
Abstract
Introduction
Osteoarthritis (OA) is a multifactorial joint disorder influenced by genetic, metabolic, and biomechanical factors, and it most commonly affects weight-bearing joints such as the knees. It is characterized by progressive cartilage degradation, joint space narrowing, osteophyte formation, and subchondral bone remodeling (De Roover et al., 2023). Among its clinical manifestations, knee pain is the most prominent and often the most disabling symptom (Geng et al., 2023). This musculoskeletal disease commonly causing functional decline, loss in quality of life, and disability (Atukorala and Hunter, 2023). OA represents a growing global health burden, with 527.8 million people affected in 2019—a 119% increase since 1990. In the same year, there were 41.5 million new cases and 18.9 million DALYs attributed to OA, according to the Global Burden of Disease Study 2019 (95% uncertainty intervals provided) (Cao et al., 2024). Women account for 60% of all OA cases around the world, with the gender gap widening after age 40 (Segal et al., 2024). The elevated risk observed in women has been associated with a combination of non-modifiable factors (i.e., joint structure, alignment, hormonal regulation, and genetic predisposition) and modifiable factors (i.e., body composition and muscle strength) (Segal et al., 2024).
In recent years, growing attention has been directed toward the role of vitamin D deficiency in OA, as it is commonly observed among individuals with OA and may contribute to disease progression and symptom severity (Buana et al., 2025; Li et al., 2024). Several studies, including meta-analyses, have reported a higher prevalence of OA in individuals with low serum 25-hydroxyvitamin D (25[OH]D) levels (Annamalai et al., 2023; Tabrizi et al., 2025; Wang et al., 2023), likely due to vitamin D's regulatory role in calcium homeostasis, bone metabolism, and cartilage integrity (Skalny et al., 2023). Moreover, chronic disease populations, including those with OA, are prone to vitamin D deficiency due to disrupted metabolic pathways, limited dietary intake, and reduced mobility that restricts sunlight exposure (Iqhrammullah, 2024; Iqhrammullah et al., 2024; Putra et al., 2023).
In a previous systematic review, the focus was on evaluating the randomized controlled trials results for the efficacy of vitamin D supplementation in OA populations (Wang et al., 2023). Separately, one meta-analysis has estimated the prevalence of vitamin D deficiency in individuals with osteoporosis (Salari et al., 2021). However, to date, no study has synthesized epidemiological evidence to estimate the global prevalence of vitamin D deficiency specifically among individuals with knee OA. This knowledge gap limits public health planning, particularly for targeted screening and preventive strategies. Therefore, this study aimed to estimate the global and regional prevalence of vitamin D deficiency in patients with knee OA using a systematic review and meta-analysis approach.
Methods
Design and registration
The study employed a systematic review followed by meta-analysis in estimating the prevalence of vitamin D deficiency among patients with knee OA. We used the serum 25(OH)D level ≤20 ng/mL as the cut-off for vitamin D deficiency, as recommended by the published guideline (Płudowski et al., 2023). The status of knee OA was based on the clinical diagnosis. The study followed the recommendations from PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses). The protocol of this systematic review and meta-analysis has been registered to PROSPERO on August 6, 2024 (CRD42024577222).
Search strategy
Digital databases for scientific literature, namely Europe PMC, Google Scholar, Scilit, Scopus, and Web of Science, were employed to identify studies reporting the prevalence of vitamin D deficiency among knee OA patients. The following combination of keywords was used in each database: (“Vitamin D” OR “25-hydroxyvitamin D” OR “25-OH vitamin” OR “Calciferol” OR “Cholecalciferol” OR “Ergocalciferol” OR “1, 25-dihydroxyvitamin D”) AND “knee, osteoarthritis.” There were few to negligible modifications for the keyword combination when applied to different databases, but the consistency was generally maintained. The search of all databases was performed on August 8, 2024. No filters (i.e., year of publication, type of study, and language) were applied during the identification stage. The search was carried out on the title, abstract, and keywords fields.
Eligibility criteria
To guide our screening and selection process, we initially designed the eligibility criteria based on the population, exposure, outcome of interest, and study design. The population was individuals of any age who were clinically diagnosed with OA. Other than recruiting patients with pregnancy, chronic kidney diseases, or malignancies, no studies were excluded because of the comorbidities. The exposure was serum 25(OH)D was 20 ng/mL or lower. Studies using different cut-offs (i.e., 30 or 50 ng/mL) or reporting data that could not be separated using the 20-ng/mL cut-off were excluded. To be included, studies should report the number of patients with 20 ng/mL or lower serum 25(OH)D level along with the total number of knee OA patients recruited. As for the study design, we did not include studies with specific pre-determined criteria, such as case-control or any type of interventional studies. Cross-sectional and cohort studies were eligible for inclusion. To minimize selection bias, we did not apply any exclusion criteria based on the laboratory method used to measure serum 25(OH)D levels. Eligible studies employed a range of analytical techniques, including high-performance liquid chromatography (HPLC), enzyme-linked immunosorbent assay (ELISA), chemiluminescent immunoassay (CLIA), and radioimmunoassay (RIA), among others. Additionally, review articles, case reports, case series, editorials, or commentaries were excluded. In this stage, we limited the screening to English-written articles only. No limitation on the time of publication was applied.
Screening and selection
Records were downloaded in a citation format file of each database, and collectively uploaded to rayyan.ai (a web-based screening and selection software designated for systematic review). The duplicates were identified automatically, and the removal of duplicated items was performed through manual selection. After the duplicate removal, the selection of relevant studies based on the title and abstract was carried out by three reviewer authors (JFW, SPN, and ERCO) independently. Studies selected by at least one author were included in the next stage, where they were sought for full-text retrieval. Thereafter, the full-text screening was carried out by the same three reviewer authors (JFW, SPN, and ERCO) independently by applying the eligibility criteria. Any discrepancies were resolved by revisiting and reassessing the article, where the fourth review (MI) would be invited if the consensus could not be reached.
Quality appraisal
The quality appraisal was conducted using the Newcastle–Ottawa Scale (NOS) and its modified version. In general, the tool is comprised of three domains, namely selection, comparability, and outcome. The selection domain includes three items, followed by one item under the comparability domain, and two items under the outcome domain. The appraisal was performed by four independent review authors (JFW, SPN, ERCO, and MI), where discrepancies were resolved by consensus.
Data extraction
The data were extracted by two review authors (SPN and ERCO) and double-checked by the other two (MI and JFW). Data extraction was carried out on characteristics of the patients, such as the number of patients, age, sex, and body mass index (BMI). Additionally, we extracted information on the laboratory methods used to measure serum 25(OH)D levels, including HPLC, ELISA, CLIA, automated immunoassays, and RIA. Continuous data were expressed in mean ± standard deviation (SD), while categorical data were expressed as frequency. If the continuous variables were reported as medians, the values were converted to means and standard deviations using the approach reported previously. Data on serum 25(OH)D and its measurement techniques were extracted as well. Serum 25(OH)D levels expressed in mmol/L or µg/L units were converted to ng/mL. In cases where any of the expected data points were unavailable in the full-text articles, we recorded them as “not reported (NR).” Data on the human development index (HDI) and national income were collected from the United Nations Development Programme and World Bank, respectively.
Statistical analysis
Data were analyzed through pooled analysis using a maximum restricted likelihood by computing the estimated pooled proportion and its 95% confidence interval (95% CI). During the analysis, the Freeman–Tukey double arcsine transformation was applied to the proportion extracted from the original study. The pooled estimate or proportion and its 95% CI were backtransformed to the original value. The prevalence was calculated by multiplying the back-transformed values by 100%. Heterogeneity was judged based on I2 > 50% or p-Het < 0.1. A meta-regression was performed using total sample size, age, BMI, ratio of male-to-female, and HDI as the moderators. Subgroup analysis was performed based on year of the study conducted (2010‒2014, 2015‒2019, and 2020‒2024), the BMI (cut-off: 28 kg/m2), national income (high, upper-middle, lower-middle, and low), region (North America, Europe, Asia, Middle East and North Africa, Sub-Saharan Africa, Oceania, and Latin America, and HDI (low, moderate, high, and very high). For the meta-regression and subgroup analysis, a p-value < 0.05 was used as the statistical significance cut-off. All the statistical analysis was carried out on RStudio (2024.04.2 Build 764) with metafor package (Viechtbauer, 2010).
Results
Included studies
The screening and selection process of the eligible studies was summarized in a PRISMA flowchart and presented in Figure 1. Identification of studies via six scientific databases yielded 1695 reports, of which 802 were identified as duplicates and removed. Thereafter, 893 were screened through title and abstract, 717 of which were excluded due to irrelevance. Out of 176 studies, eight reports were not retrievable for their full text. The remaining records were excluded due to being conference abstracts (n = 22), duplicates (n = 3), or commentaries (n = 3). After evaluating the remaining 140 full texts, as many as 114 were further excluded by applying the eligibility criteria. Fifteen reports were excluded because they used different vitamin D deficiency cut-offs other than 20 ng/mL (Alkan, 2017; Annamalai, 2018; Bergink, 2009; Bhalla et al., 2018; Bischoff-Ferrari et al., 2005; Kim et al., 2015; Kumar, 2023; Lotfi, 2014; Ramasamy, 2021). Among those with ineligible study designs, three records were initially considered but ultimately excluded because they were interventional studies (Zheng et al., 2017, 2018, 2019). Two studies were almost included but finally excluded due to the wrong population, as they recruited patients with hip OA or unspecified OA (Montemor et al., 2021; Zhang et al., 2014). Among 16 reports with uncategorized serum 25(OH)D deficiency status, seven of which were almost included, but eventually were excluded (Askari et al., 2021; Ghosh et al., 2014; Park and Park, 2021; Udomsinprasert et al., 2020; Valdes et al., 2004; Yağmur Tekeli et al., 2022; Yu et al., 2023). Finally, a total of 26 studies were included in our analysis (Abu el Maaty et al., 2013; Al-Jarallah et al., 2011; Alabajos-Cea et al., 2021; Amini et al., 2021; Astariyani and Zaki, 2022; Barker et al., 2014; Başkan et al., 2018; Cakar et al., 2018; Elbashir et al., 2023; Glover et al., 2012; Glover et al., 2015; Guler et al., 2014; Güler et al., 2015; Hariprasad et al., 2023; Javadian et al., 2017; Lee et al., 2016; Levinger et al., 2017; Manoy et al., 2018; Mohamed et al., 2015; Namutebi et al., 2021; Olama et al., 2016; Putra et al., 2024; Shea et al., 2018; Velangi et al., 2019; Wahyudi et al., 2021; Zafeiris et al., 2021).
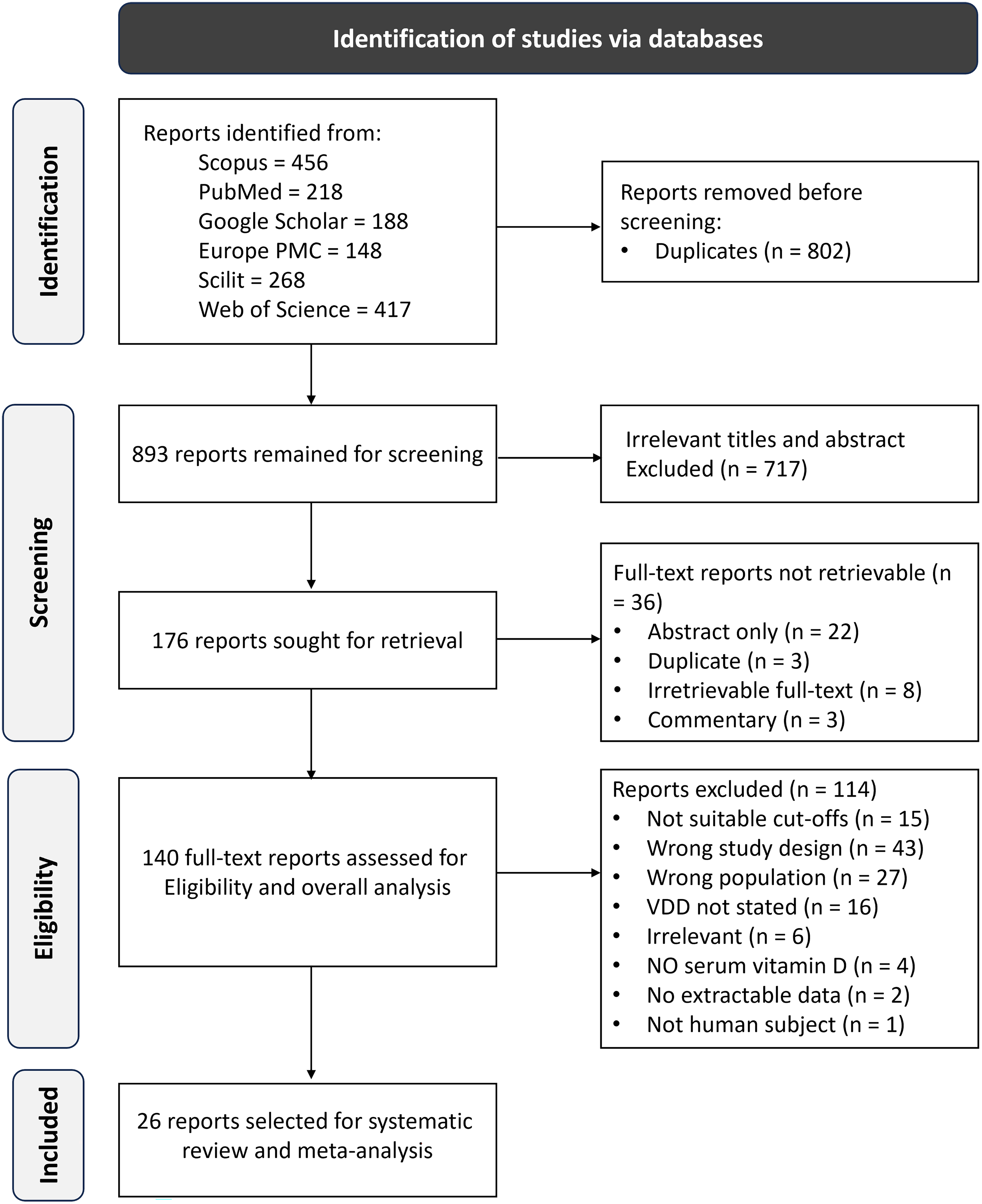
PRISMA flowchart illustrating the screening and selection process of eligible studies.
Characteristics
Characteristics of the included studies are presented in Table 1. Most of the studies were from the USA and Türkiye, with four studies each. Three studies were from Indonesia, while others were from Iran, Egypt, Saudi Arabia, and India, respectively. Only a single study employed a cohort design (Shea et al., 2018), while others were cross-sectional (Abu el Maaty et al., 2013; Al-Jarallah et al., 2011; Alabajos-Cea et al., 2021; Amini et al., 2021; Astariyani and Zaki, 2022; Barker et al., 2014; Başkan et al., 2018; Cakar et al., 2018; Elbashir et al., 2023; Glover et al., 2012; Glover et al., 2015; Guler et al., 2014; Güler et al., 2015; Hariprasad et al., 2023; Javadian et al., 2017; Lee et al., 2016; Levinger et al., 2017; Manoy et al., 2018; Mohamed et al., 2015; Namutebi et al., 2021; Olama et al., 2016; Putra et al., 2024; Velangi et al., 2019; Wahyudi et al., 2021; Zafeiris et al., 2021). Participants recruited in the included studies were mostly aged between 48.59 years and 74.67 years, with having mean BMI ranging from 25.1 to 33.78 kg/m2. Twenty-three studies were dominated by women, five of which exclusively recruited women as their subjects (Abu el Maaty et al., 2013; Guler et al., 2014; Güler et al., 2015; Shea et al., 2018; Wahyudi et al., 2021). There were 12 studies having participants with mean 25(OH)D level > 20 ng/mL (Abu el Maaty et al., 2013; Alabajos-Cea et al., 2021; Amini et al., 2021; Barker et al., 2014; Glover et al., 2012; Glover et al., 2015; Javadian et al., 2017; Levinger et al., 2017; Manoy et al., 2018; Namutebi et al., 2021; Zafeiris et al., 2021), while others were below < 20 ng/mL or did not report the value (Al-Jarallah et al., 2011; Astariyani and Zaki, 2022; Başkan et al., 2018; Cakar et al., 2018; Elbashir et al., 2023; Guler et al., 2014; Güler et al., 2015; Hariprasad et al., 2023; Lee et al., 2016; Mohamed et al., 2015; Olama et al., 2016; Putra et al., 2024; Shea et al., 2018; Velangi et al., 2019; Wahyudi et al., 2021).
Characteristics of the included studies reporting the prevalence of vitamin D deficiency among knee OA patients.
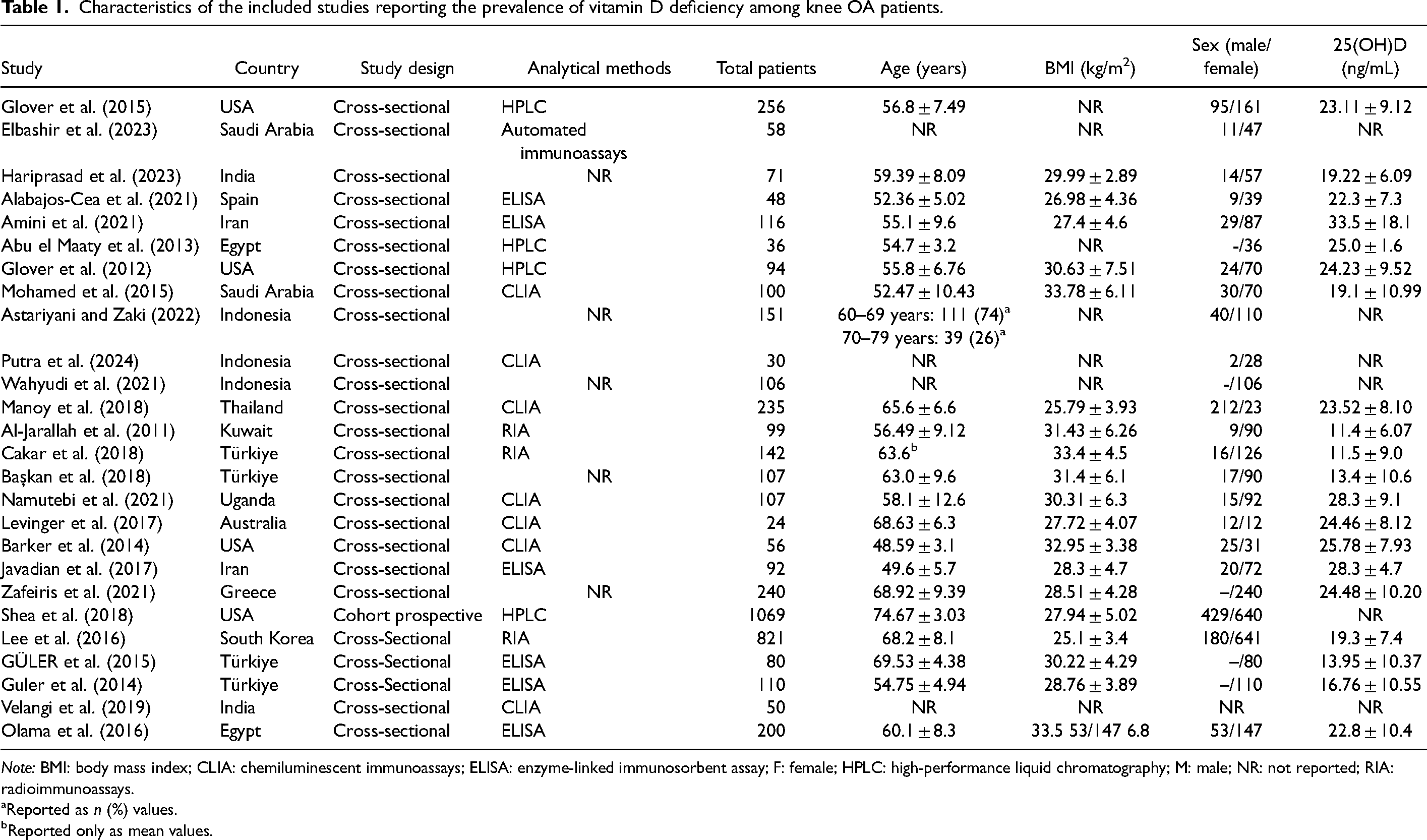
Note: BMI: body mass index; CLIA: chemiluminescent immunoassays; ELISA: enzyme-linked immunosorbent assay; F: female; HPLC: high-performance liquid chromatography; M: male; NR: not reported; RIA: radioimmunoassays.
Reported as n (%) values.
Reported only as mean values.
Global prevalence (2010–2024)
The pooled proportion for the global prevalence of vitamin D deficiency among patients with OA is presented in Figure 2A. In individual studies, the prevalence spanned from 14% (95% CI: 8‒21) (Levinger et al., 2017) to 94% (95% CI: 88‒98) (Al-Jarallah et al., 2011). The overall prevalence was estimated at 56.72% (95% CI: 46.93–66.25), based on a total of 4248 patients included in the analysis. The heterogeneity is significant as the I2 was 97.56% (p-Het < 0.001).
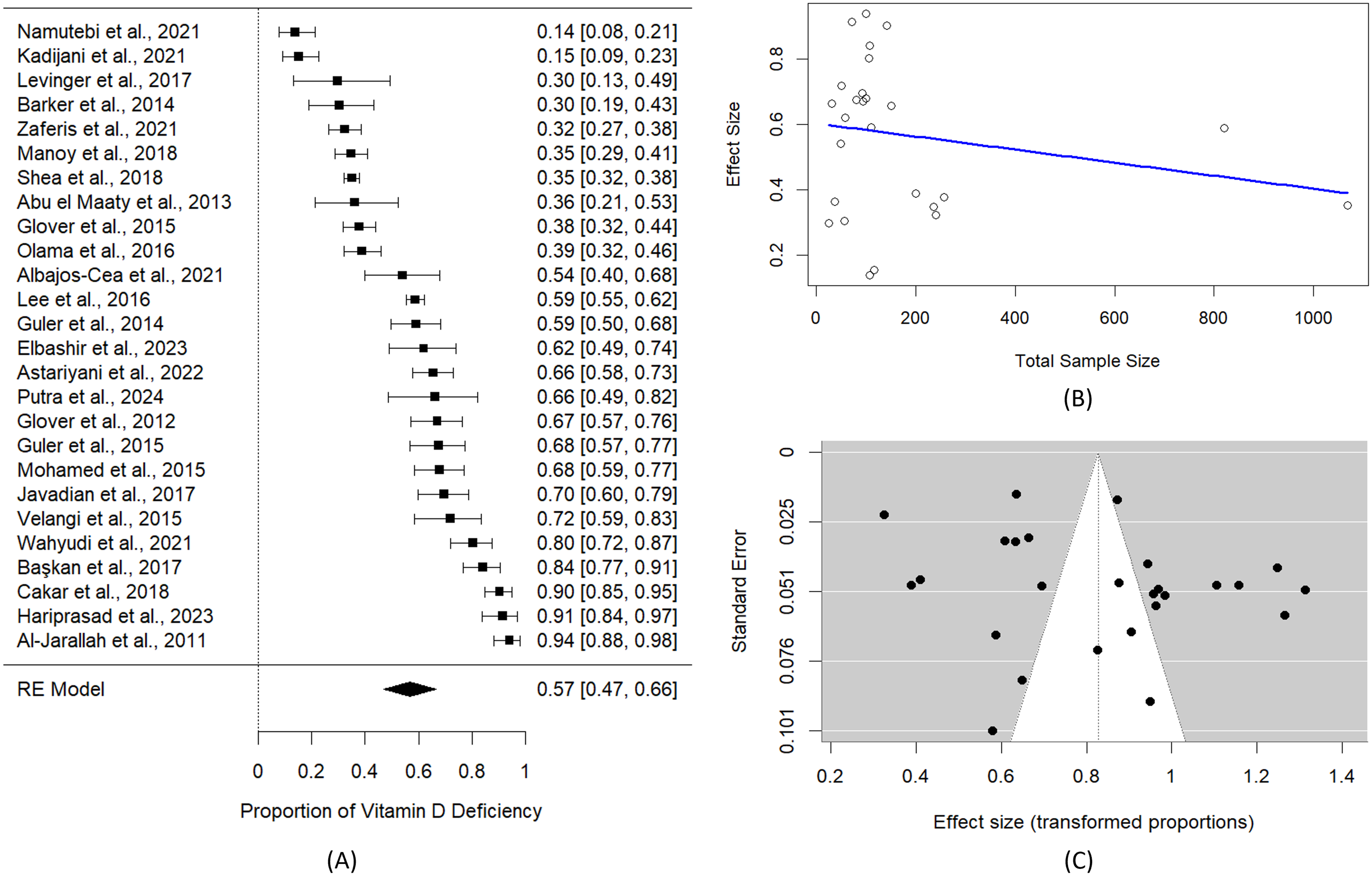
Forest plot for the proportion of vitamin D deficiency among knee OA population estimated using random-effects model and Freeman–Tukey double arcsine transformation (A). Bubble plot for the meta-regression of the vitamin D deficiency proportion with total sample (B). Begg's funnel plot for publication of bias reporting the vitamin D deficiency prevalence among patients with knee OA. Kendall's tau = 0.0109; p-Begg's = 0.941 (C).
Reporting quality
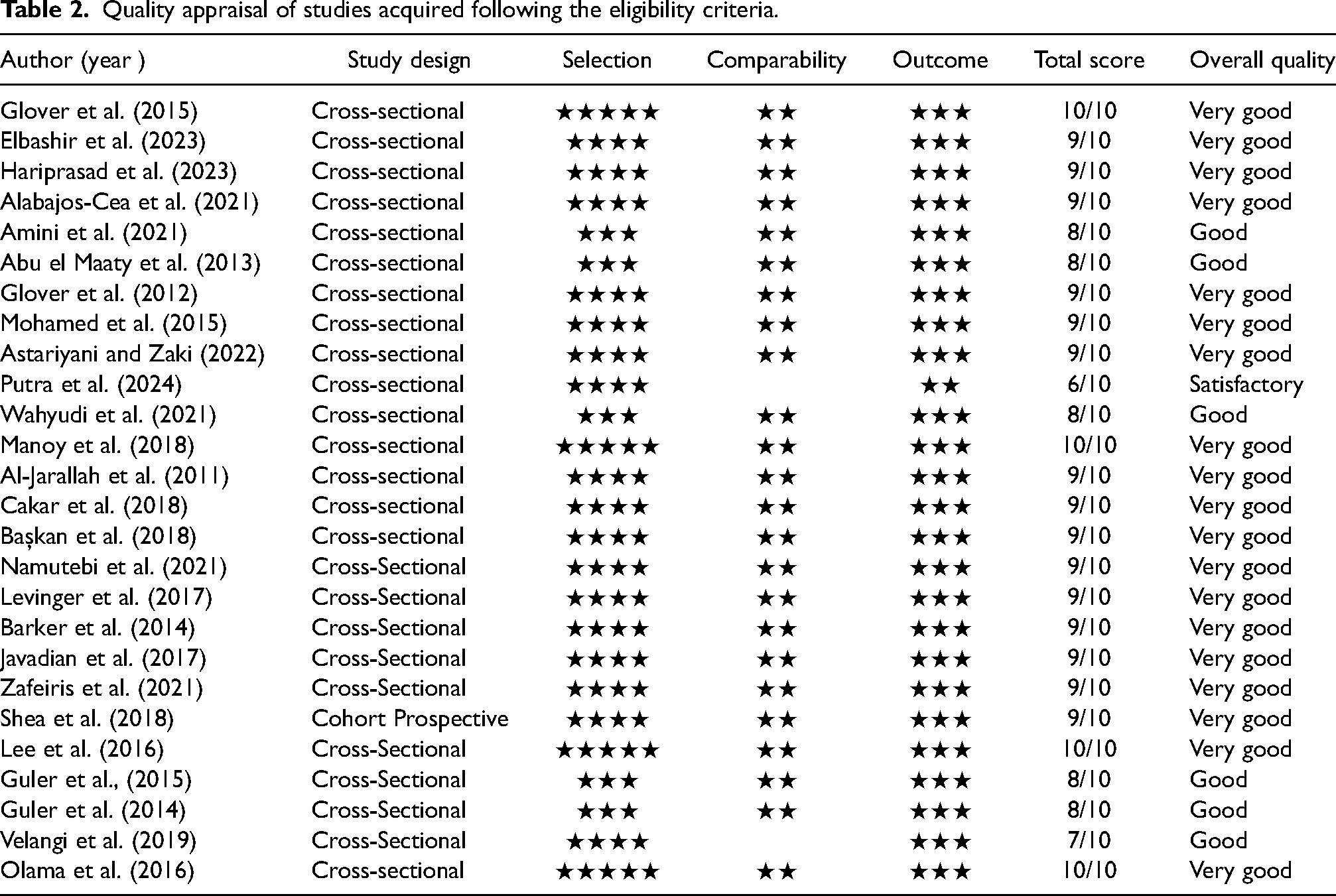
The quality appraisal results based on the NOS for cross-sectional and cohort studies are presented in Table 2. Nineteen studies have a “very good” score because the use of data sampling, data collection, and data analysis is exceptional (Al-Jarallah et al., 2011; Alabajos-Cea et al., 2021; Astariyani and Zaki, 2022; Barker et al., 2014; Başkan et al., 2018; Cakar et al., 2018; Elbashir et al., 2023; Glover et al., 2012; Glover et al., 2015; Güler et al., 2015; Hariprasad et al., 2023; Javadian et al., 2017; Lee et al., 2016; Levinger et al., 2017; Manoy et al., 2018; Mohamed et al., 2015; Olama et al., 2016; Shea et al., 2018; Zafeiris et al., 2021). The six studies have an overall quality of ‘good’, with the concern that the sample size is inadequate and does not represent the overall population (Abu el Maaty et al., 2013; Amini et al., 2021; Guler et al., 2014; Güler et al., 2015; Velangi et al., 2019; Wahyudi et al., 2021). Then, one study that contained “satisfactory” quality, as the data analysis was not available (Putra et al., 2024).
Quality appraisal of studies acquired following the eligibility criteria.
Meta-regression
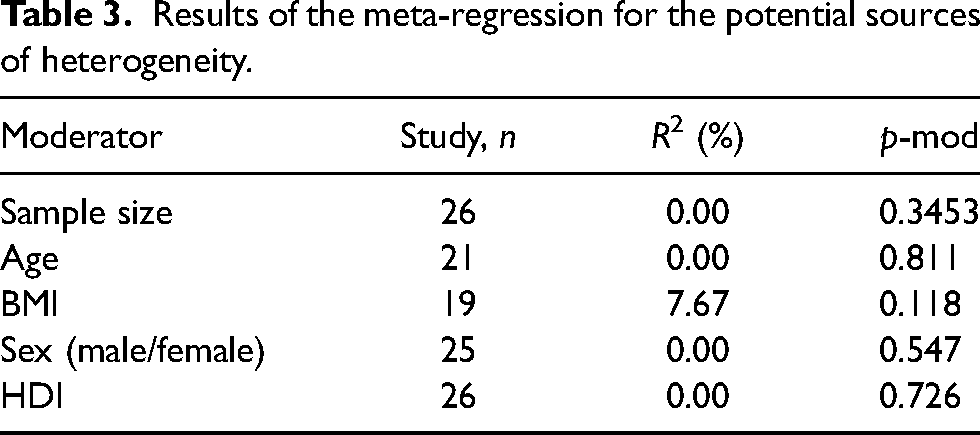
The results of meta-regression analysis are presented in Tables 2–4. The results showed that sample size did not explain the observed heterogeneity (p = 0.396). The bubble plot where the sample size acted as the moderator is presented in Figure 2B. Similarly, age (p = 0.811), sex (p = 0.547), and HDI (p = 0.726) were not significant moderators. However, BMI accounted for 7.67% of the between-study variance and approached statistical significance (p = 0.118).
Results of the meta-regression for the potential sources of heterogeneity.
Subgroup analysis of vitamin D deficiency among patients with knee osteoarthritis.
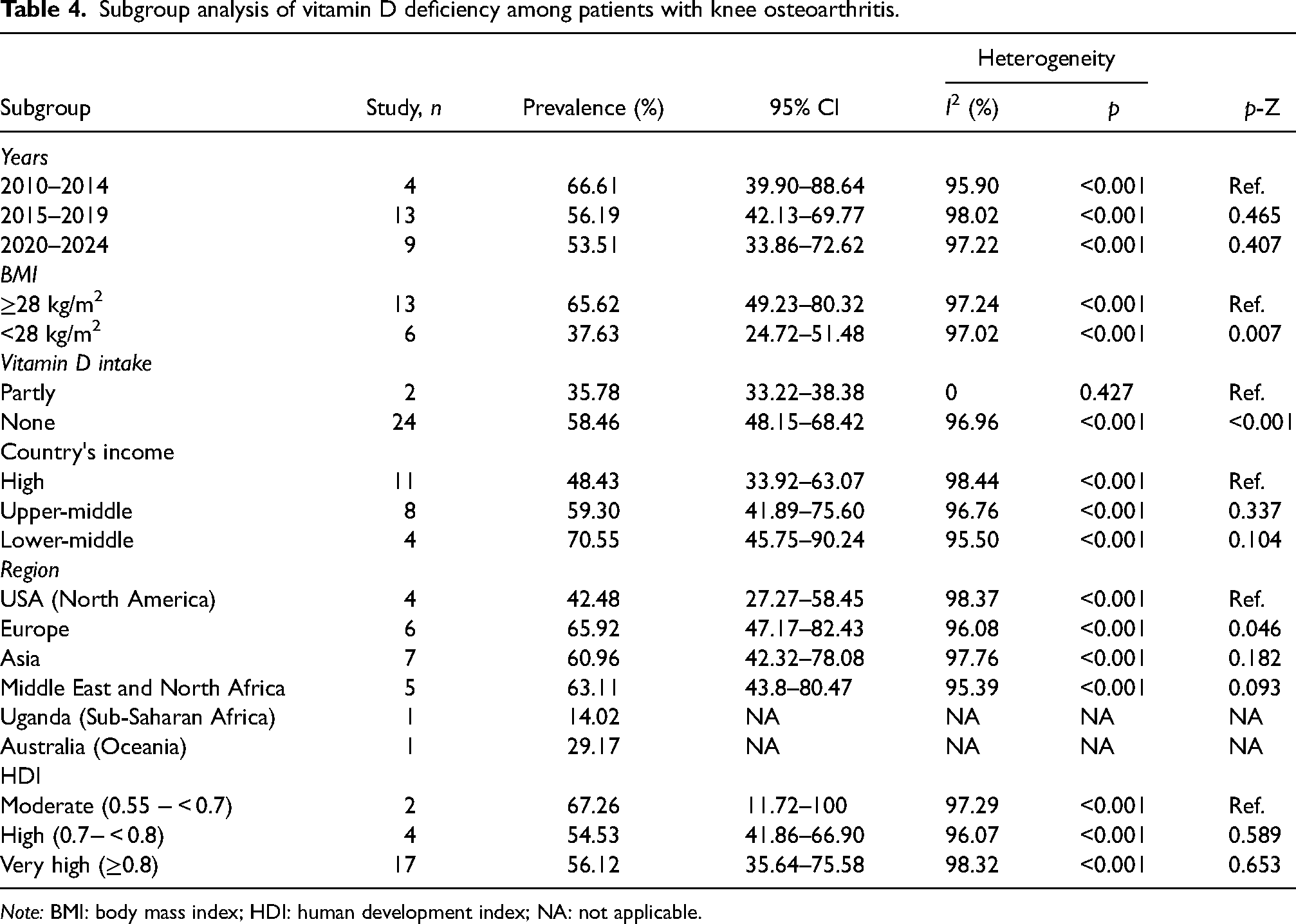
Note: BMI: body mass index; HDI: human development index; NA: not applicable.
Subgroup analysis
Subgroup analyses indicated significant differences in vitamin D deficiency prevalence across various factors. Patients with a BMI ≥ 28 kg/m² exhibited a prevalence of 65.62% (95% CI: 49.23‒80.32), which was significantly higher compared to those with a BMI < 28 kg/m², who had a prevalence of 37.63% (95% CI: 24.72‒51.48) with a p-value of 0.010. There was a significant difference in the pooled prevalence of vitamin D deficiency between studies that included patients receiving vitamin D supplementation and those that did not (p < 0.001). When compared to the prevalence in the USA, a significantly higher prevalence was observed in Europe (65.92% [95% CI: 47.17‒82.43]) with a p-value of 0.046. Other factors, including the year of study, the country's income, and HDI, did not demonstrate statistically significant differences.
Publication bias
The Begg's funnel plot analysis revealed no evidence of significant publication bias (Figure 2C). The plot exhibited a relatively symmetrical distribution of effect sizes around the overall estimate, with Kendall's tau value of 0.0109 and a p-value of 0.941, indicating a lack of bias in the included studies.
Discussion
Our findings reveal a high prevalence of vitamin D deficiency among individuals with OA, with an estimated pooled rate of 56.72% (95% CI: 46.93‒66.25). To our knowledge, this is the first epidemiological meta-analysis to estimate the global prevalence of vitamin D deficiency specifically among patients with OA. As an observational synthesis, the study does not aim to establish causality but instead highlights the distribution and magnitude of deficiency across populations. Notably, higher prevalence estimates were observed in groups with an average BMI > 28 kg/m² and among those not receiving vitamin D supplementation. Compared to osteoporosis patients, for whom a previous meta-analysis reported a prevalence of 18.3% (95% CI: 16.2‒20.7) (Salari et al., 2021), vitamin D deficiency appears more common in the OA population. Among Romanian adults, the prevalence reached 29.5% in a cohort of 1741 obese individuals (Brîndușe et al., 2024). Another study reported that vitamin D deficiency affected 90.2% of individuals with obesity (n = 342) (Alzahrani et al., 2024), reinforcing the association between higher BMI and reduced vitamin D status.
As reported in a review by Pludowski and colleagues, obesity significantly increases the risk of vitamin D deficiency, driven by multiple mechanisms including sequestration of vitamin D in adipose tissue, reduced cutaneous synthesis due to limited physical activity and sun exposure, altered dietary habits, and impaired hepatic 25-hydroxylation, particularly in the presence of fatty liver disease (Pludowski et al., 2024). As suggested in a previous research, severe obesity exacerbates mobility constraints among OA patients and subsequently reduces sunlight exposure (Messier et al., 2024). Moreover, the combination of obesity and OA may also intensify systemic inflammation, leading to vitamin D catabolism via CYP24A1 modulation (Iriani et al., 2024; Khan et al., 2025). Obesity is a low-grade systemic inflammatory disease characterized by the secretion of pro-inflammatory cytokines such as interleukin-6 (IL-6), tumor necrosis factor alpha (TNF-α), and C-reactive protein (Binvignat et al., 2024). In patients with OA, particularly those who are obese, systemic inflammation is further elevated due to the additive effect of joint-derived inflammatory mediators (Binvignat et al., 2024). Additionally, vitamin D receptor (VDR) expression may be downregulated by pro-inflammatory cytokines (Li et al., 2024). In the gut, reduced VDR expression may impair transcriptional programs that maintain epithelial barrier integrity and nutrient transport (Kellermann et al., 2024; Li et al., 2024), potentially diminishing the efficiency of calcium—and thereby vitamin D—uptake from diet or supplements.
The present study further found that the prevalences reached 42.48% (95% CI: 27.27‒58.45), 65.92% (95% CI: 47.17‒82.43), 60.96% (95% CI: 42.32‒78.08) and 63.11% (95% CI: 43.8‒80.47) in North America (represented by USA), Europe, Asia, and Middle East and North Africa, respectively. For the Sub-Saharan African and Oceania regions, the prevalences were only reported from Uganda (14.02%) and Australia (29.17%), respectively. Among osteoporosis patients, the pooled prevalence was found to be highest in the African population, reaching 39.5% (95% CI: 22.3‒59.7) (Salari et al., 2021). The prevalence of vitamin D deficiency (cut-off 30 nmol/L) in Africa among the general population was estimated to be 17·31% (95% CI: 9.86‒26.27) (Mogire et al., 2020). Among South Asian countries, the prevalence of vitamin D deficiency among the general population reached over 60% (Siddiqee et al., 2021). A meta-analysis on the Asian general population suggested that the prevalence surpassed 20% (Jiang, 2023).
Low prevalence of vitamin D deficiency in the USA might be attributed to the supplement intake along with the type of foods consumed (Lips, 2021; Polzonetti V, 2020). Fish, mushrooms, Reindeer lichen, and fish liver oils are rich sources of cholecalciferol and ergocalciferol, but fortification of vitamin D is still required (Benedik, 2022). Other various factors that contribute to the high prevalence of vitamin D deficiency in certain populations include pigmented skin, environmental pollution, and most importantly, traditional clothing that restricts sunlight exposure (i.e., Middle Eastern and Indian women) (Habeeba, 2021). Additionally, obese individuals are at risk of being deficient in circulating vitamin D due to the excessive absorption of the molecule by adipose tissues (Marzban, 2021; Simon, 2020).
A previous study revealed that a low serum 25(OH)D level was associated with OA in patients who underwent arthroplasty (Dadra, 2019). In addition, another study found that a notable number of patients undergoing total knee arthroplasty for knee OA had insufficient vitamin D levels (Heidari, 2011). Vitamin D has a significant impact on various processes such as changes in bone mechanical properties, increased bone resorption by elevating parathyroid hormone levels, raising bone turnover, and directly impacting articular chondrocytes through vitamin D metabolites, particularly 1,25(OH)2D3 (Min, 2021; Skalny et al., 2023). As a result, a deficiency in vitamin D can disrupt the balance of bone remodeling, which consequently leads to weakened subchondral bone (Saponaro, 2020; Yu, 2021). It is worth mentioning that beyond musculoskeletal complications, diminished serum 25(OH)D levels in this population suggest a double vulnerability to comorbidities, such as cardiovascular disease, type 2 diabetes, impaired immune regulation, and sarcopenia (Skalny et al., 2024).
Vitamin D deficiency has been implicated in endothelial dysfunction, arterial stiffness, and dysregulation of the renin–angiotensin–aldosterone system, all of which contribute to increased cardiovascular risk (Iqhrammullah et al., 2024; Iqhrammullah et al., 2024; Nardin et al., 2024). Moreover, insufficient vitamin D is associated with impaired immune regulation, increased systemic inflammation, and greater susceptibility to metabolic disorders such as type 2 diabetes and insulin resistance, further compounding the health burden in OA patients (Iqhrammullah et al., 2024; Wimalawansa, 2024; Xiong et al., 2024). In line with this, serum 25(OH)D screening has been endorsed in several national health programs, particularly for older adults and individuals at high risk of deficiency (Brîndușe et al., 2024; Wiedemann et al., 2025). However, considering our findings, individuals with OA—especially those with elevated BMI—should be included as a target group for routine vitamin D screening.
The interpretation of our findings is limited due to significant heterogeneity found across studies, even after subgroup analyses, which may reflect variations in study populations, measurement techniques, and unreported confounders. Although we limited our inclusion to studies using the ≤20 ng/mL cut-off, assay variability and methodological differences in measuring serum 25(OH)D levels could still affect comparability. Further, some geographic regions, such as Sub-Saharan Africa and Oceania, were represented by only one study each, which limits generalizability across global populations. Most included studies recruited predominantly female or older adult populations, which may not reflect vitamin D status in younger individuals or males with knee OA. In addition, potential small-study effects or underreporting in low- and middle-income countries may skew the global prevalence estimates. The exclusion of non-English articles may also have introduced language bias.
Future studies should adopt standardized cut-offs and validated assays to improve cross-study comparability. There is a need for prospective cohort designs to explore how vitamin D deficiency develops and progresses among OA patients over time. Randomized controlled trials are also warranted to examine the effectiveness of supplementation in this population, particularly with adjusted dosing that reflects updated knowledge on the U-shaped relationship between vitamin D levels and health outcomes (García-Gavilán et al., 2021; Rizzoli, 2021). Moreover, greater attention should be given to underrepresented regions and diverse demographic groups to ensure a more globally relevant understanding of vitamin D deficiency in knee OA.
Conclusion
The global prevalence of vitamin D deficiency among patients with knee OA is high, affecting over half of the population studied (56.72%). The deficiency was more pronounced in individuals with a BMI ≥28 kg/m2 and in those who did not receive vitamin D supplementation. Geographic disparities were evident, with Europe, Asia, the Middle East, and North Africa reporting higher prevalence rates compared to North America. However, HDI and national income level did not consistently explain the variation. Given the high prevalence, there is a need for proactive screening of vitamin D status in knee OA patients, particularly in high-risk subgroups such as those with obesity and those residing in regions with higher reported deficiency. Clinicians should consider targeted supplementation strategies, and health systems should incorporate vitamin D monitoring into OA management guidelines. Even though the clinical outcomes related to OA progression remain inconclusive, the systemic impact of vitamin D deficiency should not be overlooked, as it may affect immune regulation, muscle strength, metabolic health, and cardiovascular function—factors that are also relevant to the overall well-being of knee OA patients. Further research is needed to determine the clinical benefit of supplementation in modifying disease progression and improving functional outcomes. Further research is needed to determine the clinical benefit of supplementation in modifying disease progression and improving functional outcomes. Comprehensive assessments with long-term follow-up are essential to clarify the causal relationship between vitamin D deficiency and OA severity, as well as its broader systemic effects.
Footnotes
Authors’ contributions
Muhammad Iqhrammullah contributed in conceptualization, methodology, investigation, formal analysis, data visualization, and writing of original draft. Juan Fransiscus Wira contributed in investigation. Samuel Partogi Nababan contributed in investigation. Eunice Rima Christy Oey contributed in investigation. Seba Talat AL-Gunaid contributed in investigation and writing of original draft. Andhika Citra Buana contributed in validation and writing of original draft. Naufal Gusti contributed in validation. Muhammad Habiburrahman contributed in validation, supervising, and revision and editing. Radi Muharris Mulyana contributed in validation, supervising, and revision and editing.
Availability of data and materials
All underlying data have been presented in this article.
Consent for publication
All authors have read and agreed to the final version of the manuscript. All authors approved the publication of this work in the Journal of Nutrition and Health.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical statement
Since this study is a systematic review and meta-analysis that uses publicly available secondary data from previously published studies, ethical approval is not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.