
Abstract
Introduction
Lung cancer patients are often diagnosed late, resulting in shorter survival rates (He et al., 2022). Therefore, it is crucial to focus on their quality of life (QoL). Compared to other cancer types, the QoL for patients with lung cancer is typically inferior due to various symptoms such as fatigue, dyspnea, cough, pain, and hemoptysis, which are hallmark features of lung tumors. Fatigue and respiratory issues further diminish psychological well-being, while sleep disturbances impair cognitive function, compromising overall QoL (Polanski et al., 2016).
Malnutrition is common among lung cancer patients (Kasprzyk et al., 2021), particularly in advanced stages (Jain et al., 2020); most of these patients have non-small cell lung cancer (NSCLC) (Tran et al., 2021). The progression of the disease, symptom severity, and treatment-related side effects significantly decrease the QoL for those living with lung cancer. Poor nutrition has an inverse relationship with QoL and exacerbates symptom severity (Polański et al., 2021). However, the precise influence of nutrition-related symptoms on QoL among lung cancer patients remains indeterminate.
Within the realm of nutritional evaluation, the PG-SGA stands out as a specialized assessment tool tailored for cancer patients as it comprehensively evaluates various nutritional aspects specific to this population. This tool comprised two sections completed by a patient or a clinician accordingly. Four medical components (weight loss, nutrition impact symptoms, intakes, and functional capacity) were assessed in a checkbox format, completed by the patient. Later, the physician scored the disease status and its relation to nutritional requirements, metabolic demands, and physical examinations. PG-SGA scores were classified as introduced in the form. A higher score reflected a higher risk of malnutrition. Moreover, an appropriate action plan was recommended. A score of 0–1 indicated that the patient did not require an intervention. A score of 2–3 suggested patients and their families need nutrition education and counseling by a medical staff member (e.g. a dietitian, a nurse, or a physician) and/or a pharmacologic intervention, as indicated. A score of 4–8 meant the patient required intervention by dietitians in collaboration with nurses or physicians. A score of ≥9 indicated a critical need for improved symptom management and/or nutrient intervention options (Bauer et al., 2002).
The QLQ-LC13 QoL questionnaire is tailored specifically for assessing the QoL in lung cancer patients. It builds upon the foundation of the QLQ-C30 questionnaire, which is designed for evaluating QoL in cancer patients more broadly. By accounting for the distinct characteristics and challenges of lung cancer, the QLQ-LC13 questionnaire provides a targeted approach to assessing QoL in this patient population (Bergman et al., 1994a).
In actuality, oncology patients routinely attend hospital appointments for health assessments, chemotherapy administration, or additional treatments. Consequently, numerous factors influence the patient's QoL, including extended waiting times for examinations, treatment delays, suboptimal treatment responses, the use of chemical agents, and the frequency of chemotherapy courses. This study specifically focuses on assessing the impact of nutrition-related symptoms (indicated by Patient Generated Subjective Global Assessment- PG-SGA) to QoL among individuals diagnosed with advanced NSCLC, utilizing the EORTC QLQ-LC13 tool.
Methods
Selection and description of participants
This is a descriptive cross-sectional study, with simple random sampling, included 170 patients (129 male), aged ≥18, between March and October 2023 at the two departments of Hanoi Oncology Hospital, Vietnam (Department of Chemotherapy 1 and Department of General Chemotherapy services). Hanoi Oncology Hospital is one of three last stream oncology hospital in Vietnam, received cancer patients from Northern and North Central provinces of Vietnam. Patients diagnosed with NSCLC stage IV based on TNM classification (TxNxM1) were invited to the study. Exclusion criteria were uncertain diagnosis of neoplasm; had ≥2 cancers; state of hemodynamic instability; serious chronic co-morbidities (heart failure in exacerbation phase, severe COPD, asthmatic state; cognitive dysfunction; situations made weight and/or height measurement impossible such as edema, amputation, kyphosis, and scoliosis.
Data collection
Socio-demographic and clinical data were collected from medical records.
PG-SGA was applied to each patient and completed by a dietitian. Each item of the PG-SGA was scored. Total higher scores (the numerical PG-SGA score) represent a poorer nutritional status. Patient risk for malnutrition was categorized as low (0–3 points), medium (4–8 points), or high (≥ 9 points). The first part was patient generated. Box 1 (Weight history) and Box 3 (Symptoms) scores were additive, whereas scores of Box 2 (Food intake) and Box 4 (Activities and Function) were not. In these boxes, the highest point score was recorded. The remaining portions of the PG-SGA form were completed by the dietitian. The scores were calculated based on the disease and its stages, components of metabolic stress or use of corticosteroids and physical components (loss of subcutaneous fat, muscle wasting, and edema or ascites). The PG-SGA category score also applied with stage A (well nourished), stage B (moderate or suspect of malnutrition) or stage C (severe malnourished).
Quality of Life Questionnaire Lung Cancer-13 (QLQ-LC13) incorporates one multi-item scale (n = 3) to assess dyspnea, and a series of single items (n = 1) assessing pain, coughing, sore mouth, dysphagia, peripheral neuropathy, alopecia, and hemoptysis. All the scales and single-item measures range in score from 0 to 100. A high score for the scales and single items represents a high level of symptomatology or problems. The raw score (RS) was calculated as RS = (I1 + I2 + … In)/n. Then score S = [(RS − 1)/IR × 100] with IR (Item range) is the difference between the possible maximum and the minimum response to individual items. All items were scored 1 to 4, giving IR = 3.
A total of 170 patients were included to final analysis. Participants received a comprehensive briefing on the study and voluntarily consented to partake in the research. They were assured of the confidentiality of the collected data and that under no circumstances would their names be disclosed in the published results. Additionally, they were informed of their right to withdraw from the study at any time. The study has been approved by the Ethics Committee of Hanoi Oncology hospital, number 1041/QĐ-BVUB on 27 April 2023. The study protocol was carried out in accordance with the tenets of the Declaration of Helsinki and Good clinical practice guidelines.
Statistical analysis
Epidata (Version 3.1) software was used to develop datasets. All input data were statistical analyzed using the Statistical Package for the Social Sciences (IBM SPSS Statistics version 20.0 for Windows). Continuous variables were presented as the mean ± standard deviation (SD); whereas categorical variables were presented as the number and percentage values (n; %). Inter-group differences were assessed by Kruskal–Wallis's test and were significant at p < 0.05. The aspects of EORTC-QLQ-13 scale were differentiated between the two groups of PG-SGA total score (a score of 8 or below, while the remaining scores are 9 or above) and presented as figure in Microsoft excel. To assess the relation between QoL (dependent variables) and PG-SGA score (independent variables), the correlation coefficient between two variables was assessed using the Pearson's correlation coefficient for normally distributed continuous variables and Spearman's between two variables of at least ordinal measurement level. The correlation was perfect if the value given by ± 1; very strong if the value between ± 0.8 and ± 0.9; moderate if the value between ± 0.6 and ± 0.7; fair if the value between ± 0.3 and ± 0.5; poor if the value between ± 0.1 and ± 0.2 and the value = 0 indicated no correlation (Akoglu, 2018). To assess age group-related QoL, aged was classified as under 40, 40 to 60, and over 60 (Gort-van Dijk et al., 2021).
Results
Patients’ characteristics
The patients’ mean age in this study was 59.1 ± 7.8 years, nearly three-fourth was male (75.9%) and 68.8% smoke. All of them lived with their family. The prevalence of hypertension and diabetes was 10.6% and 12.9%, respectively; hypertension combined with diabetes occurred in 7.6% patients. The mean PG-SGA score was 13.8 ± 5.9. Most of patients required urgent nutrition intervention (82.9%). The categorized PG-SGA identified 62.4% patients at risk (PG-SGA B) and 33.5% had malnutrition (PG-SGA C)
In terms of nutrition-related symptoms, patients with loss of appetite and anorexia accounted for the highest rate of 77.6%. The next were fatigue (67.6%) and dry mouth (65.9%). The proportion of patients with constipation and nausea was 40.0% and 30.6%, respectively. The symptom of pain and taste change were similar with 31.2%. Symptoms of difficulty swallowing, bad smell, vomiting, and early satiety were minor (< 20%) (Figure 1).
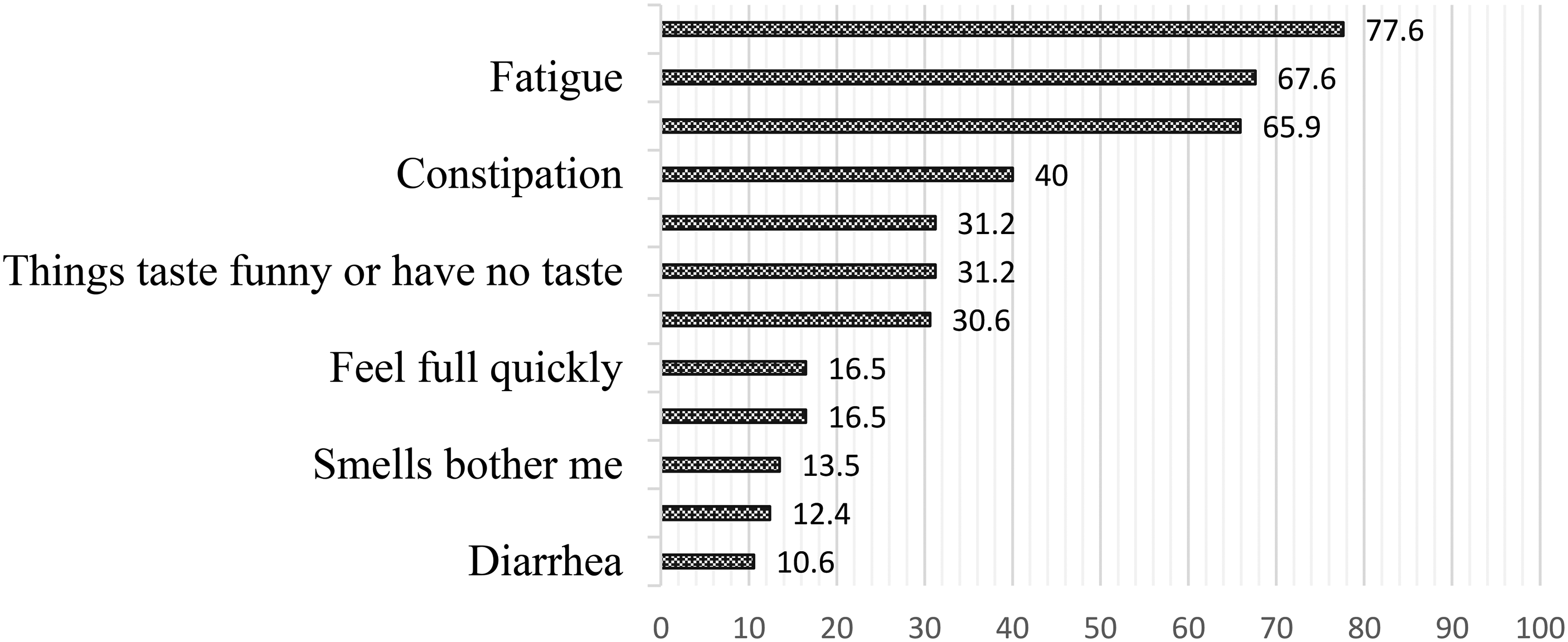
Nutrition-related symptoms experienced in the past two weeks as evaluated by the PG-SGA assessment.
Most of patients had cough with 40.6% a little; 25.9% quite a bit; 5.3% had cough very much but only 10.6% had cough up blood a little or quite a bit.
Short of breath was typically with 85.9% patients’ recorded. Nearly a half of them (46.5%) reported pain in chest and 38.2% had pain in other parts of their body. One-fifth of this study population (21.2%) took medicine for pain (Figure 2).
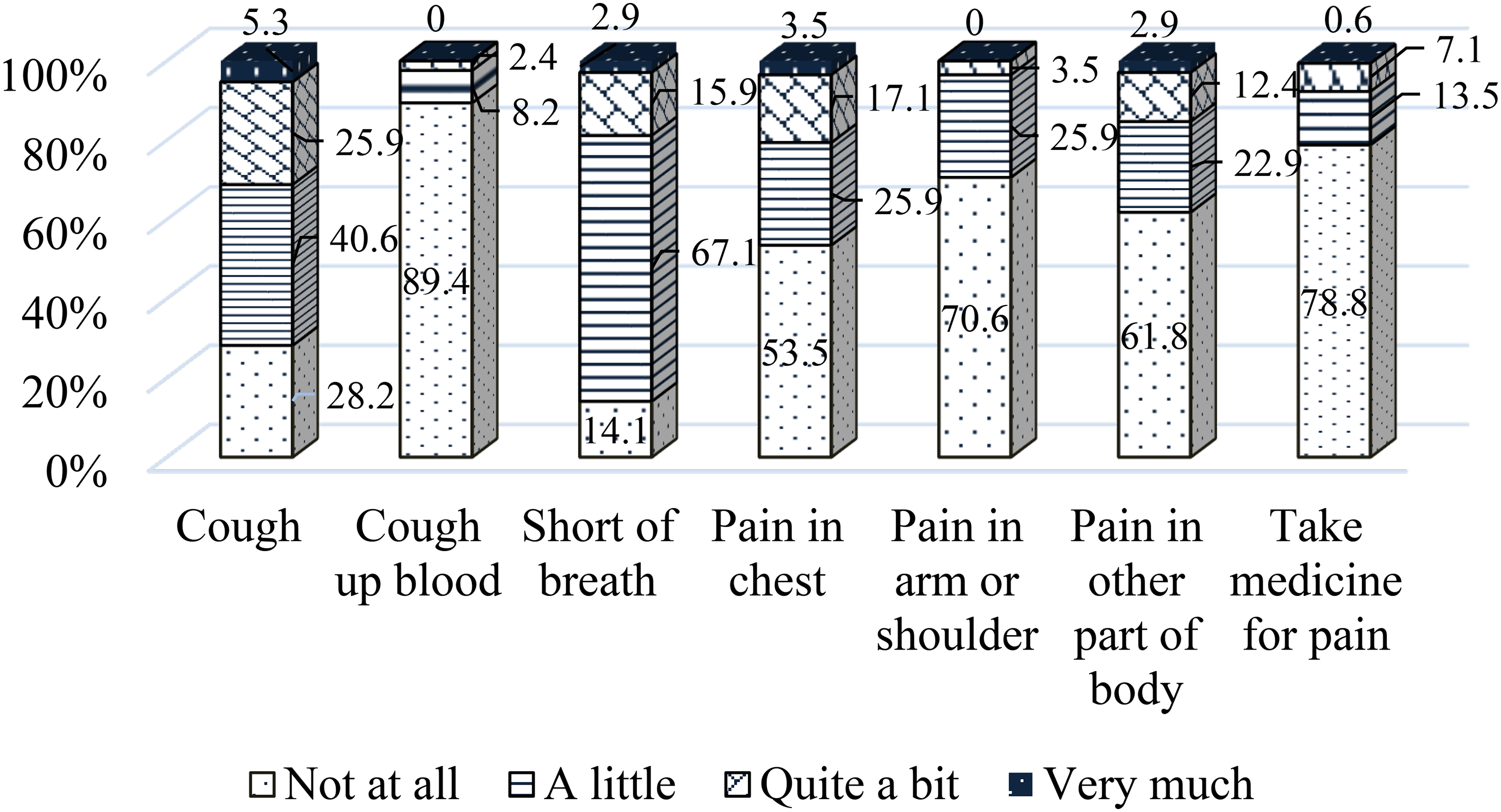
Symptoms-related quality of life in advance stage NSCLC patients.
In comparison between the two groups of PG-SGA classification cut-off, patients with PG-SGA total score ≥ 9 required urgent intervention, the aspects of EORTC-QLQ-13 scale were differentiated, as shown in Figure 3.
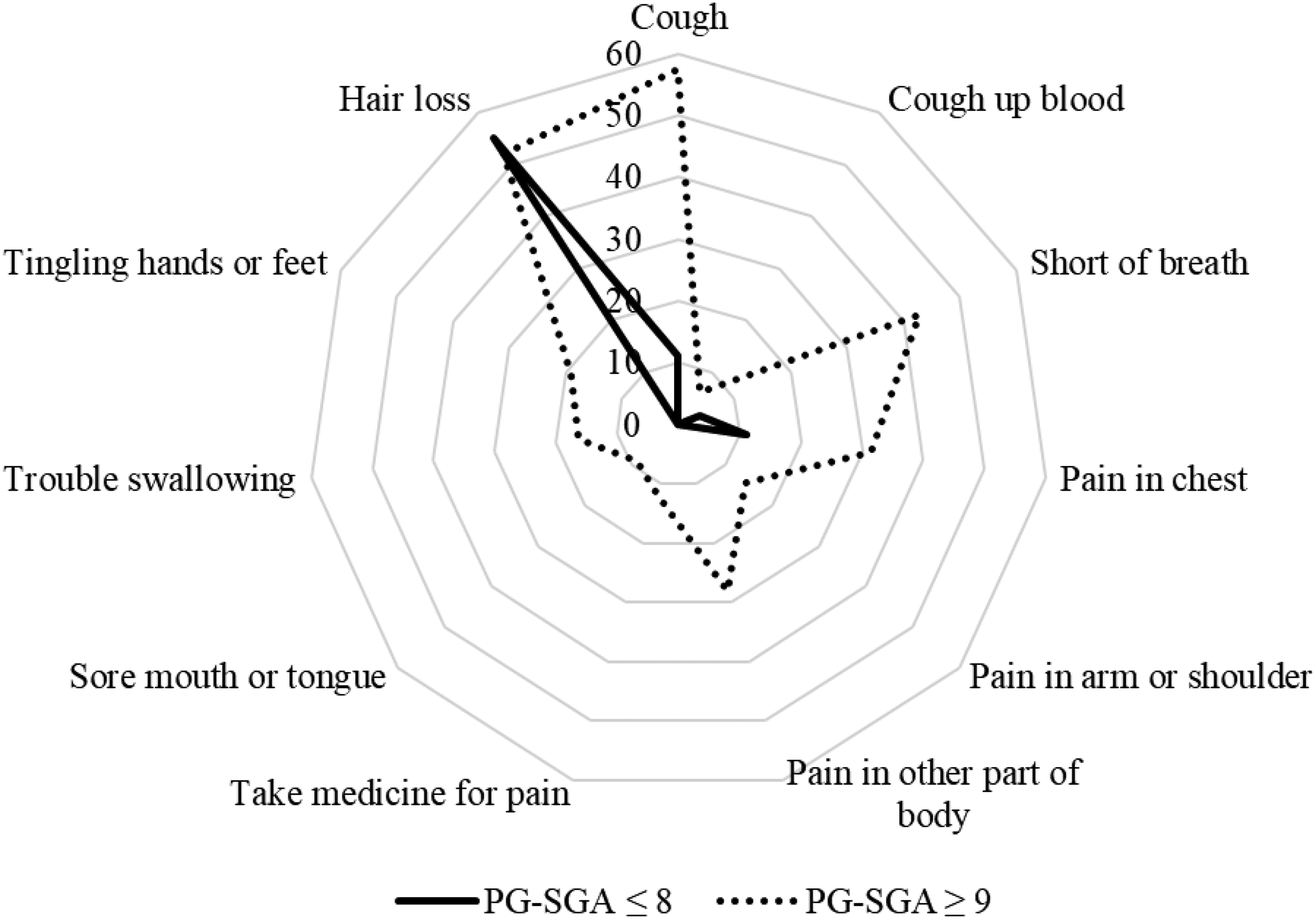
Components of the EORTC-QLQ-13 scale in the two groups classified by the PG-SGA.
Nutrition symptoms-related QoL in advance stage NSCLC patients
The Kruskal–Wallis test was used to evaluate the impact of age on the mean scores of all indexes QoL. The higher the symptom assessment score in the EORTC-QLQ-13 scale (indicating a decrease in QoL), the poorer the nutritional status according to PG-SGA, except the symptoms of cough up blood and take medicine for pain, and this difference is statistically significant with p < 0.05. The Pearson's test showed symptoms-related QoL positively correlated with PG-SGA score with cough and short of breath were at moderate correlation; pain (in chest, in arm or shoulder and in other part of body), take medicine for pain and trouble swallowing were fairly correlated. The symptoms of cough up blood, sore mouth or tongue, tingling hands or feet and hair lost had poor correlation with PG-SGA score (Table 1).
Malnutrition-related QoL in advance stage NSCLC patients.
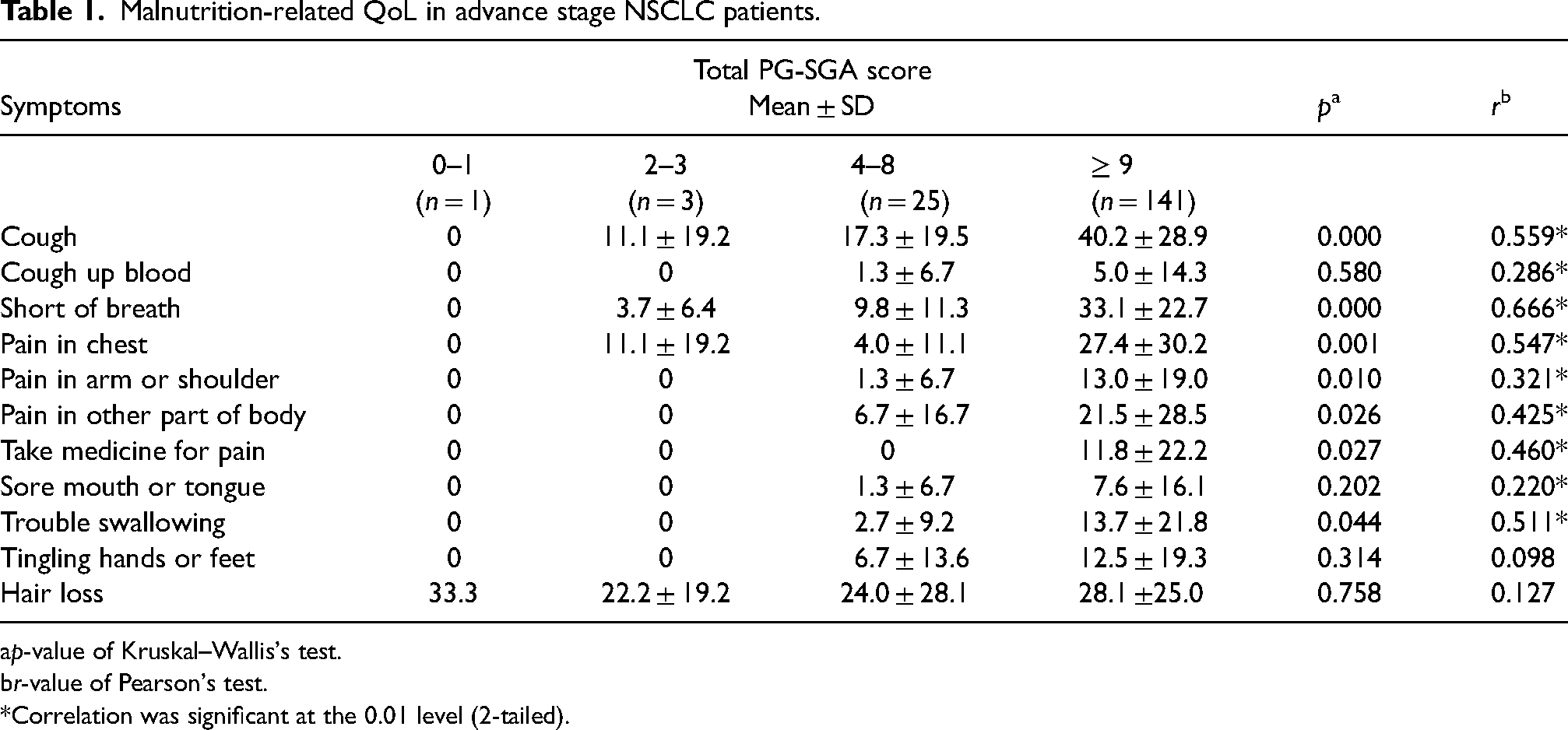
p-value of Kruskal–Wallis's test.
r-value of Pearson's test.
Correlation was significant at the 0.01 level (2-tailed).
In patients with loss of appetite and anorexia (n = 132) by PG-SGA assessment, there were a negative correlation with short of breath and pain in arm or shoulder in the QoL LC13 scale, but the correlates were poor. The correlates between fatigue (PG-SGA assessment) and short of breath and chest pain (QoL LC13 scale) were negatively fair. Dry mouth (PG-SGA assessment) positively fair correlated with cough up blood, short of breath and pain in chest (QoL LC13 scale). Constipation had poor correlation with short of breath and tingling hands or feet (QoL LC13 scale) (Table 2).
Correlation between QoL symptoms and common nutrition symptoms.
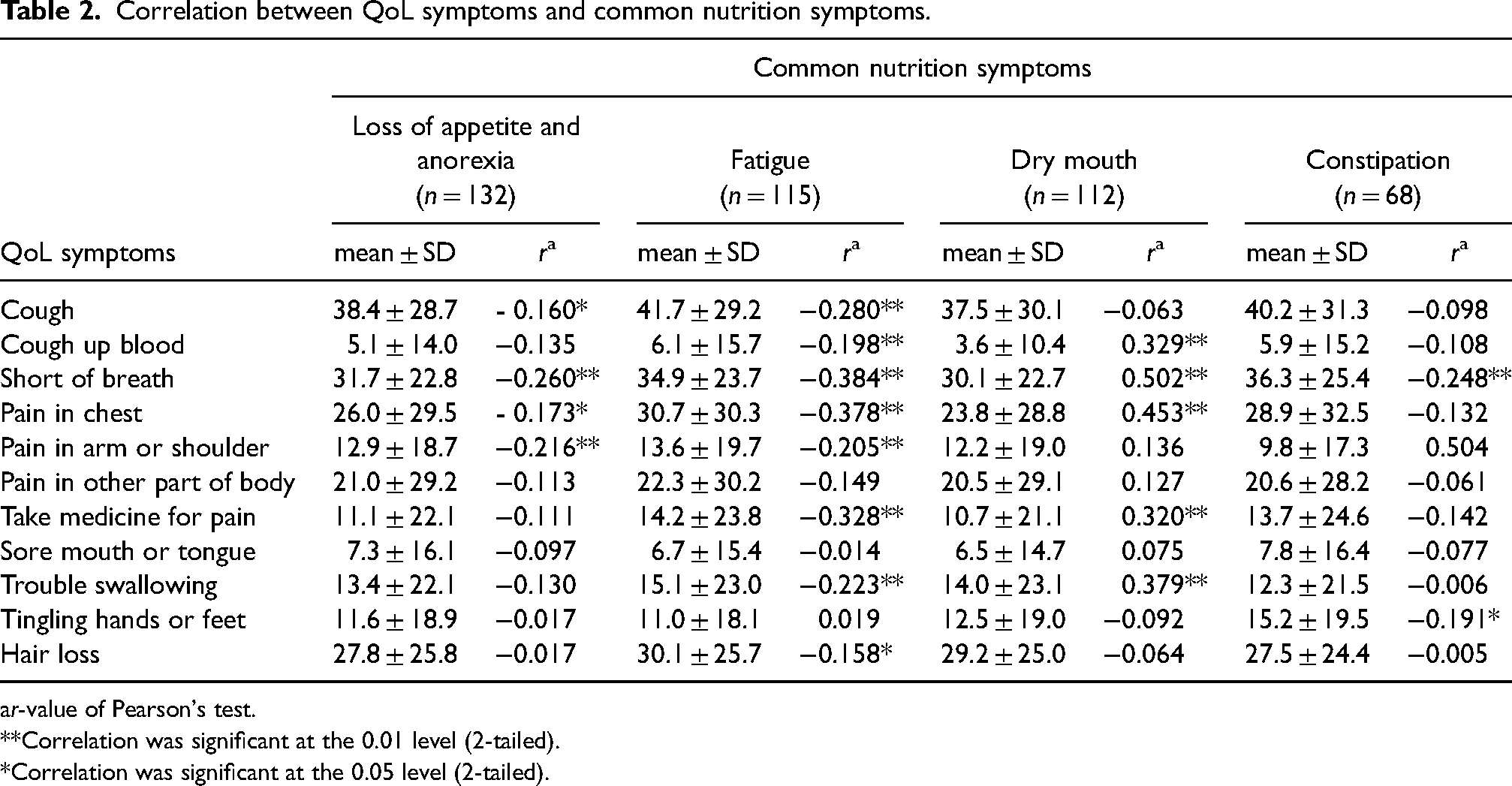
r-value of Pearson's test.
Correlation was significant at the 0.01 level (2-tailed).
Correlation was significant at the 0.05 level (2-tailed).
Between age groups, only tingling hands or feet and hair loss had significant difference (p < 0.05; Kruskal–Wallis's Test), but the correlation (Pearson's Test) were poor (r = 0.217 and 0.113, respectively) (Table 3).
Age group-related QoL in advance stage NSCLC patients.
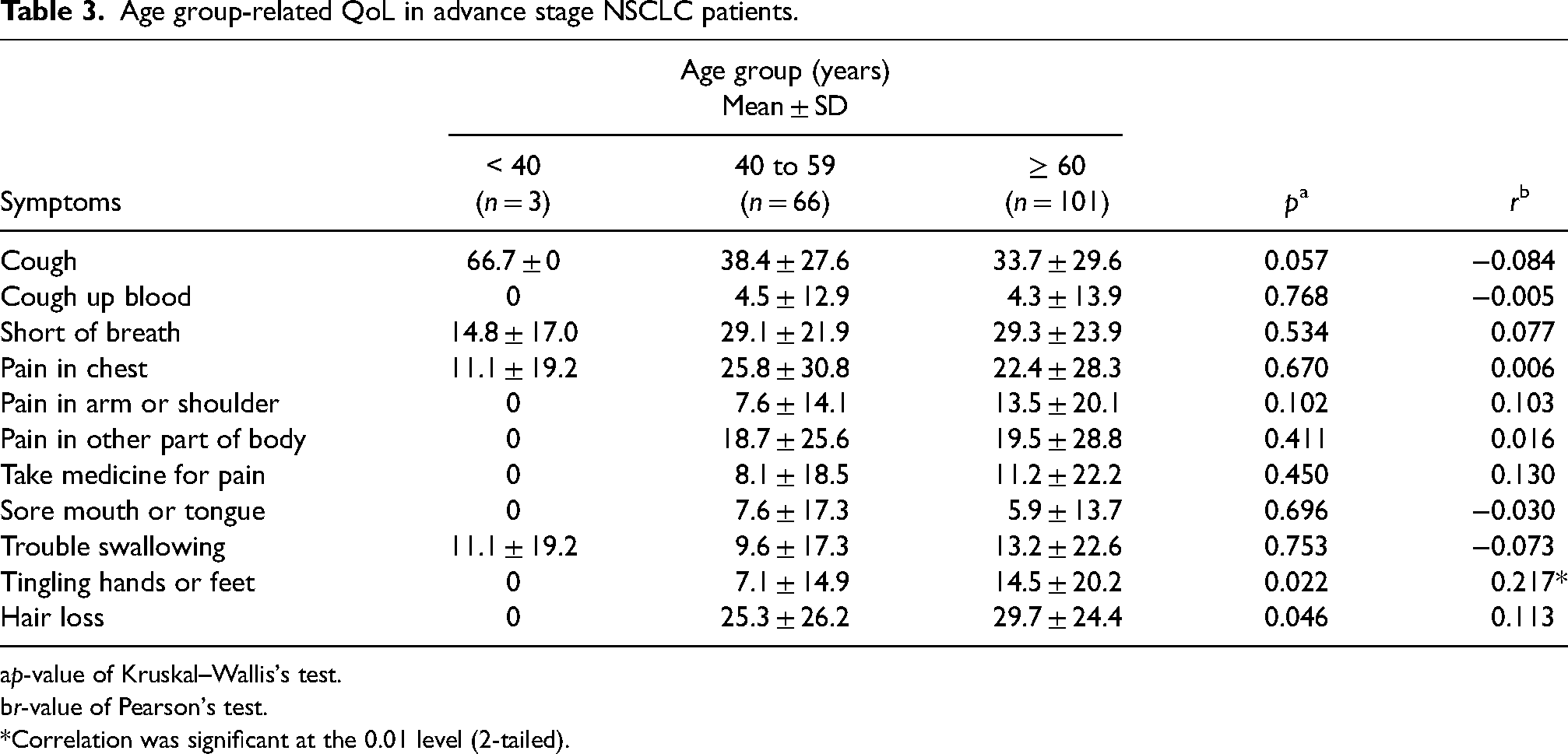
p-value of Kruskal–Wallis's test.
r-value of Pearson's test.
Correlation was significant at the 0.01 level (2-tailed).
Discussion
QoL associated with malnutrition
QoL negatively correlated with malnutrition. Malnutrition was well defined as an independent determinant of lower QoL (Polański et al., 2021). In our results, the mean ± SD of PG-SGA scores was 13.8 ± 5.9, implying that the patients required urgent nutritional intervention. Moreover, according to PG-SGA classification, 95.9% patients were or at risk of malnutrition.
The PG-SGA, a well-established tool, is tailored for evaluating the nutritional status of cancer patients. Its findings offer guidance on the necessary nutritional support for each patient. Nonetheless, its drawback lies in the time-consuming nature and the requirement for skilled medical personnel proficient in identifying clinical indicators, particularly those associated with nutrition like muscle depletion and reduced subcutaneous fat (Bauer et al., 2002). EORTC-QLQ-C13 is a questionnaire developed to assess health-related QoL of people with lung cancer (Bergman et al., 1994b). Several studies have explored the correlation between nutritional status and QoL among individuals with lung cancer. However, these studies commonly utilized the Mini Nutritional Assessment (Konstantinidis et al., 2023; Polański et al., 2021) or GLIM (Landgrebe et al., 2023) toolkit to evaluate nutritional status. However, the findings of this study were consistent with prior research, all indicating a link between nutritional status and a decline in QoL. Prior research conducted by S. Xará and colleagues also examined the correlation between nutritional status (utilized the PG-SGA tool), and QoL (the EORTC-QLQ-C13), included 56 patients diagnosed with NSCLC at all stages, the result showed undernutrition is associated with worsen QoL, specifically in the parameters of appetite loss, nausea and vomiting, constipation and fatigue (Xará et al., 2011). Our study focuses on patients diagnosed with NSCLC at advance stage, which occurred in about 80% of Vietnamese lung cancer patients (Tran et al., 2021), and the most frequent symptoms were loss of appetite and anorexia, fatigue, and dry mouth.
Nutrition-related symptoms associated with low QoL
In our study, symptoms-related QoL included cough and short of breath; pain (in chest, in arm or shoulder and in other part of body), take medicine for pain and trouble swallowing were positively moderate correlated with PG-SGA score. The rest symptoms had fair or poor correlation with PG-SGA score. Previously, it was restricted in scope in cancer population. This finding may be a first step toward the development of evidence-based nutritional intervention for advance stage NSCLC patients who were in poor QoL or malnutrition.
In addition to the correlation between common nutrition symptoms in this study population, which included loss of appetite and anorexia, fatigue, dry mouth, and constipation, and QoL symptoms, we found that the correlation were poor to fair. Some common nutrition symptoms (PG-SGA toolkit) such as loss of appetite and anorexia, fatigue, dry mouth, and constipation correlate with QoL aspects (cough up blood, shortness of breath, pain in chest, take medication for pain, and trouble swallowing), but the correlations were poor or fair. Previous study showed nutrition intervention was beneficial to the QoL of patients with gastrointestinal cancer (Nguyen et al., 2021). Our finding implied that solely addressing nutritional symptoms to enhance QoL may be insufficient in advance stage NSCLC patients. This indicates a contrast in the influence of nutrition on patients with and without gastrointestinal tract engagement and suggests there is a necessity for a thorough investigation to establish a model aimed at enhancing the QoL for lung cancer patients, whose survival rate is limited.
In addition, most of this study patients were around 60 years old (59.1 ± 7.8 years), the age of sarcopenia onset (Metter et al., 1997), which linked to reduced survival outcomes (Su et al., 2023) and worsen the QoL especially in those with advance cancer (Nipp et al., 2018). In terms of age group, this study found QoL were not significant between age groups, except tingling hands or feet and hair loss. This suggests the QoL of NSCLC at advance stage was not contingent upon age.
The current investigation introduces fresh insights into the field. While earlier studies primarily examined individual facets such as nutritional status or QoL or explored the broader relationship between malnutrition and overall QoL, our research uniquely explores the nuanced connections between specific nutritional symptoms and distinct categories within the QoL spectrum. Secondly, our study indicates the limited efficacy of addressing nutritional symptoms alone in improving the QoL among lung cancer patients when compared to gastrointestinal tract cancers. Third, QoL of NSCLC at advance stage was found to be independent of age. The maximum age of this study was 78 years, so further research is warranted to evaluate the influence of sarcopenia on both nutritional status and QoL.
This study has some limitations. Firstly, this work conducted at the hospital when the patients admitted for periodically treatment, we might expect that findings from this study extend to community-based groups as well. Secondly, this study focused on patients at advanced stage with metastases. Further research is required to assess whether these findings remain consistent across other stage groups as well.
Conclusion
In summary, we found that there was a link between malnutrition (defined by PG-SGA toolkit) and a decline in QoL (using EORTC-QLQ-C13 questionnaire) in advance stage NSCLC patients. Second, the nutrition-related symptoms had poor to fair correlation with QoL categories. This result suggests the insufficiency on solely addressing nutritional symptoms to enhance QoL for advance stage NSCLC patients. Thirdly, the QoL of NSCLC at advance stage was not contingent upon age in this study, but the impact of sarcopenia to nutrition status and QoL need to be determined further.
Footnotes
Acknowledgements
We thank all patients for participating in the study, and physicians/nurses in the Department of Chemotherapy 1 and Department of General Chemotherapy services for their help and cooperation during the study.
Authors’ contributions
Bui Thi Kim Hue and Tran Chau Quyen: conceived of the presented idea; data analysis and manuscript development. Bui Thi Kim Hue: developed the theory and performed the computations. Nguyen Quang Dung and Bui Vinh Quang: supervised the findings of this work; aided in interpreting the results and worked on the manuscript. Le Thu Ha contributed to patients’ preparation. Tran Thi Nam and Nguyen Thi Loan: data collected, data input and contributed to the interpretation of the results. All authors discussed the results and contributed to the final version of the manuscript.
Availability of data and materials
The authors confirm that the data supporting the findings of this study are available within the article.
Consent for publication
All authors provide consent for the publication of the manuscript detailed above, including any accompanying images or data contained within the manuscript that may directly or indirectly disclose our identity. We understand that this information will be freely available online, and accessible to the public. We understand that under the Nutrition and Health Journal terms of publication, this information may be reproduced and used for other purposes, including commercial uses. We acknowledge that this will reduce my actual privacy to the extent of the content of the manuscript. We confirm that we have been given the opportunity to view the manuscript prior to publication, and understand that once published, it cannot be removed from the published record except in exceptional circumstances. A total of 170 patients were included to final analysis. All patients were informed about the purpose and content of this study with explaining that they could withdraw at any time. The study has been approved by the Ethics Committee of Hanoi Oncology hospital, number 1041/QĐ-BVUB on 27th April, 2023. The study protocol was carried out in accordance with the tenets of the Declaration of Helsinki and Good clinical practice guidelines.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
This study was conducted according to the guidelines laid down in the Declaration of Helsinki and all procedures involving research study participants were approved by the Ethics Committee of Hanoi Oncology hospital, number 1041/QĐ-BVUB on 27th April 2023. Written informed consent was obtained from all patients.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.