmin et al., 2011; Rahman et al., 2015). This is reasonable because the father's education is crucial for his children's health and nutritional status because of their participation in household income and his involvement in decision-making for selecting food for the family. On the other hand, educated mothers also have a higher understanding regarding the health and nutrition of their children, enhanced child care, utilization of health services, hygiene and sanitation, etc. (Das and Gulshan, 2017).
Wasting and stunting were more likely to happen among children with underweighted mothers compared to those not underweight. This finding corroborates the previous reports (Khan and Raza, 2014). This demonstrates that mothers’ nutritional status has a significant impact on the nutritional status of their offspring. A systematic review also concluded that maternal autonomy improves the nutritional status of children (Carlson et al., 2015). Thus, maternal nutrition needs to be taken into consideration while designing any nutritional interventions for under-five children.
In the present study, the children living in Sylhet Division were more likely to be stunted and less likely to be overweight compared to the children living in the other areas. A previous study also revealed that the Sylhet Division lags substantially behind the other Divisions of Bangladesh in terms of controlling children's malnutrition (Das and Gulshan, 2017). The children with a poor wealth index exhibited more stunted compared to those with a middle/ rich wealth index in the present study. This is consistent with previous findings (Janevic et al., 2010; Khor and Sharif, 2003). Thus, living areas and wealth index should be taken into consideration while designing any nutritional interventions for the under-five children in Bangladesh.
Mother's malnutrition
In the regression analysis, age was significantly associated with both being underweight and overweight. Being underweight was associated with younger age, and being overweight was associated with older age of women. The finding is consistent with the previous studies (Hashan et al., 2020; Khanam et al., 2021). This may be attributed to the lack of physical activity and the increased consumption of energy-rich meals in old age, resulting in obesity (Alemu et al., 2014). Furthermore, body fat rises, and fat-free mass declines are possible in women over 30 years old (Gallagher et al., 1997).
Underweight and overweight were significantly associated with the educational status of mothers and their husbands in the present study. The odds of being underweight were significantly higher among participants with no/primary education and having husbands with no/primary education. In addition, the odds of being overweight were higher among participants’ husbands with higher education. The findings are concurrent with the previous reports (Hashan et al., 2020; Khanam et al., 2021). This is reasonable because educated women tend to work in sedentary occupations that require long periods of sitting or standing, increasing their risk of obesity (Hu et al., 2003). Because of their contribution to household income and engagement in decision-making for picking food for the family, the father's education is critical for the family's health and nutritional status (Das and Gulshan, 2017). Moreover, Baecke et al. also revealed that while educational status positively influences leisure time, it negatively affects habitual physical activity (Baecke et al., 1982).
We found that women from urban regions had increased odds of being underweight and overweight compared to rural areas. Moreover, regional differences were also observed among women living in Dhaka, Rajshahi, Rangpur, Sylhet, and Mymensingh Divisions showed a greater likelihood of being overweight than those who resided in the Barishal Division. The findings corroborate with the prior reports (Kamal, 2021). Thus, geographical location should be considered when designing any nutritional intervention for women in Bangladesh.
In this study, we observed that the mothers with a poor wealth index were more likely to be underweight, while overweight women obtained higher middle and rich wealth indexes. The finding supports the earlier research, which also demonstrated the higher prevalence of overweight among women from households with a higher household wealth index and a higher prevalence of underweight among those with a lower household wealth index (Kamal et al., 2015; Sarma et al., 2016). People from higher-income households simply have more money to purchase food, have a sedentary lifestyle and require less work, and live in a more affluent place where there is better food security which may predispose individuals to overweight/obesity (Ogden et al., 2014).
Strengths and limitations
Our analysis has several strengths. Firstly, the study was analyzed using the rich BDHS data, which is a nationally representative survey with large sample size and an adequate response rate. Secondly, the BDHS dataset covers a wide geographic area of Bangladesh, encompassing all divisional areas through face-to-face interviews using a standard sampling technique.
However, the study also has some limitations, which should be acknowledged when interpreting the findings. Firstly, as it was a cross-sectional design, the causal relationship cannot be explained. Secondly, as the data were acquired from the BDHS, the study did not include the compressive factors connected to the malnutrition of the children and mothers due to the specific information given by the BDHS.
Conclusion
We found that certain socio-economic and demographic factors and characteristics related to children and mothers are associated with malnutrition among Bangladeshi children and women. Strategies to eradicate poverty, enhance mothers’ nutritional and educational status, and facilitate better access to primary healthcare facilities are required to lessen the emerging burden of maternal and child malnutrition in such a low-resource country.
Supplemental Material
sj-docx-1-nah-10.1177_02601060231200521 - Supplemental material for Contribution of socio-economic and demographic factors to maternal and child malnutrition in Bangladesh: Insights from a nationwide survey
Supplemental material, sj-docx-1-nah-10.1177_02601060231200521 for Contribution of socio-economic and demographic factors to maternal and child malnutrition in Bangladesh: Insights from a nationwide survey by Abu Sayeed, Ema Akter, Promit Barua Chowdhury and Md. Saiful Islam, Mst. Sadia Sultana, Nowrin Nusrat, Lubna Hossain, Rita Karmoker, Ritu Rana, Manika Saha, M. Tasdik Hasan in Nutrition and Health
Footnotes
Acknowledgments
The authors would like to acknowledge DHS (Demographic and Health Surveys) who has made their data available for free.
Author’s contribution
AS: conceptualisation, methodology, and writing – original draft; EA: formal analysis and writing – original draft; PBC: formal analysis; MSI, MSS, NN, LH, RK: writing – original draft; RR, MS, MTH: review, editing and validation.
Availability of data and materials
On reasonable request made to the corresponding author, all data will be made available.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.