
Abstract
Background
Smart infusion pumps are widely adopted to improve medication safety, yet their effectiveness depends on nurses’ perceptions, usability, and integration into clinical workflows.
Study Aim
This study evaluated nurses’ perceptions of smart infusion pumps in Saudi Arabian hospitals, focusing on learnability, memorability, efficiency, error management, and medication administration performance.
Methods
A cross-sectional survey was conducted among 249 registered nurses across nine hospitals. Data were collected using a validated questionnaire and analyzed with descriptive statistics, t-tests, and ANOVA.
Results
Most nurses reported daily pump use (76.8%). Learnability and memorability scores were higher among younger nurses, diploma holders, and those in the Central Region (p < 0.05). Efficiency differed significantly by gender (p = 0.041), while error management varied by gender and region (p < 0.05). Medication administration performance showed no significant differences across demographics (p > 0.05).
Conclusion
Smart infusion pumps were positively perceived overall, though regional and demographic disparities highlight the need for standardized training and stronger system-level support.
Introduction
Medication administration errors present a persistent threat to patient safety, often resulting in adverse outcomes and increased healthcare costs globally (Afaya et al., 2021; Ali et al., 2024). In response, healthcare systems have adopted smart infusion pumps: these technologically advanced devices integrate programmable features, dose error-reduction systems (DERS), and extensive drug libraries to enhance safety, accuracy, and efficiency in medication administration. By replacing traditional infusion pumps with smart technology, healthcare institutions aim to reduce medication errors, streamline workflows, and support clinical decision-making (Borrelli et al., 2025a, 2025b). The integration of these pumps with electronic prescribing and barcode medication administration systems has demonstrated a substantial reduction in infusion-related medication errors (Alamer and Alanazi, 2023; Skog et al., 2022), in some cases by up to 73% (Jani et al., 2020). These errors occur across multiple routes of administration, not solely intravenous (IV). However, IV medications account for a disproportionately high proportion—approximately 48 to 53%—of all medication administration errors in hospitals, which elevates their clinical and safety significance. In response, healthcare systems have increasingly adopted smart infusion pumps, technologically advanced devices designed to improve dosing accuracy, increase safety, and reduce the risk of IV-related medication errors (MacDowell et al., 2024; Tsegaye et al., 2020).
While the technical promise of these devices is well-documented, their true impact hinges on the perceptions, competence, and workflows of the nurses who operate them in real-world hospital settings. Nurses are pivotal in the safe administration of medications and represent the first line of defense against preventable harm (Giuliano et al., 2022; Herrero et al., 2025; Klarich et al., 2022). Studies (Kuitunen et al., 2022; Schnock et al., 2023) have shown the presence of medication errors, despite using smart infusion pumps, and the reasons were mainly attributed to the nurses’ administration and knowledge. Their experiences and acceptance of smart infusion pumps determine whether the theoretical improvements in safety translate into practice. Key determinants of successful adoption and sustained impact include learnability (how smoothly nurses acquire proficiency with the device) (Algushairy et al., 2023; Obuseh et al., 2022), memorability (the extent to which nurses can reliably recall correct use after lapses) (Kalun and Chan, 2024), efficiency (streamlined, rapid operation within the bounds of routine clinical tasks) (Blake et al., 2025; Rothschild et al., 2005), error management (the ability to identify, intercept, and correct programming and administration errors) (Alamer and Alanazi, 2023; Borrelli et al., 2025a), and the overall effect on medication administration performance (El-sayed et al., 2019; Trbovich et al., 2010).
Despite wide implementation of smart infusion pump technology in hospitals across Saudi Arabia, there remains a knowledge gap regarding nurses’ lived experiences and perceptions relating to these crucial elements. Factors such as prior training, experience with similar devices, demographic influences, and organizational support all shape the acceptance and effectiveness of smart pumps (Algushairy et al., 2023; Ismail et al., 2023). Addressing these gaps through targeted evaluation is critical to ensuring not only the safe administration of medications but also optimal integration of technology into clinical practice.
Despite the global adoption of smart infusion pumps, the Saudi Arabian healthcare context presents unique challenges and characteristics—such as diverse multinational nursing staff, varied regional healthcare infrastructure, and particular workflow practices shaped by ongoing healthcare reforms and system modernization—which may influence nurses’ perceptions and the effective integration of smart pump technology. However, limited research has explored these factors within Saudi hospitals, underscoring the need for localized studies to inform tailored training, implementation, and policy strategies. Therefore, this study aims to provide an in-depth assessment of nurses’ perceptions of smart infusion pumps in Saudi Arabian hospitals, focusing specifically on the domains of learnability, memorability, efficiency, error management, and medication administration performance via a structured survey instrument. By identifying strengths and barriers, the findings will support the development of focused strategies for staff training, device configuration, and workflow optimization.
Research questions
What are the nurses’ perceptions of the impact of smart infusion pumps on medication administration performance in Saudi Arabian hospitals?
How do nurses’ perceptions of smart infusion pumps’ impact vary across different demographic profiles?
Background
Learnability
Learnability refers to how quickly and effectively nurses can master the use of smart infusion pumps. Studies have found that the learnability of these systems often improves over time, particularly through repeated exposure and practice (Carayon et al., 2010). Initial implementation phases may be hindered by insufficient training materials or poorly communicated guidelines, leading to frustration and slower uptake (Hoffman and Bacon, 2020). However, with ongoing targeted education and user feedback, nurses become significantly more comfortable and adept at using smart pumps within one year of introduction (Shah and Jani, 2020). Heuristic evaluations reveal that the learning curve for smart pumps can be steep, necessitating high-quality tutorials, clearly defined protocols, and support for new hires, especially given the diversity of device brands and functionalities across institutions (Skog et al., 2022). Nurses appreciate training programs that combine simulation, peer coaching, and referenceable online guides, resulting in better preparedness and increased confidence in device use.
Memorability
Memorability addresses the ease with which nurses can recall proper device use after periods of inactivity or transition between different models of smart pumps. Smart pump technology's reliance on preprogrammed dosage and drug libraries reduces the cognitive load on nurses, lessening the necessity to remember precise dosing rules and procedures for every medication (Blake et al., 2022). However, when device settings change or new functionalities are introduced, memorability can suffer if refresher training is lacking. Continuous education and periodic drills help nurses retain proficiency and reduce procedural lapses (Aziz, 2023). Memorability issues also arise when nurses are faced with infrequent but high-risk programming tasks, such as those for rare drugs or complicated regimens. Clear, accessible job aids and the integration of standardized organizational protocols within the device's interface can support best practices and minimize errors related to memory lapses (Khademi et al., 2015).
Efficiency
The efficiency of smart infusion pumps is measured by how quickly and accurately nurses perform medication administration tasks. Smart infusion pump interoperability with EHRs has been shown to increase operational efficiency by reducing manual programming steps and time spent on infusion setup. Biltoft & Finneman (Biltoft and Finneman, 2018) found that implementing full pump–EHR interoperability resulted in an 86% reduction in manual keystrokes, translating to approximately 3.5 million fewer keystrokes per month across their eight-hospital health system. The same study also reported a 19% reduction in the number of infusions requiring reprogramming after a DERS (Dose Error Reduction System) alert, highlighting both workflow and safety efficiencies gained through automation. Perceived efficiency increases as nurses become accustomed to the user interface and as device reliability and programming speed improve. Reduced manual calculations, automatic population of medication orders from pharmacy systems, and user-friendly interfaces further boost operational speed and minimize workflow disruptions. Despite these advantages, inefficiencies can arise due to overly complex software, poorly designed alarms, or cumbersome programming screens (Carayon et al., 2010; Zaborowski, 2018). Addressing these usability issues through iterative design and feedback ensures that nurses spend less time troubleshooting and more time on direct patient care.
Error management
Smart infusion pumps are designed to intercept programming and administration mistakes before they reach patients by using preset dosing limits, alerts, and drug-specific safety advisories. The presence of hard (non-overridable) limits on dosage, rate, or concentration can prevent serious medication errors, while soft limits provide warnings that nurses may override if clinical judgment dictates (Carrington-Hahn et al., 2025). Empirical data demonstrate that, with smart pumps, nurses remedy more “wrong dose hard limit” errors (75%–79%) compared to traditional pumps (38%), underscoring the effectiveness of automated safety features (Trbovich et al., 2010). However, these devices are not foolproof. Studies (Kirkendall et al., 2020) show that certain types of errors—such as wrong drug, wrong patient, or keypad entry mistakes—are not fully mitigated, and that low adherence to safety protocols (e.g., overriding dose-error reduction software, or failing to update drug libraries) allows avoidable errors to persist. Integration with barcode systems and EHRs improves error interception rates, especially with “wrong patient” errors, but ongoing efforts are needed to encourage full utilization and protocol compliance. Alert fatigue, workflow interruptions, and overreliance on the technology's safeguards contribute to new error types, suggesting that both device design and user training must continually evolve to support robust error management (Kirkendall et al., 2020).
Medication administration performance
Overall medication administration performance encompasses the cumulative effect of smart pump technology on dosing accuracy, patient safety, and workflow. Nurses widely report positive impacts, especially when devices are properly configured and integrated with the hospital drug library and electronic health systems. Studies in diverse clinical settings have shown reductions in severe adverse drug events and error rates after smart pump deployment, although proper use and adherence are critical to maximizing these benefits (Alamer and Alanazi, 2023; Blake, 2024; Giuliano and Blake, 2021; Hoffman and Bacon, 2020). Improvement in performance is most pronounced when organizations provide comprehensive training, encourage feedback, and maintain ongoing support for system updates and troubleshooting. Device standardization, continuous quality improvement initiatives, and the strategic deployment of nurse champions further promote safe and efficient medication administration (Alamer and Alanazi, 2023; Blake, 2024; Giuliano and Blake, 2021; Hoffman and Bacon, 2020; Marwitz et al., 2019).
In summary, while smart infusion pumps have significantly advanced medication safety and nurse performance, targeted attention to learnability, memorability, efficiency, error management, and ongoing practice support is essential to realizing the full promise of these technologies in clinical care.
Methods
Study settings
A descriptive correlational cross-sectional design is adopted in this study. The study was conducted in selected hospitals across Saudi Arabia where smart infusion pumps were routinely used in clinical practice. These hospitals included government, non-governmental, and private healthcare institutions, ensuring representation of diverse healthcare delivery contexts. Data were collected from different hospital units such as medical–surgical wards, intensive care units (ICUs), emergency departments, operating rooms, pediatric ICUs, and neonatal ICUs, thereby capturing the perceptions of nurses working in varied clinical environments.
Recruitment and sampling
Registered nurses directly involved in patient care and medication administration were eligible to participate. Inclusion criteria consisted of: (1) current employment as a registered nurse in one of the selected hospitals, (2) prior experience using smart infusion pumps, and (3) willingness to provide informed consent. Nurses who were not engaged in direct medication administration or who lacked experience with smart infusion pumps were excluded. A purposive sampling strategy (Etikan, 2016) was applied to recruit participants across different hospitals and regions of Saudi Arabia (Central, Eastern, Western, Northern, and Southern). This approach ensured a heterogeneous sample with respect to age, gender, nationality, education level, and years of nursing experience, allowing comparisons across demographic groups.
The sample size for this study was guided by previous research on impact of smart infusion pumps (Carayon et al., 2010; Mason et al., 2013; Montague et al., 2013). Given the exploratory nature of the research, a pragmatic approach was adopted by including all eligible nurses available during the data collection period across the selected hospitals. Using the minimum sample size formula for correlation studies at a 95% confidence level, a medium effect size (r = 0.3), and 80% power, the required sample was estimated at approximately 185 participants. The final sample achieved was 249 nurses, which exceeded this threshold and enhanced both the statistical power and the generalizability of the findings within the study context.
Questionnaire design
The structured questionnaire was developed based on validated instruments and previous studies on smart infusion pumps and medication administration (Afaya et al., 2021; Borrelli et al., 2025b; Carayon et al., 2010; Kuitunen et al., 2022; Marwitz et al., 2019; Schnock et al., 2023; Tsegaye et al., 2020). It consisted of two main sections. The first section captured demographic information such as age, gender, nationality, marital status, region, type of hospital, highest educational qualification, years of nursing experience, primary work setting, prior training on smart infusion pumps, and frequency of pump use. The second section focused on nurses’ perceptions of smart infusion pumps and was organized into five dimensions: learnability (five items), memorability (one item), efficiency (ten items), errors management (five items), and medication administration performance (ten items). Learnability assessed the ease of operating the device, navigating software, and identifying functions, while memorability examined the ability to recall commands and functions. Efficiency measured the perceived impact of smart infusion pumps on speed, safety, quality of care, and ease of use in emergencies, whereas errors management evaluated the handling of alarms, correction of mistakes, and prevention of medication errors. Finally, medication administration performance examined accuracy, workflow integration, confidence, access to resources, user-friendliness, and workload impact. All items were rated on a 5-point Likert scale, ranging from strongly disagree/difficult (1) to strongly agree/easy (5). A pilot study was conducted with 30 nurses to assess the clarity, reliability, and validity of the questionnaire items. The results of the reliability analysis indicated that all major constructs achieved a Cronbach's alpha greater than 0.70 (Taber, 2017), demonstrating acceptable internal consistency for use in the main study.
Data collection
Data collection was carried out between 1st July 2025 and 2nd August 2025, following ethical approval from the Institutional Review Board (IRB Approval No. IRB-2025-04-0420) at Imam Abdulrahman Bin Faisal University. The survey was administered using a secure online platform (Google Forms) and distributed through official hospital communication channels, including institutional email lists, internal messaging systems, and nursing supervisors. Institutions, representing both governmental, non-governmental and private hospitals across different regions of Saudi Arabia, participated in disseminating the survey link to registered nurses involved in medication administration. Each invitation included an information sheet outlining the study objectives, voluntary nature of participation, and assurances of confidentiality. Nurses were able to complete the questionnaire at their convenience using workplace computers or personal devices, which minimized disruption to clinical duties and encouraged honest responses.
Data analysis
Survey responses were coded and entered into SPSS software for analysis. Descriptive statistics (frequencies, percentages, means, and standard deviations) summarized demographic variables and perception scores. Reliability testing (Cronbach's alpha) was conducted for each construct to ensure internal consistency. Inferential statistics, including independent t-tests and one-way ANOVA, were applied to assess differences in perceptions across demographic variables such as age, gender, region, hospital type, and years of experience. Statistical significance was set at p < 0.05.
Ethical considerations
The study adhered to the ethical principles of the Declaration of Helsinki. Ethical approval was obtained from the institutional review board (IRB) of the sponsoring academic institution. Informed consent was obtained from all participants prior to data collection, and participation was voluntary with the right to withdraw at any time without penalty. Anonymity and confidentiality were ensured by using coded data and excluding any identifying information. Collected data were stored securely and used solely for research purposes.
Results
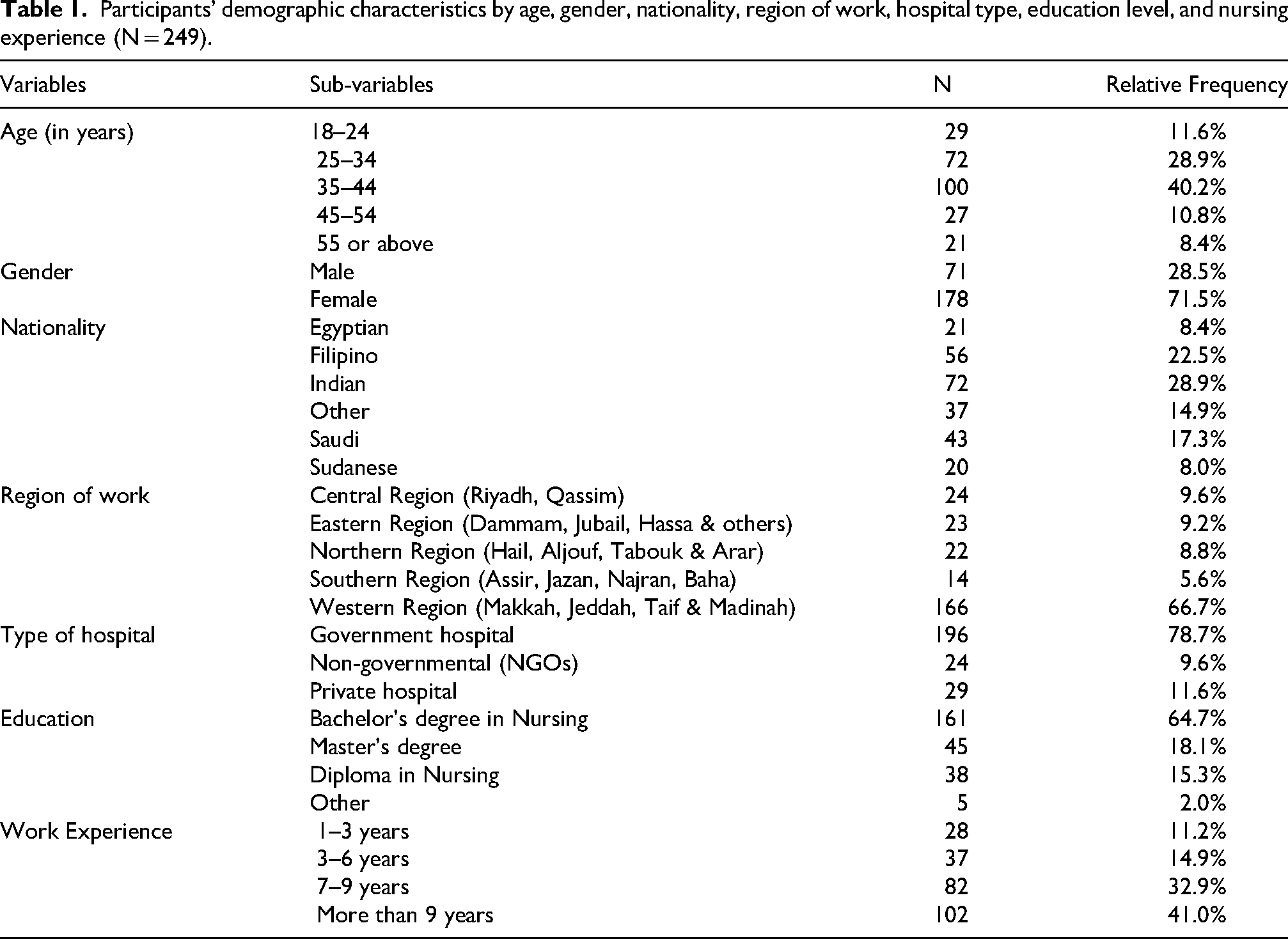
The study included 249 registered nurses from diverse backgrounds (see Table 1), primarily female (71.5%) and mainly employed in government hospitals (78.7%). Most nurses had substantial experience, with 41% reporting over nine years of practice, and the majority were from the Western Region (66.7%).
Participants’ demographic characteristics by age, gender, nationality, region of work, hospital type, education level, and nursing experience (N = 249).
The ANOVA results (see Table 2) revealed statistically significant differences in perceived learnability of smart infusion pumps based on age (p = 0.014), gender (p = 0.031), region (p = 0.002), education (p = 0.001), and work experience (p = 0.009), but not for nationality or hospital type. Younger nurses (18–24 years), males, and those from the Central Region or holding diploma qualifications reported higher learnability scores, while nurses with over nine years of experience scored lowest.
The differences in the perceptions of learnability of smart infusion pumps among the participants using ANOVA.
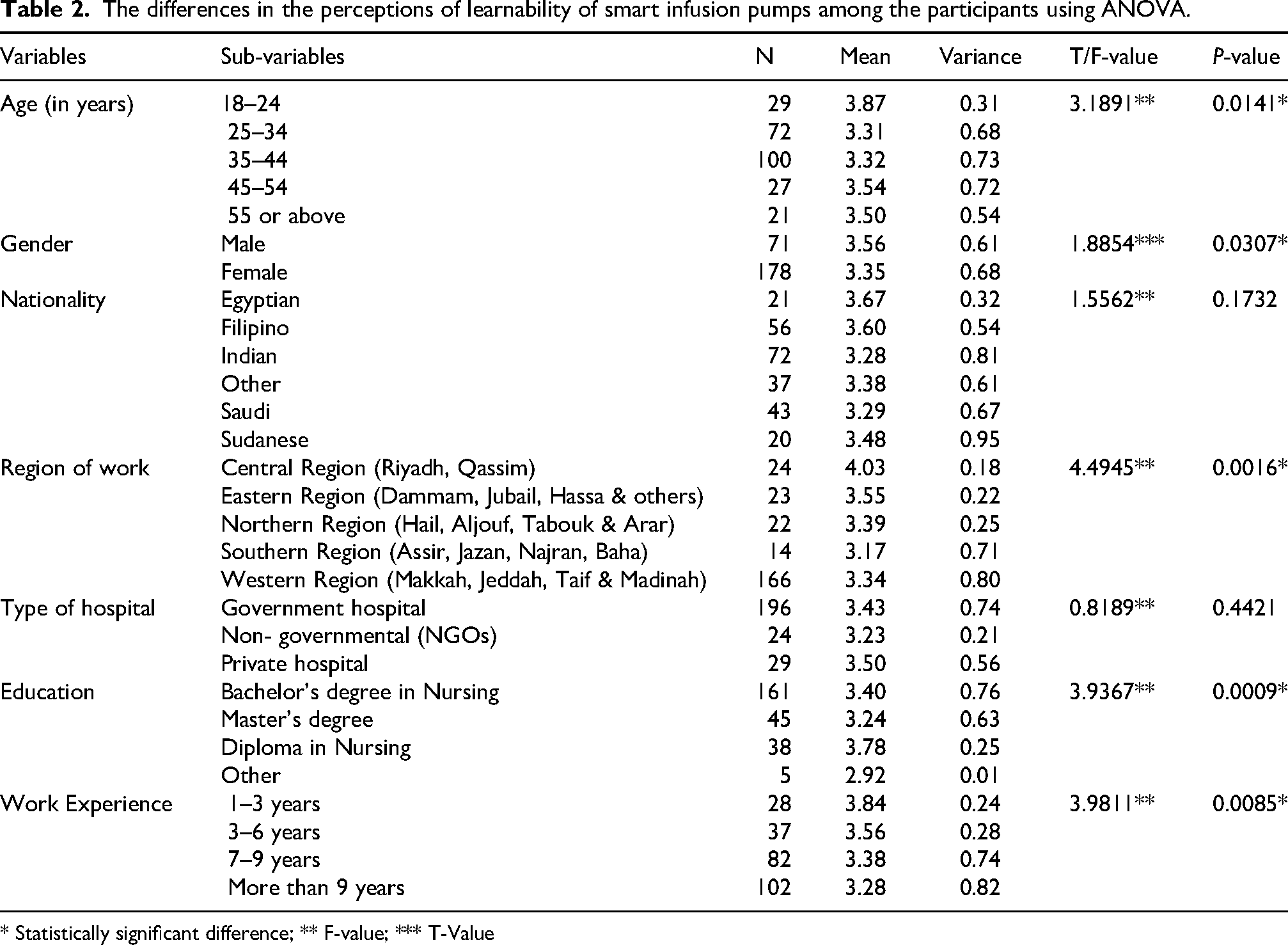
* Statistically significant difference; ** F-value; *** T-Value
The ANOVA results (see Table 3) reflected significant differences in memorability perceptions by region (p = 0.006) and education level (p = 0.014), with no significant variation across other demographics. Nurses in the Central and Northern Regions reported higher memorability scores compared with those in the Southern Region, while diploma holders rated their recall ability higher than bachelor's and master's graduates. Although not statistically significant, male and mid-career nurses (3–6 years) tended to report slightly higher memorability.
The differences in the perceptions of memorability of smart infusion pumps among the participants using ANOVA.
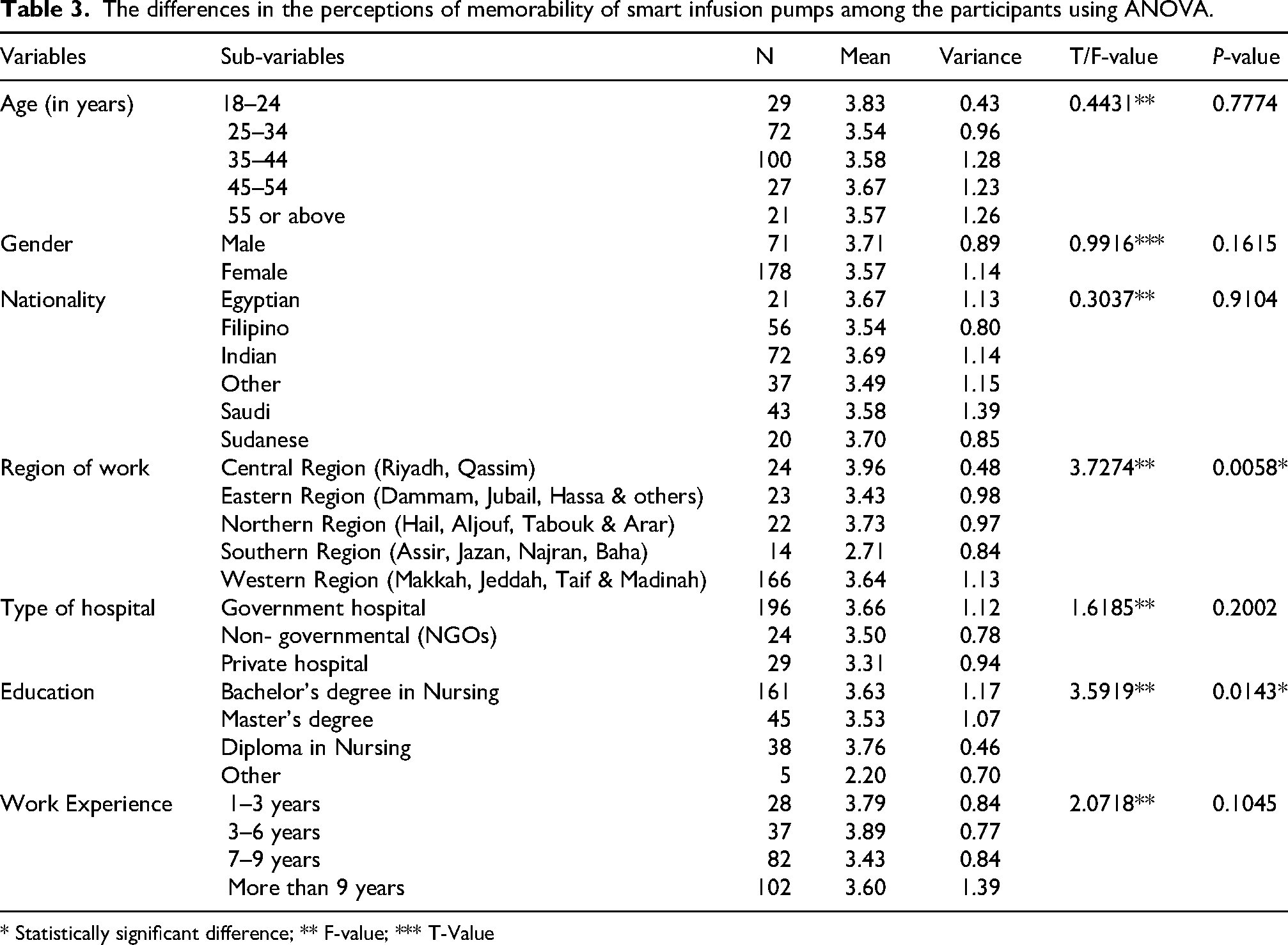
* Statistically significant difference; ** F-value; *** T-Value
The ANOVA results for efficiency (see Table 4) show a statistically significant difference in perceived efficiency by gender (p = 0.001), with males rating smart infusion pump efficiency higher than females. No other demographic variables showed significant differences, although nurses in the Central Region and diploma holders tended to report higher efficiency scores. Nurses with 3–6 years of experience also rated efficiency slightly higher than other experience groups.
The differences in the perceptions of efficiency of smart infusion pumps among the participants using ANOVA.
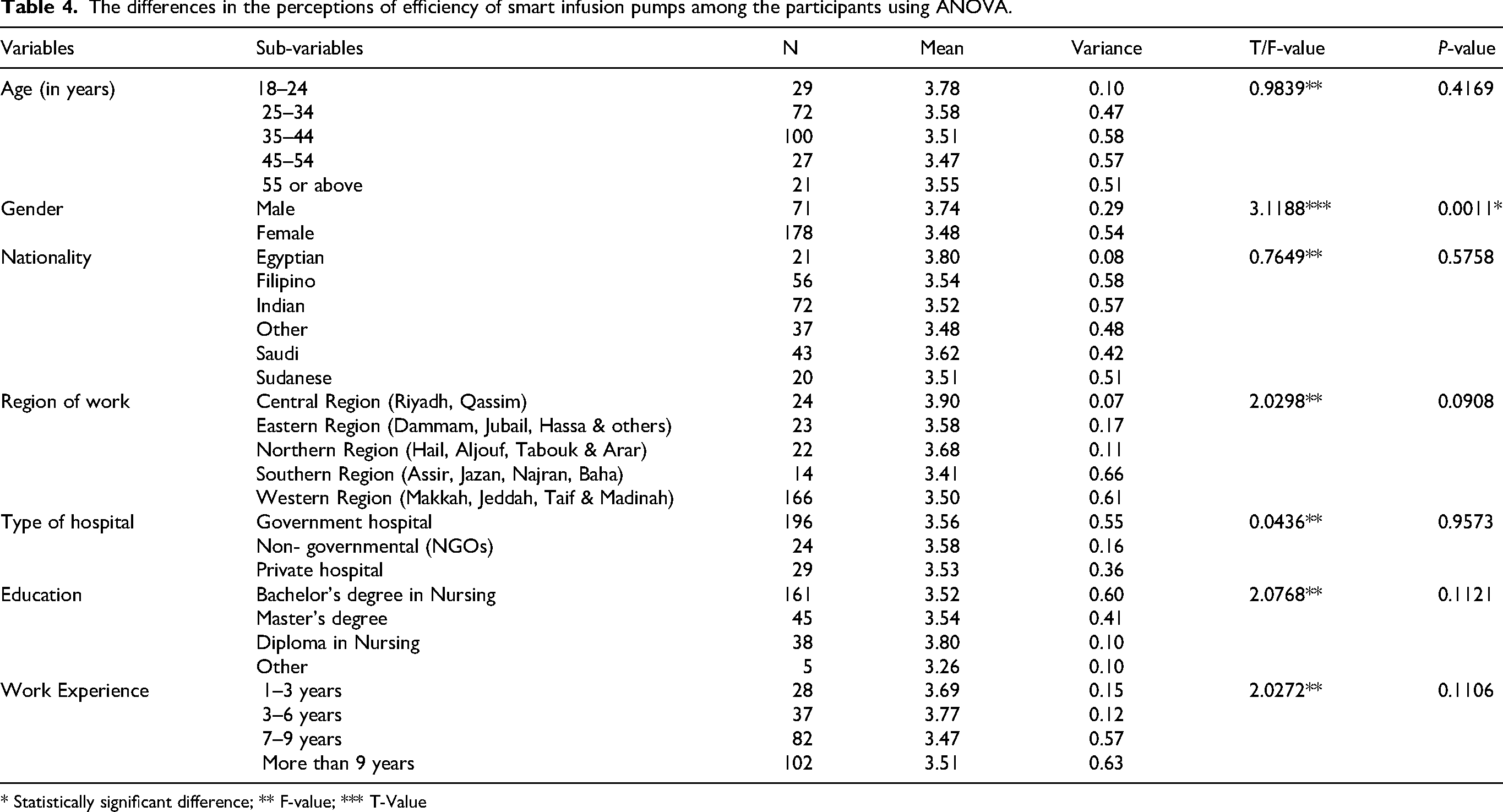
* Statistically significant difference; ** F-value; *** T-Value
The ANOVA results (see Table 5) for error management reflected significant differences in error management perceptions by gender (p = 0.012) and region (p = 0.010), with males and nurses in the Central Region reporting higher scores. No significant differences were found for age, nationality, hospital type, education, or experience, although diploma holders and nurses with fewer years of experience tended to rate error management higher.
The differences in the perceptions errors management of smart infusion pumps among the participants using ANOVA.
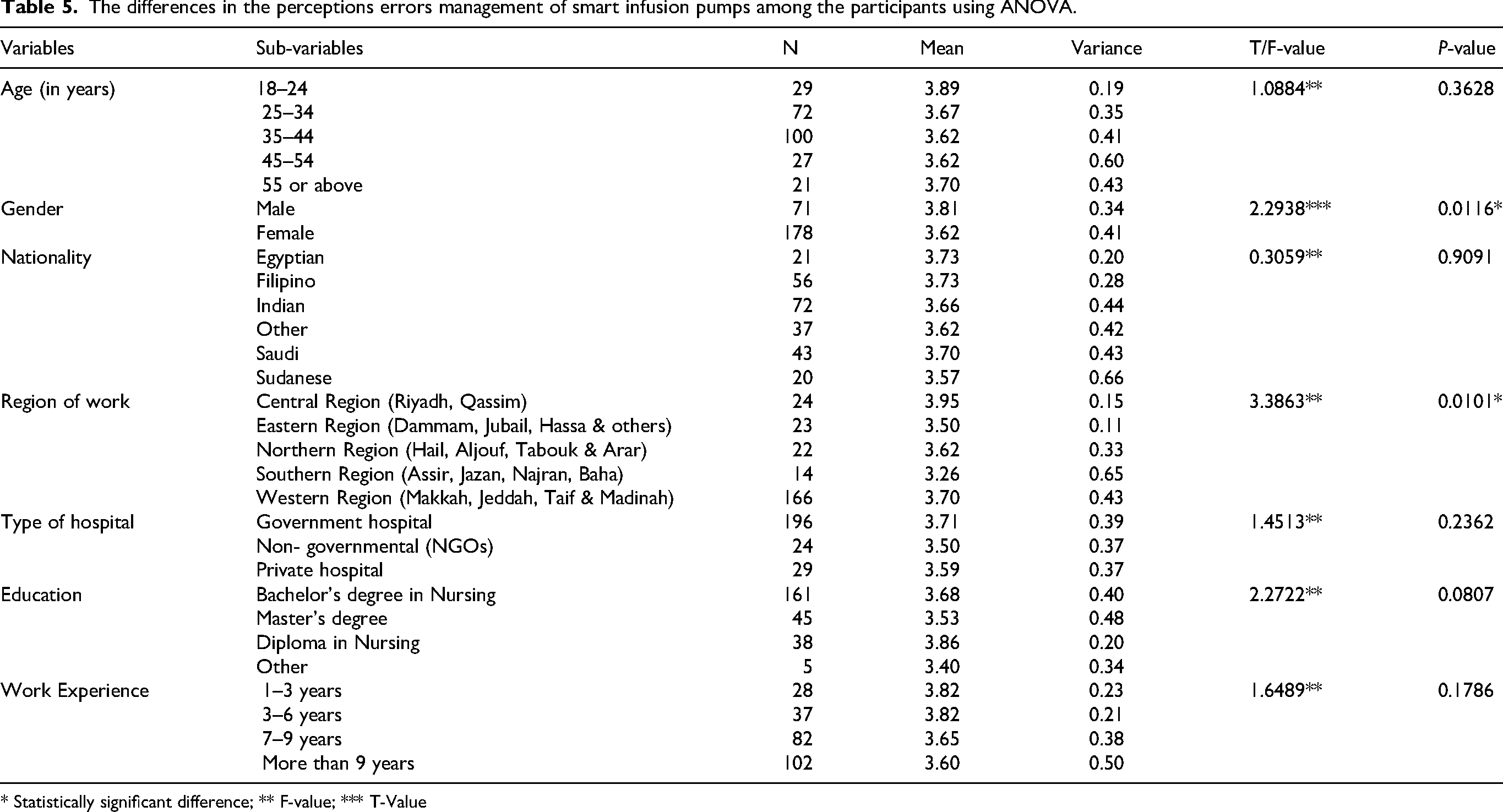
* Statistically significant difference; ** F-value; *** T-Value
The ANOVA results (see Table 6) for medication administration performance show no statistically significant differences across any of the examined variables, including age, gender, nationality, region of work, type of hospital, education level, and work experience. Despite the lack of statistical significance, some trends are observable. These trends suggested somewhat higher scores among nurses in the Central Region, those in the “Other” nationality category, bachelor's degree holders, and nurses with over nine years of experience.
The differences in the perceptions of medication administration performance of smart infusion pumps among the participants using ANOVA.
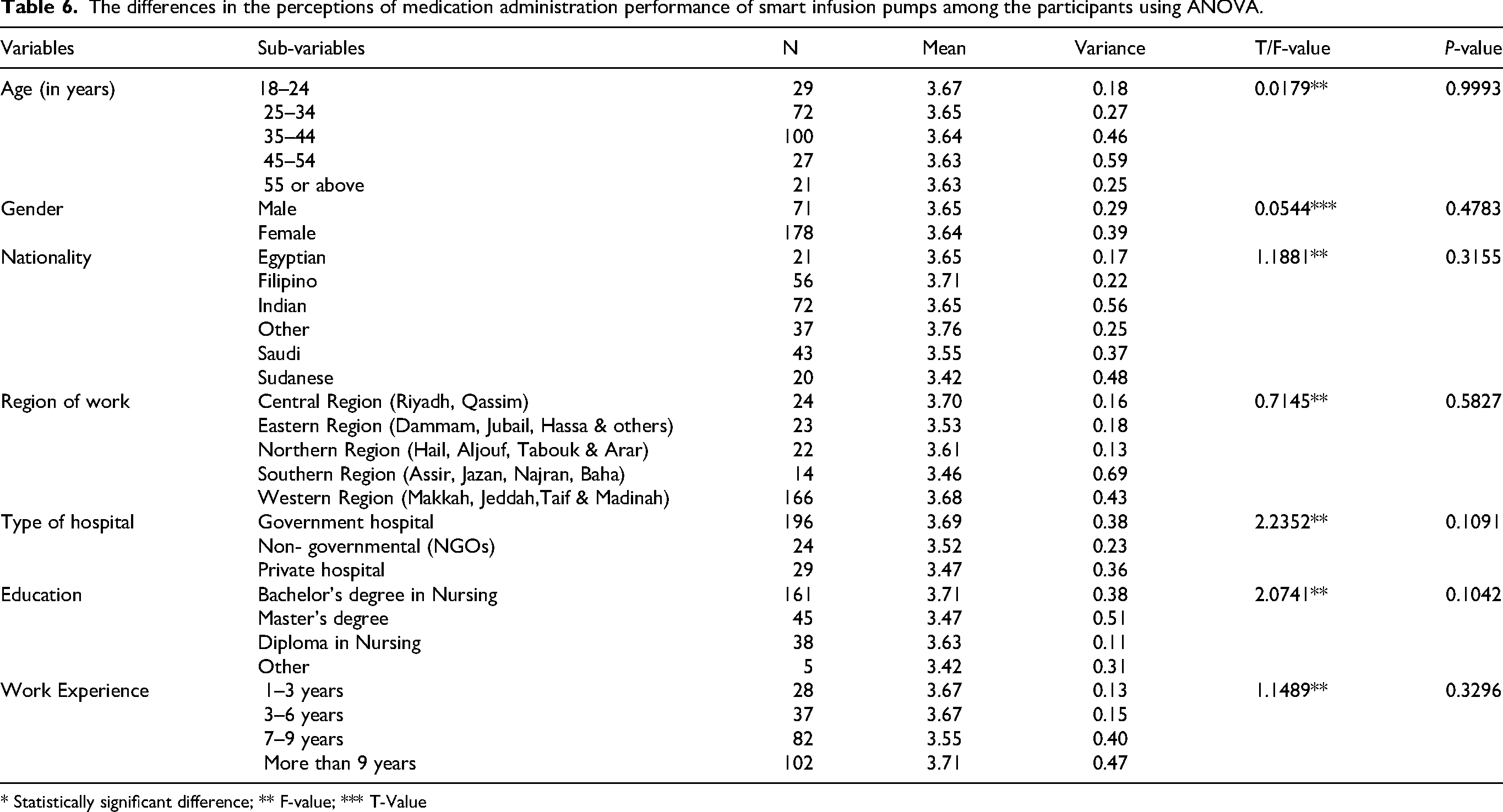
* Statistically significant difference; ** F-value; *** T-Value
Discussion
This study found generally favorable nurse perceptions of smart infusion pumps across learnability, memorability, efficiency, error management, and medication administration performance, with most nurses reporting daily use—an indicator of high exposure that likely shapes attitudes and proficiency. Despite overall positive perceptions meaningful subgroup differences emerged. These patterns underscore that technology benefits are not uniformly experienced; they depend on user characteristics and organizational context.
Learnability varied significantly by age, gender, region, education, and experience. Younger nurses (18–24 years) and those with 1–3 years’ experience rated learnability highest, suggesting that recent training and fewer entrenched habits may ease adoption. Diploma holders also reported higher learnability than bachelor's and master's degree holders, which may reflect more hands-on device exposure in certain training pathways. These results align with prior work showing steep initial learning curves mitigated by targeted education, simulation, and iterative guidance (Carayon et al., 2010; Hoffman and Bacon, 2020; Shah and Jani, 2020; Skog et al., 2022). They also fit with evidence that clear protocols and sustained support improve proficiency over time, converting early implementation friction into routine competence (Hoffman and Bacon, 2020; Shah and Jani, 2020). Regionally, Central Region nurses scored higher than Southern Region nurses, highlighting site-level differences in onboarding and support that echo reported variability in training quality and device configuration across institutions (Skog et al., 2022).
Memorability differed by region and education, again favoring the Central Region and diploma-prepared nurses. Literature indicates that while drug libraries can reduce cognitive load, proficiency decays with infrequent or shifting workflows without refreshers and accessible job aids (Aziz, 2023; Blake et al., 2022; Khademi et al., 2015). Given that nearly one in five nurses used pumps less than weekly or monthly, structured refreshers and embedded “how-to” cues (e.g., on-device prompts, quick-reference guides) are warranted to buffer memory lapses, particularly in units with variable exposure or multiple device models.
Efficiency only differed by gender, with men reporting higher efficiency, whereas age, region, hospital type, education, and experience were nonsignificant. Although this could reflect real differences in role assignments (e.g., device super-users) or confidence, social desirability and occupational segmentation cannot be ruled out. Prior studies attribute efficiency gains primarily to interoperability—reduced keystrokes and automated order transfer—rather than demographics per se (Biltoft and Finneman, 2018; Carayon et al., 2010; Zaborowski, 2018). The absence of broad subgroup effects here may indicate partial standardization of workflows or similar device generations across sites, but it may also signal unrealized efficiency potential where EHR integration is incomplete.
Error management showed significant differences by gender and region, with higher ratings among men and the Central Region. This heterogeneity mirrors literature noting that dose error-reduction systems (DERS) and hard/soft limits curb many programming errors, yet benefits hinge on adherence to updated libraries and avoidance of unnecessary overrides (Carrington-Hahn et al., 2025; Kirkendall et al., 2020; Trbovich et al., 2010). Sites with stronger informatics governance and pharmacy–nursing collaboration typically see better interception of “wrong dose hard limit” errors and fewer workarounds (Kirkendall et al., 2020; Trbovich et al., 2010). Given the Southern Region's lower scores across several domains, targeted interventions—library maintenance discipline, override audits, and local champions—are justified to mitigate alert fatigue and normalize safe responses to alarms.
Medication administration performance did not differ significantly across demographics, despite visible trends (e.g., slightly higher means in the Central Region and among the most experienced nurses). This finding is consistent with the view that system-level factors—library quality, integration with barcode/EHR, and organizational safety culture—dominate individual attributes in shaping downstream safety outcomes (Alamer and Alanazi, 2023; Blake, 2024; Giuliano and Blake, 2021; Hoffman and Bacon, 2020). Studies report substantial error reductions (sometimes approaching 73%) when smart pumps are fully integrated and used as intended (Alamer and Alanazi, 2023; Blake, 2024; Giuliano and Blake, 2021; Hoffman and Bacon, 2020; Jani et al., 2020; Tsegaye et al., 2020). The lack of subgroup effects here may indicate a floor of standardized safeguards that equalize performance, even where perceptions of usability vary. It also suggests that raising performance further will depend less on who the nurse is and more on how the system is designed, integrated, and governed.
Focusing on the implications and recommendations, first, address regional disparities through standardized onboarding, recurrent micro-learning to bolster memorability, and robust informatics stewardship of drug libraries. Second, deepen interoperability to convert perceived efficiency into measurable time savings and error interception (Biltoft and Finneman, 2018; Carayon et al., 2010; Zaborowski, 2018). Third, operationalize error-management best practices—override governance, alarm optimization, and nurse-pharmacist co-ownership of DERS—to counter alert fatigue and sustain safe behaviors (Carrington-Hahn et al., 2025; Kirkendall et al., 2020; Trbovich et al., 2010). Finally, nurse leadership and hospital administration play a critical role in addressing challenges such as pump maintenance, drug library updates, and ongoing training. Effective leadership involvement ensures dedicated resources for regular drug library management, enforces adherence to safety protocols, and promotes continuous education programs. Engaged nurse leaders serve as advocates for front-line staff, facilitating communication, coordinating multidisciplinary collaboration, and fostering a culture of safety that supports the sustained, effective use of smart infusion pumps.
Strengths include a large, experienced sample with high daily device exposure; limitations include cross-sectional, self-reported data, overrepresentation of the Western Region and government hospitals, and unmeasured confounders such as pump brand and integration level. Future work should triangulate perceptions with objective telemetry (alert/override logs, compliance with drug libraries) and patient-level safety outcomes to close the perception–performance loop.
Conclusion
This study found that nurses in Saudi Arabian hospitals generally viewed smart infusion pumps positively, particularly in enhancing safety and efficiency in medication administration. Significant differences in perceptions across demographics and regions highlighted the influence of training, experience, and institutional support on usability. Notably, medication administration performance remained consistent across groups, suggesting that system-level factors such as interoperability, drug library management, and organizational safety culture play a more decisive role than individual characteristics. To maximize benefits, hospitals should focus on standardizing training, maintaining robust drug libraries, and strengthening governance to ensure equitable and safe pump utilization.
Footnotes
Acknowledgements
Not applicable.
Ethical considerations
Ethical approval was received from the Institute Review Board of Imam Abdulrahman Bin Faisal University “IRB-2025-04-0420” obtained 19/06/2025.
Consent to participate
Participant informed consent to participate was written. Attached with the questionnaire
Consent for publication
Not applicable
Authors’ contributions
The researcher did all the parts of the research (Abstract, introduction, literature review, data collection, data analysis, results discussion, writing up)
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data is available upon request.