
Abstract
The global prevalence of oxidative stress-related disorders is increasing; hence, understanding the dietary sources that are involved in maintaining high antioxidant levels gains great importance. This study aims to explore the relationship between adherence to the healthy eating index (HEI) and the alternative healthy eating index (AHEI) with an antioxidant profile of young women. Diet quality was assessed using a Food Frequency Questionnaire to calculate HEI and AHEI scores. The serum total oxidant/antioxidant status was evaluated by measuring ferric reducing antioxidant power (FRAP), 2,2′-diphenyl-1-picrylhydrazyl radical scavenging activity, thiobarbituric acid reactive substances, pro-oxidant–antioxidant balance, and nitric oxide (NO) levels. This cross-sectional study was conducted among 155 women aged 18–24 years. While no significant associations were found between any parameters and adherence to AHEI recommendations, serum FRAP levels were significantly correlated with HEI scores (r = 0.297, P < 0.001). Higher serum FRAP was associated with greater reported consumption of fruit, dark green vegetables, total vegetables, and empty calories, as well as a lower intake score for polyunsaturated fatty acids (P < 0.05). Linear regression analysis confirmed a direct association between HEI scores and serum FRAP levels (β=3.03, P = 0.001). Overall compliance with a HEI diet was related to higher levels of antioxidant index in healthy young women.
Introduction
The complex association between dietary patterns and health outcomes has attracted considerable attention in recent years, especially in relation to chronic diseases influenced by oxidative stress (OS) (Aleksandrova et al., 2021). Studies of nutritional epidemiology have moved from single-nutrient analysis to dietary pattern analysis to provide a better understanding of the effect of diet on OS (Schulz et al., 2021). Among the different dietary assessment tools, the healthy eating index (HEI) and the alternative healthy eating index (AHEI) have emerged as instrumental criteria for assessing the quality of dietary habits (Hao and Li, 2024; Mohandas and Prema, 2020).
The HEI is a comprehensive tool developed to evaluate the quality of diets based on the United States Department of Agriculture dietary guidelines. It encompasses a wide spectrum of food components that aims to quantify adherence to these guidelines through a scoring system that reflects the consumption of fruits, vegetables, grains, protein sources, dairy, and other resources of calories (Guenther et al., 2014). A higher HEI score indicates a greater commitment with nutritional recommendations, which is associated to lower risks of different chronic diseases such as cardiovascular diseases, diabetes, and human malignancies. A systematic review assessing 13 original articles showed that diet is a crucial factor in the modulation of OS during pregnancy (El Sherbiny et al., 2023).
The AHEI was designed to better emphasize foods and nutrients linked with lower chronic disease risk, in contrast to the HEI, which has a more general approach. The AHEI focuses on specific dietary components suggested to be protective against chronic diseases. AHEI emphasizes the role of whole grains, fruits, vegetables, nuts, legumes, and healthy fats, whereas restricting red and processed meats, sugar-sweetened beverages, and trans-fats (Chiuve et al., 2012).
OS is a biological phenomenon related to an imbalance between the generation of free radicals and the body's ability to neutralize their harmful effects via antioxidant mechanisms (Forman and Zhang, 2021). Antioxidants play a critical role in this defense, scavenging free radicals and mitigating cellular damage (Pisoschi et al., 2021). Given the global prevalence of OS-related conditions, understanding the dietary sources that implicate to circulating antioxidant levels, such as fruits and vegetables, gains superior importance.
It has been shown that diets rich in fruits, vegetables, nuts, and whole grains are abundant in various phytochemicals and vitamins—such as vitamin C, vitamin E, and carotenoids—known for their antioxidant properties (Liu, 2013). So, dietary patterns that are adherent to the principles outlined in the HEI and AHEI may contribute to enhanced antioxidant capacity. It has been suggested that the antioxidant capacity of serum, a measurement indicating the presence and activity of these protective components in the blood, is influenced remarkably by dietary intake (Wang et al., 2013). However, there are inconsistent results between different studies. For instance, adherence to the HEI diet was shown to be weakly associated with higher levels of FLOP_320 and FLOP_360 as fluorescent oxidation products which are biomarkers of OS (Jung et al., 2016). But, Peluso et al. reported that the non-significant relationships between HEI with total antioxidant capacity (TAC) and malondialdehyde (MDA) (Vahid et al., 2022).
The field of biomarker discovery has seen significant advancements in recent years, particularly concerning molecules that characterize oxidative in human research (Dennis et al., 2019). This progress is momentous, as OS is a fundamental process contributing to various chronic diseases. As researchers elucidate the intricate biological pathways connected with this phenomenon, the identification of novel biomarkers becomes necessary for early diagnosis, monitoring, and management of health conditions originating from OS responses.
There are sex differences in OS biomarkers (Brunelli et al., 2014). Recently, OS has been suggested to contribute to multiple female reproductive disorders (Manokaran et al., 2022). Therefore, we aimed to rigorously assess the association between dietary patterns and panel of biomarkers characterizing OS in apparent healthy young women.
Materials and methods
Design and participants
This cross-sectional study was performed in Birjand city, located in northwestern Iran, during January 2020. The sample size required for 80% power and α′ = 0.05 (z value of 1.96) was calculated by findings from a previous study (r = 0.25 for correlation between Dietary Approach to Stop Hypertension Diet score and theobromine) (Kim et al., 2021). Based on these assumptions, at least 140 participants were required. A total of 155 female university students were invited from five different universities. For recruiting a homogeneous population and rigorous controlling for potential confounding variables, inclusion criteria were limited to single, aged between 18 and 24 years, apparently healthy women. Individuals who had experienced any acute or chronic health complications or those currently undergoing pharmacological treatment were excluded. The study received ethical approval from the Ethical Committee of Birjand University of Medical Sciences. Additionally, informed written consent was obtained from all participants, ensuring that they were fully aware of the study's purpose and protocol.
Dietary assessment
A validated Food Frequency Questionnaire (FFQ) was used for estimating individual food consumption. Participants were asked to report their consumption frequency for different food items as daily, weekly, monthly, rarely, or never (Ahmadnezhad et al., 2017). After gathering dietary information, food analysis was conducted using Diet Plan 6 software (Forest Field Software Ltd, UK).
HEI and AHEI are helpful nutritional indicators that can be used for evaluating the diet quality within a population. The HEI 2010 comprises 12 components; 9 of which represent the diet sufficiency, including whole fruit, total fruit, dark green vegetables, total vegetables, whole grains, dairy products, total protein foods, seafood and plant proteins, and fatty acids. The remaining three components are refined grains, sodium, and empty calories (calorie form solid fats, added sugars, and alcohol) that must be consumed moderately. Each component has a maximum score (5–20) and a minimum score (0). Higher intake of each component results in getting a higher score, while lower scores are due to low consumption of components. The standard for getting the maximum score is a definite serving intake of each component per 1000 kilocalorie of total daily energy intake. For instance, consuming ≥0.8 serving of whole fruit per 1000 kilocalorie of total daily energy intake results in getting 5, which is the highest score of this component. On the other hand, those with no whole fruit intake in a day will get zero for this component. Finally, the scores of all components will sum up, and the highest total score is 100 for HEI (Guenther et al., 2014).
The AHEI comprises 11 components, including vegetables, fruit, whole grains, sugar-sweetened beverages, nuts and beans, red meat and processed meat, trans fatty acids, n-3 fatty acids, polyunsaturated fatty acids (PUFA), sodium, and alcohol. The maximum score for each component is 10, and the lowest is zero. Higher intake of each component results in getting a higher score, while lower scores are due to a low consumption of components. The standard for getting the maximum score is a definite serving intake of each component per day. For instance, consuming ≥5 servings of vegetables in 1 day results in getting 10, which is the highest score of this component. On the other hand, those with no vegetable intake in a day will get zero for this component. Finally, the scores of all components will sum up, and the highest total score is 110 for AHEI (Chiuve et al., 2012).
Blood sampling and laboratory measurements
Fasting 10 mL blood samples were collected into serum separator blood collection tubes and stored at −80 °C until analysis.
Oxidant–antioxidant status quantification
The ferric reducing antioxidant power (FRAP) assay is based on reduction reactions, where antioxidants in the sample reduce ferric ions (Fe³+) to ferrous ions (Fe²+), thereby leading to a measurable color change in the reaction medium. Ten microliters of each sample was added to 250 µL of freshly prepared FRAP solution. The incubation period of 10 min at 37 °C allows for adequate interaction between the sample and the FRAP solution, ensuring optimal reaction conditions for the reduction process. Subsequently, the absorbance of the resulting solution was measured at a wavelength of 593 nm, where the intensity of the color change correlates with the antioxidant capacity of the sample (Benzie and Strain, 1996; Choudhary et al., 2019; Zhong and Shahidi, 2015). All experiments were performed in duplicate, and the average values were calculated.
The α,α-diphenyl-β-picrylhydrazyl (DPPH) assay measures the free radical scavenging activity of serum antioxidants by quantifying the reduction of the stable DPPH radical, which results in a color change proportional to radical quenching capacity. This assay reflects the ability of circulating antioxidants to neutralize reactive species, complementing the FRAP assay, which measures total reducing power. The DPPH assay was originally developed by Brand-Williams et al., as described previously (Brand-Williams et al., 1995). The measurement was based on the decrement of DPPH solution radicals into a steady state, which is detectable through distinct color changes. The mixture was then allowed to incubate at room temperature for a period of 15 min. During incubation, the DPPH radicals undergo reduction, leading to a noticeable alteration in color that corresponds to the scavenging activity of the specimen. Following incubation, the mixture was subjected to centrifugation, and the absorbance of the remaining DPPH radicals was quantified at a wavelength of 517 nm, against a blank of ethanolic DPPH solution. The percentage (%) of DPPH scavenging was calculated using this formula [(absorbance of the control − absorbance of the specimen)/absorbance of the control] × 100.
The thiobarbituric acid reactive substances (TBARS) assay was used for assessing lipid peroxidation content (MDA metabolites). This assay relies on the reaction between thiobarbituric acid (TBA) and MDA, which results in the formation of a colored compound indicative of lipid peroxidation, detectable as a pink pigment at an absorbance wavelength of 532 nm (Aguilar Diaz De Leon and Borges, 2020). A sample volume of 100 μL was carefully combined with 1 mL of a TBA/HCl mixture. This combination was subsequently incubated in a hot water bath for 20 min, followed by immediate chilling to halt the process. The excitation and emission fluorescence peaks were precisely measured at 515 and 553 nm, respectively. These measurements were interpreted against a standard calibration curve, constructed using propane and 1,3,3, tetra methoxy.
Pro-oxidant–antioxidant balance (PAB) assay was developed by Alamdari et al. (2008), for simultaneous measurement of oxidant levels and antioxidant capacity. To make accurate comparisons between specimens, both standard and working solutions were prepared. The standard solutions were used to establish a calibration curve against which the antioxidative and oxidative capacities of the test samples can be quantified. The values obtained are reported as Hamidi Koliakos units.
The measurement of the oxidized metabolites (NOx) is a valid and reliable method for reporting nitric oxide (NO) concentration. We quantified the NOx concentration according to the Griess method, as described formerly (Farrokhfall et al., 2023). Briefly, precipitation of serum proteins was conducted through an equivalent volume of 90% ethylic alcohol. The Griess reagents consist of N-L(naphthyl) ethylenenndiamine dihydrochloride in H2O and sulfanialamide in HCl. An absorbance reading at 540 nm was performed by a spectrophotometer (Kalugalage et al., 2013). A standard curve was prepared by serial dilution of nitrite solution, and then NOx levels were calculated.
Biochemical and anthropometric variables
Body mass index (BMI) was calculated based on height and weight. Additionally, the waist-to-hip ratio was determined. Systolic and diastolic blood pressure were recorded in a resting state and reiterated during the same visit to ensure accuracy and reliability of the results. Serum levels of fasting blood glucose, urea, creatinine, alanine transaminase, aspartate transaminase, alkaline phosphatase, bilirubin levels (total and direct), lipid profile, total protein, albumin, and uric acid levels were quantified through Pars Azmun commercial kits (Karaj, Iran) and the Prestige 24i auto-analyzer (Japan).
Statistical analysis
Data was analyzed using R version 4.3.1 (R Development Core Team, New Zealand) and SPSS for Windows version 22.0. The data normality assumption was explored by the Kolmogorov–Smirnov analysis. The females were categorized according to the HEI/AHEI scores into tertiles; T1 was in the lowest tertiles (lowest commitment), T2 was in the second (moderate commitment), and T3 was in the highest (higher commitment). For comparison of quantitative variables between tertiles of these indices, analysis of variance and post hoc Tukey's test were recruited for normal distribution variables. Linear regression was used to calculate adjusted β estimates for the relation of HEI and AHEI components score with serum antioxidant concentration. The relationship between parameters was examined via Spearman's correlation coefficient analysis. A P < 0.05 was set as statistically significant.
Results
One hundred and fifty young women aged 20.8 ± 2.3 years were included in the study. The baseline anthropometric and laboratory characteristics of study groups are shown in Table 1 (according to the different tertiles of adherence to the HEI/AHEI). All the variables were normally distributed based on the Kolmogorov–Smirnov test (P > 0.05). The general parameters of participants were not significantly different across HEI/AHEI tertiles, but the uric acid was significantly higher in the highest tertile (T3) of HEI score compared to the lowest tertile (T1) (P < 0.05). Also, mean serum levels of total cholesterol were lower in the T3 than in the T1 of the AHEI score (P = 0.04; Table 2).
The comparison of antioxidant concentration of serum between tertiles of HEI and AHEI (n = 155).
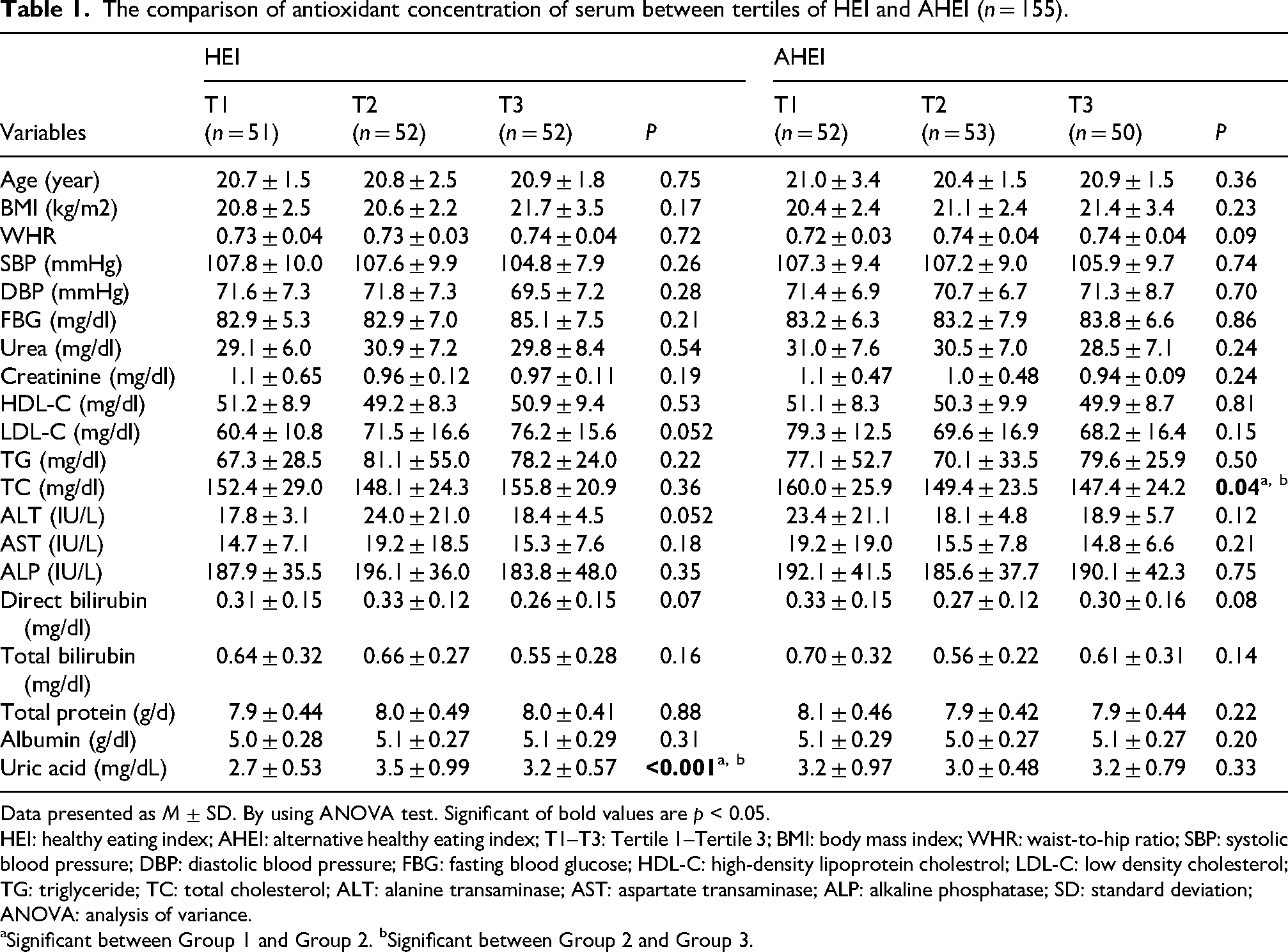
Data presented as M ± SD. By using ANOVA test. Significant of bold values are p < 0.05.
HEI: healthy eating index; AHEI: alternative healthy eating index; T1–T3: Tertile 1–Tertile 3; BMI: body mass index; WHR: waist-to-hip ratio; SBP: systolic blood pressure; DBP: diastolic blood pressure; FBG: fasting blood glucose; HDL-C: high-density lipoprotein cholestrol; LDL-C: low density cholesterol; TG: triglyceride; TC: total cholesterol; ALT: alanine transaminase; AST: aspartate transaminase; ALP: alkaline phosphatase; SD: standard deviation; ANOVA: analysis of variance.
Significant between Group 1 and Group 2. bSignificant between Group 2 and Group 3.
The comparison of antioxidant concentration of serum between tertiles of HEI and AHEI.
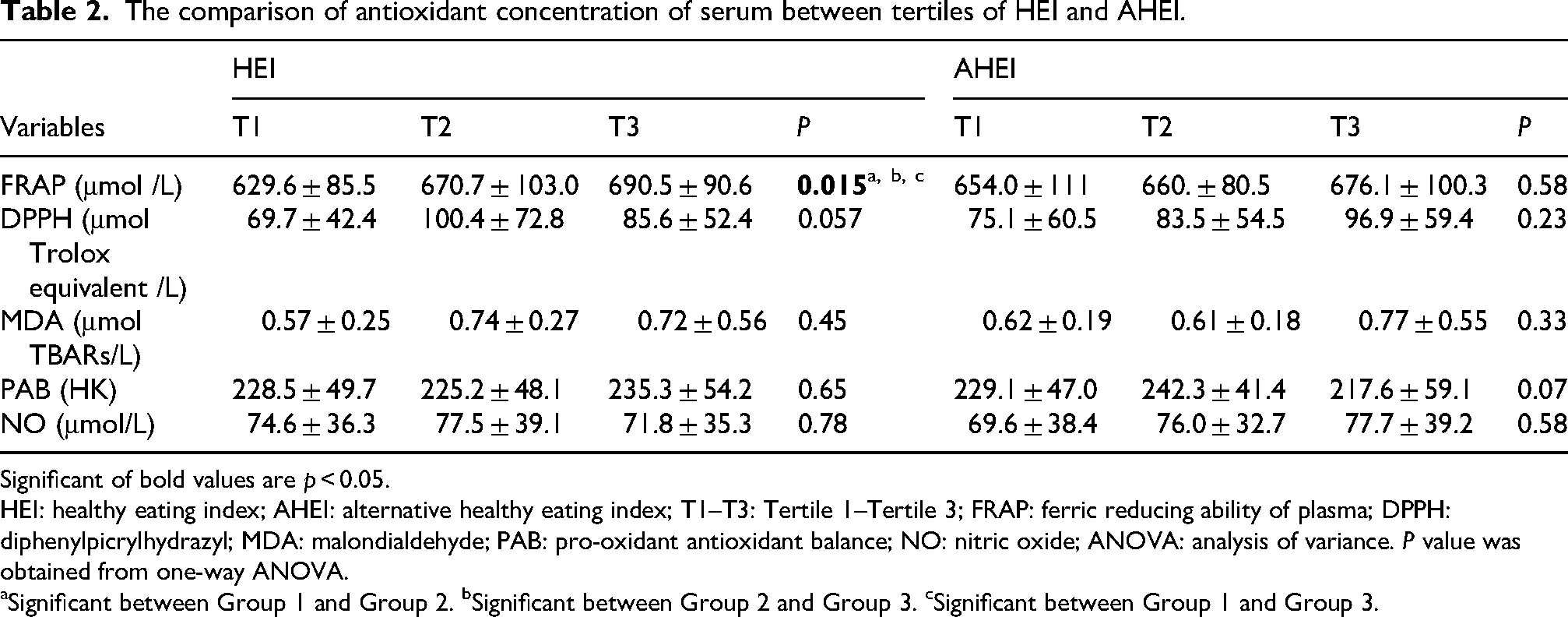
Significant of bold values are p < 0.05. HEI: healthy eating index; AHEI: alternative healthy eating index; T1–T3: Tertile 1–Tertile 3; FRAP: ferric reducing ability of plasma; DPPH: diphenylpicrylhydrazyl; MDA: malondialdehyde; PAB: pro-oxidant antioxidant balance; NO: nitric oxide; ANOVA: analysis of variance. P value was obtained from one-way ANOVA.
Significant between Group 1 and Group 2. bSignificant between Group 2 and Group 3. cSignificant between Group 1 and Group 3.
The oxidative status assessment showed that those who were in the third tertile for the HEI score had significantly higher levels of serum FRAP levels (P = 0.015). Although, the mean level of other antioxidant status biomarkers did not exhibit any statistically significant difference across tertiles of HEI/AHEI (P > 0.05; Table 2).
Multivariate linear regression analysis indicated that higher levels of serum FRAP were associated with a higher score for consumption of total fruit, dark green vegetables, total vegetables, and empty calories as well as lower score of PUFA intake (P < 0.05; Table 3). Intake of seafood and plant protein, nuts, and beans was positively associated with DPPH scores (β = 8.3, P = 0.012, and β = 2.4, P = 0.026, respectively)
Multivariate linear regression between score of HEI and AHEI components and antioxidant concentration of serum.
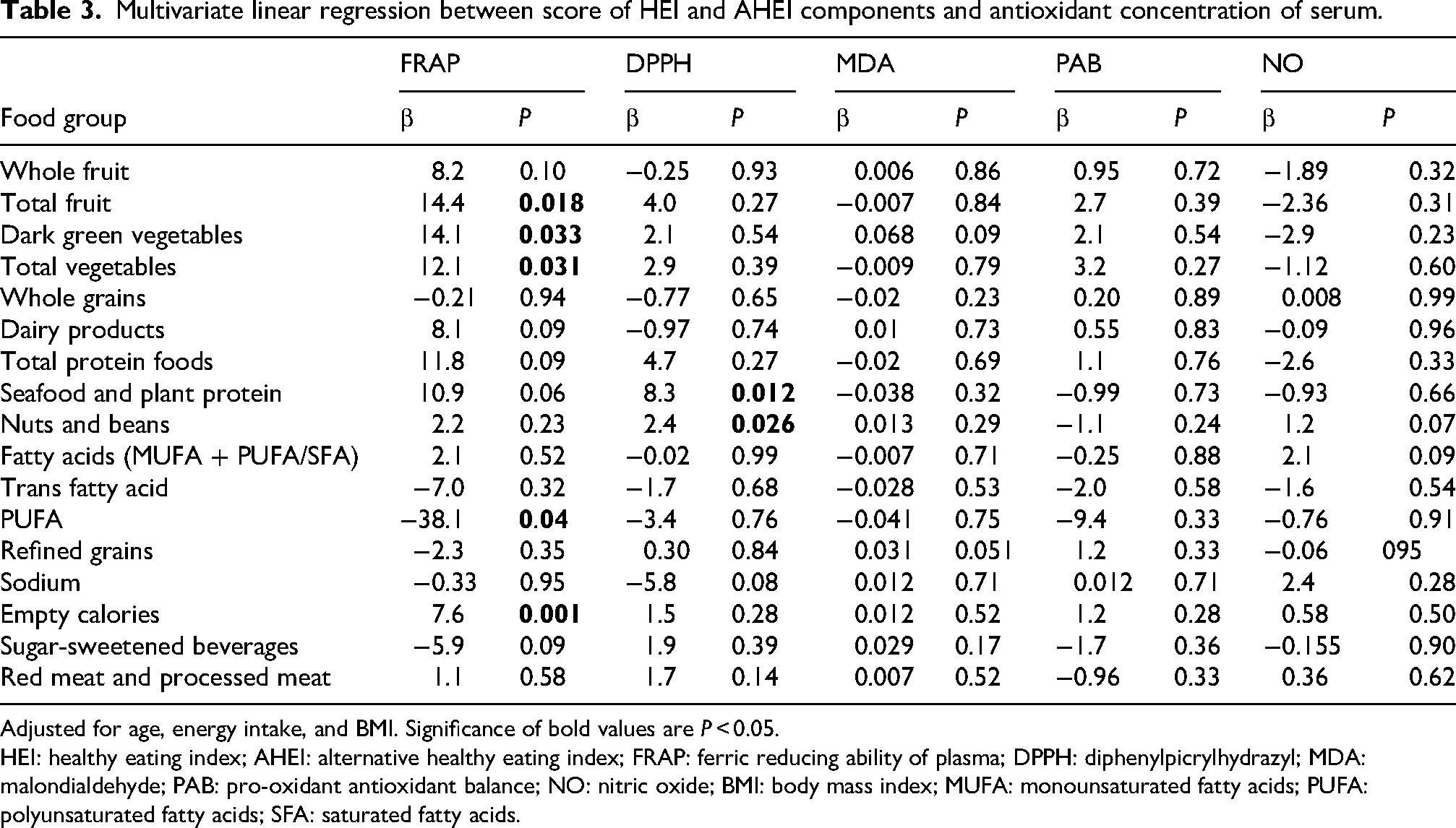
Adjusted for age, energy intake, and BMI. Significance of bold values are P < 0.05.
HEI: healthy eating index; AHEI: alternative healthy eating index; FRAP: ferric reducing ability of plasma; DPPH: diphenylpicrylhydrazyl; MDA: malondialdehyde; PAB: pro-oxidant antioxidant balance; NO: nitric oxide; BMI: body mass index; MUFA: monounsaturated fatty acids; PUFA: polyunsaturated fatty acids; SFA: saturated fatty acids.
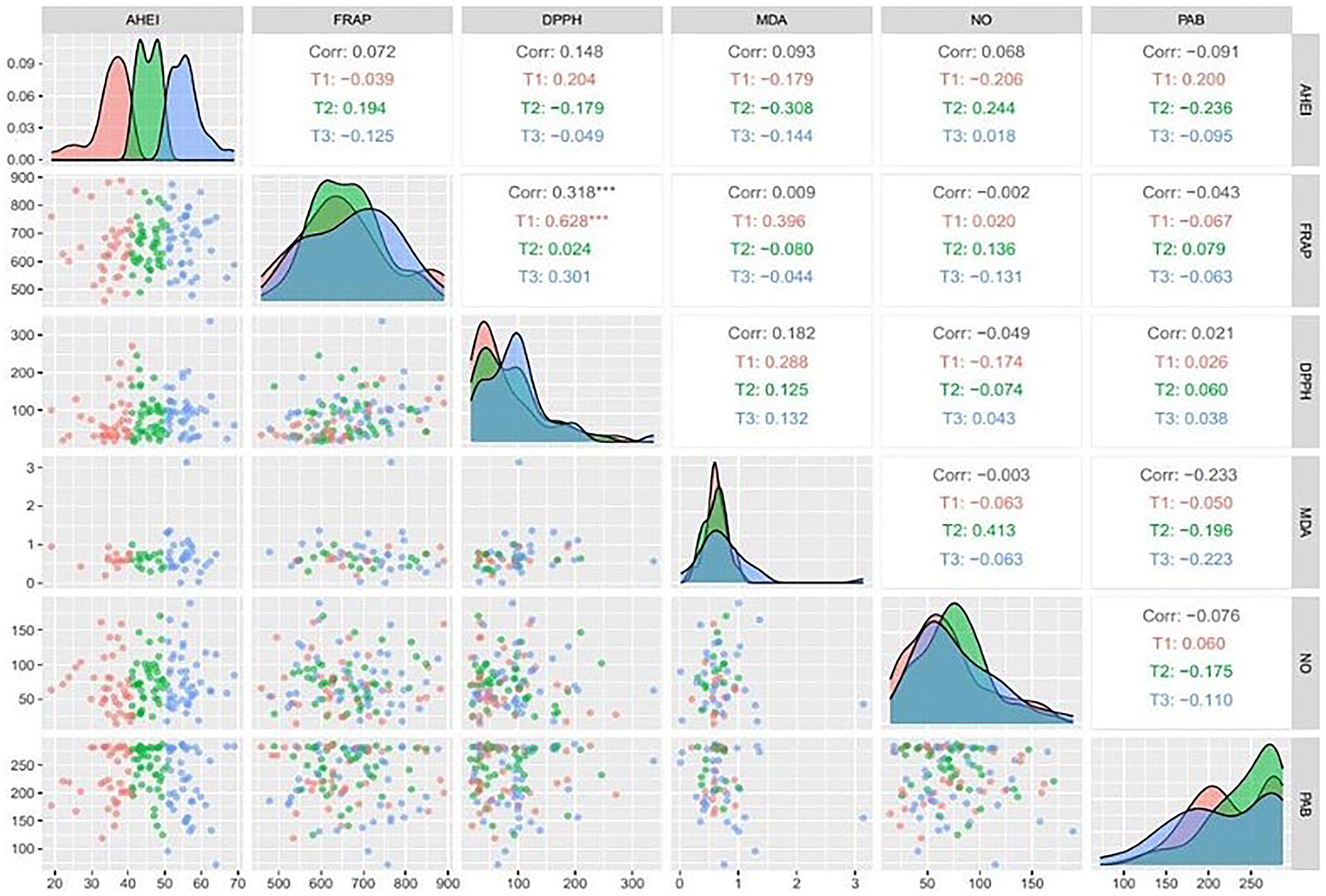
Results from correlation analysis between serum antioxidant levels and score of HEI and AHEI were shown in Figures 1 and 2. The serum levels FRAP significantly correlated with HEI score (r = 0.297, P < 0.001). Serum DPPH and FRAP levels also directly correlated with each other (r = 0.318, P < 0.001).
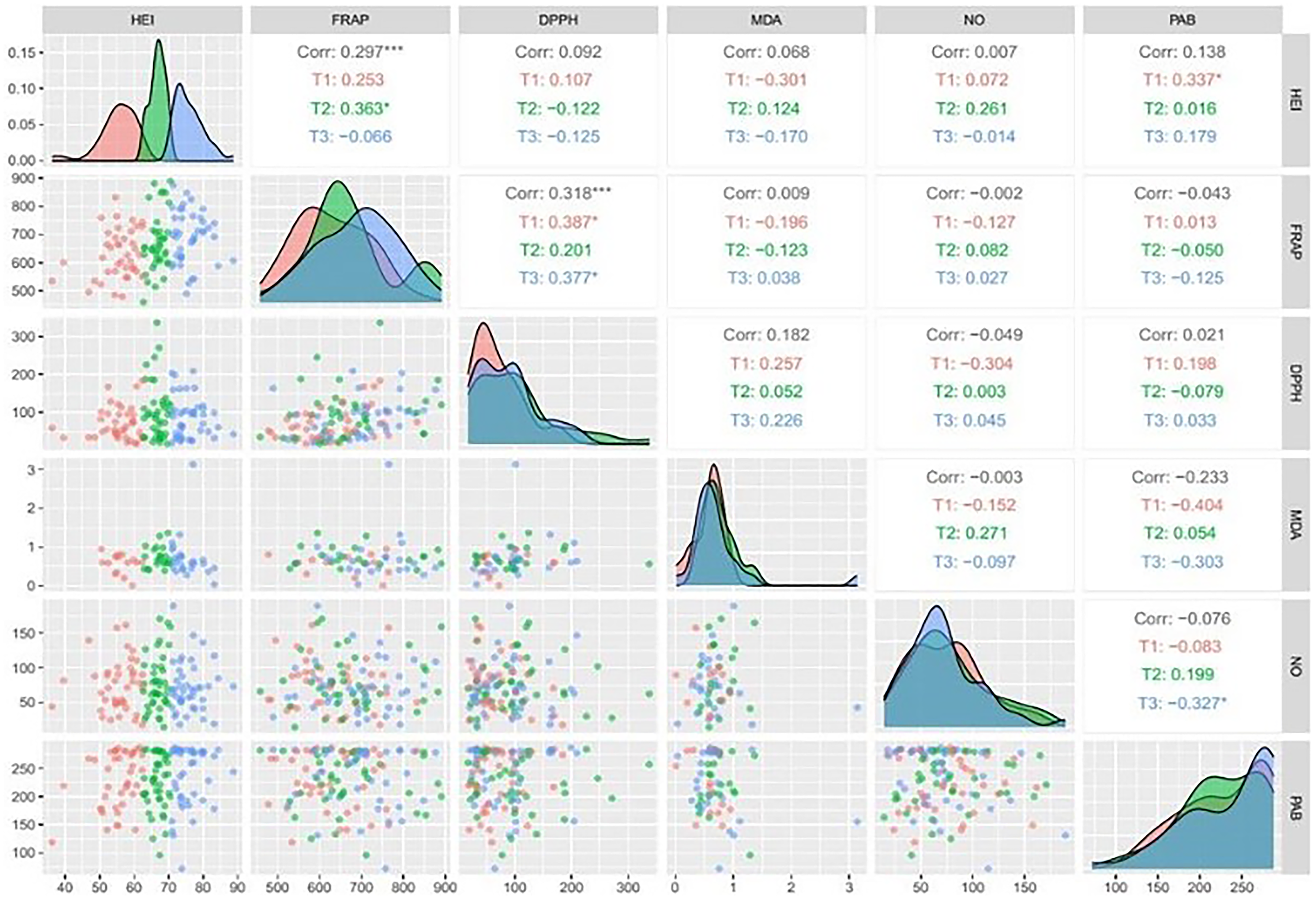
Correlation matrix showing overall and tertile-specific (T1–T3) Spearman correlations between healthy eating index (HEI) scores and serum antioxidant biomarkers (FRAP, DPPH, MDA, no, and PAB). Red, green, and blue represent tertiles; asterisks denote significant correlations (***P < 0.001).
Correlation matrix showing overall and tertile-specific (T1–T3) Spearman correlations between alternative healthy eating index (AHEI) scores and serum antioxidant biomarkers (FRAP, DPPH, MDA, no, and PAB). Red, green, and blue represent tertiles; asterisks denote significant correlations (***P < 0.001).
Linear regression analysis after adjustment for age and BMI demonstrated a direct association between HEI and serum FRAP level (β=3.03, SE = 0.89, P = 0.001; Figure 3).
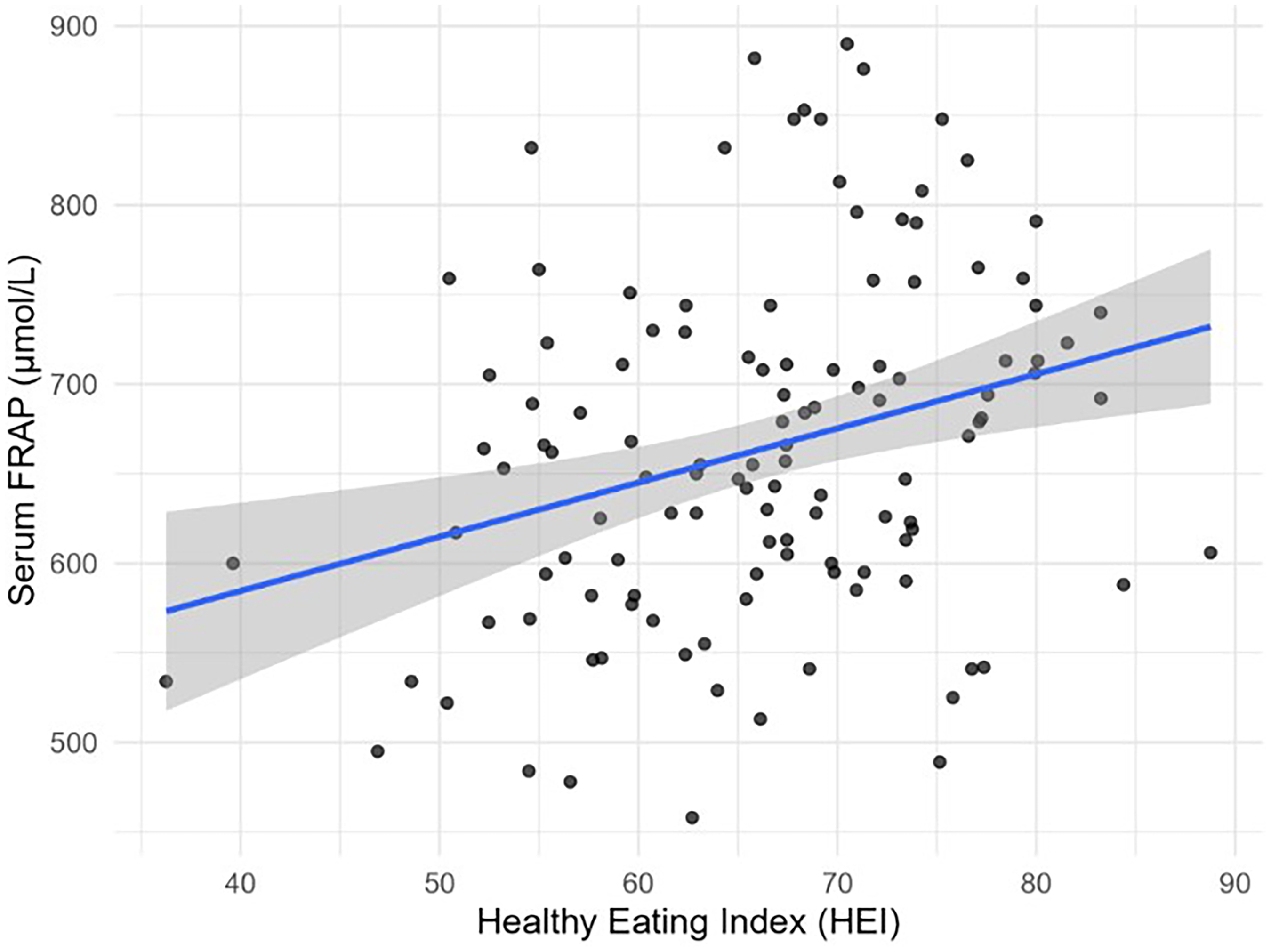
Adjusted linear regression between HEI and serum FRAP level (β = 3.03, SE = 0.89, P = 0.001).
Discussion
A significant weak positive correlation between HEI scores and serum antioxidant index levels, FRAP was found in this study. Although no significant differences were found between oxidant–antioxidant parameters and adherence to AHEI dietary recommendations (high AHEI scores). The HEI score ranges from 0 to 100, with higher scores reflecting a diet that is more followed with recommended dietary patterns. We found that young healthy women with a higher HEI have significantly greater serum FRAP concentrations. FRAP is a widely recognized laboratory method used to quantify the antioxidant capacity of serum or other biological samples. This biomarker is indicative of the ability of antioxidants in the diet to scavenge free radicals and reduce OS, thereby improving health and potentially alleviating the risk of chronic conditions (Bitla et al., 2012).
It has previously been reported that the serum FRAP levels were correlated with a higher HEI score in women with breast cancer, which could suggest the long-term advantageous effect of the diet on the health of these patients (Reitz et al., 2021). But in three trials, high dietary TAC (Peluso et al., 2018; Valtuena et al., 2008) and high vegetable (Peluso et al., 2018) diets did not significantly affect serum FRAP levels. Results from a population-based case-control study did not support a significant correlation between HEI and antioxidant status parameters, including MDA and TAC (Vahid et al., 2022).
Among the five oxidative/antioxidant biomarkers measured in our study, only FRAP showed a significant positive correlation with HEI score. Other investigations measuring multiple indices have reported similar apparent inconsistencies (Bahrami et al., 2023; Vahid et al., 2022). Similar findings were also reported previously in which FRAP was positively associated with dietary quality scores, including food quality score (Karbasi et al., 2023b), low-carbohydrate diet score (Moradi-Binabaj et al., 2023), Mediterranean diet score (Karbasi et al., 2023a), as well as healthy dietary pattern (Karbasi et al., 2022). The approach of using different biomarkers for conceptual endpoints, such as oxidative status, is reaffirmed by our present study.
We observed that a high consumption of antioxidant-rich foods such as fruits and vegetables was related to higher serum FRAP levels, which might reduce OS. Root et al. have also reported that a higher intake of fruit and vegetable associated with elevated plasma FRAP concentrations (Root et al., 2012). Fruits and vegetables are well-known for their health benefits, mainly due to their high amounts of vitamins, minerals, and phytochemicals. Fruits such as berries, citrus, and apples are known for their high levels of vitamin C, flavonoids, and polyphenols, all of which possess substantial antioxidant properties (Addi et al., 2022; Proteggente et al., 2002). Similarly, dark green vegetables, including spinach, kale, and broccoli, are rich in vitamins A, C, E, and K, along with carotenoids and other phytochemicals, which have been shown to contribute significantly to the antioxidant capacity of the diet (Butt and Sultan, 2018; Kaparapu et al., 2020; Podsędek, 2007). A diverse vegetable intake implicates synergistically to the antioxidant capacity because of the presence of a variety of phytonutrients. For instance, red and orange vegetables such as carrots and tomatoes contain lycopene and beta-carotene, powerful antioxidants that complement the effects of dark green vegetables (Soytong et al., 2021). Cruciferous vegetables, such as cabbage, are known for their high glucosinolate content, which may enhance detoxification processes and fortify the body's defense against OS (Akram et al., 2021). The antioxidant capacity of fruits and vegetables isolated from their phytochemical composition can be attributed to several mechanisms. Phytochemicals such as polyphenols possess potent free radical scavenging actions. This capability to neutralize free radicals alleviates the damage to cellular structures and DNA, which are important in the prevention of chronic diseases. Secondly, specific vitamins, particularly vitamin C and vitamin E, function as electron donors, which potentially stabilize free radicals. Furthermore, dietary fiber abundant in fruits and vegetables contributes to gut health, which in turn can affect OS and inflammation status within the body. Moreover, the consumption of fruits and vegetables is usually accompanied with promoted overall dietary quality, which requires higher intakes of essential nutrients and lower intakes of processed and high-sugar foods, causing to a more balanced metabolic profile (Chang et al., 2019; Prakash et al., 2011). This comprehensive approach to nutrition can significantly improve the body's inherent antioxidant defenses, which eventually enhances serum FRAP levels.
Although both FRAP and PAB are indicators of redox status, FRAP primarily reflects the plasma's total reducing capacity, while PAB represents a combined measure of pro-oxidant and antioxidant forces (Alamdari et al., 2008). In our young, healthy population, the pro-oxidant load was likely low, resulting in limited variability in PAB values and consequently reducing the likelihood of observing a significant correlation with FRAP.
Another finding of our study revealed that higher HEI is also related to increment serum uric acid levels. This can be explained that uric acid is an endogenous antioxidant that accounts for up to 80% of the total antioxidant potential. In a physiological concentration, it is the most substantial plasma antioxidant, while in higher levels, it can produce free radicals with pro-oxidative features (Puścion-Jakubik et al., 2022).
In our study, participants with higher AHEI scores had significantly lower total cholesterol levels, which are in line with previous studies. Findings of two cross-sectional studies revealed a significant direct association between high-density lipoprotein cholestrol and HEI scores (Rashidipour-Fard et al., 2017; Vahid et al., 2022). An elevated HEI/AHEI score highlights a higher intake of fruits, vegetables, low-fat dairy products, whole grains, as well as low-fat meats, which could considerably improve lipid profiles (Lavoie et al., 2013; Rashidipour-Fard et al., 2017).
Our findings indicate that the HEI was more strongly associated with serum FRAP levels compared to the AHEI. This may be explained by the fact that the HEI captures overall diet quality based on general dietary guidelines, including components such as dairy, total protein foods, refined grains, sodium, and empty calories, which may show greater variability in young populations (Guenther et al., 2014). In contrast, the AHEI is more focused on predicting chronic disease risk and emphasizes components such as trans fat, red/processed meat, and alcohol, which likely had limited variability in our study population (Chiuve et al., 2012). Furthermore, fruit and vegetable intake—a key contributor to antioxidant status—is heavily weighted in the HEI and has been consistently associated with higher serum FRAP levels (Root et al., 2012). This may explain the stronger association we observed between the HEI and FRAP.
This study has several limitations. First, the dietary data are subject to recall bias, as intake was assessed using an FFQ. Second, the cross-sectional design does not allow for the establishment of causal relationships. Finally, the study consisted of a specific demographic group (young women), which may limit the generalizability of the findings to the broader population.
Conclusion
We found the HEI as an important measurement tool evaluating dietary quality, significantly associated with serum antioxidant FRAP levels. Promoting high HEI scores via healthy dietary practices not only reflects a commitment to balanced nutrition but also strengthens the body's defenses against OS, eventually developing overall health and well-being. While higher HEI scores were associated with elevated FRAP levels, other lifestyle or genetic factors may contribute to antioxidant status. Future studies should investigate whether improving HEI scores through dietary interventions leads to measurable increases in serum FRAP levels and whether these changes translate into reduced risk of chronic diseases associated with OS. Longitudinal and randomized controlled trials across more diverse populations, including men and older adults, are warranted to confirm these associations and establish causal relationships.
Footnotes
Acknowledgements
We would like to thank the Clinical Research Development Unit, Imam Reza Hospital, Mashhad University of Medical Sciences, for their assistance in this manuscript. We also appreciate the assistance of the Clinical Research Development Unit of Akbar Hospital, Mashhad, in conducting this research.
Ethics approval and consent to participate
This study was performed in accordance with the Declaration of Helsinki. This study received ethical approval from the Research Ethics Committee of Birjand University of Medical Sciences (IR.BUMS.REC.1398.402). Informed consent was obtained from all participants included in this study.
Consent for publication
All authors have read and consent for publication of this manuscript.
Author contributions
Afsane Bahrami contributed to project administration, conceptualization, resource, funding acquisition, and writing–original draft. Zahra Asadi contributed to supervision, investigation, methodology, software, formal analysis, and writing–review and editing. Gordon A. Ferns contributed to investigation, validation, and writing–review and editing. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Birjand University of Medical Sciences.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data supporting the findings of this study are available on request from the corresponding author. “Clinical trial number: not applicable.”