
Abstract
Study purpose: this study aims to analyze QOL and psychosocial impact on patients with blood disorders. Methods: A cross-sectional survey design is adopted in this study. The survey questionnaire included SF-36 form for measuring quality of life (QOL), along with psychosocial impact assessment scale. Adult patients with different types of blood disorders were recruited for the survey. Out of the 417 responses received, 389 were considered for data analysis and the remaining were avoided due to incomplete data. Results: In terms of psychosocial impact scales, the highest mean is observed for financial stress (4.09 ± 1.22), followed by social exclusion (3.76 ± 1.19) and relationship challenges (3.31 ± 1.18). Among the QOL scales, the highest mean was observed for pain (3.81 ± 1.17), followed by physical functioning (3.68 ± 1.12). Statistically significant differences (p < 0.05) were observed among the participants groups characterized by age and type of disorder. Strong positive correlations between social exclusion and general health (r = 0.513), as well as pain and relationship challenges (r = 0.735) were observed. Conclusion: Given the existing challenges in social exclusion, poor awareness, and support there is a need to develop comprehensive and personalized treatment plans integrating physical and mental support, awareness creation, and financial support.
Introduction
Blood disorders encompass a diverse range of medical conditions that affect the proper functioning of blood components, such as red blood cells, white blood cells, platelets, and plasma. There are several types of blood disorders. For instance, diseases like anemia, thalassemia, and Polycythemia vera are caused due to red blood cell disorders; diseases like leukemia, lymphoma, multiple myeloma are caused due to white blood cell disorders; and diseases like hemophilia, primary thrombocythemia, acquired platelet function disorder are caused due to platelet disorders (Metropolis, 2024; National Institute of Diabetes and Digestive and Kidney Diseases, 2024). Although symptoms vary for each disorder, common symptoms include fatigue, tiredness, prone to multiple infections, which may significantly affect the quality of life (QOL) of the patients with blood disorders (Blaauwgeers et al., 2019; Caocci et al., 2012; Karimi et al., 2015; Talaulikar et al., 2006; Von Mackensen, 2011). Studies have observed significant impact on QOL of patients with blood disorders, which included sleep disorders, employment/work, pain, depression and anxiety, lack of support, decreased physical functioning, limitations in daily activities due to physical health problems, limitations in social activities, decreased energy levels, and lower general health status (Kadir, Edlund and Von Mackensen, 2010; Mougianis et al., 2020; Pereira et al., 2013; Schipper et al., 2021; Solovieva et al., 2004). It has been observed that blood disorders have affected both physical and mental well-being of the patients, reflecting a reduced health-related quality of life compared to the general population (Mehic et al., 2023). It is also emphasized that blood disorders not only affect physical dimensions, but also, functional, role, psychological, and psychosocial dimensions in patients life (Allart-Vorelli et al., 2015).
Due to the array of effects of blood disorders significant impact on psychosocial aspects has been observed. Psychosocial costs represent a large part of the overall burden of blood disorders. Research findings indicate that most families experience adverse effects following receiving a diagnosis. These effects include disturbances in family interactions, a variety of negative emotions in the patient such as despair, despondency, and impatience, as well as challenges in maintaining social relationships. Furthermore, they document adverse consequences in the sibling-parent relationship and the caregiver's spouse/partner relationship, as well as a deterioration in the financial situation of the primary caregiver (Borrescio-Higa and Valdes, 2022). Further analysis in a recent study (Knisely et al., 2020) revealed significant associations between QOL factors and psychosocial factors. It was observed that pain due to blood disorders was associated with age, education, employment, time since last pain attack, hydroxyurea use, opioid use, sleep impact, social functioning, and cognitive functions; sleep impact was associated with household income, opioid use, pain impact, social functioning, depressive symptoms, and tiredness; and social functioning was associated with employment, pain attacks, symptoms, tiredness, and cognitive functions. Furthermore, external factors like Covid-19 pandemic added to the woes of already affected patients, further elevating the impact (Zeiler et al., 2022). A recent study (Woodman et al., 2023) has observed significant impact of blood disorders on children, leading to increased levels of depression, stress, anxiety, emotional and conduct problems, hyperactivity, and pro-social behavior. Lack of awareness about blood disorders, especially in early diagnosis, symptoms identification; and lack of comprehensive treatment plans covering both physical and mental treatments were identified to be the major reasons for increasing effects of blood disorders on QOL and psychosocial aspects (Drouin et al., 2023).
A recent study (AbuAlhommos et al., 2022) assessed the quality of life of type 2 diabetic patients in Saudi Arabia and found that pain/discomfort, mobility, and depression and anxiety as the common effects that affected QOL. Another study (Khaled et al., 2020) on the patients with sickle cell disease observed that the disorder had a negative effect on physical and mental health of the patients. However, exercise and family support positively affected QOL. A similar study (Alzahrani et al., 2021) with sickle cell disease patients also found that psycho-social aspects like parental and marital support had a positive impact on QOL. Furthermore, a recent study (Altwaijri et al., 2023) in Saudi Arabia found that the prevalence of a mental disorder among Saudi youth was 40.10%, where anxiety disorders affected 26.84% of the sample, followed by disruptive behavior disorders (15.44%), mood disorders (9.67%), substance use disorders (4%) and eating disorders (7.06%). Furthermore, stress and anxiety were most common aspects identified in various studies (Al-Sayed et al., 2020). Given these conditions, the association between QOL and psycho-social aspects is an important aspect that need to be further explored among the individuals in different conditions and contexts.
Most of the previous studies discussed above were focused on specific disorder, lacking a comprehensive understanding on the impact of blood disorders. Furthermore, the associations between QOL and psychosocial factors are not clearly understood among the researchers (Knisely et al., 2020). Research on the impact of blood disorders on quality of life and psychosocial aspects holds significant implications for patient care and well-being. By analyzing the psychosocial dimensions of these conditions, healthcare professionals can enhance patient-centered care, tailoring treatment plans to address not only the physical symptoms but also the emotional and social challenges faced by individuals. This approach is crucial for optimizing treatment outcomes and improving overall patient satisfaction. Moreover, understanding the psychosocial impact allows for the development of more targeted interventions, aiding in the design of comprehensive strategies that address both the medical and emotional aspects of blood disorders. Such research is pivotal for allocating resources effectively and ensuring a holistic approach to healthcare that considers the broader implications of these conditions on patients’ lives. Therefore, this study aims to analyze QOL and psychosocial impact on patients with blood disorders.
Methods
A cross-sectional survey design is adopted in this study.
Study setting & participants
As the study is focused on blood disorders, patients with various types of blood disorders such as Anemia, Leukemia, Hemophilia, Sickle Cell Disease, Thalassemia, and other major blood-related disorders were considered for this study. Participants included outpatients (18 years or above) from the hospital at King Fahad University, Saudi Arabia. The hospital was selected based on its comprehensive blood disorder treatment programs and its diverse patient population, providing a representative sample for our study. During outpatient visits, the patients were requested to participate in the research while the purpose and objectives were explained. Patients were instructed, with their consent, to undertake the online survey, at their convenience, within the specified time-period of four weeks.
Selection and sampling
As the study required patients with blood disorders, it was imperative that the researchers use a readily accessible sample. Consequently, both purposive and convenience sampling techniques were used in this study, as was customary for comparable research (Bonsu and Baffour-Koduah, 2023). Purposive sampling was used for selecting participants based on their existing conditions related to blood disorders; and convenience sampling was used to recruit individuals who can be easily accessed, i.e., from university hospital. The estimated sample size was calculated using Cochran's formula (Ahmad and Halim, 2017), which is identified to be 383, and the post-hoc power analysis resulted in 100% power. When 462 adult patients were initially asked if they were interested in participating in the study, 435 responded positively. Consequently, 435 patients were selected to participate in the study to whom, the survey link was sent through email and social media applications. Before participating in the survey, the patients were thoroughly informed of the study's objectives and given the opportunity to provide informed consent during their outpatient visit.
Questionnaire design
In this study, a descriptive quantitative cross-sectional survey design was adopted. The demographic part of the questionnaire includes items: age, gender, education, type of disorder (Independent variables). The survey questionnaire includes pre-validated survey questionnaire SF-36 for measuring QOL (dependent variables) (Azzizadeh et al., 2015), including physical functioning, role limitations due to physical health, role limitations due to emotional problems, energy/fatigue, emotional well-being, social functioning. pain, and general health factors. By assessing general health, insights into patients’ overall perceptions of their health status can be gained. The pain scale enables in understanding the severity and impact of pain, a common symptom in blood disorders. Social functioning can evaluate the extent to which health issues interfered with patients’ social activities and relationships. Emotional well-being can assess the mental health aspects, including feelings of anxiety and depression. The energy/fatigue scale can provide information on patients’ vitality and levels of tiredness. Role limitations due to emotional problems and physical health can explore how these factors restricted daily activities and responsibilities. Finally, physical functioning can assess the ability to perform physical activities. Together, these scales provided a holistic view of how blood disorders affect patients’ lives, highlighting the multifaceted challenges they face and the need for integrated care approaches that address both physical and psychosocial aspects.
The second part of the questionnaire focuses on psychosocial impact (dependent variables) encompassing areas such as social exclusion, access to treatment, financial stress, workplace or educational support, discrimination, social understanding, comfort seeking support, relationship challenges, future uncertainties, and awareness of available resources, which were adopted from previous studies (Drouin et al., 2023; Knisely et al., 2020; Woodman et al., 2023; Zeiler et al., 2022). The rating scale for all the questions was adjusted to five-point Likert scale ratings. The survey questions were then translated from English to Arabic by a qualified translator (Cha et al., 2007). Two professors from the eHealth department at Imam Abdulrahman Bin Fahd University certified the translated questionnaire. A few grammatical adjustments were suggested, and the Arabic version was revised to incorporate them. A pilot study was undertaken with a sample of 14 patients, and subsequent analysis was performed on the collected data. The Cronbach alpha coefficient was computed for all items and found to exceed 0.7 suggesting good internal consistency and reliability (Taber, 2018).
Data collection
In order to collect information, a questionnaire survey was designed with Google Forms, and it was distributed online through emails and social media platforms to patients. Out of the 435 patients, who received the survey link, 417 patients participated in the survey. However, 19 respondents did not fully complete the survey, and were removed from the data used for analysis. Therefore, a final sample of 398 was considered for data analysis.
Data analysis
To attain the objectives of the research, the researcher utilized the statistical package for the Social Sciences (SPSS, IBM Version 24) for analyzing the data. Descriptive statistics will be used to characterize the participants’ demographic data. In addition, two-sample t-test with unequal variances, and single factor ANOVA were used for analyzing the data. Furthermore, Person correlation coefficients were used for comparing relationship between various factors.
Ethics-related factors
The research ethics committee at Abdulrahman Bin Faisal University approved the study. The data collection and analysis process were conducted in accordance with all applicable ethical standards. The purpose of the investigation and the participants’ legal rights were disclosed in full. Before the survey, all participants gave their informed consent, and participation was entirely voluntary.
Results
The survey includes data from 398 participants (see Table 1), with a breakdown of demographics based on age, gender, education, and type of disorder. In terms of age, the majority falls within the 18–24 range, comprising 34.4% of the participants, followed by 25–34 (25.4%), 35–44 (19.8%), 45–54 (14.3%), and >54 (6.0%). Gender distribution shows 58.5% males and 41.5% females. Education levels vary, with 5.3% uneducated, 14.1% having primary/secondary education, 38.7% holding a diploma, 26.1% having a bachelor's degree, and 15.8% having a master's degree. Regarding the type of disorder, the survey covers various conditions, with anemia being the most prevalent at 28.9%, followed by leukemia (19.3%), others (35.4%), sickle cell disease (5.3%), hemophilia (6.3%), and thalassemia (4.8%).
Participants demographics.
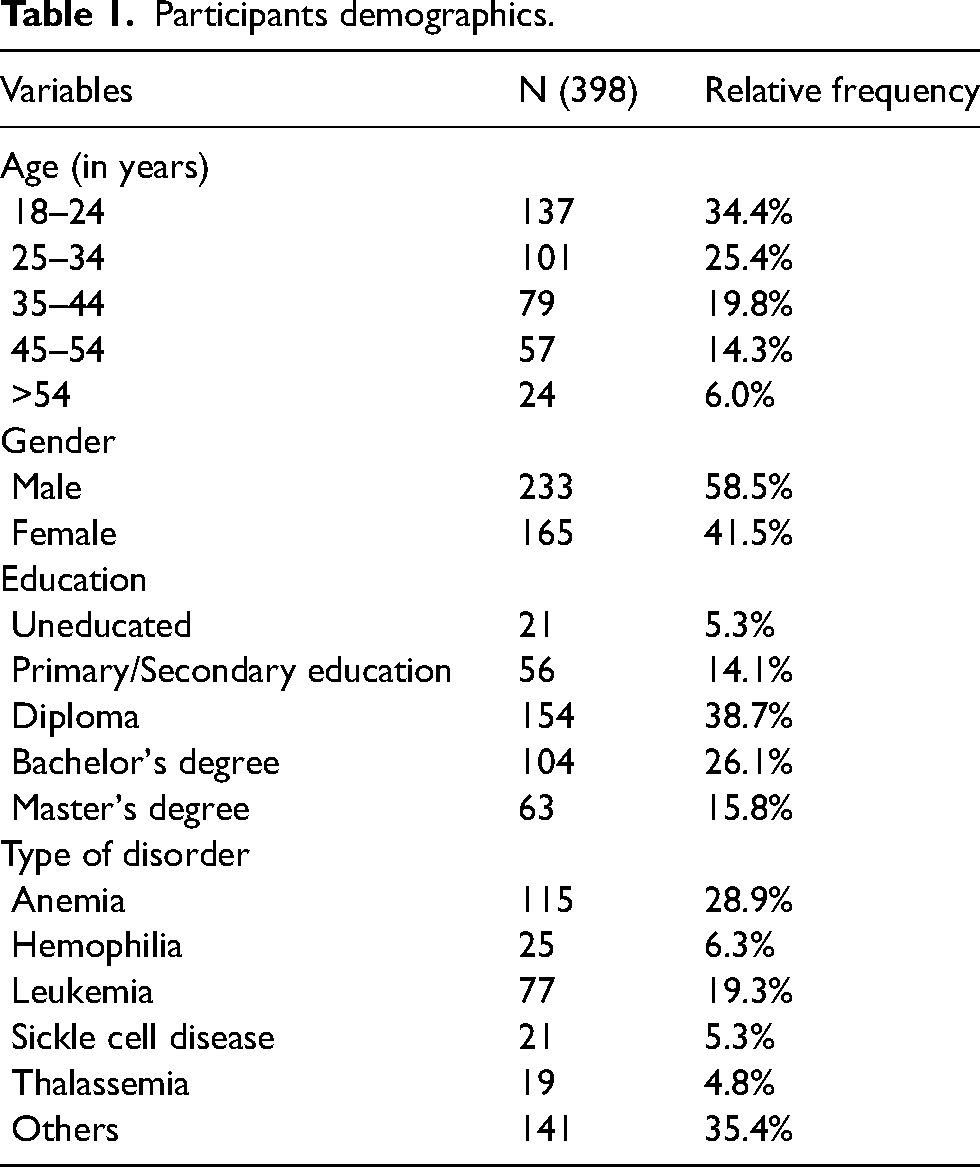
Table 2 presents mean and standard deviations for psychosocial impact scales and quality of life (QOL) scales measured on a rating scale of 1 to 5 for patients with blood disorders. In terms of psychosocial impact scales, the highest mean is observed for financial stress (4.09 ± 1.22), indicating significant perceived stress in this aspect. Social exclusion (3.76 ± 1.19) and relationship challenges (3.31 ± 1.18) also show notable impacts. Among the QOL scales, the highest mean is for pain (3.81 ± 1.17), suggesting a considerable negative impact on patients’ well-being. General health (3.17 ± 1.12) and emotional well-being (2.81 ± 0.81) also have moderate to high means. The standard deviations across scales indicate variability in responses, emphasizing the diverse experiences within the patient population. These findings underscore the multifaceted challenges faced by individuals with blood disorders, encompassing social, financial, and health-related aspects, and highlight the need for comprehensive support and interventions to enhance their overall quality of life.
Psychosocial impact and QOL scales.
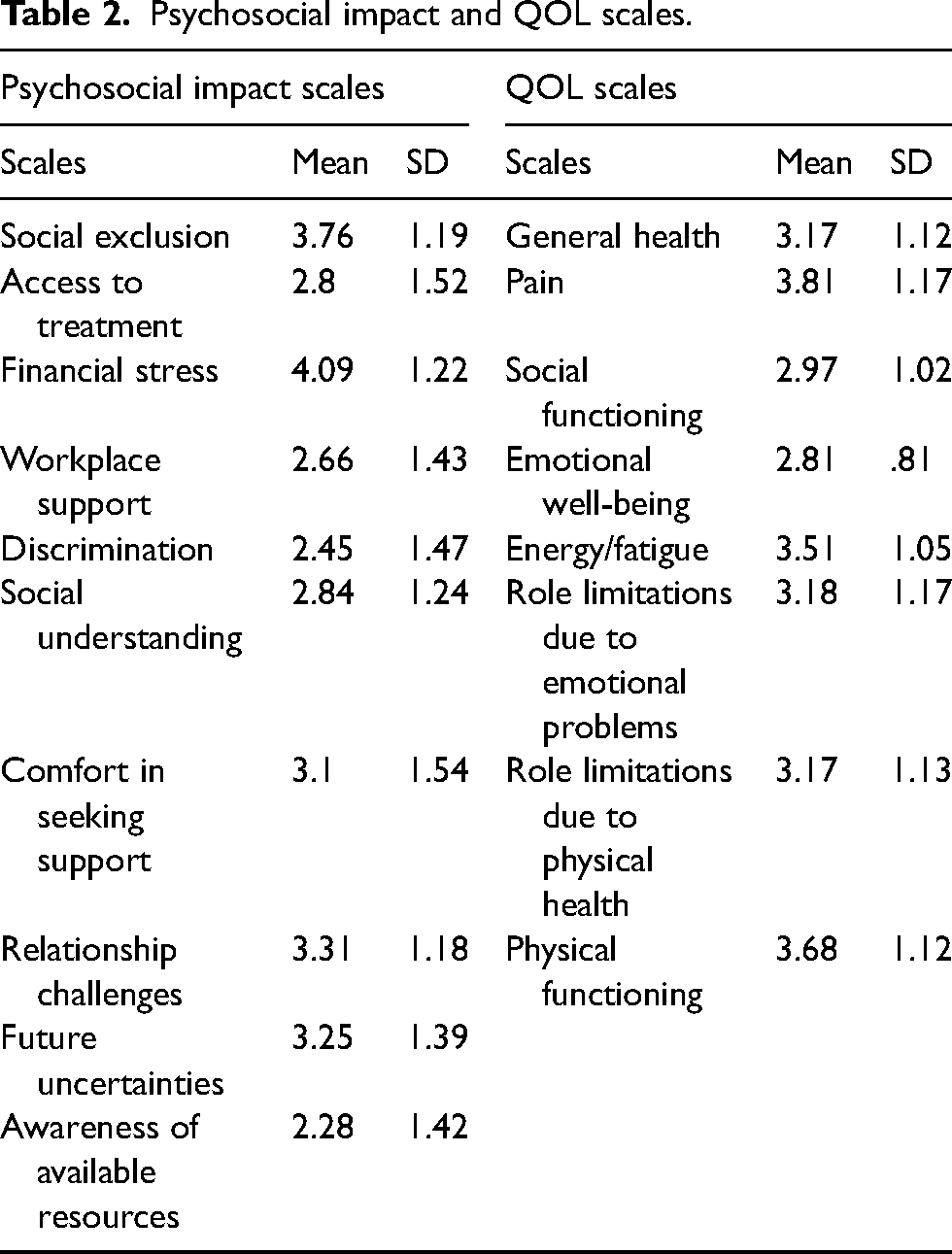
Table 3 presents the differences in blood disorder patients’ perceptions regarding psychosocial impact scales, stratified by age, gender, and type of disorder. The mean scores and p-values are provided for each psychosocial impact scale, indicating the significance of differences within each subgroup. Regarding age groups, participants aged 18–24 show statistically significant differences in social exclusion (p = 0.0212), discrimination (p = 0.0275), and comfort in seeking support (p = 0.0363) compared to other age groups. Gender differences reveal no statistically significant variations in most scales, except for discrimination (p = 0.0754). Notably, participants with different types of disorders exhibit statistically significant variations in several scales, including financial stress (p = 0.0061), discrimination (p = 0.0006), and awareness of available resources (p = 0.0006). These findings underscore the importance of considering age and type of disorder when assessing psychosocial impact among blood disorder patients, providing valuable insights for tailored interventions and support systems.
Difference of opinions among participants grouped by age, gender, and type of disorder in relation to psychosocial impact.
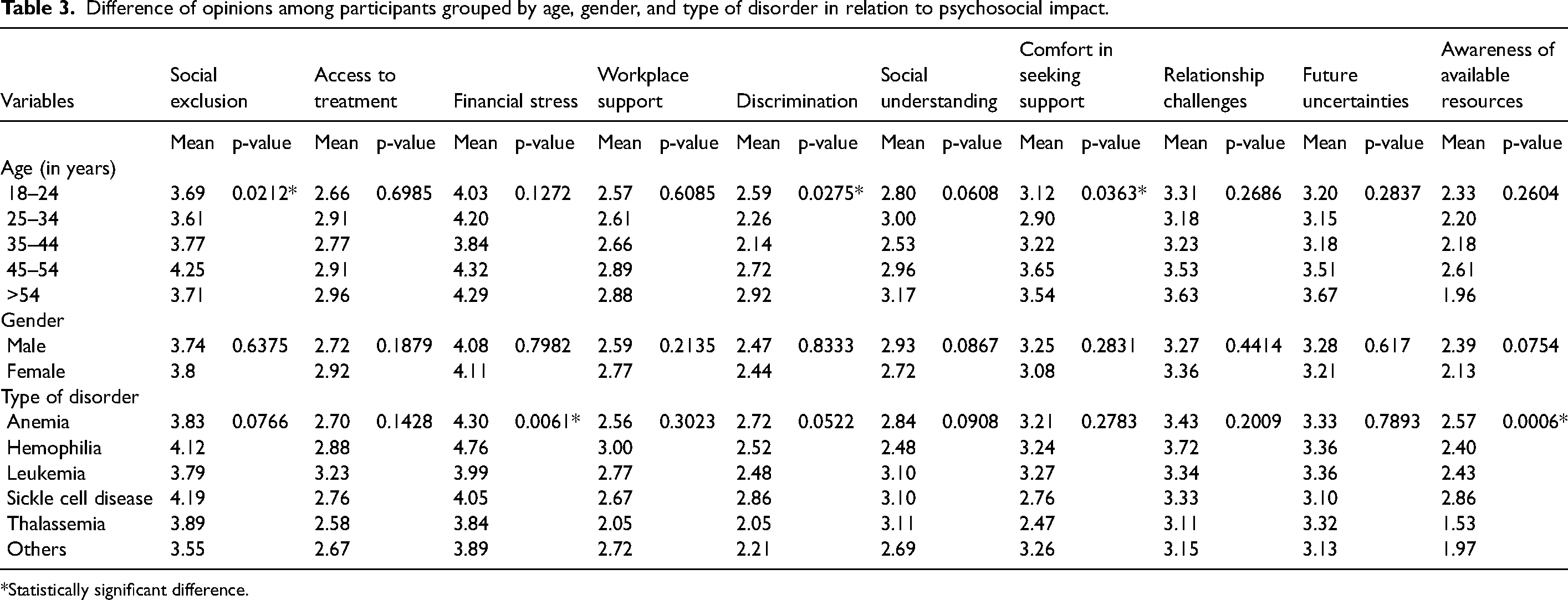
Statistically significant difference.
Table 4 provides insights into the differences in blood disorder patients’ perceptions regarding QOL scales, categorized by age, gender, and type of disorder. Mean scores and p-values are reported for each QOL scale, highlighting significant variations within subgroups. Participants aged 18–24 exhibit statistically significant differences in general health (p = 0.0175), pain (p = 0.0128), emotional well-being (p = 0.0263), and role limitations due to emotional problems (p = 0.0263) compared to other age groups. Gender differences show a significant variation in energy/fatigue (p = 0.0269). Notably, participants with different types of disorders demonstrate statistically significant differences in several scales, including emotional well-being (p = 0.0318), role limitations due to emotional problems (p = 0.0266), and physical functioning (p = 0.0318). These findings underscore the importance of considering age, gender, and type of disorder when assessing the QOL among blood disorder patients, providing valuable insights for tailored interventions and support systems.
Difference of opinions among participants grouped by age, gender, and type of disorder in relation to QOL.
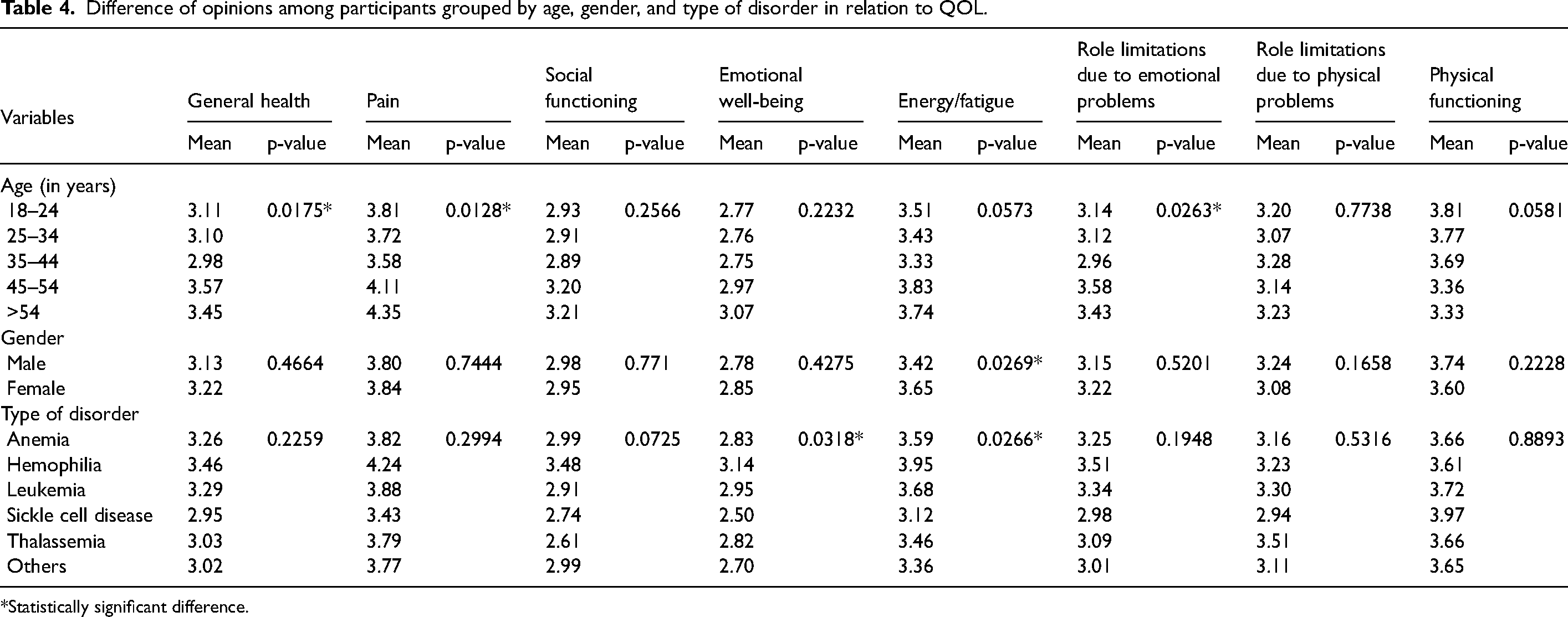
Statistically significant difference.
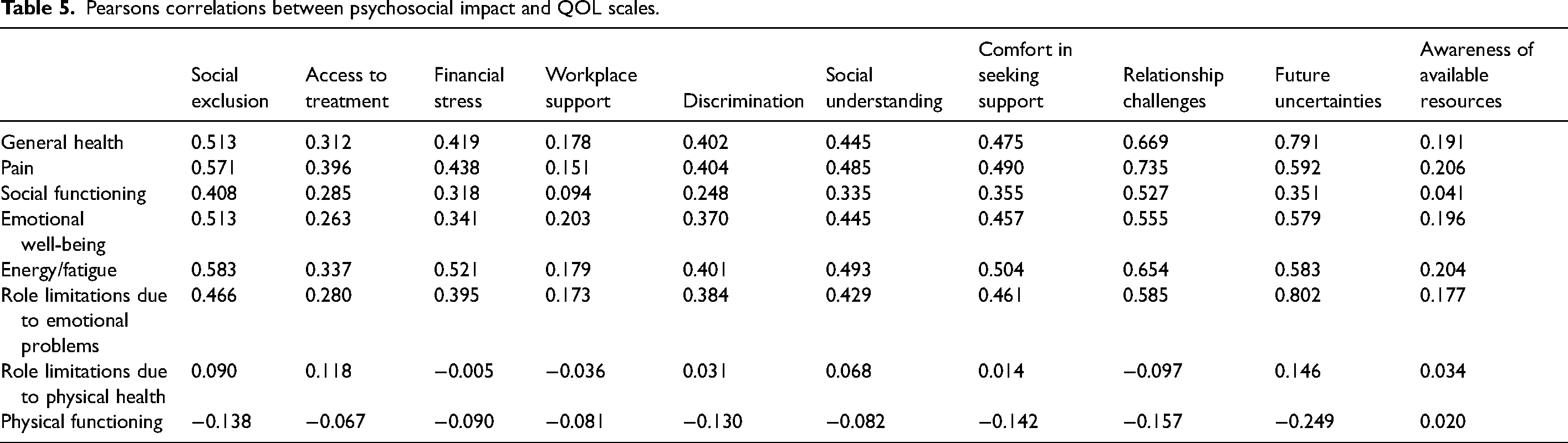
Table 5 displays Pearson's correlations between psychosocial impact and QOL scales for patients with blood disorders. The positive correlations indicate the strength and direction of the relationships between the variables. Strong positive correlations are observed between several psychosocial impact scales and QOL scales. Notably, there is a substantial positive correlation between social exclusion and general health (r = 0.513), pain and relationship challenges (r = 0.735), and energy/fatigue and future uncertainties (r = 0.583). Financial stress also shows moderate to strong positive correlations with general health (r = 0.419), pain (r = 0.438), and energy/fatigue (r = 0.521). Interestingly, role limitations due to emotional problems exhibit a strong positive correlation with several QOL scales, including general health (r = 0.669), pain (r = 0.592), and future uncertainties (r = 0.802). On the other hand, role limitations due to physical health and physical functioning demonstrate weaker correlations with psychosocial impact scales. These findings underscore the interconnectedness of psychosocial impact and QOL among individuals with blood disorders, emphasizing the need for comprehensive and holistic interventions addressing both psychosocial and health-related aspects to enhance overall well-being.
Pearsons correlations between psychosocial impact and QOL scales.
Discussion
The findings in this study provided a comprehensive understanding of the psychosocial impact and QOL among individuals with blood disorders. Analyzing the data collectively reveals several noteworthy trends and insights. Firstly, the demographics of the surveyed participants indicate a diverse sample in terms of age, gender, education, and types of disorders. Such diversity is crucial for capturing the heterogeneity of experiences within the population.
In terms of psychosocial impact, participants report relatively high mean scores for financial stress (4.09), social exclusion (3.76), and relationship challenges (3.31). These elevated scores suggest that individuals with blood disorders experience notable difficulties in financial aspects, social inclusion, and maintaining relationships in similar to the findings in (Borrescio-Higa and Valdes, 2022; Knisely et al., 2020). On the other hand, awareness of available resources receives the lowest mean score (2.28), indicating potential gaps in knowledge or access to support resources among the surveyed individuals (Abu-Odah et al., 2020; Grassi, 2020; Korszun et al., 2013; Stadler et al., 2021; Zeiler et al., 2022). However, access to treatment (2.8) indicated the lack of comprehensive treatment plans that entail all the services including education, physical and mental treatments as suggested in (Drouin et al., 2023). Turning to the QOL scales, the mean scores for general health (3.17) and energy/fatigue (3.51) suggest moderate levels of well-being, pain perception, and energy levels, respectively. However, pain (3.81) indicated significantly high impact on the well-being in similar to observations in (Atallah et al., 2021; Ballas and Darbari, 2020; Di Francia et al., 2021; Niscola et al., 2011). Emotional well-being and social functioning also receive moderate mean scores (2.81 and 2.97, respectively), indicating room for improvement in these domains. Interestingly, role limitations due to emotional problems and physical health, as well as physical functioning, exhibit relatively higher mean scores (3.18, 3.17, and 3.68, respectively), suggesting that individuals perceive significant challenges in these areas.
Exploring the differences in participants’ perceptions based on age, gender, and type of disorder, highlight the significance of these demographic factors in shaping psychosocial impact and QOL. For instance, age differences show that younger participants (18–24) experience distinct psychosocial challenges, including social exclusion, discrimination, and comfort in seeking support. Similarly, the younger age group (18–24) and female participants demonstrate unique QOL challenges, particularly in domains such as general health, pain, and energy/fatigue. These findings indicate major concern as the young population could be at risk of developing mental challenges, which may significantly impact their lifestyle, and also the public health and economy (Fusar-Poli et al., 2021; Knapp and Wong, 2020; Shanahan et al., 2022). The findings suggested that there is no significant difference among the genders in relations to the psychosocial and quality of life impact, suggesting the similar experiences across both genders. However, focusing on type of disorders, significant differences in financial stress, lack of awareness, emotional well-being, and energy/fatigue were observed. As the treatment costs vary with respect to the disorders, the differences among the patients can be understood. Pearson's correlations, underscores the interrelationships between psychosocial impact and QOL scales. Strong positive correlations between social exclusion and general health, as well as pain and relationship challenges, indicate the interconnectedness of psychosocial factors with overall well-being. Moreover, the significant positive correlations between financial stress and various QOL scales emphasize the impact of economic factors on individuals with blood disorders.
These findings offered valuable insights into the psychosocial impact and QOL of individuals with blood disorders. The findings underscore the importance of considering demographic factors and the interconnectedness of psychosocial and health-related aspects when designing interventions and support systems. While the data aligns with broader trends observed in previous studies, future research could further explore these relationships and assess the effectiveness of targeted interventions in improving the overall well-being of individuals with blood disorders.
The study's findings reveal significant impacts on the quality of life and psychosocial well-being among patients with blood disorders. These impacts are often intertwined with nutritional health. For instance, many blood disorders, such as anemia, are linked to deficiencies in iron, vitamin B12, and folic acid (Bhadra and Deb, 2020). Addressing these nutritional deficiencies can alleviate symptoms and improve patients’ overall well-being. Moreover, the psychosocial challenges identified in this study, such as stress and fatigue, can influence and be influenced by nutritional choices. Enhancing nutritional support can thus play a crucial role in improving both the physical and mental health of these patients, underscoring the importance of integrating nutritional considerations into their overall care plan.
This study contributes to the existing literature by providing a comprehensive analysis of the quality of life and psychosocial impacts on patients with blood disorders, a topic that has not been extensively explored. While previous research has often focused on clinical outcomes and treatment efficacy, our study highlights the everyday challenges and mental health concerns faced by these patients. By using a large and diverse sample, we offer valuable insights into the lived experiences of patients, which can inform more holistic care approaches. Additionally, our findings underscore the importance of integrating psychosocial support and nutritional interventions into patient care, paving the way for more patient-centered health policies and practices. This research fills a gap in the literature by linking the physical, psychological, and nutritional needs of patients with blood disorders, thus providing a more nuanced understanding of their overall well-being.
Limitations
While the study on QOL and psychosocial impact of patients with blood disorders provides valuable insights, it is essential to acknowledge its limitations. Firstly, the cross-sectional survey design employed in this research restricts the establishment of causal relationships, limiting the ability to explore the dynamic nature of psychosocial and QOL factors over time. The reliance on self-reported data may introduce response biases, as participants might provide socially desirable answers or recall inaccurately. Additionally, the study's focus on patients from a specific hospital in Saudi Arabia, particularly those with various blood disorders, might limit the generalizability of findings to broader populations or specific blood disorder categories prevalent in other regions. Furthermore, the use of a Likert scale for psychosocial and QOL assessments, while providing quantitative data, may oversimplify the complex and multifaceted nature of individuals’ experiences with blood disorders. Despite these limitations, the study offers valuable groundwork for understanding the interplay between psychosocial factors and QOL among individuals with blood disorders, highlighting the need for further longitudinal, diverse, and in-depth investigations to enhance the robustness and generalizability of findings.
Implications
Theoretical implications of the study on the QOL and psychosocial impact among patients with blood disorders contribute to the existing literature by providing a comprehensive understanding of the interconnectedness between psychosocial factors and health-related quality of life. The findings underscore the relevance of considering demographic variables, such as age, gender, and type of disorder, in assessing the unique challenges faced by individuals with blood disorders. Moreover, the study reveals the intricate relationships between psychosocial impact and various aspects of QOL, offering a nuanced perspective on the multifaceted nature of patients’ experiences. The identification of strong correlations between specific psychosocial factors and QOL dimensions emphasizes the need for a holistic approach to patient care that addresses both psychological and physical well-being.
Practically, the study's implications are crucial for healthcare professionals and policymakers in tailoring interventions and support systems for individuals with blood disorders. By recognizing the distinct challenges faced by different demographic groups and understanding the factors influencing QOL, healthcare providers can enhance patient-centered care. The study advocates for the development of targeted strategies to address financial stress, social exclusion, and relationship challenges, emphasizing the importance of comprehensive support networks. Practitioners can utilize these insights to formulate more effective treatment plans that not only focus on medical aspects but also integrate psychosocial considerations. Additionally, the study highlights the potential gaps in awareness of available resources, suggesting the need for improved dissemination of information and support services for individuals with blood disorders and their families.
Conclusion
This study significantly contributes to the understanding of the QOL and psychosocial impact experienced by individuals with blood disorders. The complex issues these individuals confront are illuminated by examining psychosocial factors and their relationship to QOL. The variable age, gender, and disorder profile of the participants highlights the necessity for personalized therapies that incorporate these subgroups’ distinct experiences. The study found significant financial stress, social marginalization, and interpersonal troubles for blood condition patients, highlighting their complex burden.
This research is useful for healthcare professionals, policymakers, and practitioners. Psychosocial factors affecting QOL dimensions can be identified to generate targeted therapies beyond medical treatments. The study promotes holistic patient care that addresses physical and mental health. The results also suggest resource awareness gaps, requiring more communication and support. The study's cross-sectional design and self-reported assessments must be considered despite these great contributions. The study also focused on one institution, limiting its generalizability. Future research could examine the dynamic nature of psychological effect on QOL in blood disorder patients using longitudinal methods and larger samples. This study advances research and improves holistic care for people with complex blood diseases.
Footnotes
Availability of data and materials
Data will be available upon request.
Authors’ contributions
All authors contributed equally to this work.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The research ethics committee at Imam Abdulrahman Bin Faisal University approved the study / IRB- 2024-03-046.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.