
Abstract
Background
Rheumatoid arthritis (RA) is a chronic autoimmune disease causing joint damage and disability. Vitamin D (VD) shows immunomodulatory effects in RA, but its causal role and potential mediation by sex hormones remain unclear.
Objectives
To examine the VD-RA causal relationship and investigate androgen/estrogen mediation using Mendelian randomization (MR).
Methods
We conducted two-sample MR analyses using UK Biobank and IEU OpenGWAS data, with genetic variants as instruments. Mediation analyses assessed sex hormone effects.
Results
Dietary VD associated with reduced RA risk (odds ratio (OR) = 0.994, 95%CI 0.992–0.996). Protective effects were stronger in males with seropositive RA (OR = 0.97, 95%CI 0.96–0.99) and females with seronegative RA (OR = 0.99, 95%CI 0.98–0.99). VD significantly lowered female testosterone (OR = 0.54, 95%CI 0.42–0.66), a RA risk factor (OR = 1.03, 95%CI 1.01–1.04), but did not affect male testosterone or female estrogen levels.
Conclusion
VD may reduce RA risk via gender-specific mechanisms, particularly by decreasing female testosterone. While MR supports causality, potential confounding requires cautious interpretation.
Introduction
Rheumatoid arthritis (RA) is a chronic, progressive autoimmune disease characterized by symmetrical joint inflammation, leading to joint destruction and functional impairment (Di Matteo et al., 2023; Smolen et al., 2016). It is associated with progressive disability, premature mortality, and significant socio-economic burden (Aletaha and Smolen, 2018). The pathogenesis of RA is multifactorial, involving genetic predispositions (e.g. HLA-DRB1), environmental triggers (e.g. smoking, viral infections), and lifestyle factors (e.g. diet), which contribute to the production of autoantibodies such as rheumatoid factor and anti-citrullinated peptide antibodies. These autoantibodies drive immune dysregulation, particularly through the abnormal activation of T cells, resulting in chronic inflammation and joint damage (Di Matteo et al., 2023). Despite advances in understanding RA, its complex etiology remains incompletely elucidated, limiting the development of effective therapies.
Vitamin D (VD), a fat-soluble vitamin essential for bone health, has recently emerged as a potential immunomodulator in RA. Beyond its classical role, the active form of VD exhibits anti-inflammatory and immunoregulatory properties, which may mitigate RA progression (Jeffery et al., 2016). Mechanistically, VD suppresses the PKC δ/ERK pathway, inhibiting Th1 cell activation while promoting Th2 differentiation. It also modulates Th17 cell development and enhances regulatory T cell (Treg) function, thereby restoring immune balance (He et al., 2016; Ishikawa et al., 2017). Furthermore, VD regulates dendritic cell maturation, reduces pro-inflammatory cytokines (e.g. TNF-α, IL-6), and increases anti-inflammatory mediators (e.g. IL-10), creating a microenvironment conducive to resolving inflammation (Cutolo et al., 2007; Ishikawa et al., 2017). These mechanisms suggest that VD may play a pivotal role in controlling immune dysregulation and joint inflammation in RA.
Clinically, VD deficiency is prevalent among RA patients and correlates with higher disease activity, greater disability, and reduced quality of life (Al-Saoodi et al., 2024; Vojinovic et al., 2017). However, the therapeutic and preventive potential of VD remains controversial. Genetic studies indicate that higher VD levels and increased expression of VD metabolic genes are associated with a reduced risk of autoimmune diseases, including RA (Vanderlinden et al., 2022). Conversely, Mendelian randomization (MR) studies suggest that low VD levels in RA patients may be a consequence rather than a cause of the disease (Viatte et al., 2014). Clinical trials have yielded mixed results, with some demonstrating improvements in RA symptoms following VD supplementation (Cutolo et al., 2007), while others report no significant association between VD intake and RA risk or disease activity (Costenbader et al., 2008). Notably, the incidence of RA is two–three times higher in women over 40 than in men, implicating sex hormones as potential mediators in the VD-RA relationship (Al-Saoodi et al., 2024).
The inconsistent findings on VD and RA may stem from confounding factors, measurement errors, limited sample sizes, geographical variations, and reverse causality in observational studies. To address these limitations, this study employs a two-sample MR approach, leveraging genetic variants as instrumental variables (IVs) to minimize confounding and establish causal inference. By integrating data from the UK Biobank and IEU OpenGWAS databases, we aim to clarify the causal relationship between VD and RA and explore the mediating role of sex hormones. This study not only advances our understanding of the relationship between VD and RA but also provides a scientific foundation for developing targeted prevention and treatment strategies for RA.
Methods
Study design
We employed a two-sample MR approach to investigate unidirectional causal pathways between VD and RA, with testosterone and estrogen analyzed as potential mediators. Data were primarily sourced from the UK Biobank (UKB), a large-scale, non-overlapping database. VD was considered as the exposure, with two markers analyzed: dietary VD intake and blood VD levels. For RA, we included general RA cases as well as seropositive (M05RA) and seronegative (M06RA) subtypes. To ensure robust MR results, IVs were selected based on three key assumptions: (1) strong association with the exposure; (2) independence from confounders affecting both exposure and outcome; and (3) influence on the outcome solely through the exposure (Burgess et al., 2015). The study followed the Strengthening the Reporting of Observational Studies in Epidemiology Using Mendelian Randomization (STROBE-MR) guidelines and involved genetic IV selection, pleiotropy assessment, and heterogeneity and sensitivity analyses (Skrivankova et al., 2021). A bidirectional MR design is illustrated in Figure 1.
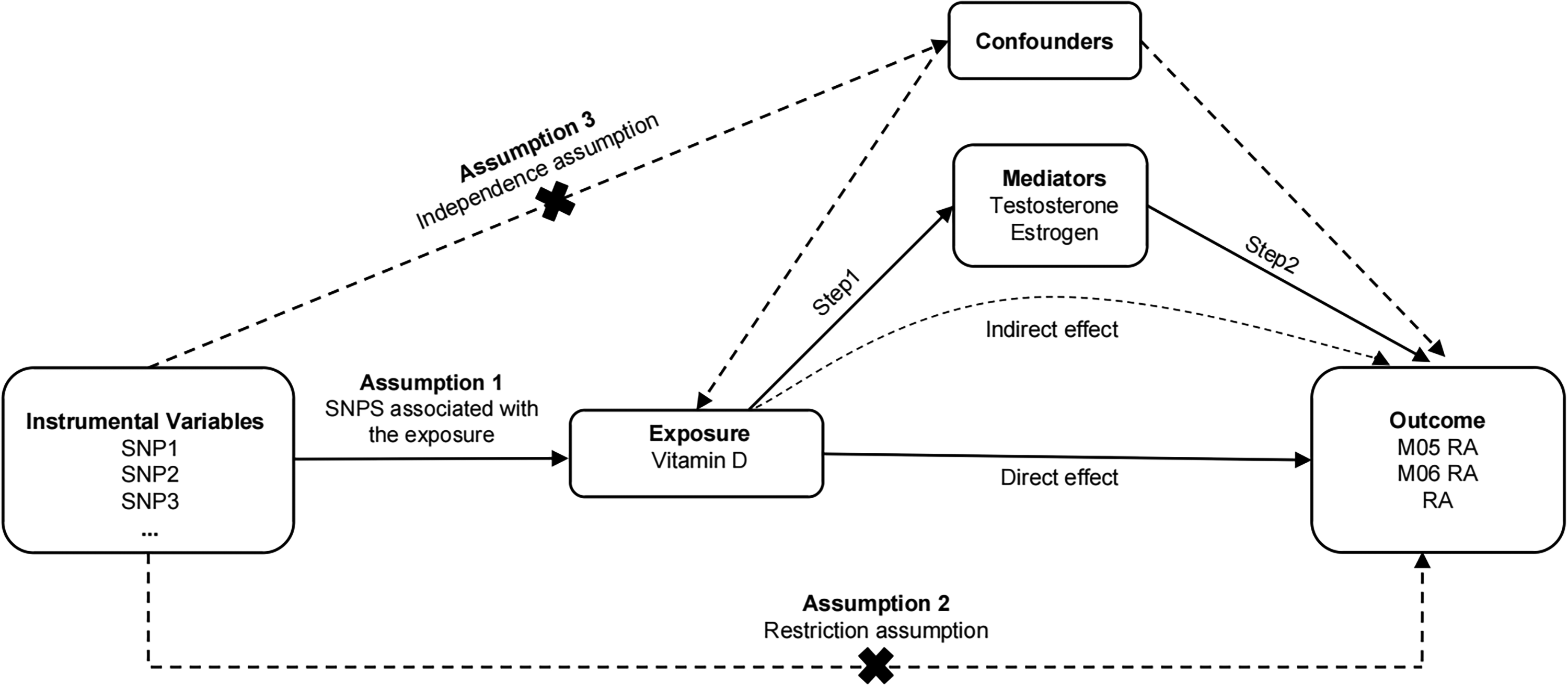
MR analysis of the effect of VD on RA and the mediating role of sex hormones. The mediation effect is assessed using a two-step MR framework. Step 1 estimated the causal effect of the exposure on the sex hormone mediators, and step 2 assessed the causal effect of the mediators on RA risk. RA: rheumatoid arthritisl VD: vitamin D; MR: Mendelian randomization.
GWAS data sources
Summary statistics for VD were obtained from two datasets: dietary VD intake (n = 1,436,758) and blood VD levels (n = 465,082), both from the UK Biobank. RA data (n = 1,268,194) were also sourced from the UK Biobank. Hormone-related data (testosterone and estrogen) were extracted from the IEU OpenGWAS project and the UK Biobank. Detailed information on data sources, sample sizes, and instrument strength is provided in the Supplementary material Tables S1 and S2. Ethical approval and informed consent were obtained for all original studies within the GWAS datasets.
Selection of genetic instruments
For each exposure, genome-wide significant SNPs (p < 5 × 10−6) were selected as IVs. To ensure independence, SNPs were clumped at r2 < 0.001 and F > 10, with a linkage disequilibrium threshold of 10,000 kb. This approach minimized multicollinearity and ensured the reliability of the MR analysis. The final list of SNPs used as IVs is provided in the Supplementary material Table S2.
Statistical analysis
The primary analysis used random effects inverse variance weighted (IVW) regression to combine Wald ratios from multiple SNPs. Effect sizes were reported as odds ratios (ORs) for binary outcomes and standardized beta coefficients (β) for continuous outcomes. Sensitivity analyses included MR-Egger, weighted median, weighted mode, and MR-PRESSO to address potential pleiotropy and violations of MR assumptions. Heterogeneity was assessed using Cochran's Q test, and I2 statistics were calculated to quantify its extent (I2 < 25%: mild; 25–75%: moderate; >75%: severe). All MR analyses were conducted in R (version 4.2.1) using the TwoSampleMR package. Meta-analyses were performed in STATA (version 12.0) using random effects models, with forest plots generated to visualize pooled ORs. Only outcomes with data from at least two non-overlapping studies were included in the meta-analysis. Notably, the analytical approach of this study exhibits enhanced comprehensiveness compared to previous studies, addressing key limitations of existing methods: 1) We adopted an integrated framework of “two-sample MR + mediation effect analysis”. Unlike prior studies that only verified the direct association between VD and RA, this study further dissected the mediating pathway of sex hormones, comprehensively revealing the “exposure-mediator-outcome” causal chain. 2) Multiple MR models (IVW, MR-Egger, weighted median, and weighted mode) were combined with heterogeneity and sensitivity analyses (MR-PRESSO). This approach overcomes the limitation that traditional single MR models are susceptible to pleiotropy and confounding, thereby improving the reliability and robustness of causal inference.
Results and discussion
Causal relationship between vitamin D and rheumatoid arthritis
A meta-analysis of 173 MR datasets showed that dietary VD intake significantly reduces the risk of RA, with an overall OR of 0.994 (95% CI: 0.992–0.996, I2 = 35.8%). Gende-stratified analyses revealed stronger protective effects in specific subgroups: males with M06RA (OR = 0.97, 95% CI: 0.96–0.99, I2 = 20%) and females with M05RA (OR = 0.99, 95% CI: 0.98–0.99, I2 = 54.4%). Additionally, analysis of 22 MR datasets on blood VD levels indicated a modest reduction in RA risk among females (OR = 0.998, 95% CI: 0.996–0.999, I2 = 32%) (Figure 2), while no statistically significant associations were observed in other subgroups (Supplementary material Table S3). Individual MR analyses corroborated these findings, confirming that VD intake is associated with a reduced incidence of RA (Table 1).
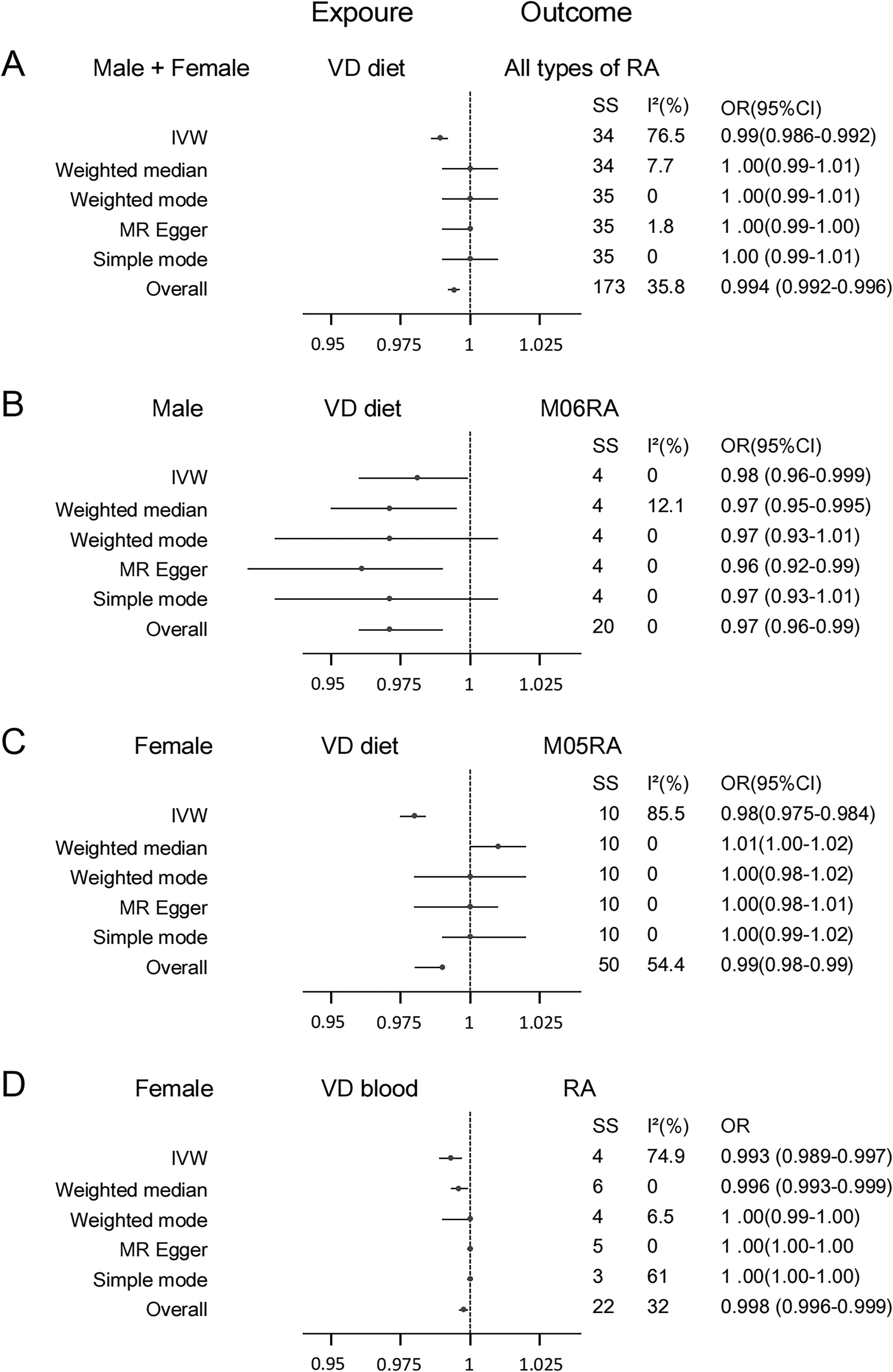
Summary MR estimates derived from the IVW, weighted median, weighted mode, MR-Egger and simple mode methods for the effect of VD on RA. A) VD diet and all types of RA. B) Male VD diet on M06 RA. C) Female VD diet on M05 RA. D) Female VD levels in blood on unspecified RA. SS: sample size; RA: rheumatoid arthritis; VD: vitamin D; MR: Mendelian randomization; IVW: inverse variance weighted.
Positive causal relationship between Vitamin D and RA through De Novo Mendelian randomization.
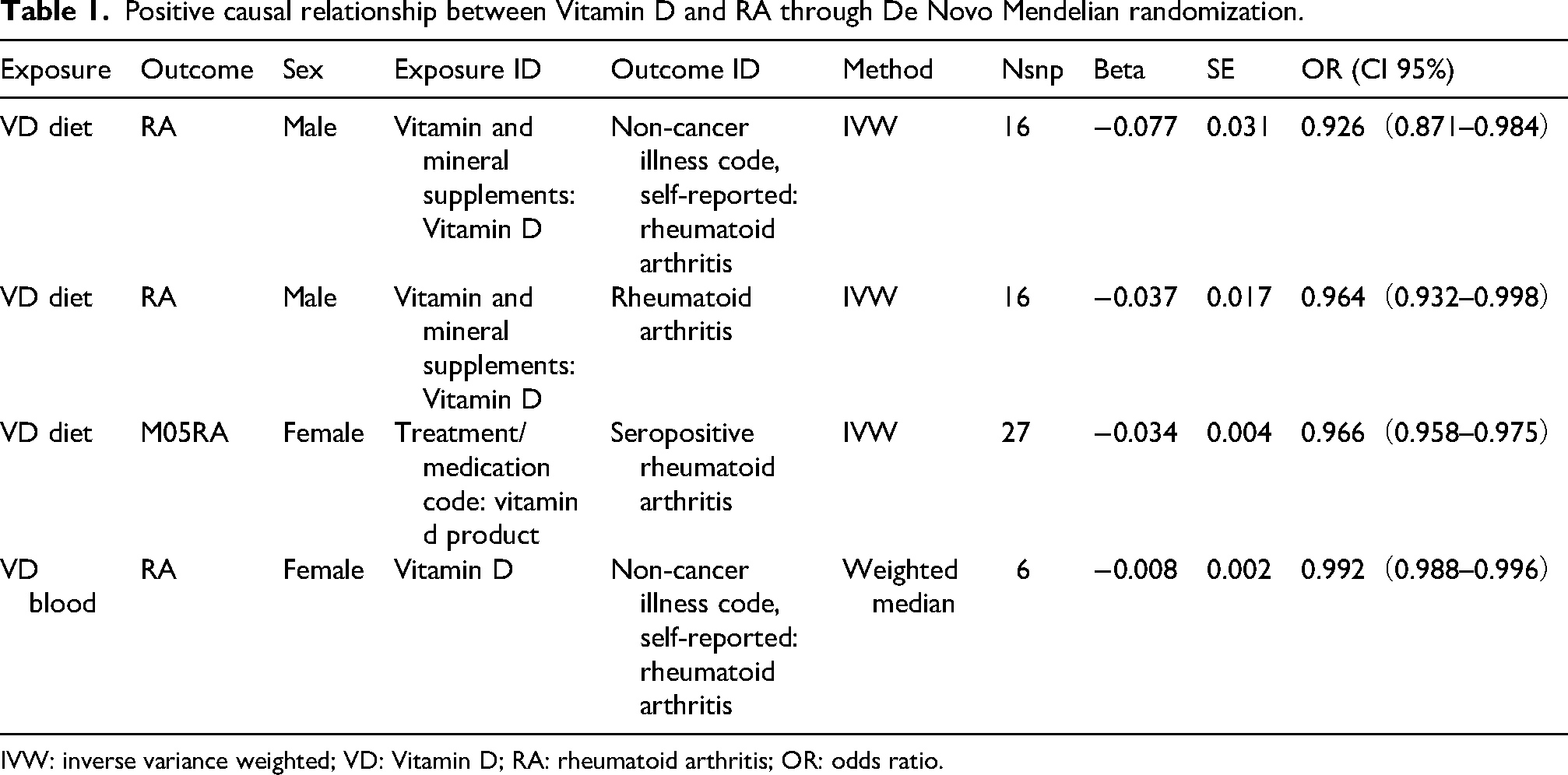
IVW: inverse variance weighted; VD: Vitamin D; RA: rheumatoid arthritis; OR: odds ratio.
RA is a classic autoimmune disease characterized by symmetrical joint inflammation, and its pathogenesis is often linked to low circulating VD levels (Murdaca et al., 2019). Preclinical studies support VD's protective role: in animal models, VD suppresses RA-related inflammation by reducing anti-type II collagen antibodies (Moghaddami et al., 2012; Tsuji et al., 1994; Zhou et al., 2019); in vitro studies demonstrate its ability to inhibit pro-inflammatory cytokines (e.g. TNF-α, IL-1α, IL-1β, IL-6) and osteoclast activation in RA macrophages (Neve et al., 2014). Additionally, VD downregulates aromatase expression in macrophages (Villaggio et al., 2012), mitigating local estrogen-driven synovial proliferation (Capellino et al., 2008; Cutolo et al., 2012). These mechanisms collectively highlight VD's potential in modulating RA pathogenesis.
Our MR findings provide genetic evidence supporting VD's protective role in RA, consistent with prior studies linking higher VD metabolic gene expression and circulating VD levels to reduced autoimmune disease risk (Vanderlinden et al., 2022). However, the protective effects of VD exhibit population heterogeneity, with stronger benefits in male M06RA and female M05RA subgroups. While large cohort studies have reported no significant association between dietary VD intake and RA risk in women (Costenbader et al., 2008), our results suggest that maintaining high serum VD levels—rather than dietary intake alone—may be critical for immune-modulatory effects, underscoring the importance of considering VD bioavailability and metabolic variability in supplementation strategies.
Mediating role of sex hormones in the VD-RA pathway
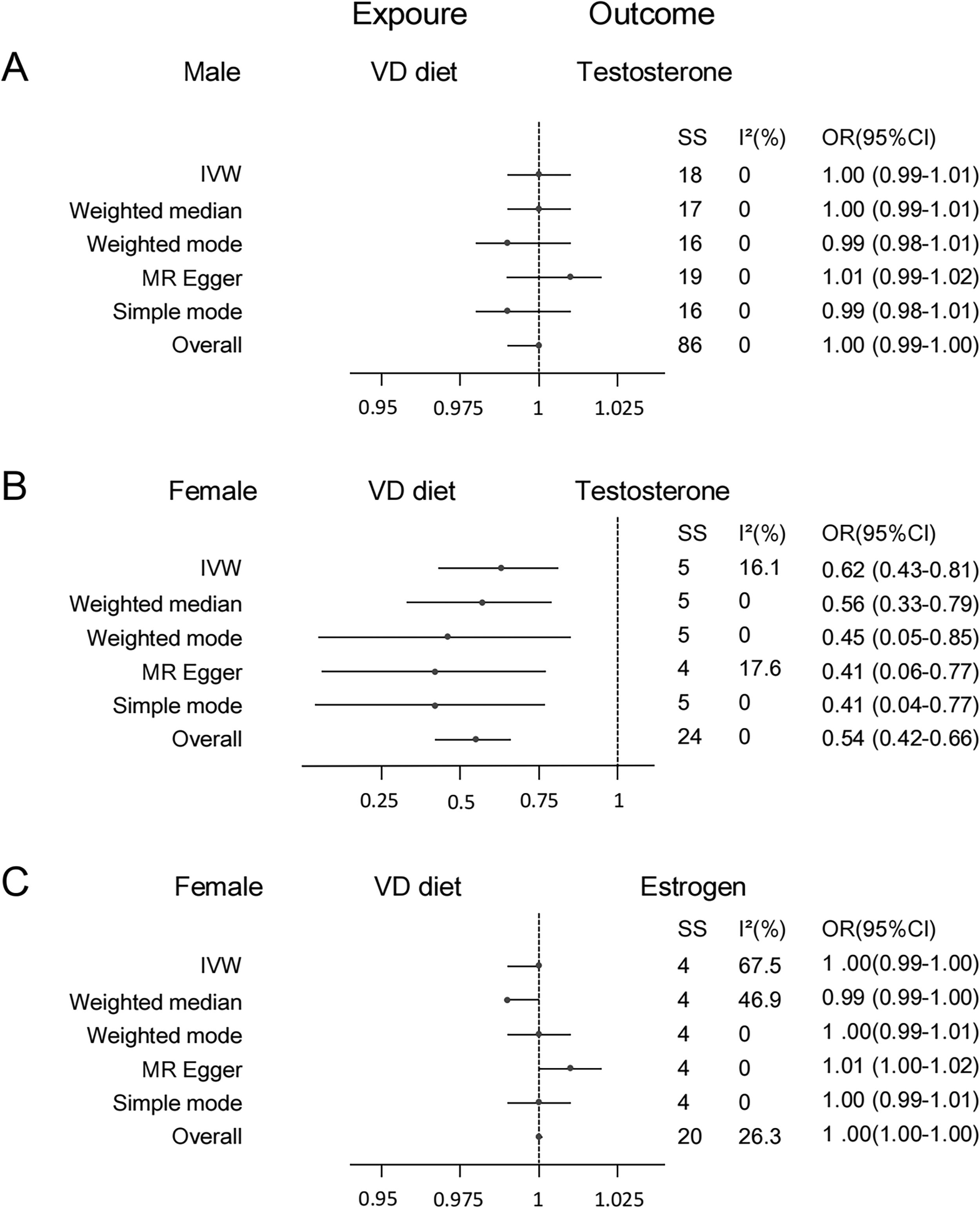
Summary MR estimates the effect of VD on sex hormone. A) VD diet on testosterone levels. B) Female VD diet on testosterone. C) Female VD diet on estrogen. VD: vitamin D; MR: Mendelian randomization.
Positive causal relationship between Vitamin D, and RA through De Novo Mendelian randomization.
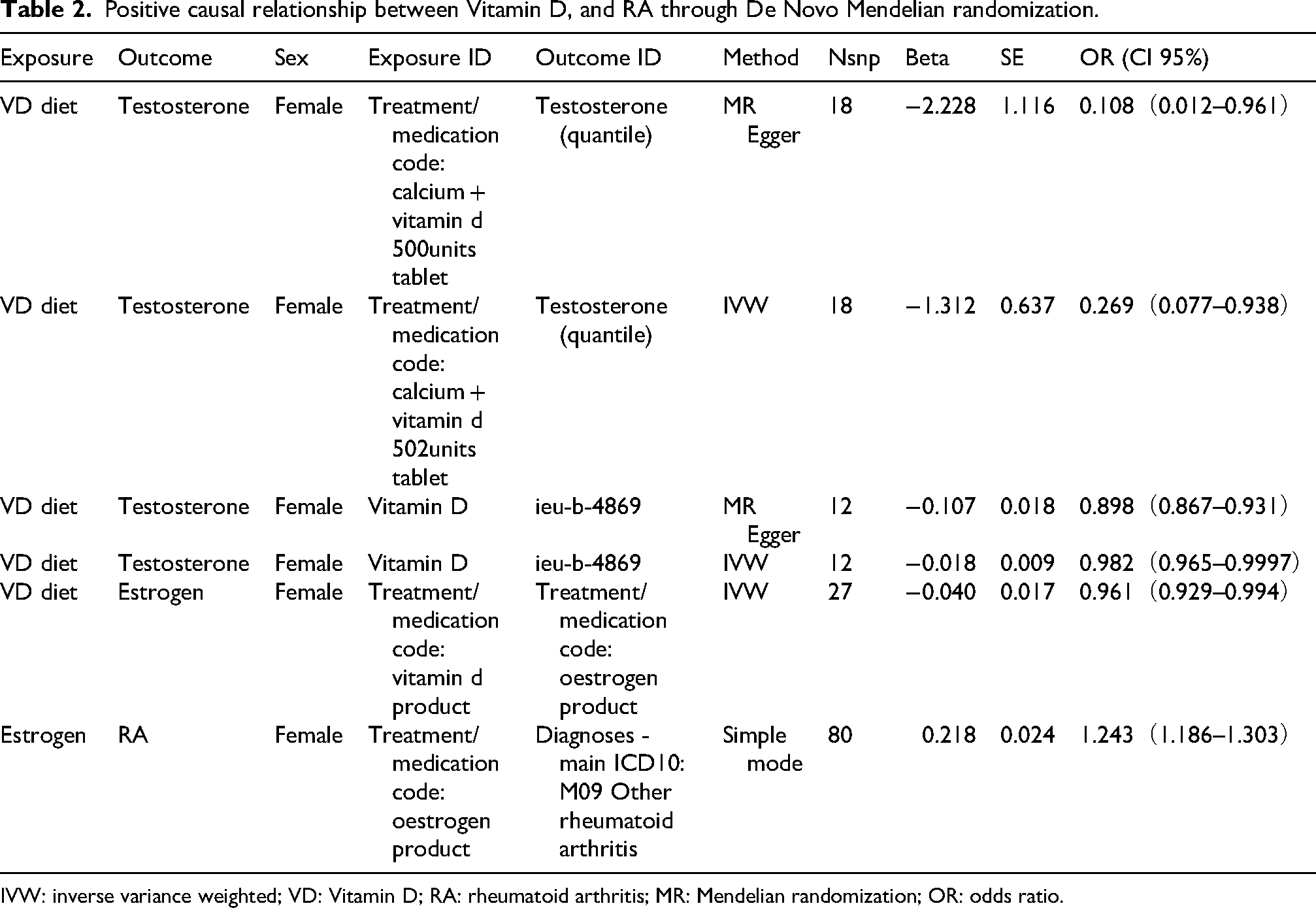
IVW: inverse variance weighted; VD: Vitamin D; RA: rheumatoid arthritis; MR: Mendelian randomization; OR: odds ratio.
VD's interaction with sex hormones displays gender-specific patterns. Cross-sectional and randomized controlled trials have consistently shown no significant association between VD and androgen levels in males (Chen et al., 2019; Ksiazek et al., 2021), aligning with our findings. In terms of estrogen, a cohort study involving 616 postmenopausal women in China found a positive correlation between serum 25(OH)D and estradiol (Huang et al., 2019). Although our study did not observe a significant association between estrogen and VD, MR-Egger analyses suggested a trend toward increased estrogen levels with VD intake, potentially limited by data availability.
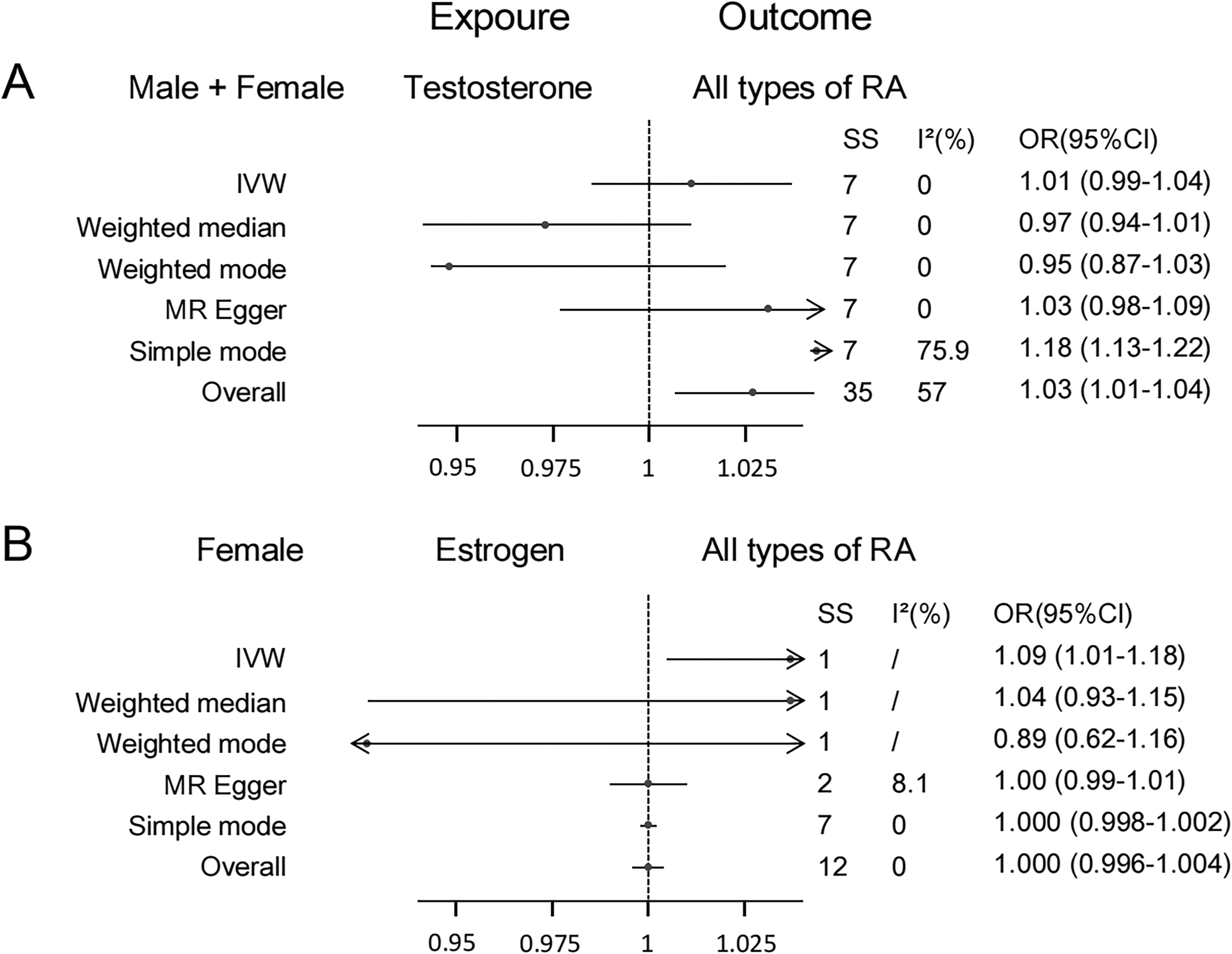
Summary MR estimates the effect of sex hormone on RA. A) Among all groups of people,testosterone on RA. B) Female estrogen on RA. RA: rheumatoid arthritis; MR: Mendelian randomization.
Sex hormones exert divergent effects on RA pathogenesis. Androgens traditionally exhibit anti-inflammatory properties by inhibiting NF-κB signaling and pro-inflammatory cytokine secretion (Gubbels and Jorgensen, 2018; Trigunaite et al., 2015) while estrogen's effects are concentration-dependent: high levels (>300 pmol/L) promote anti-inflammatory Treg differentiation via ERα activation, whereas low levels (<100 pmol/L) drive pro-inflammatory Th17 polarization (Straub, 2007). Our pooled analysis of androgen data revealed a positive association with RA risk, albeit with high heterogeneity. This contradictory finding may stem from methodological limitations: (1) Gender-mixed analyses introduced confounding bias, as female androgen levels are 5–10% of male levels and are metabolically dominated by estrogen; (2) The biological differences between androgen subtypes (e.g. free testosterone vs. sex hormone-binding globulin-bound testosterone) were not accounted for.
Regarding estrogen, our study found no significant association with VD, likely due to the inclusion of both premenopausal and postmenopausal women without stratification. The >10-fold difference in estrogen levels between these groups may have diluted the observed effects.
Advantages
This study offers several methodological strengths. First, by employing a MR design with genetic variants as IVs, we minimized confounding and reverse causality, establishing a robust causal link between VD and RA while systematically exploring the mediating role of sex hormones—a novel contribution to the field. Second, to enhance internal validity, the study population was restricted to individuals of European ancestry. This choice was primarily driven by two critical considerations: genetic background homogeneity of European populations effectively mitigates population stratification bias, a key prerequisite for reliable MR causal inference; additionally, European ancestry cohorts (e.g. UK Biobank and IEU OpenGWAS) provide the most comprehensive, standardized GWAS summary data covering VD, sex hormones, and RA phenotypes, which are currently unavailable for non-European populations at sufficient sample sizes and phenotypic precision. Third, we integrated quality data from UK Biobank and IEU OpenGWAS project, to construct a two-sample MR framework. Combined with meta-analysis, this approach provided a comprehensive evaluation of the causal relationship between VD and RA, including gender-specific effects.
Limitations
Several limitations should be acknowledged. First, as a meta-analysis of summary-level data, this study lacked access to individual patient data, precluding detailed patient-level analyses. Second, while MR can establish causality, it is limited to assessing preventive effects and cannot evaluate the therapeutic efficacy of VD in RA. Third, the restriction to European populations may limit the generalizability of our findings to other ethnic groups. Fourth, despite the advantages of MR over traditional meta-analyses, it remains model-dependent and relies heavily on underlying assumptions. Additional limitations include the Mendelian database's limited characterization of dietary VD, potential confounding from gender-mixed analyses, and heterogeneity due to age stratification.
Conclusion
This study identifies gender- and subtype-specific effects of VD on RA risk: Dietary VD intake reduces RA incidence, particularly in males with M06RA and females with M05RA, while maintaining elevated blood VD levels—rather than dietary intake alone—emerges as a critical protective factor. Notably, dietary VD selectively lowers androgen levels in females, which is independently associated with increased RA risk, revealing a novel hormone-mediated pathway in RA pathogenesis.
These findings advance our understanding of VD's immunomodulatory role by highlighting its sex-specific interaction with endocrine pathways, offering insights for gender-tailored prevention strategies. However, limitations including oversimplified characterization of dietary VD in Mendelian databases, age-stratified confounding, and mixed-sex hormone analyses necessitate cautious interpretation. Future research should prioritize large-scale randomized trials to validate the causal VD-RA relationship mediated by sex hormones, delineate optimal VD supplementation thresholds for RA prevention and explore mechanisms underlying sex-specific VD effects on immune-endocrine crosstalk. Such efforts could revolutionize precision prevention paradigms for high-risk populations.
Supplemental Material
sj-docx-1-nah-10.1177_02601060261425460 - Supplemental material for Vitamin D and rheumatoid arthritis in European populations: Unraveling causal links and the mediating role of sex hormones via Mendelian randomization
Supplemental material, sj-docx-1-nah-10.1177_02601060261425460 for Vitamin D and rheumatoid arthritis in European populations: Unraveling causal links and the mediating role of sex hormones via Mendelian randomization by Mingdong Liu, Junwei Yan, Hongran Lv, Xiaopeng Yang, Yiying Yao and Zheng Liu in Nutrition and Health
Supplemental Material
sj-docx-2-nah-10.1177_02601060261425460 - Supplemental material for Vitamin D and rheumatoid arthritis in European populations: Unraveling causal links and the mediating role of sex hormones via Mendelian randomization
Supplemental material, sj-docx-2-nah-10.1177_02601060261425460 for Vitamin D and rheumatoid arthritis in European populations: Unraveling causal links and the mediating role of sex hormones via Mendelian randomization by Mingdong Liu, Junwei Yan, Hongran Lv, Xiaopeng Yang, Yiying Yao and Zheng Liu in Nutrition and Health
Footnotes
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors have agreed to publish this article.
CRediT authorship contribution statement
Conceptualization, ML, ZL and JY; methodology, HL and JY; software, XY; validation, HL and XY; formal analysis, XY and JY; investigation, XY, YY; resources, JY, HL; data curation, XY, YY JY and HL; writing—original draft preparation, JY; writing—review and editing, ML, ZL and JY; visualization, XY, ML and JY; supervision, ZL; funding acquisition, ZL. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Zheng Liu, (grant number Shaoxing University enterprise important horizonta).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of generative AI and AI-assisted technologies in the writing process
During the preparation of this work the author(s) used DeepSeek and Kimi in order to improve language and readability. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Data availability
No data were used for the research described in this article.
Supplemental material
Supplemental material for this article is available online.