
Abstract
Background
Schizophrenia and depression are disabling mental disease conditions that have multifactorial pathophysiology involving the dysregulation of the gut–brain axis. Probiotics have been advocated as an adjunct therapy that could have an impact on psychiatric symptoms by normalizing the gut immune mechanisms.
Aims
This meta-analysis evaluated whether probiotic supplementation improves psychiatric symptoms in patients with schizophrenia or depression.
Methodology
A systematic search of multiple databases identified randomized controlled trials (RCTs) that tested probiotic interventions in these populations. Eligible studies were analyzed for pooled effect sizes, heterogeneity, and publication bias.
Findings
Thirteen RCTs (n = 893 participants) were included. Meta-analysis revealed no significant difference in PANSS score reduction between probiotic and placebo groups of schizophrenia patients (P = .546). However, a significant pooled standardized mean difference between intervention and control groups was found (P = .043). Significant heterogeneity was observed, and subgroup analyses indicated variations in outcomes based on geographic region and ethnicity. A potential moderating effect of vitamin D status was identified as a factor requiring future study.
Conclusion
Currently, there is no evidence that probiotics consistently improve depression or schizophrenia. The significance of subgroup analysis raises questions and emphasizes the necessity of carefully planned, sufficiently powered studies to determine whether probiotic efficacy is influenced by particular populations, settings, or supplemental techniques.
Keywords
Introduction
Mental illness, which is defined by abnormal emotion, behavior, or thought, is suffered by some 970 million individuals globally (World Health Organization, 2022). These disorders significantly reduce quality of life, and schizophrenia, depression, and bipolar disease, respectively, constitute three of the five highest contributors to disability globally, causing 2.8% and 11.8% of the disability burden, respectively (Whiteford et al., 2015; World Health Organization, 2017). The precise etiology and pathophysiology are still unknown although socioeconomic and genetic determinants have been influenced mental health, spurring exploration of alternate mechanisms—specifically the microbiota–gut–brain axis.
The human gut harbors a diverse microbial ecosystem of up to 100 trillion organisms, including bacteria, viruses, fungi, archaea, and parasites (Rieder et al., 2017; Yang et al., 2020). Over 1000 bacterial species colonize the adult gut (Bermon et al., 2015), and emerging evidence suggests their interactions with neural and immune pathways may influence brain function through the bidirectional gut–brain axis (Carabotti et al., 2015; Halverson and Alagiakrishnan, 2020; Jabrink-Sehgal and Andreasson, 2020; Madabushi et al., 2023; Socala et al., 2021). Gut dysbiosis, in particular, has been associated with altered gut permeability and chronic inflammation, both of which are implicated in mental illness (Safadi et al., 2022).
Probiotics—live microbes that offer health effects to the host—have thus been examined as adjunct therapy of psychiatric illness such as schizophrenia, depression, and anxiety (Alli et al., 2022; Genedi et al., 2019; Johnson et al., 2021, 2023; Merkouris et al., 2024; Reninghaus et al., 2020; Schaub et al., 2022). Postulated mechanisms of action involve the improvement of intestinal motility, reinforcement of gut barrier integrity, and modulation of microbial composition and immune signaling (Hemarajata and Versalovic, 2012; Petrariu et al., 2024; Thomas and Greer, 2010). Some strains, such as Lactobacillus rhamnosus and Lactobacillus plantarum PS128, have been demonstrated preclinically to modulate neurotransmitter circuits such as GABA, dopamine, and serotonin (Akkasheh et al., 2016; Foster et al., 2016; Liu et al., 2016), whilst others of the genera Lactobacillus and Bifidobacterium have been demonstrated to be related to stress, sleep, and inflammation (Johnson et al., 2023; Lee et al., 2021).
In spite of these mechanistic theories, clinical evidence is still conflicting to date. A number of trials show no or very small impacts of probiotics on depression, stress, or mood endpoints versus placebo (Rao et al., 2009; Chung et al., 2014; Ng et al., 2018; Amirani et al., 2020; Sequeira et al., 2022). These differences may be due to small sample sizes, short study periods, and strain variability of probiotics. To clarify the ambiguity, the current meta-analysis compares the effectiveness of probiotics on clinical symptoms of depression and schizophrenia and provides a test of whether adjunctive supplementation of vitamin D alters these effects.
Methodology
Literature search and selection
Studies published between 2010 and December 2024 were selected using the databases of PubMed and Scopus. The studies were searched based on keywords of “probiotics” and “schizophrenia” OR “depression.” Meta-analysis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.”
Inclusion criteria
The following inclusion criteria were used for study eligibility:
Articles published in the English language Articles reporting randomized controlled trials Patients were diagnosed with schizophrenia or depression or bipolar disorder using standard diagnostic methods Both the intervention and the placebo were included Sufficient data for the clinical symptom improvement calculation were presented Probiotic supplementation was reported Age range (both adults and adolescents) Self-reported depressive symptoms
Exclusion criteria
The exclusion criteria were as follows:
Articles using non-human subjects Non-research articles, including reviews, meta-analyses, overviews, and books
Data extraction
The information of the first author's name, publication year, sample size, demographic characteristics such as gender and age, illness types, diagnostic method, types of probiotics used, and clinical symptoms improvement were extracted from each selected article.
Data analysis
The difference in clinical symptoms improvement between interventions and placebo was analysed using Comprehensive Meta-Analysis (CMA) version 2. Random-effects size models were used to pool effect sizes and 95% confidence intervals (CIs). The heterogeneity was presented using I-squared and the Q statistic value. Publication bias was tested with Egger's test, while the trim-and-fill test was used when the bias was present. Egger's regression tests and trim-and-fill procedures were applied only to the PANSS score for schizophrenia and the pooled standardised mean difference between intervention and control groups of depression, which precluded reliable assessment of publication bias.
The methodological quality of the included randomized controlled trials was evaluated using the Cochrane Risk of Bias tool (Review Manager version 5.4). Two independent reviewers assessed the following domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other potential sources of bias. Discrepancies were resolved by consensus. Separate risk-of-bias evaluations were performed for schizophrenia and depression studies.
Dietary interactions and genetic background may play essential roles in treatment response. Therefore, subgroup analyses were conducted to determine whether the effects of the intervention varied by (1) ethnic group and (2) vitamin D co-supplementation status. Subgroup analyses were performed to determine the effect of different ethnics based on their diet (Western countries, Asia, Iran) and co-supplementation (vitamin D) on schizophrenia and depression patients. The analyses were performed if a minimum of two studies existed within each subgroup. A P value of <.05 was considered as statistically significant.
Four distinct instruments (BDI, HAM-D, HDRS-24, and MADRS) with differing sensitivity and scoring ranges were used to assess depressive symptoms in the included studies. Cross-scale comparability was made easier by expressing effect sizes as standardized mean differences (SMDs) with 95% confidence intervals in order to address this heterogeneity.
Results
A total of 13 studies were eligible after the literature review. Seven studies included schizophrenia patients, six consisted of depressive patients, and we could not find any study that involved bipolar disorder patients (Figure 1). Study characteristics of the included studies are presented in Table 1. A total of 893 subjects (454 patients and 439 placebo) were included in this meta-analysis. In these studies, probiotic interventions lasted 4–14 weeks (mean 10.07 weeks). Findings across durations were inconsistent, with some short and long trials. However, the role of treatment duration could not be determined due to no formal subgroup analysis by duration was conducted.
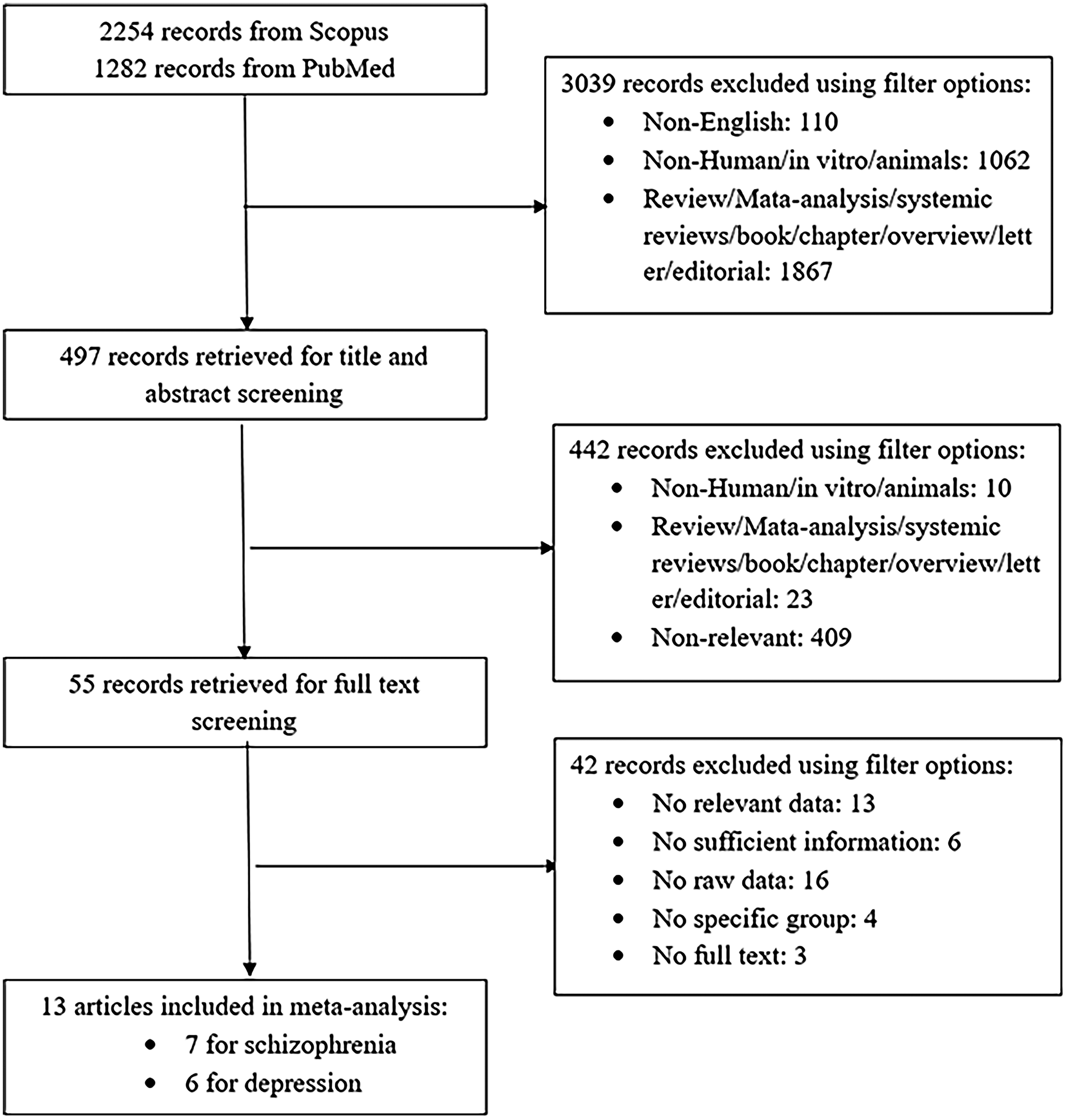
Flow diagram of study selection for meta-analysis of the impact of probiotics on clinical symptoms of schizophrenia and depression.
Summary table of included studies.
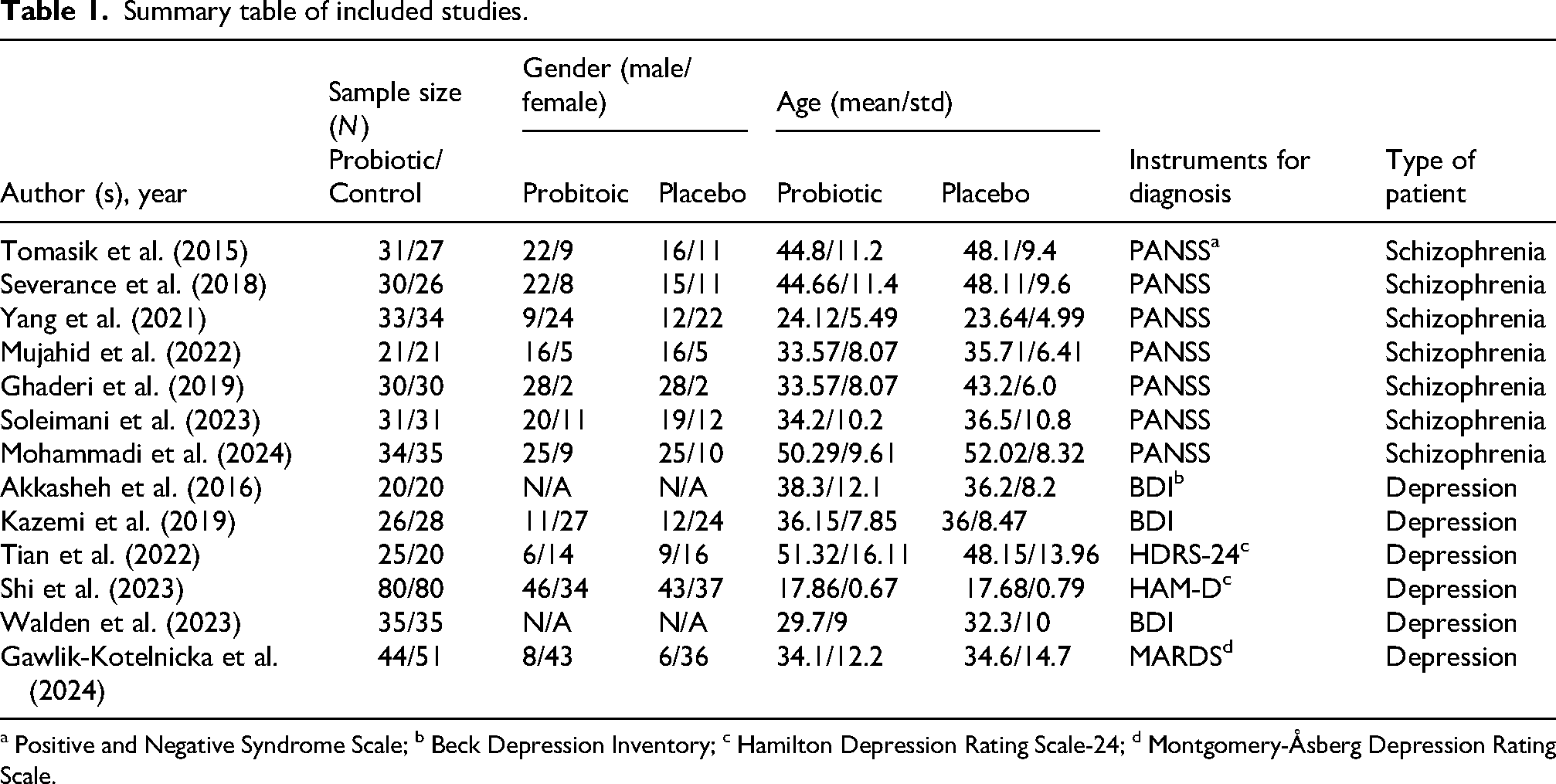
a Positive and Negative Syndrome Scale; b Beck Depression Inventory; c Hamilton Depression Rating Scale-24; d Montgomery-Åsberg Depression Rating Scale.
Study characteristics and quality
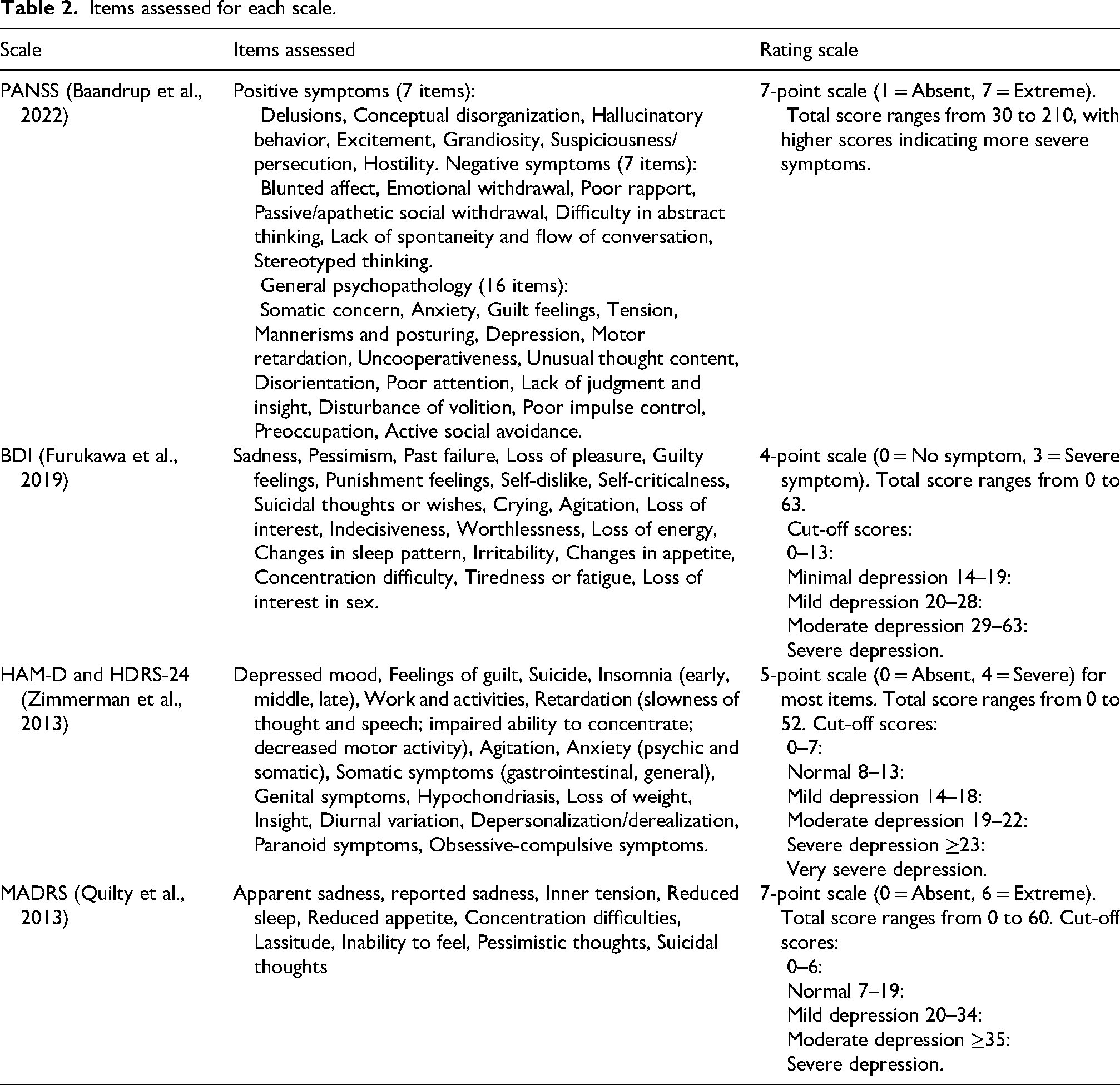
Table 1 summarizes the characteristics of the included studies, including study title, sample size, mean age, and gender distribution. In the seven studies of schizophrenia, symptom severity was assessed using the scale of PANSS. Besides, the status of depression reported in the included studies was assessed using four different questionnaires: BDI, HAM-D, HDRS-24, and MADRS. The score for each scale is summarized in Table 2.
Items assessed for each scale.
Risk-of-bias assessments were conducted using the Cochrane Risk of Bias tool. The summarized results for schizophrenia and depression studies are provided in Supplementary Figures 1 and 2, respectively, which highlight variability in methodological rigor across the included trials.
Publication bias
Publication bias was assessed using funnel plots, Egger's regression test, and the trim-and-fill method. The funnel plots showed no clear asymmetry, Egger's test was not significant (P > .05), and no missing studies were imputed by the trim-and-fill method. Together, these findings indicate little evidence of publication bias.
Probiotics
The intervention across studies involved various probiotic capsules containing different strains and concentrations of beneficial bacteria, such as Lactobacillus (e.g., L. rhamnosus, L. casei, L. plantarum), Bifidobacterium (e.g., B. bifidum, B. longum), Streptococcus salivarius, Bacillus coagulans, and Enterococcus. Some formulations were additionally fortified with vitamin D. Among the 13 included studies, 11 used probiotics alone, while 2 combined probiotics with vitamin D supplementation. Table 3 summarizes each study's design, follow-up duration, probiotic species, and dosages.
Probiotic used for each study.
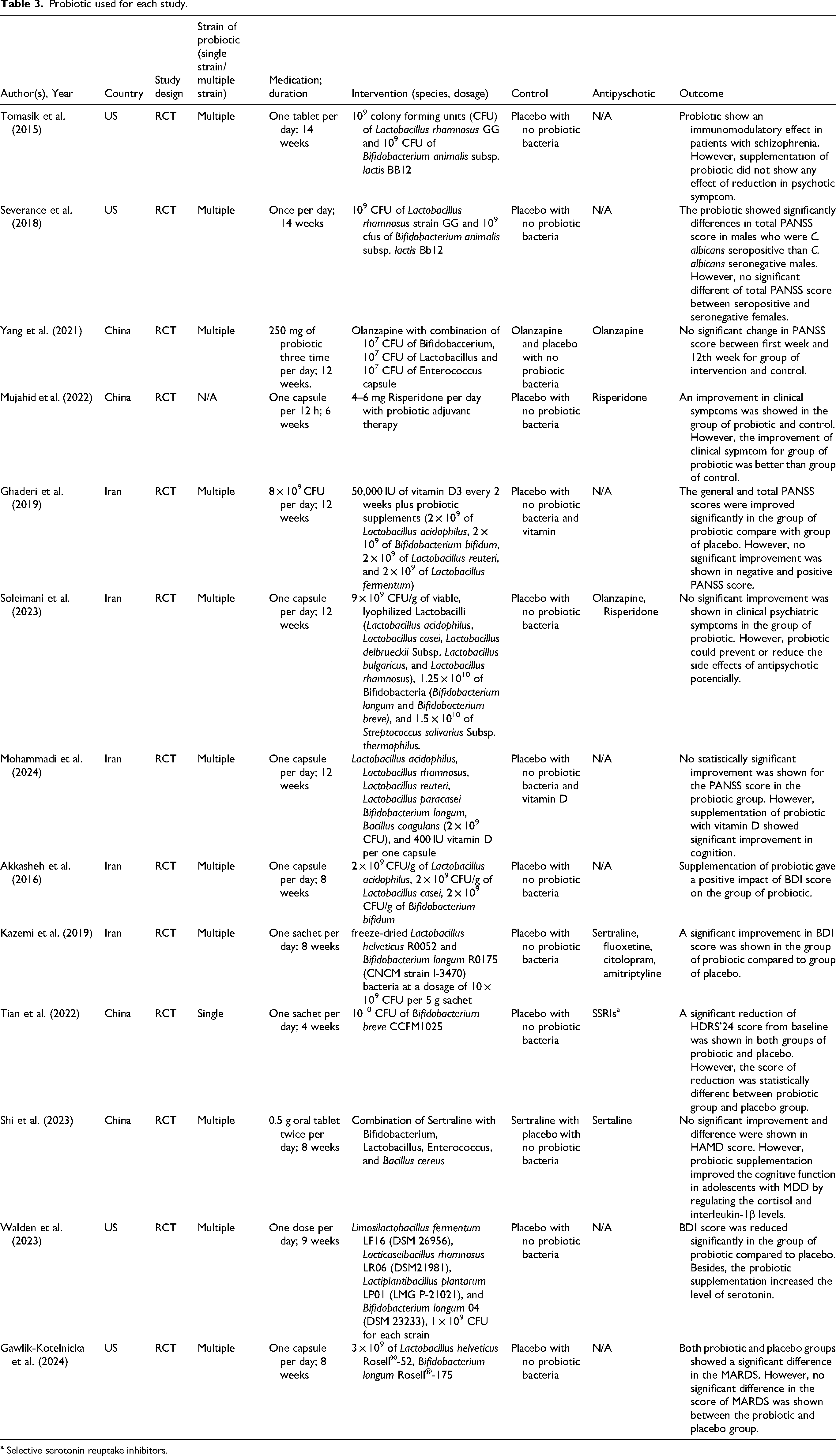
a Selective serotonin reuptake inhibitors.
Heterogeneity
In this study, high heterogeneity (I2 > 97%) restricts the confidence in pooled estimates. Sensitivity analyses showed that, while most exclusions did not substantially alter the pooled results, the overall dataset became significant upon the removal of one study. In the depression subgroup, exclusion of three studies also yielded significant results, whereas findings in the schizophrenia subgroup remained unchanged (Supplementary Tables 2–4).
The probiotic treatment did not show any statistically significant impact on clinical negative symptoms compared with placebos (P = .425) (Figure 2). As expected, we found high heterogeneity as I2 = 98.34%: Q = 2118.02; df(Q) = 12; P < .001, which may be due to the fact that the studies included various probiotic supplementations. Besides, no publication bias was shown (P = .36) with Egger's test, and no studies were missing.
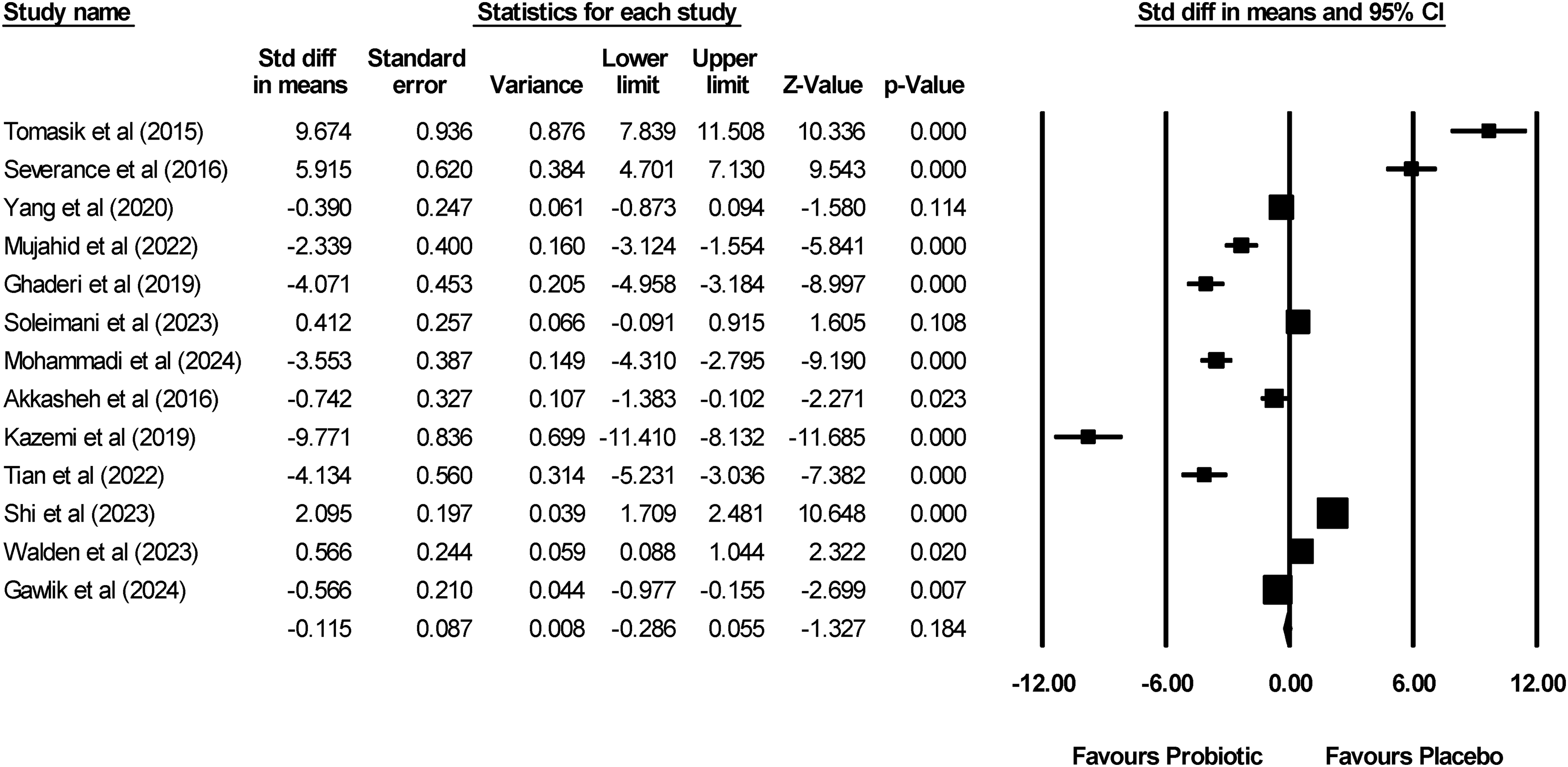
Meta-analysis of the impact of probiotics on clinical symptoms of schizophrenia and depression.
Schizophrenia
A total of seven studies, consisting of 414 schizophrenia subjects (210 patients and 204 placebo), were selected after the literature research. These studies did not show significant improvement in the treatment group (P = .546) (Figure 3(a)). However, high heterogeneity was found in this subgroup analysis, I2 = 98.46%: Q = 390.86; df(Q) = 6; P < .001. No publication bias was shown (Egger's test: P = .45), and no studies appeared to be missing.
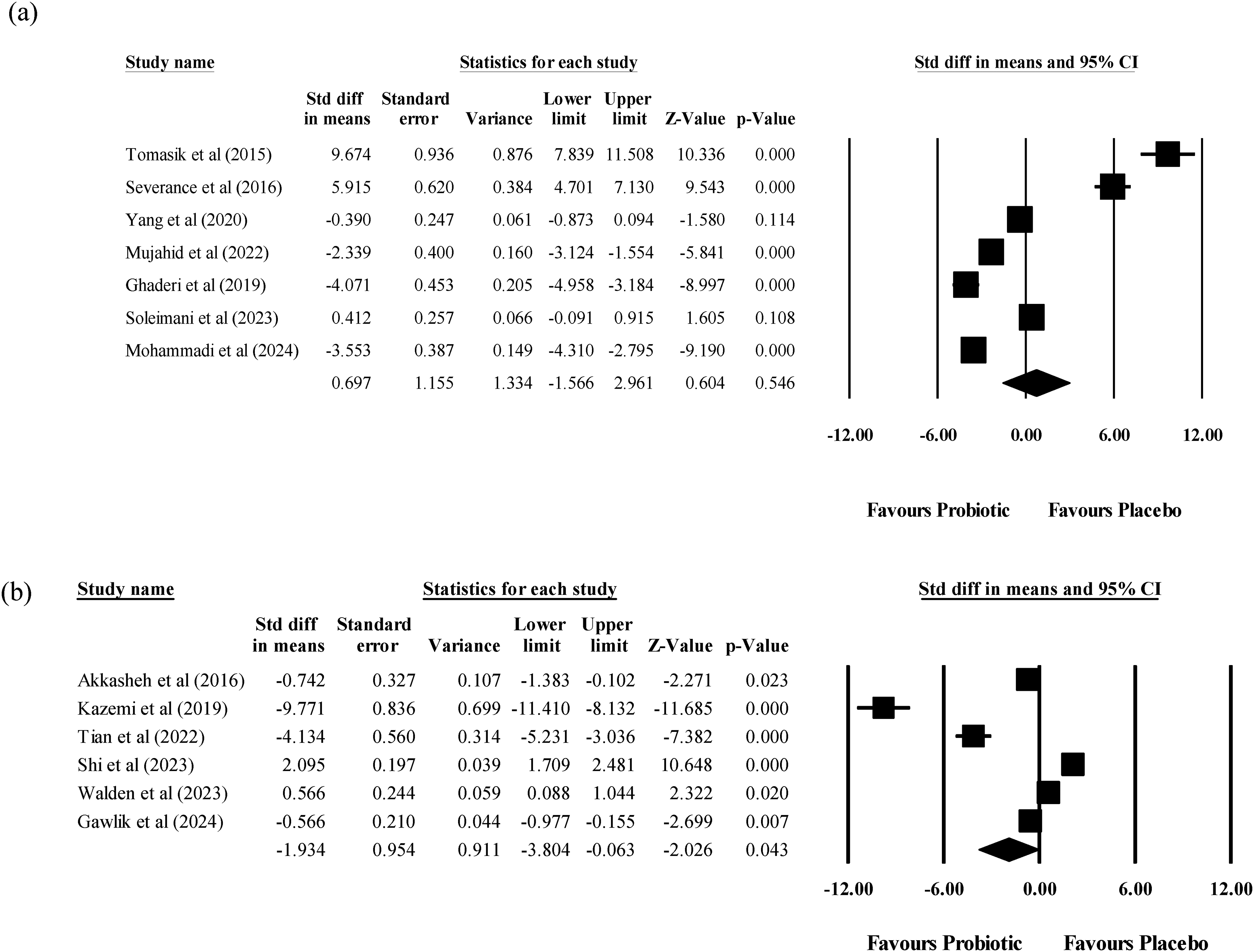
(a) Meta-analysis of the impact of probiotics on clinical symptoms of schizophrenia; (b) meta-analysis of the impact of probiotics on clinical symptoms of depression.
A subgroup analysis was conducted based on participants’ ethnic backgrounds. The clinical negative symptoms were significantly improved for patients with schizophrenia in the United States (American) (P < .001). However, no significant change for patients with schizophrenia in Asia (Asian) (P = .169) and Iran (Iranian) (P = .129). Co-administration of probiotics and Vitamin D showed a significant improvement in patients with schizophrenia (P < .001).
Depression
After screening studies, six studies with a total of 479 subjects (244 patients and 235 placebos) were included. The pooled standardized mean difference between intervention and control groups was marginal (P = .043) based on a random-effects model (Figure 3(b)). However, the heterogeneity was high (I² = 97.05%; Q = 169.26; df = 5; P < .001). Funnel plot asymmetry and a significant Egger's regression test (P = .0238) suggested possible publication bias or small-study effects. However, comparison between placebo with probiotic-treated depressive patients did not demonstrate any clinical symptom improvement in all the countries (United States; P = .990, Asia; P = .749, Iran; P = .247. Although the overall analysis revealed a statistically significant reduction of depressive symptoms (P = .043), one of the country-level sub-analyses did not reach statistical significance.
Discussion
There were no overall significant effects of probiotics against placebo on depressive and schizophrenic negative symptoms. Individual trials have, on occasion, shown improvement on the one hand, but these did not endure on pooling and overall were consistent with the prior reviews that have shown variable amelioration of psychiatric illness by probiotic intervention (Amirani et al., 2020; Ng et al., 2018; Nutt et al., 2008; Sequeira et al., 2022)
A major limitation of the evidence base is the high heterogeneity across trials, arising from differences in study design, probiotic strains, patient populations, and outcome measures. In schizophrenia studies, all used the PANSS (Kumar and Khess, 2012; Luo et al., 2023; Santor et al., 2007; Zagorska et al., 2020), yet reported mixed results, with some noting benefits for negative symptoms while others found no changes (Jacka et al., 2010; Ng et al., 2019; Romero-Ferreiro et al., 2025). In depression, outcomes varied depending on the use of BDI, HAM-D, or MADRS (Carrozzino et al., 2020; Karbownik et al., 2022; National Center for Health Statistics, 2023; Paketci, 2021; Tsolakis, 2025), complicating interpretation.
The observed small overall effect should be viewed with caution, as the results were not uniform across subgroups. Such heterogeneity can be caused by the relatively small sample sizes in subgroups and attenuated statistical power in individual subgroup analyses that may suppress modest effects. The pooled estimate would also not reflect constant effects uniformly between geographic locations, and hence caution should be used in generalizing these results.
Subgroup analyses suggested possible differences by region, diet, and vitamin D co-supplementation. However, these were based on very small numbers of studies (often only two per subgroup) and are therefore underpowered and hypothesis-generating only. For example, improvements observed in U.S. cohorts may reflect contextual factors such as proinflammatory dietary patterns (Astudillo-Lopez et al., 2021; Calder et al., 2020; Clemente-Saurez et al., 2023; Djuricic and Calder, 2021; Latif et al., 2023; Oddy et al., 2018; Statovci et al., 2017; Zheng et al., 2023) or higher prevalence of vitamin D deficiency in certain groups (Clemens et al., 1982; Looker et al., 2011; Parva et al., 2018; Webb and Engelsen, 2008). Similarly, studies testing probiotics in combination with vitamin D showed encouraging effects (Akkasheh et al., 2016; Mazziota et al., 2023; Sepehrmanesh et al., 2016), consistent with plausible biological mechanisms (Ghaseminejad-Raeini et al., 2023; Hamza et al., 2023; Ostadmohammadi et al., 2019; Pagnini et al., 2021), but these findings require replication before firm conclusions can be drawn.
Although mechanistic studies support the promise of probiotics to act on the gut–brain axis, immune signalling, and transmitters (Ansari et al., 2023; Gao et al., 2023; Jang et al., 2024; Kris-Ethertin et al., 2021; Meher et al., 2024; Sabit et al., 2023; Shoubridge et al., 2022; Vasquez et al., 2019; Virik et al., 2021; Wang et al., 2021), the evidence is indirect. Again, geographic differences in the intake of fermented foods can be responsible, at least partially, for the minimal difference between probiotic and placebo that has been recorded by Asian and Middle Eastern populations (Gaebler et al., 2022; Liu et al., 2011; Massomian et al., 2025; Meybodi et al., 2020; Soemarie et al., 2021; Yazadi et al., 2017), and again, these expository considerations surpass the scope of the analysis and must be treated with caution.
As a group, available data demonstrate that psychiatric symptoms do not reproducibly lower by administration of probiotics alone, and subgroup effects must not be overinterpreted. High heterogeneity and lack of generalizability call for appropriately powered, appropriately controlled studies with standardized preparations of probiotics and long follow-up. The marked differences in probiotic strains and intervention durations across studies (summarized in Supplementary Table 1) represent a major source of clinical heterogeneity. This diversity complicates the interpretation of pooled results and limits their applicability to specific clinical settings. However, there is still unexplained heterogeneity, and further meta-regression could reveal the causes. Future research should venture away from the “one-size-fits-all” hypothesis to discern which populations of patients will benefit the most so that more appropriate and justifiable interventions can be made.
Limitation
This study has several limitations. First, some relevant trials were excluded due to insufficient data, and the included randomized controlled trials had small sample sizes and methodological heterogeneity, potentially affecting the overall outcome. Second, due to the situation with only very few studies, our analysis did not account for the effects of specific antipsychotic medications, as participants received varied treatments. Additionally, the impact of co-supplementation with vitamin D and probiotics on mental health remains underexplored, limiting conclusions on their combined efficacy. Antipsychotics can also interact with supplements, foods, and drinks. High levels of vitamin D may counteract the benefits of antipsychotics. Most of the participants in this meta-analysis were prescribed numerous antipsychotics or antidepressants, and the possibility of interactions between these pharmacological interventions and probiotic supplementation could therefore not be evaluated. The use of concomitant medication might have been a confounder by precluding the identification of the isolated effects of the probiotics on the psychiatric symptoms.
Conclusion
In summary, the available evidence fails to show robust therapeutic efficacy of probiotic supplementation against depression or schizophrenia. While exploratory subgroup analyses point to tantalizing context-sensitive effects, these are drawn on the basis of small, poorly powered subsets and may result from either bias or chance. To conclusively establish if various preparations of the probiotic, patient profiles, or adjunctive methods can modify psychiatric endpoints, subsequent studies should emphasize mechanistic studies and adequately powered, well-matched trials. The majority of the available study patients were taking antipsychotic medication or antidepressants concurrently, and the contribution of these pharmacologic agents to the efficacy of the probiotic could not be severed, and it is a confounder that constrains the interpretability of the observed effects.
Supplemental Material
sj-docx-1-nah-10.1177_02601060251395942 - Supplemental material for Evaluating the efficacy of probiotics in schizophrenia and depression: A meta-analysis of clinical outcomes and subgroup effects
Supplemental material, sj-docx-1-nah-10.1177_02601060251395942 for Evaluating the efficacy of probiotics in schizophrenia and depression: A meta-analysis of clinical outcomes and subgroup effects by Xin Yi Tai, Shiau Foon Tee and Pek Yee Tang in Nutrition and Health
Footnotes
Acknowledgements
This work was supported by grants (IPSR/RMC/UTARRF/2023-C1/T07) from Universiti Tunku Abdul Rahman.
Ethical approval
Not applicable.
Consent of publication
Not applicable.
Author contributions
Tai X.Y.: conceptualization, methodology, validation, formal analysis, investigation, data curation, writing—original draft, visualization, resources; Tee S.F.: conceptualization, writing—review and editing, supervision, project administration, funding acquisition, resources; Tang P.Y.: conceptualization, writing—review and editing, supervision, resources.
Funding
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Universiti Tunku Abdul Rahman Research Fund (IPSR/RMC/UTARRF/2023-C1/T07).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and contribution
All data used in this meta-analysis were obtained from previously published studies (see References). The extracted dataset supporting the findings of this study is available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.