
Abstract
Chylothorax, a rare condition, results when excessive chyle accumulates in the thoracic region. The etiological basis of chylothorax is categorized into three types: spontaneous, non-spontaneous, and idiopathic. However, it is usually manifested as a post-operative complication after thoracic or abdominal surgeries. Due to its rarity, limited research has been done to explore its causes and treatment. This review aims to explore treatment options for chylothorax with a special focus on its management through medium-chain triglyceride provision. In this article, we discussed the etiology, complications, clinical manifestations, and diagnosis of chylothorax, and reviewed the effectiveness of the medium-chain triglycerides diet as a first-line approach in the treatment of chylothorax. As chylothorax diagnosis is established by the presence of triglycerides in chyle fluid, the provision of medium-chain triglycerides has been thought to be an effective treatment strategy due to their efficient absorption. However, chylothorax complications have not only included immunological and localized complications, but nutritional complications are also an important concern during their management. Medium-chain triglyceride provision has emerged as an important therapeutic aid in the medical nutrition therapy of chylothorax. However, there is no current consensus on specific parameters reflecting the effectiveness of medium-chain triglycerides in chylothorax. Therefore, it is reflected by reduced chyle output, improved nutritional status, shortened drainage duration, and decreased need for surgical intervention in cases where medium-chain triglycerides intervention was done.
This is a visual representation of the abstract.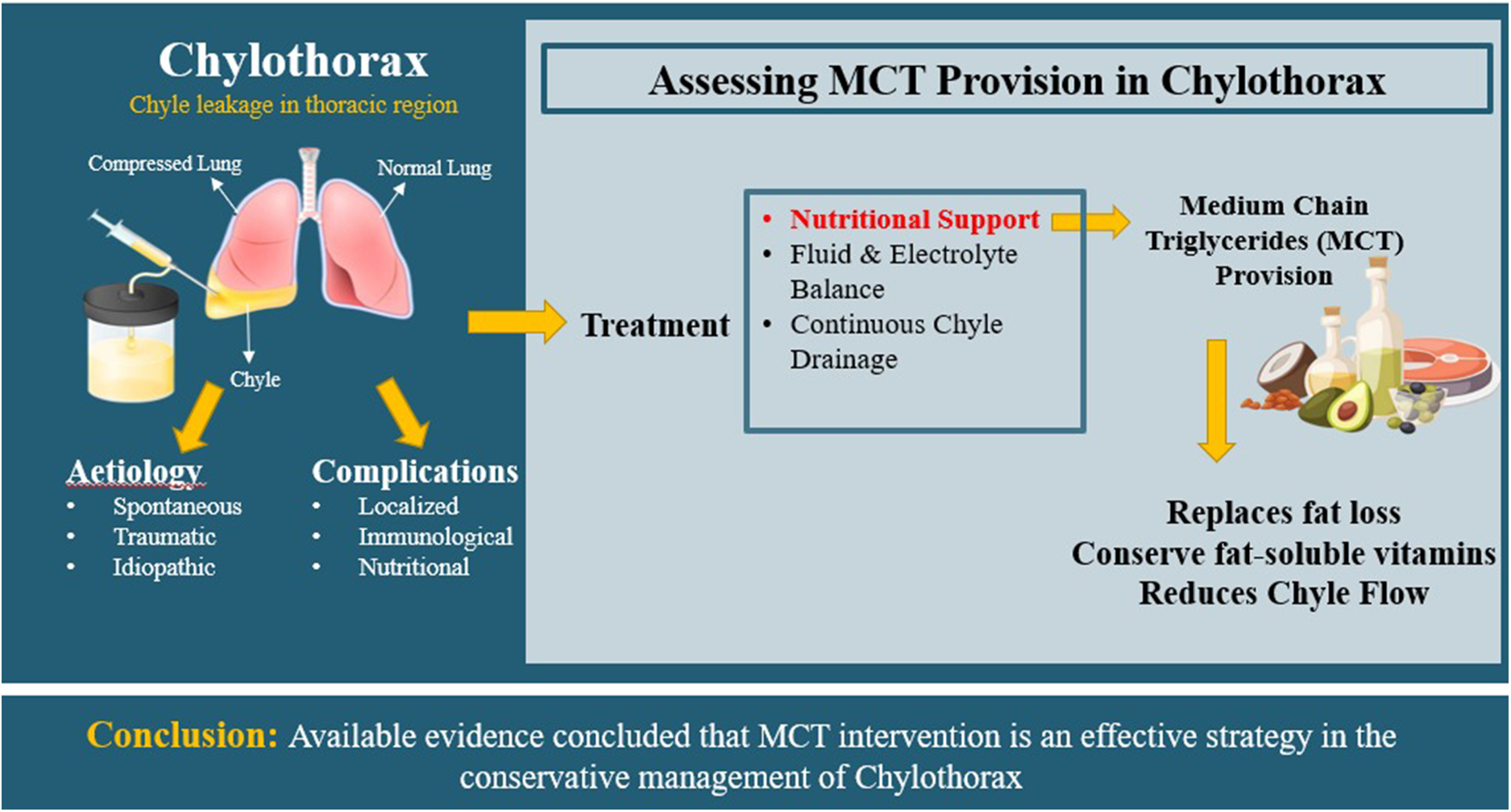
Introduction
Chylothorax or Chylous Pleural Effusion is a pathological condition that develops with the accumulation of chyle, a lymphatic fluid, in the pleural region (Hock et al., 2021). Although it represents only 3% of pleural effusion cases, it accounts for 82% of associated mortality due to profound malnutrition and immunosuppression (Bhatnagar et al., 2024). It usually occurs due to any obstruction or blockage in the thoracic duct and is characterized by the presence of chylomicrons (Bender et al., 2016). Anatomically, the thoracic duct arises in the abdomen from the superior aspect of the cisterna chyli and ascends into the thoracic cavity through the aortic hiatus of the diaphragm. In this course, it travels upward along the right side of the aorta, positioned posteriorly in close association with the esophagus (Thuraisingam, 2023). Chylothorax is usually manifested as a postoperative complication, particularly following esophageal surgery, with an incidence ranging from 2% to 6.5% (Bauer et al., 2023).
Chylothorax can arise from diverse etiologies, including traumatic injury, malignancies, congenital lymphatic abnormalities, infectious causes, and other non-traumatic conditions (Bhatnagar et al., 2024). In addition, chylothorax diagnosis is primarily confirmed through pleural fluid analysis, wherein elevated triglycerides and cholesterol levels serve as key biochemical markers, making fluid examination a crucial diagnostic cornerstone (Garcia Franco et al., 2023). In terms of management, conservative management remains a first-line approach, typically followed by surgical interventions when necessary (Nyatsambo et al., 2023). However, due to the rarity and limited research of this condition, there is currently no universally validated treatment algorithm, and existing literature largely comprises single-center studies, retrospective analyses, and case reports (Hock et al., 2021; Jeckowski et al., 2023; Paciotti et al., 2023).
Dietary modification forms the foundation of conservative management, with emphasis on reducing long-chain triglycerides (LCTs) while incorporating a high-protein, low-fat diet supplemented with medium-chain triglyceride (MCT) and/or Total Parenteral Nutrition (TPN) to reduce lymphatic flow and promote healing (Clark et al., 2023; Hock et al., 2021). Although MCT-based nutritional strategies have been increasingly explored over the past decade, further evidence is still required to determine optimal dosing and treatment protocols (Kerstein et al., 2023).
The present review discusses the etiology, clinical manifestation, and complications associated with chylothorax, with particular focus on evaluating the therapeutic role of MCTs within conservative management strategies. By synthesizing current literature and highlighting the most promising clinical outcomes associated with MCT-based dietary interventions, this review offers a timely perspective that contributes novel insight into conservative therapeutic approaches for chylothorax.
Chyle composition and transportation
The word chyle originates from its Greek root word “Chylos” which refers to juice. Dietary fats are an integral component of chyle, a turbid and odorless fluid, with a milky appearance due to the high content of chylomicrons (Besselink et al., 2017). Dietary fat, primarily triglycerides, makes up about 70% of the chylomicron. The typical composition of chyle includes 5–30 g/L of fats, 20–30 g/L of protein, and 200 kcal/L, along with varying amounts of phosphate (0.8–4.2 mmol/L), sodium (104–108 mmol/L), potassium (3.8–5.0 mmol/L), chloride (85–130 mmol/L), and calcium (3.4–6.0 mmol/L). Chyle also contains cellular components with lymphocyte counts ranging from 400 to 6800/mL and erythrocyte counts between 50 and 600/mL, respectively (Fogg et al., 2023; McCray and Parrish, 2011). Furthermore, chyle is a triglyceride-rich lymphatic fluid (Mohan Rudrappa and Paul, 2023). Lymph fluid constitutes the major portion of chyle, but it also contains LCTs, free fatty acids, fat-soluble vitamins, and chylomicrons. Moreover, a small proportion of enzymes and immunoglobulins is also present in chyle (Fogg et al., 2023).
In addition, short-chain triglycerides and MCTs are rapidly hydrolyzed by intestinal lipases, facilitating their direct absorption into portal circulation. On the other hand, complex LCTs are not directly absorbed in the intestinal mucosa; instead, they are re-esterified and assembled into chylomicrons through association with cholesterol, phospholipids, and cholesterol esters within enterocytes of the jejunum. These chylomicrons are subsequently transported to the intestinal lymphatic vessels of the intestinal villi, contributing to the formation of chyle (Mohan Rudrappa and Paul, 2023; Zarei et al., 2023).
The intestinal lymphatic system converges with the lymphatic drainage of the lower extremities to form the thoracic duct, which subsequently empties into the systemic circulation (Breslin et al., 2018). Approximately 60% of dietary fat is transported into the lymphatic system, with the thoracic duct serving as the principal pathway for lipid transport from the gastrointestinal tract into the bloodstream (Zhou et al., 2020). Under physiological conditions, an adult normally produces 2.4 liters of chyle/day; however, obstruction or disruption of the thoracic duct can result in chyle leakage and accumulation within adjacent spaces, ultimately leading to the development of chylothorax (Mohan Rudrappa and Paul, 2023).
Etiology of chylothorax
Chylothorax etiology has been classified into three categories: spontaneous, traumatic, and idiopathic (Cholet et al., 2020; McGrath et al., 2010). Spontaneous chylothorax, also referred to as non-traumatic or tumorous, includes malignancies, congenital, neoplastic, and infectious etiology, as well as conditions that compromise the thoracic duct, such as goiter, amyloidosis, thrombosis, cirrhosis, primary thoracic lymphangiectasia associated with disorders like Down Syndrome, or sarcomas, and chest irradiation (Almasri et al., 2021). Only a limited number of studies have explored the association of chylothorax with Down syndrome, which increases the risk not by directly damaging a normal thoracic duct, but by being associated with congenital lymphatic and venous anomalies that predispose individuals to thoracic duct dysfunction (Avci et al., 2009; Danopoulos et al., 2021).
The traumatic cause of chylothorax is broadly divided into iatrogenic (surgical) and non-iatrogenic (McGrath et al., 2010). Iatrogenic chylothorax most commonly occurs following surgical procedures involving the neck, thorax, or upper abdomen, including esophagectomy, mediastinal resection, and vagotomy, and accounts for approximately 50% of all reported cases (Agrawal et al., 2022; Zarei et al., 2023). Furthermore, thoracic duct obstruction or damage associated with central venous catheterization is also recognized as an important iatrogenic cause (Alkayed et al., 2013). Inclusively, iatrogenic etiologies account for approximately 80% of all traumatic chylothorax cases, underscoring their clinical significance (Pillay and Singh, 2016). In contrast, non-iatrogenic traumatic chylothorax typically results from blunt or penetrating thoracic injuries, including gunshot wounds or knife and stab injuries (Hussein et al., 2024). Additionally, it may arise due to a sudden and substantial increase in intrathoracic pressure from severe coughing or vomiting, which can lead to ductal rupture (Bhatnagar et al., 2024).
Idiopathic chylothorax refers to the occurrence of chylothorax in the absence of a clearly identifiable underlying cause (Nayir Buyuksahin et al., 2023). Although classified as idiopathic, this category is frequently linked to previously undiagnosed malignancies and accounts for approximately 10% of all reported cases (McGrath et al., 2010; Mohan Rudrappa and Paul, 2023). Moreover, primary or secondary lymphatic dysfunction and oncological causes, including lung cancer, esophageal cancer, thyroid cancer, and lymphoma, are some other known causes of chylothorax (Cholet et al., 2020).
Figure 1 depicts a graphical representation of spontaneous, traumatic, and idiopathic causes of chylothorax.
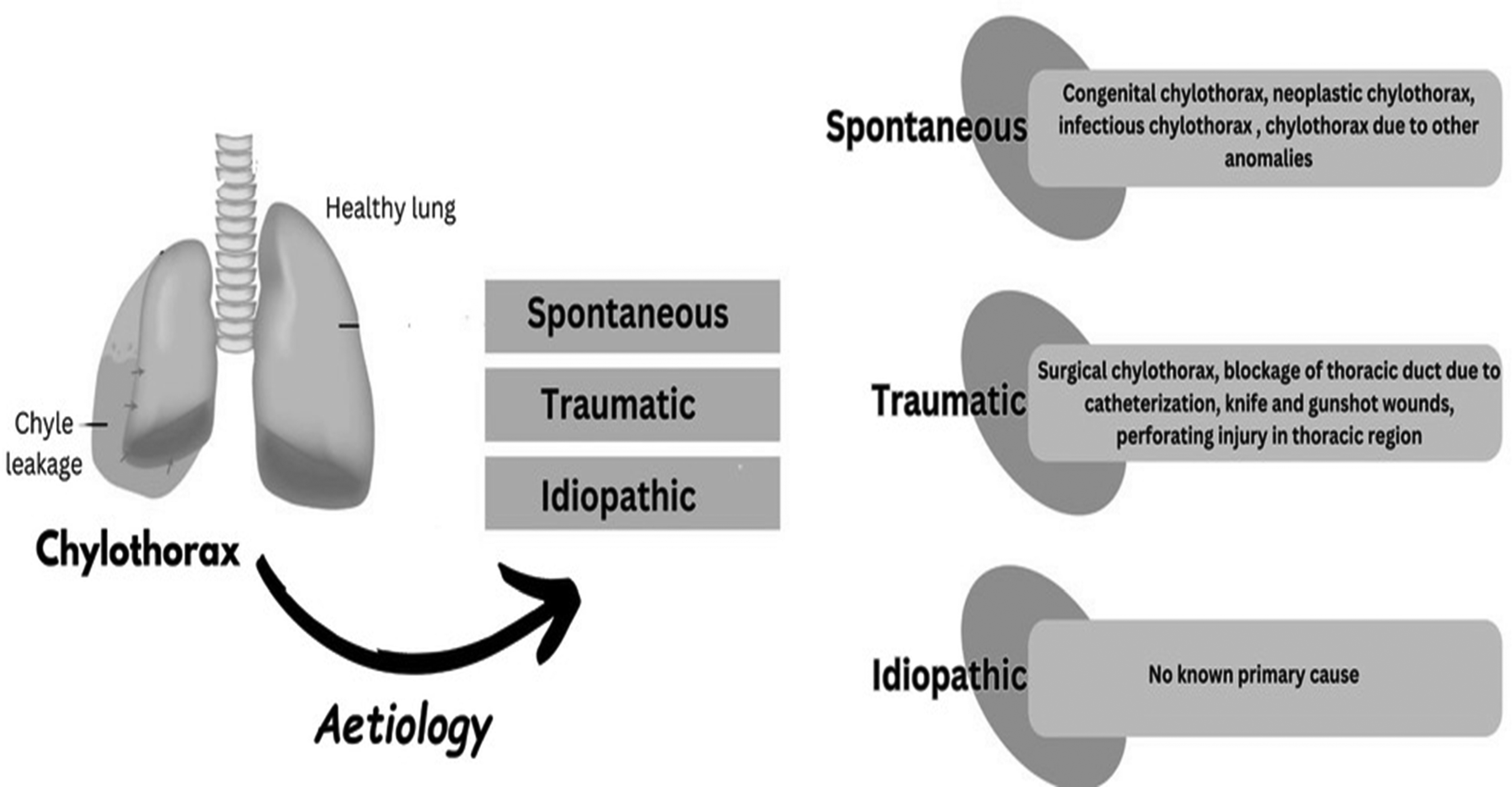
Etiology of chylothorax.
Clinical manifestation and diagnostic criteria of chylothorax
Shortness of breath, which is referred to as dyspnea and hypoxia (deficiency of oxygen), is the typically observed clinical feature in patients of chylothorax due to increased pressure on the lungs because of pleural effusion (Nayir Buyuksahin et al., 2023). Gradual symptoms occur in non-traumatic chylothorax, while traumatic chylothorax shows spontaneous symptoms in less than 2–10 days of surgery or injury (Mohan Rudrappa and Paul, 2023).
Pleural fluid analysis remains the cornerstone for diagnosing chylothorax. Notably milky appearance of pleural fluid is observed macroscopically; however, in fasting and post-operative states, pleural effusion may appear clear due to limited fat intake. The milky effusion may also occur in the case of pseudo-chylothorax, which is caused by chronic diseases like tuberculosis (Schild et al., 2013). A turbidity test is done to distinguish between chylothorax and pseudochylothorax by adding small quantities, up to 1–2 ml of ethyl ether in chyle, as the latter condition loses its milky appearance (Riley and Ataya, 2019; Surabhi et al., 2024). However, some studies have reported otherwise, indicating consideration of other parameters as well (Anand et al., 2022; Ur Rehman and Sivakumar, 2022). Moreover, the pleural fluid analysis was performed to determine the triglyceride levels in the pleural fluid. If the triglyceride amount in chyle is >100 mg/dL, then chylothorax is confirmed; <50 mg/dL elucidates the absence of chylothorax, but if the test shows the triglyceride levels between 50–100 mg/dL, then the pleural chylomicrons test should be done by lipoprotein electrophoresis, which validates the presence of chylothorax (Bhatnagar et al., 2024). Cholesterol is <200 mg/dL in this case, while >200 mg/dL in pseudo-chylothorax (Nair et al., 2007; Riley and Ataya, 2019). Hence, key diagnostic features include chylomicron-rich pleural fluid with raised triglycerides and lowered cholesterol levels (Bhatnagar et al., 2024; Garcia Franco et al., 2023). Chylomicron presence is considered a standard diagnostic criterion for chylothorax (Esme, 2019). Moreover, the absence of chylomicrons in other pleural effusions makes it a distinguishing feature for establishing chylothorax diagnosis regardless of their quantification. Elevated triglyceride levels with the presence of chylomicrons in the pleural fluid confirm chylothorax in any patient (García et al., 2017). When fasting, an average adult's thoracic duct can transport fluid up to 0.38 mL/min (550 mL/24 h), and in the post-prandial state, it can transport 3.9 mL/min (Sriram et al., 2016). Protein, albumin, fat, and vitamins are lost result of continuous leakage from the thoracic duct (Nair et al., 2007). Pleural fluid differential lymphocyte analysis is a key diagnostic indicator of chylothorax, accounting for more than 50–70% of total cellular content in affected individuals (Arrigo et al., 2023; Bhatnagar et al., 2024).
In non-traumatic chylothorax, abdominal and thoracic imaging is recommended to identify the underlying malignancy (Rehman and Sivakumar, 2022). Further, chylous pleural fluid is typically exudative, with high protein content relative to lactate dehydrogenase (LDH), and is commonly assessed using criteria: a pleural fluid serum protein ratio >0.5, pleural fluid/serum LDH ratio>0.6, or a pleural fluid/LDH exceeding two-thirds of the upper serum LDH limit, whereas average protein concentration in chyle ranges from 20–60 g/L (Duletzke et al., 2023; Porcel, 2021; Ur Rehman and Sivakumar, 2022).
Complications and consequences of chylothorax
Chyle is a nutrient-dense lymphatic fluid containing substantial amounts of dietary lipids, fat-soluble vitamins, lipoproteins, enzymatic proteins, immunoglobulins, electrolytes, and a high concentration of lymphocytes. Therefore, persistent chyle leakage in chylothorax results in significant nutritional depletion, metabolic imbalances, and immunological compromises (Du Rieu and Mabrut, 2011; Edna Patatanian and Sharp, 2022). Clinically, patients may present with progressive weight loss, fatigue, lethargy, dehydration, electrolyte imbalance, recurrent infections, and impaired wound healing. Early metabolic consequences typically include hypovolemia, hyponatremia, hypocalcemia, metabolic acidosis, and deficiencies in fat-soluble vitamins due to continuous loss of triglyceride-rich lymphatic fluid (Du Rieu and Mabrut, 2011). In some cases, hypoalbuminemia, which is low levels of blood albumin <3 g/dL and low blood IgG levels <500 mg/dL, is reported to be a complication of chylothorax. In addition, severe lymphopenia expressed as <1000 lymphocytes/mL in blood has also been reported (Perez-Perez et al., 2023).
If chylothorax remains unrecognized and inadequately managed, the accumulation of chyle in the pleural cavity compromises pulmonary mechanics, leading to dyspnea, decreased lung expansion, and eventually progressive pulmonary atelectasis (Du Rieu and Mabrut, 2011). The resulting respiratory compromise may manifest as hypoxia, tachypnea, and in severe cases, acute respiratory failure (Riley and Ataya, 2019). Additionally, chronic chylous effusion can exert pressure on intrathoracic structures and impair cardiovascular physiology. Accumulation of chyle fluid around the pericardium can be a cause of mechanical compression of the heart, locally affecting the cardiorespiratory system, and can cause tamponade (Stephens and Morell, 2023). Furthermore, prolonged chyle loss disrupts gastrointestinal lymphatic drainage and digestive processes, contributing to malabsorption, worsening nutritional decline, and an overall deterioration of physiological homeostasis (Hock et al., 2021). The associated immune suppression markedly increases the risk of recurrent respiratory infections, Pneumonia, and sepsis, which are significant contributors to morbidity and mortality in chylothorax (Bauer et al., 2023; Paciotti et al., 2023). A schematic diagram of complications of chyle leakage has been presented in Figure 2.
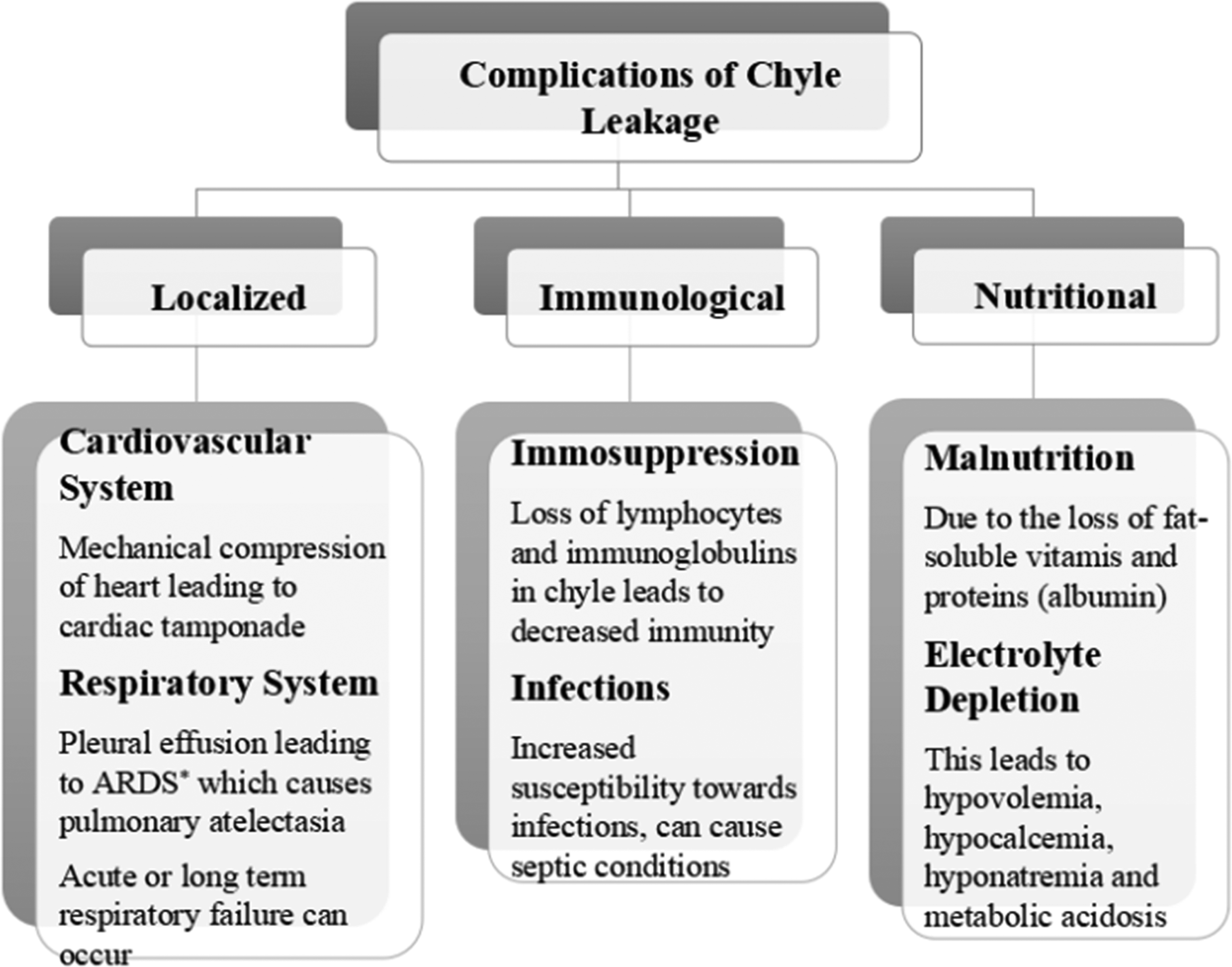
Complications of chyle leakage.
Treatment strategies
There is a lack of adequate randomized trials regarding the treatment of chylothorax and its efficacy. Nevertheless, the approach to treating chylothorax is entirely contingent on the underlying cause and the severity of the condition (Mohan Rudrappa and Paul, 2023). Various management strategies are suggested in previous literature, i.e., conservative and surgical treatment, and interventional radiology (Schild et al., 2013). The initial approach to treating chylothorax involves conservative measures, with a primary focus on adequate fluid and electrolyte replacement, coupled with proper nutritional support (Lee et al., 2008). Repeat thoracocentesis is typically reserved for situations where short-term treatment of the underlying disease is anticipated to bring improvement or when occasional aspiration is sufficient to address clinical symptoms. In cases of high-volume or notably symptomatic chylothorax, continuous drainage is employed to facilitate lung re-expansion and optimize pulmonary function (Berg, 2012). The patient may receive a diet rich in MCT (Benedix et al., 2012). Additionally, medication such as somatostatin or its analog octreotide can be employed to diminish lymph flow (Das and Shah, 2010). Modern drug treatments to reduce chyle output employ alpha-adrenergic agonists (Agrawal et al., 2022). A case series reported the use of midodrine as a first-line drug in drug therapy for chylothorax (Peralta et al., 2024). Similarly, etilefrine treatment in two infants for postoperative chylothorax was proven successful after failure of conservative measures (Muniz et al., 2018). In cases of non-traumatic chylothorax, addressing the underlying disease through treatments like chemotherapy or irradiation may result in improvement, although the success rates are constrained (TENG et al., 2012).
When conservative measures prove ineffective, surgery has traditionally been the only remaining treatment option. If employed early, surgical intervention can significantly reduce the mortality rate associated with chylothorax from 50% to 10% (Itkin et al., 2011). Surgical treatment is considered warranted when daily drainage exceeds 1000–1500 mL of chyle (with a pediatric threshold of >100 mL/kg body weight), when the drain output reaches 1000 mL/day for five consecutive treatment days, or in the case of children, when it amounts to 100 mL/year of age. Other indications for operative intervention include a persistent leak lasting more than 2 weeks (100 mL/day for >2 weeks), unchanged drain output over 1–2 weeks, or clinical deterioration marked by conditions like malnutrition or metabolic issues. Surgical procedures encompass a range of interventions such as thoracic duct ligation, pleurodesis, pleurectomy, pleuroperitoneal shunt, and intermittent external drainage through catheter systems (Schild et al., 2013). These techniques are found most effective in postoperative chylothorax, with reported success rates of 90%; however, efficacy for spontaneous and idiopathic cases is comparatively less (Agrawal et al., 2022).
Currently, various radiological treatments are available for both traumatic and non-traumatic chylothorax, with some still limited to specific centers. In cases of hepatic chylothorax, a transjugular intrahepatic portosystemic shunt can be utilized to decrease portal venous pressure and, consequently, lymph flow. For non-traumatic chylothorax, procedures such as lymphography, percutaneous thoracic duct embolization, and percutaneous needle disruption of lymphatic pathways are viable options (Schild et al., 2013). Figure 3
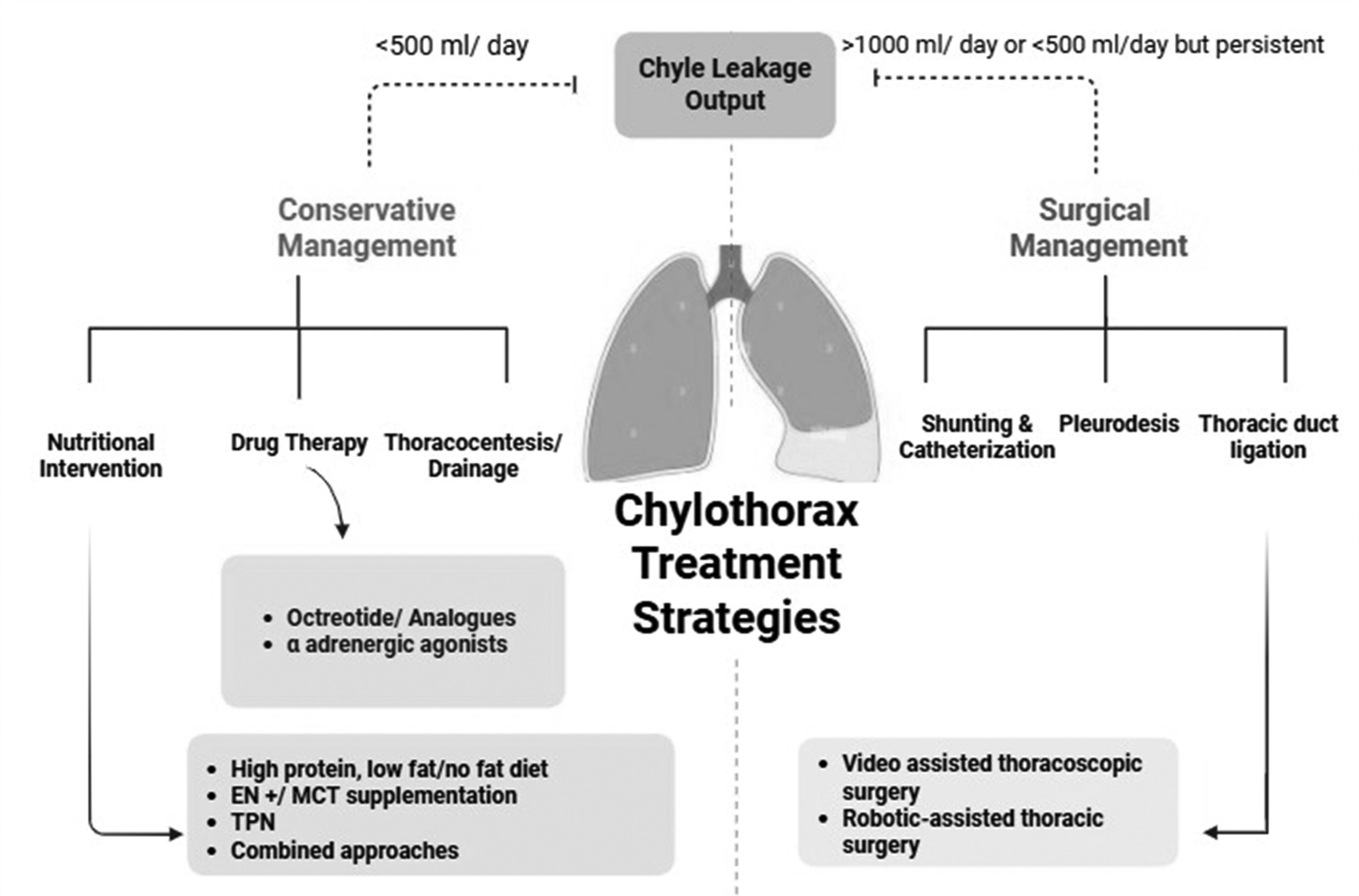
Treatment strategies of chylothorax
Effectiveness of MCT provision in chylothorax
The focus of this review article is to elaborate on the efficiency of MCT provision in the management of chylothorax as evidenced through previous literature. In order to lower the overall complication profile and promote spontaneous healing of the causing injury, it is essential to reduce chyle flow. After meals, especially those high in fat, there is an increase in the flow of chyle in the thoracic duct (Al-Sahaf, 2021). Therefore, in conservative management of chylothorax, the optimal therapeutic approach includes limited fat intake. However, it is virtually impossible to remove all fats from the diet as all food commodities contain fat traces to some extent. Currently, there is no established protocol for treating chylothorax (Pulle et al., 2021). However, it is suggested that fat intake should be limited to <10 g/day with restricted LCTs, preferably administered orally (Fogg et al., 2023; Takuwa et al., 2013). In addition, MCTs supplementation should be provided. Enteral nutrition remains the first-line treatment, typically consisting of 90% MCTs and 10% other proteins (Zheng et al., 2020). Commonly administered enteral formulas are Lipistart, Monogen, and Enfaport (for infants), Portagen (for pediatric), and Vivonex and Tolerex (for adults). Modular additives typically provided in chylothorax are MCT oil, MCT procal, and Liquigen (Fogg et al., 2023).
MCT consists of medium-chain fatty acids (MCFAs) and originated as byproducts of coconut oil production in the 1950s. Despite the classification of MCFAs as saturated fatty acids, their nutritional, physiological, and physicochemical attributes distinguish them from the long-chain saturated fatty acids (Watanabe and Tsujino, 2022). MCTs are present naturally in certain vegetable oils such as coconut and palm kernel oils, as well as in milk fat. The usual composition of typical MCT primarily includes caprylic acid (8:0) and capric acid (10:0) (Yuan et al., 2022).
The diet contains fats in the form of triacylglycerols/triglycerides, which are hydrolyzed by gastric and intestinal lipases into fatty acids. If these triglycerides are from an MCT source, then they break to form MCFAs which directly cross the enteral walls and absorb into the portal vein (bypassing the lymphatic system), from where they go to the liver and prove as an immediate source of fats for the body, this decreases the chyle flow into the thoracic duct and prevents the severity of condition and complications as shown in Figure 4 (Yuan et al., 2022). The energy production process of MCT involves beta oxidation. MCFAs’ carnitine-independent transport and rapid oxidation make them a key energy source in metabolic stress. Rapid oxidation in mitochondria yields acetyl-CoA, which enters the Krebs cycle to generate energy. Moreover, the ketogenic ability of MCT leads to the production of ketone bodies, utilizing excess acetyl-CoA, especially during fasting states (Lee et al., 2022).
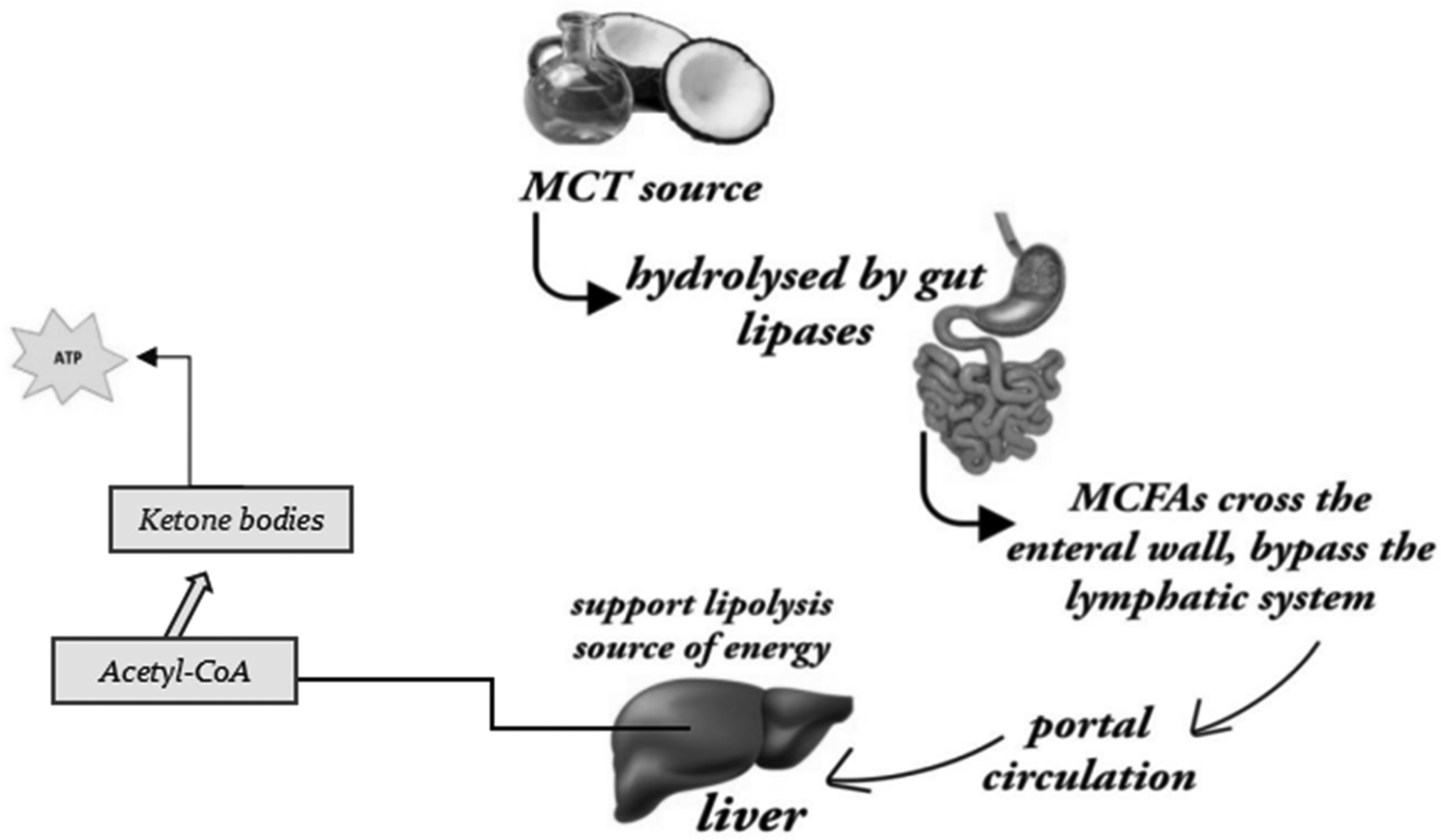
Mechanism of MCTs metabolism
MCTs are introduced during conservative management of chylothorax both through parenteral and oral routes, as they serve to correct the fat deficiency and help to reduce the chyle flow. MCTs are not always potent as an individual treatment, but they ensure the energy needed for the true metabolic functioning of the body and to correct malnutrition. Literature reports that MCT supplementation with enteral nutrition stands out as a more effective strategy than a solely MCT-fed diet (Pan et al., 2016). Furthermore, long-term deprivation of LCTs can lead to a deficiency of essential fatty acids (EFAs) and weakness; therefore, chyle flow needs to be closely monitored to devise long-term treatment plans (Winder et al., 2024). Deficiency of fat-soluble vitamins can be observed in cases of prolonged MCT therapy, particularly in the elderly and females suffering from chronic pancreatitis (Duletzke et al., 2023).
When central venous pressure is not elevated, diets enriched with MCT help reduce lymphatic flow, while avoiding complications associated with parenteral nutrition (Chan et al., 2005). The majority of patients respond positively to enteral MCT provision within the initial weeks. The MCT-based diet is generally continued for up to 4 weeks, not for ongoing treatment but to prevent recurrence of chylothorax after resolution of effusion (Panthongviriyakul and Bines, 2008; Tedjaatmadja and Wulandari, 2024). The optimal timing for reintroducing a regular diet after chest tube removal remains debated; however, a 2–4-week transition period is commonly recommended, particularly in breastfed infants (Al-Sahaf, 2021).
Evidence on MCT efficacy: A temporary treatment regimen in chylothorax
MCTs are administered in chylothorax as part of conservative nutritional therapy through both parental and oral routes. They help correct fat deficiency and reduce chyle flow (Tedjaatmadja and Wulandari, 2024). MCTs supplementation has also been shown to improve nutritional biomarkers in malnourished patients (Watanabe and Tsujino, 2022). In critically ill hospitalized patients, MCTs intake has been associated with improved nitrogen status and reduced protein losses due to increased lipid oxidation (Gura, 2025; Lindgren et al., 2001). This was further supported by elevated serum albumin levels along with optimized nitrogen balance in MCT-fed malnourished rats (Kojima et al., 2008). In certain chylothorax patients, conservative management involving effusion drainage, a low-fat diet, and supplementation with MCT oil is sufficient. However, if fluid loss surpasses 1.5 liters per day for over 5–7 days in adults or >20 ml/kg/day in children, the drainage should be discontinued after a week unless the treatment of an underlying malignancy is expected to resolve a thoracic duct obstruction (Browse et al., 1997; Nakano et al., 2022).
MCT oil is often relatively costly and is typically not covered by insurance when consumed orally. It should be administered in moderation, as excessive intake may lead to diarrhea and gastrointestinal discomfort (Shah and Limketkai, 2017). Generally, in chylothorax treatment, MCT doses ranging from 60–70 g/day (equivalent to 4–5 tablespoons, providing approximately 500–600 calories) distributed throughout the day are well-tolerated (McCray and Parrish, 2004; Duletzke et al., 2023). Individuals adhering to a fat-free diet or relying solely on MCT oil as their fat source for an extended period may require supplementation with EFAs and fat-soluble vitamins (Fogg et al., 2023; McCray, 2004). For idiopathic chylothorax, initiating MCTs as a primary treatment approach for up to 1 week is considered (Epaud et al., 2008). If improvement is evident, the MCT diet can be continued until a cure is achieved. In cases where MCTs prove ineffective, transitioning to TPN and somatostatin for up to 4 weeks is recommended. If improvement occurs, the patient can be shifted back to an MCT diet; otherwise, invasive lymphatic interventions may be considered, followed by the continuation of an MCT diet until the cessation of chyle leakage (Epaud et al., 2008; Perisson et al., 2014).
Newborns and infants who have undergone intricate cardiac surgery face the greatest susceptibility to chylothorax. This risk is elevated, particularly in cases involving secondary chest closure. The efficacy of an MCT-supplemented diet has been proven to be effective in different chylothorax cases in children. A 17-month-old child affected with postoperative chylothorax after esophagitis and stricture surgery was treated with MCT supplementation for 6 months. The results not only led to rapid and reduced clearing of the chylothorax but also resulted in improvement in the child's nutrition and general condition. Lichter et al. (1968) reported total triglyceride content in chyle was 2048 mg/100 ml and 434 mg/100 ml before and after MCT treatment. In a study on postoperative chylothorax in newborns and infants, it was reported that in 71% of these patients, the leakage of chyle was temporary and effectively managed with an MCT-enriched diet devoid of long-chain fatty acids (Biewer et al., 2010). This indicates that resorting to more extended and invasive treatments may not be universally essential; however, there is a lack of consensus on single or optimal chylothorax treatment (Ahmed, 2021; Biewer et al., 2010). When gastrointestinal tract function is permissible, and the daily chest drainage volume remains below 1500 mL, enteral nutrition with MCT should be the preferred initial approach for managing postoperative chylothorax. This approach may also be considered in the context of postoperative chylous ascites (Zheng et al., 2020). A comprehensive description of relevant literature on the efficacy of MCT as a treatment regimen in patients with chylothorax has been presented in Table 1.
Relevant literature on the efficacy of MCT as a treatment regimen in patients with chylothorax.
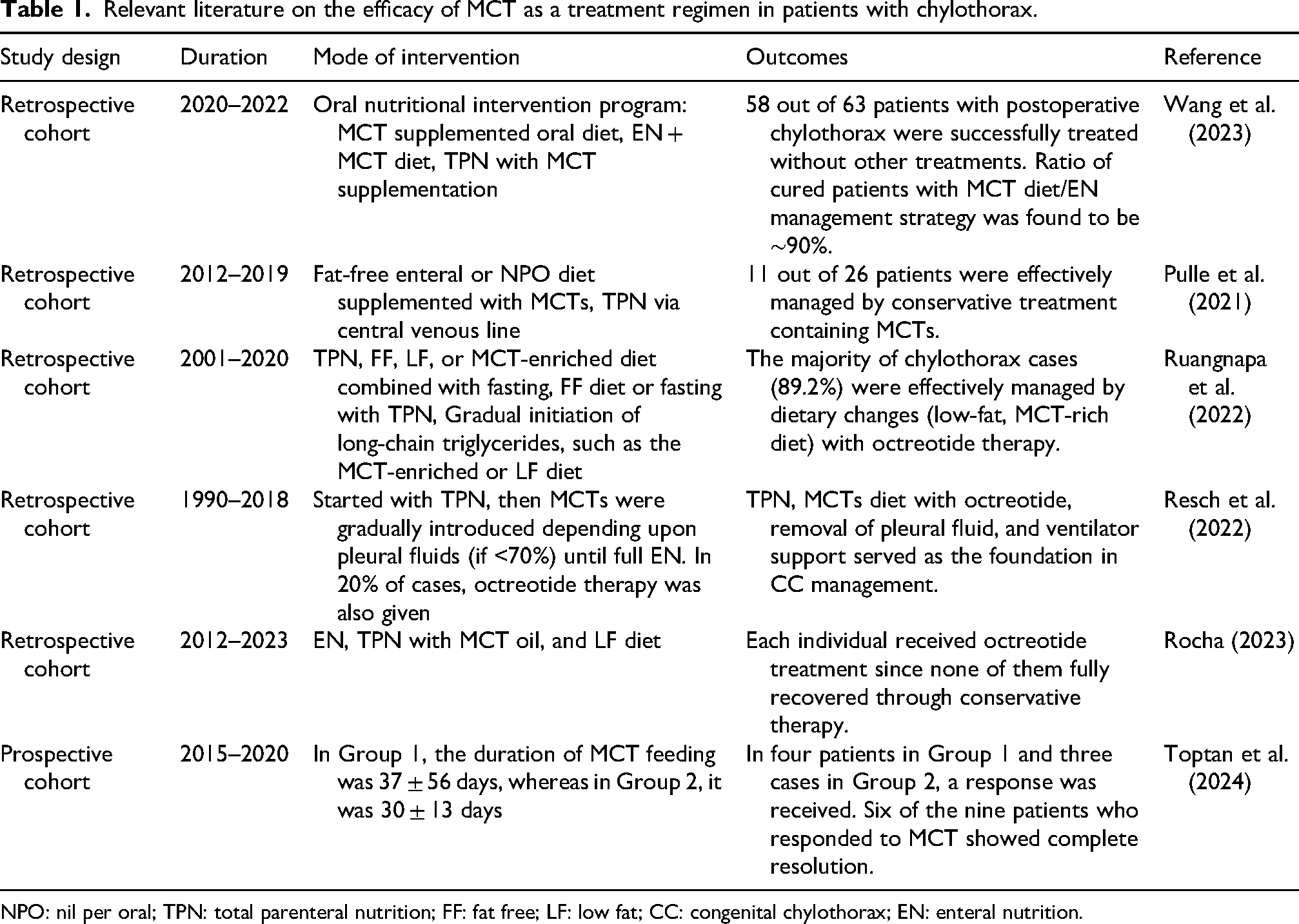
NPO: nil per oral; TPN: total parenteral nutrition; FF: fat free; LF: low fat; CC: congenital chylothorax; EN: enteral nutrition.
The effectiveness of MCT in the management of chylothorax can be evaluated through several clinical and nutritional parameters, including reduction in chyle drainage volume, duration of leakage, improvement in biochemical markers, and overall clinical recovery. Wang et al. (2023) demonstrated that patients receiving an MCT-enriched enteral diet exhibited a significant decline in daily drainage volume and faster resolution of chylous leakage, accompanied by improved serum albumin and total protein levels. Similarly, Pulle et al. (2021) emphasized decreased output and shorter hospital stay as indicators of successful conservative management with MCT-based nutrition. In pediatric and neonatal populations, Ruangnapa et al. (2022) and Rocha (2023) reported that MCT administration reduced the need for surgical interventions and promoted earlier transition to full enteral feeding, while Resch et al. (2022) found that nutritional recovery, weight gain, and shorter duration of pleural drainage were consistent markers of effective therapy. Collectively, these studies highlight that parameters such as decreased chyle output, improved nutritional indices, reduced hospitalization, and avoidance of invasive procedures represent the primary indicators of MCT effectiveness in chylothorax management. The MCT diet represents the least intrusive and most cost-effective choice. However, a unanimous agreement on its application has not been achieved.
Conclusion
Chylothorax treatment cannot be precisely determined due to its varied etiology and uncommon occurrence. The patient's preliminary nutritional status, the cause, and the degree of the chylothorax determine how the patient should be managed. However, the latest researches indicate that MCTs are a valuable but temporary treatment regimen in chylothorax management. They are considered the first-line therapy in the conservative treatment of chylothorax but are effective with other treatment strategies, including TPN, a fat-free or low-fat diet, and octreotide therapy. This means overall, a multidisciplinary approach is needed in chylothorax, which includes medication therapy, dietary changes, pleural fluid drainage, and, in rare cases, surgery. Further researches are needed on its efficacy and mechanism in reducing chyle flow and improving the chylothorax condition.
Footnotes
Ethics statement
Ethics approval was not requested as no individual patient data were included.
Authors’ contributions
Sobia Nasir: conceptualization, methodology, writing–original draft, and writing–review and editing. Javeria Siddique: conceptualization, methodology, writing–original draft, and writing–review and editing. Zaheer Ahmed: conceptualization, supervision, and writing–review and editing. Saba Liaqat: formal analysis, software, and writing–review and editing. Ifra Ferheen: formal analysis and writing–review and editing. Muhammad Usama Umer: formal analysis, software, and writing–review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
No data are available to share.