
Abstract
Background
To date, the mechanisms that underlie the relationship between the onset of anxiety/depression symptoms and the risk of developing psychotic experiences (PEs) remain poorly understood. This study aimed to examine the direct and indirect effects of depression and anxiety on PEs through the mediating role of caffeine addiction symptoms.
Method
In total, 1447 young adults from the general population of Tunisia, aged 18–35 years, enrolled in this cross-sectional study and filled an online survey. A mixed convenience and snowball sampling technique was used to collect data.
Results
Caffeine addiction symptoms partially mediated the associations between depression and PEs and between anxiety and PEs. Depression and anxiety scores were associated with higher caffeine addiction symptoms (Beta = 0.37; p < 0.001 and Beta = 0.38; p < 0.001, respectively). In turn, caffeine addiction symptoms were associated with higher PEs (Beta = 0.29; p < 0.001 and Beta = 0.30; p < 0.001, respectively). Depression and anxiety scores were directly associated with PEs (Beta = 0.36; p < 0.001 and Beta = 0.32; p < 0.001, respectively). The R2 values of both models showed that 29.0% and 26.7% of the variance in PEs is accounted for by caffeine addiction symptoms, respectively.
Conclusion
Young people presenting with depression and anxiety symptoms should be carefully assessed for caffeine intake in clinical practice, educated regarding the known health risks associated with this substance, and advised to limit excessive caffeine intake, which can, in turn, help prevent the occurrence of PEs.
Introduction
It is now well-established that the symptoms of schizophrenia occur along a continuum of severity, suggesting that any person within the general population can experience, at least to some degree, mild psychotic symptoms, such as experiencing paranoid thoughts or hearing voices, and yet never develop a psychotic disorder (Linscott and van Os, 2010). These phenomena are called psychotic experiences (PEs).
There is a growing and compelling body of evidence derived from both non-clinical and clinical samples to indicate that preceding depression and anxiety can induce the emergence or progression of PEs. For instance, based on data from 18 countries and 31,261 adults, McGrath et al. (2016) found that baseline major depression and anxiety disorders were associated with respectively 2.5 and up to 2.8-fold higher odds for subsequent development of de novo PEs. A longitudinal birth cohort study found that children and adolescents with persistent high levels of anxiety were at increased risk for developing both PEs (odds ratio 2.02) at early adulthood (Morales-Muñoz et al., 2022). Researchers argued that depression enhances the sense of vulnerability and anxiety produces anticipation of threat, consequently leading to greater risk for psychotic symptoms (Freeman et al., 2012).
To date, however, the mechanisms that underlie the relationship between the onset of anxiety/depression symptoms and the risk of developing PEs remain poorly understood. This highlights the critical need to better identify the moderator and mediating variables involved in the pathways linking depression and anxiety to PEs. This study focuses on caffeine addiction symptoms as a possible mediator.
The pathways from depression and anxiety to caffeine addiction symptoms
It is increasingly established that caffeine is able to induce dependence as evidenced by the development of difficulty cutting down or quitting, withdrawal and tolerance (Uddin et al., 2017). Thus, caffeine use disorder was recognized by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) as a condition for further study (American Psychiatric Association, 2013), with diagnosis criteria significantly overlapping with other substance use disorders. Notably, caffeine consumption exists on a continuum of addiction within the general population, ranging from no symptoms of addiction to addictive disorder (Freimuth, 2008).
Research has shown that people who are anxious or depressed will increase their caffeine consumption. In these cases, caffeine use can be driven by coping purposes (Ratliff-Crain and Baum, 1990). For instance, Jacobsen and Hansen (1988) showed that women who experienced depression and had trouble finding alternative coping strategies were more prone to consume higher amounts of caffeine. Other authors mentioned the self-medication hypothesis as a plausible explanation of correlations between psychological distress and caffeine use (e.g., (Khantzian, 1997)). A study found that anxiety and depression correlated positively with total weekly caffeine intake in a large cohort of secondary school children from the South West of England (Richards and Smith, 2015); Using caffeine as “an attempt to self-medicate, with the intention of obtaining relief from symptomatology” in individuals with mental health problems was also reported by other researchers (Chelben et al., 2008). In support of this speculation, Whalen et al. (2008) used an Ecological Momentary Assessment and showed that treatment-naive youth with major depressive disorder reported significantly more caffeine consumption relative to healthy youth, and experienced a four-fold decrease in their consumption across treatment (consisting of Selective Serotonin Reuptake Inhibitors and/or Cognitive Behavioral Therapy, or both). Authors suggested that caffeine was used as “an affect regulator” to help treat symptoms of depression, much as other stimulants (like cigaretes) are used (Whalen et al., 2008).
The pathways from caffeine addiction symptoms to PEs
There is accumulating evidence to indicate that caffeine intake can cause an increased proneness to PEs in non-clinical samples (Crowe et al., 2011; Jones and Fernyhough, 2009). A few decades ago, researchers have begun to observe that individuals who ingest large amounts of caffeine present psychosis-like symptoms (Kruger, 1996). Since then, multiple case reports have suggested that ingesting large quantities of caffeine can either aggravate a preceding psychotic illness (Cerimele et al., 2010; Peng et al., 2014; Tibrewal and Dhillon, 2011; Vainer and Chouinard, 1994) or precipitate the emergence of psychotic symptomatology in individuals with no history of psychiatric illness (Adeleye et al., 2023; Goiney et al., 2012; Hearn et al., 2020; Hernandez-Huerta et al., 2017b; Kelsey et al., 2019; Mannix et al., 2024; Valdivieso-Jiménez, 2022). The published cases varied in the consumed amounts of caffeine and the duration of consumption (from a few days to several years), suggesting individual differences in the underlying predisposition to develop caffeine-related psychosis (Elhag and Auf, 2021). A literature review encompassing 43 studies showed that the higher the caffeine consumption, the greater the likelihood of developing psychotic symptoms/episodes and chronic psychosis (Ganhao et al., 2021).
An explanation of how consuming large quantities of caffeine may be responsible for the onset or exacerbation of psychotic symptoms and experiences is by means of its dopamine agonist properties (Ribeiro and Sebastião, 2010). Indeed, caffeine is different from classical substances of misuse in leading to the release of dopamine in the prefrontal cortex rather than the nucleus accumbens (Winston et al., 2005). Caffeine consumption effects might therefore be conceptualized via a stress-diathesis model, whereby the occurrence of PEs might be triggered by a super-sensitization of an already vulnerable system (Mikkelsen, 1979). The capacity of caffeine to produce distinctive impacts in different individuals can therefore be related to genetic predispositions, especially since some genetic factors seem to play a role in predisposing people to both heavy caffeine use and dependence and the risk for psychiatric disorders (Kendler et al., 2006).
To summarize the above, there is a known association of high levels of anxiety and depression with PEs, and large amounts of caffeine intake were shown to relate to psychosis proneness in non-clinical individuals. Therefore, caffeine addiction symptoms could possibly shed some light on the connection between depression/anxiety and the emergence of PEs.
Rationale and aim of the present study
Our study contributes to the literature by examining the direct and indirect effects of depression and anxiety on PEs through the mediating role of caffeine addiction symptoms among Tunisian young adults aged 18–35 years from the general population of Tunisia. This age range was chosen as the at-risk for psychosis population predominantly belongs to this age range (Di Luzio et al., 2022). Over the past years, Tunisia has faced a series of profound challenges, including social, political and economic crises, that has impacted the population's mental health (Fekih-Romdhane et al., 2020b). Research has documented prevalence rates of severe or extremely severe levels of depression and anxiety of 28.3% and 24.4%, respectively (Fekih-Romdhane and Cheour, 2021). A Tunisian study observed that 51.4% of Tunisian young adults had at least one positive PLE “nearly-always” (Fekih-Romdhane et al., 2020a). In addition, comparative research showed that significantly more Tunisians consume coffee daily compared to people from other nations (Adamov et al., 2023). These data emphasize the importance of conducting the present study. It is anticipated that individuals who have high levels of self-reported depression and anxiety, and who tend to be addicted to caffeine consumption would be more likely to report PEs.
Methods
Ethics approval for this study was obtained from the ethics committee of the School of Pharmacy at the Lebanese International University. A cross-sectional study was conducted between May and July 2024. Inclusion criteria consisted of: (1) being a young adult aged between 18 and 35 years, (2) originating from and residing in Lebanon at the time of the survey, and (3) reporting caffeine consumption at least once during the last 12 months. Data were collected from each participant using an online questionnaire. To facilitate broader recruitment of participants, a mixed convenience and snowball sampling technique was used. An initial pool of participants was first recruited through convenience sampling; those readily accessible to the research team through institutional networks and online platforms were invited to take part in the study. Then, the sample was expanded through participant-driven referrals, whereby initial participants were requested to share the link with their own contacts and networks. Participation was voluntary, anonymous and not compensated. The questionnaire link was distributed through various social media platforms, including Instagram, Facebook, Twitter, and WhatsApp. The first section of the questionnaire provided potential participants with the necessary information about the study, and asked them to give an electronic informed consent to participate. The study questionnaire contained the following data and measures.
Minimal sample size calculation
A minimum sample size of 409 was determined to have sufficient statistical power, following the formula suggested by Fritz and MacKinnon (2007) n = L/f2 +k + 1, where f = 0.14 for small effect size, L = 7.85 for an α error=5% and power β = 80%, and k = 7 variables that will be included in the model.
Sociodemographic information
The questionnaire collected sociodemographic data consisting of sex, age, marital status, and educational attainment. Household crowding index (i.e., the number of persons divided by the number of rooms in the house except the kitchen and bathrooms) was calculated, with higher scores reflecting worse socioeconomic status (Melki et al., 2004).
The patient health questionnaire-9
The Patient Health Questionnaire-9 (PHQ-9) was used to evaluate the severity of depression symptoms during the past 15 days via nine items (Kroenke et al., 2001). Items are scored on a four-point Likert-type scale ranging from 0 (not at all) to 3 (nearly every day), with global scores ranging from 0 to 27. Higher scores reflect more severe depression. Scores range from 0 to 27 and can be interpreted as follows: 0–4 (none/minimal), 5–9 (mild), 10–14 (moderate), 15–19 (moderately severe), and 20–27 (severe). The Arabic validated version was adopted (Dagher et al., 2023; Sawaya et al., 2016) (Cronbach's alpha = 0.92).
The generalized anxiety disorder 7-item
The Generalized Anxiety Disorder 7-item (GAD-7) is a self-report scale that contains seven items and assesses the severity of generalized anxiety symptoms during the past 15 days following the DSM-5 criteria (Spitzer et al., 2006). Each item is scored from 0 (Not at all) to 3 (Nearly every day). Total scores range from 0 to 21 and can be interpreted as follows: 0–4 (none/minimal), 5–9 (mild), 10–14 (moderate), > 15 (severe). The Arabic validated version was used (El Khoury-Malhame et al., 2024; Sawaya et al., 2016) (Cronbach's alpha = 0.92).
The caffeine use disorder questionnaire
The Caffeine Use Disorder Questionnaire (CUDQ) is composed of 10 items (e.g., “Did you feel a strong desire or had unsuccessful attempts to reduce or control your caffeine consumption?”) which are designed based on the nine criteria proposed for caffeine use disorder in the DSM-5, combined with a tenth item on distress engendered by caffeine-related symptoms (Ágoston et al., 2018). The CUDQ measures varying levels of caffeine addiction symptoms among non-clinical individuals. Each respondent is asked to rate how often they experienced the symptoms over the past year on a 4-point Likert scale ranging from 1 (Never) to 4 (Very often). The Arabic validated version was used (α = 0.90) (Fekih-Romdhane et al., 2024a).
The prodromal questionnaire-brief
The Prodromal Questionnaire-Brief (PQ-B) is a 21-item self-administered tool. It is the most widely used measure to assess the severity PEs in the general population worldwide (Loewy et al., 2005, 2011). Each item should be rated as yes/no. A “yes” response to an item is followed by an item asking to rate the degree of distress experienced in relation to the statement. A cut-off score of >9 in the frequency scale is indicative of a positive screening for psychosis risk, suggesting a need for a further, more detailed diagnostic interview. The Arabic validated version of the PQ-B was used (Fekih-Romdhane et al., 2024b) (Cronbach α = 0.98).
Statistical analysis
The SPSS software v.25 was used for the statistical analysis. The PQB score was considered normally distributed since the skewness and kurtosis values varied between −1 and +1 (Hair et al., 2022). To know which variables should be included in the mediation model, we conducted a bivariate analysis; the Student t was used to compare a continuous variable and a dichotomous one and the Pearson test to correlate two continuous variables. Structural equation modeling (SEM) was performed to examine the structural relationship between workplace ostracism and workplace interpersonal conflict, taking self-esteem and psychological distress as possible mediators. Multiple indices were calculated to check the fit of the models: the Relative Chi-square (χ2/df; < 5), the Root Mean Square Error of Approximation (close and acceptable fit are considered for values < 0.05 and < 0.11, respectively), the standardized root mean square residual (< 0.05) and the Comparative Fit Index (≥ 0.90) (Byrne, 2013). The R2 values were calculated for each model, with values between 0.02 and 0.13 reflect small effect, whereas values between 0.13–0.26 and ≥ 0.26 indicate medium and large effect, respectively (Cohen, 2013). Covariates were variables that showed a p < 0.25 in the bivariate analysis. We considered the mediation analysis to be significant if the Boot Confidence Interval did not pass through zero. P < 0.05 was deemed statistically significant.
Results
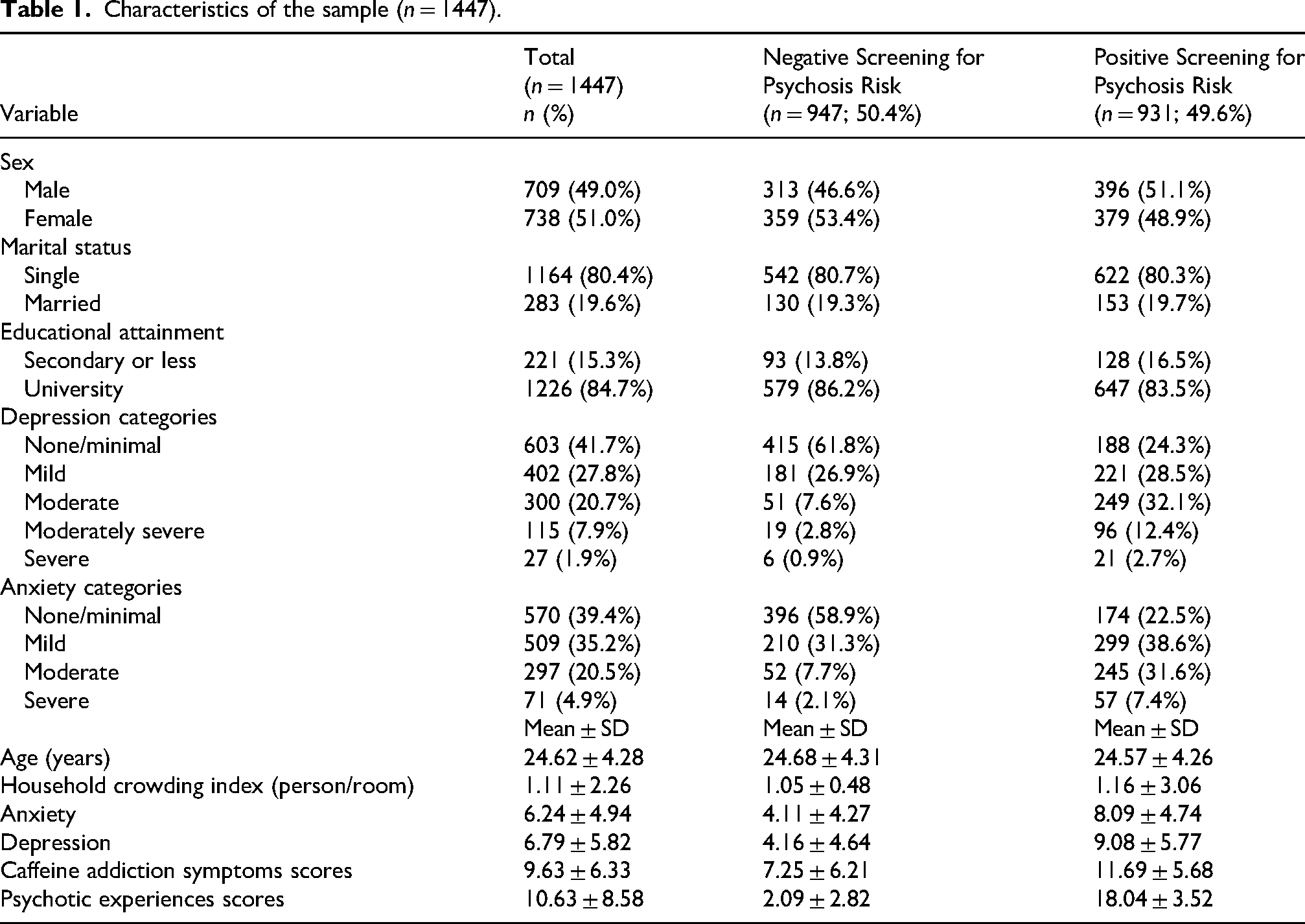
A total of 1447 young adults filled the survey, with a mean age of 24.62 ± 4.28 years and 51.0% females. All other details are shown in Table 1.
Characteristics of the sample (n = 1447).
Bivariate analysis of factors associated with PEs
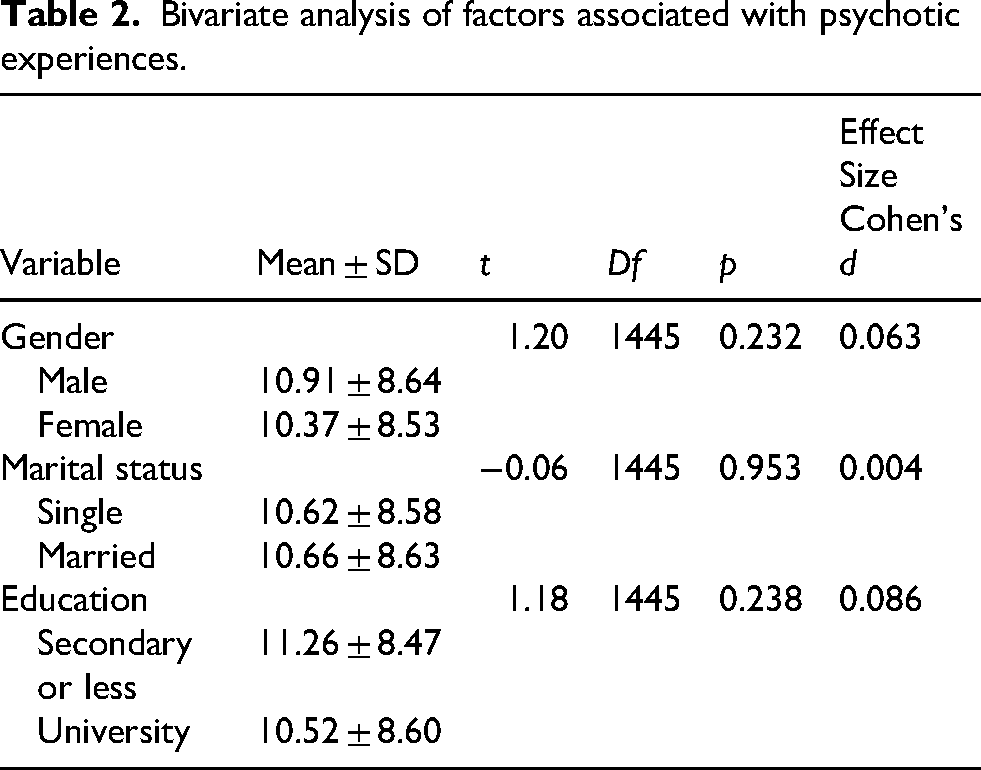
No significant differences in PEs were observed across gender (t(1445) = 0.88; p = 0.377), martial status (t(1445) = 0.70; p = 0.484) or education level (t(1445) = 0.90; p = 0.368) (Table 2). (Higher depression (r = 0.47; p < 0.001), anxiety (r = 0.44; p < 0.001) and caffeine addiction symptoms (r = 0.40; p < 0.001) were significantly associated with more PEs. No significant correlations were found between PEs and age (r = −0.03; p > 0.05) or household crowding index (r = 0.03; p > 0.05) (Table 3).
Bivariate analysis of factors associated with psychotic experiences.
Pearson correlation matrix.
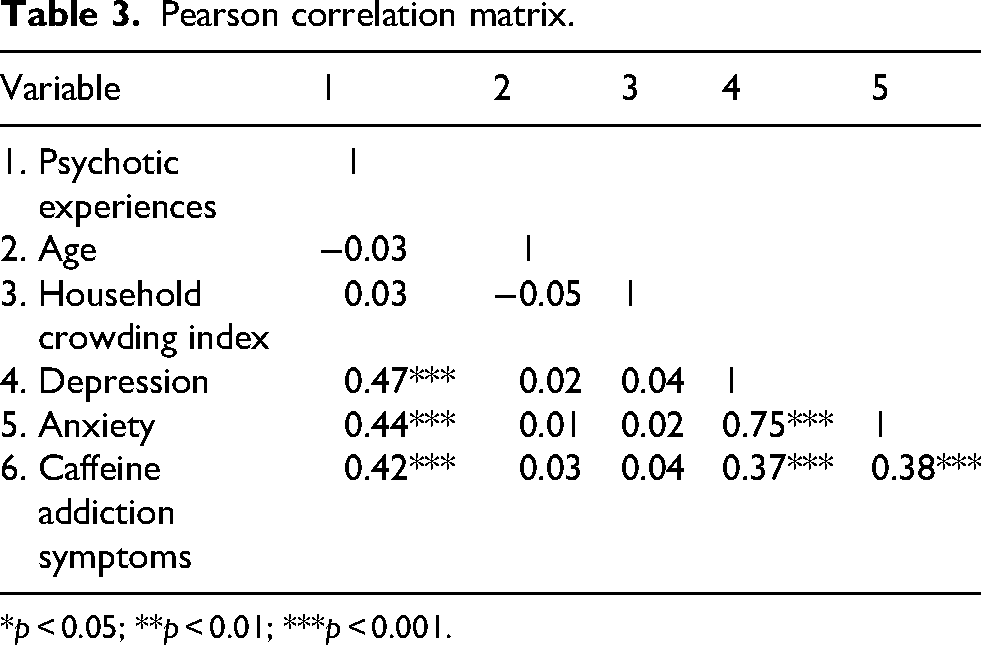
*p < 0.05; **p < 0.01; ***p < 0.001.
Mediation analysis
Mediation analyses were performed using PEs as the dependent variable and adjusting for age and household crowding index. The model-taking depression as the independent variable showed that caffeine addiction symptoms partially mediated the association between depression and PEs (standardized indirect effect: Beta = 0.10; BootSE = 0.01; Boot CI 0.08; 0.13) (Figure 1). Depression scores were significantly associated with higher caffeine addiction symptoms (Beta = 0.37; p < 0.001). In turn, caffeine addiction symptoms were significantly associated with higher PEs (Beta = 0.29; p < 0.001). Depression scores were also directly associated with PEs (Beta = 0.36; p < 0.001), while the total effect was significant (Beta = 0.47; p < 0.001). The R2 value of the model was 0.290 (high effect size), showing that 29.0% of the variance in PEs is accounted for by caffeine addiction symptoms.
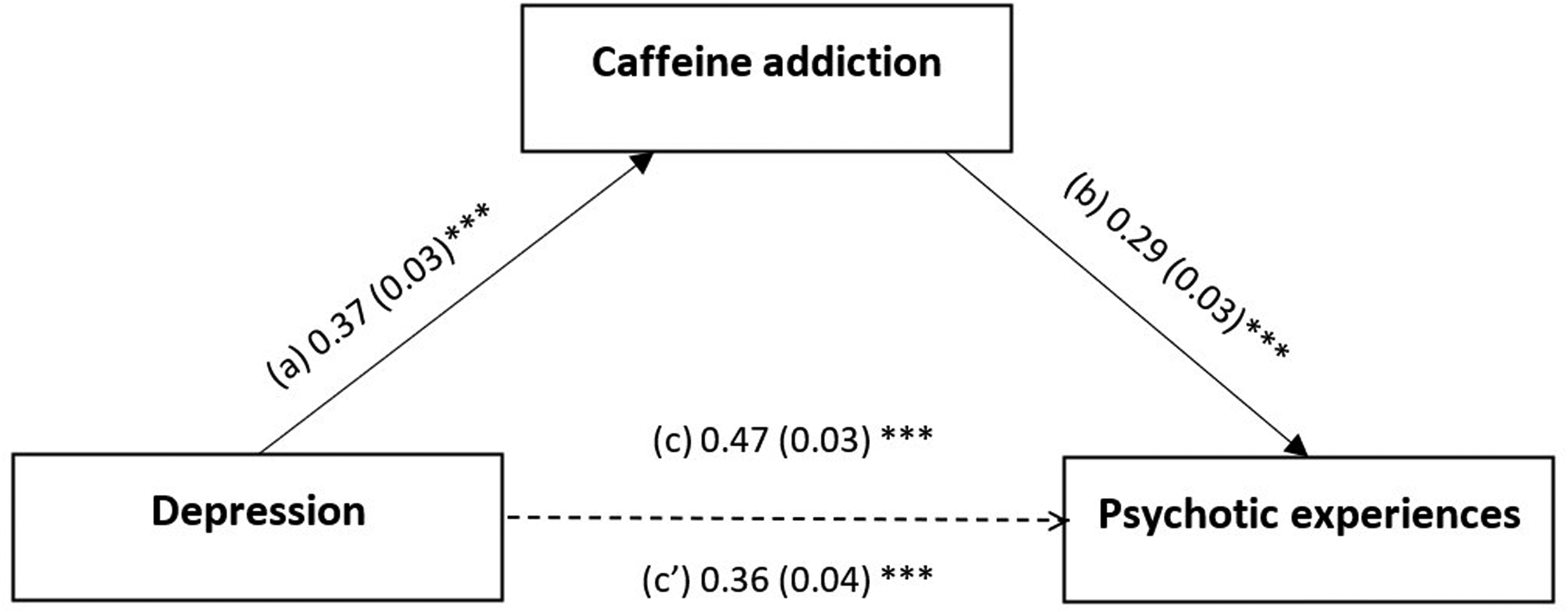
Moderation effect of caffeine addiction symptoms between depression and psychotic experiences. (a) Relation between depression and caffeine addiction (R2 = 0.137); (b) Relation between caffeine addiction and psychotic experiences (R2 = 0.290); (c) Total effect of depression on psychotic experiences (R2 = 0.219); (c') Direct effect of depression on psychotic experiences. Numbers are displayed as regression coefficients (standard error). ***p < 0.001.
The model taking anxiety as the independent variable showed that caffeine addiction symptoms partially mediated the association between anxiety and PEs (standardized indirect effect: Beta = 0.11; BootSE = 0.01; Boot CI 0.09; 0.14). Higher anxiety was significantly associated with higher caffeine addiction symptoms (standardized Beta = 0.38; p < 0.001). Higher caffeine addiction symptoms were significantly associated with more PEs (standardized Beta = 0.30; p < 0.001). Finally, higher anxiety was significantly and directly associated with more PEs (standardized Beta = 0.32; p < 0.001), while the total effect was also significant (standardized Beta = 0.44; p < 0.001) (Figure 2). The R2 value of the model was 0.267 (medium effect size), showing that 26.7% of the variance in PEs is accounted for by caffeine addiction symptoms.
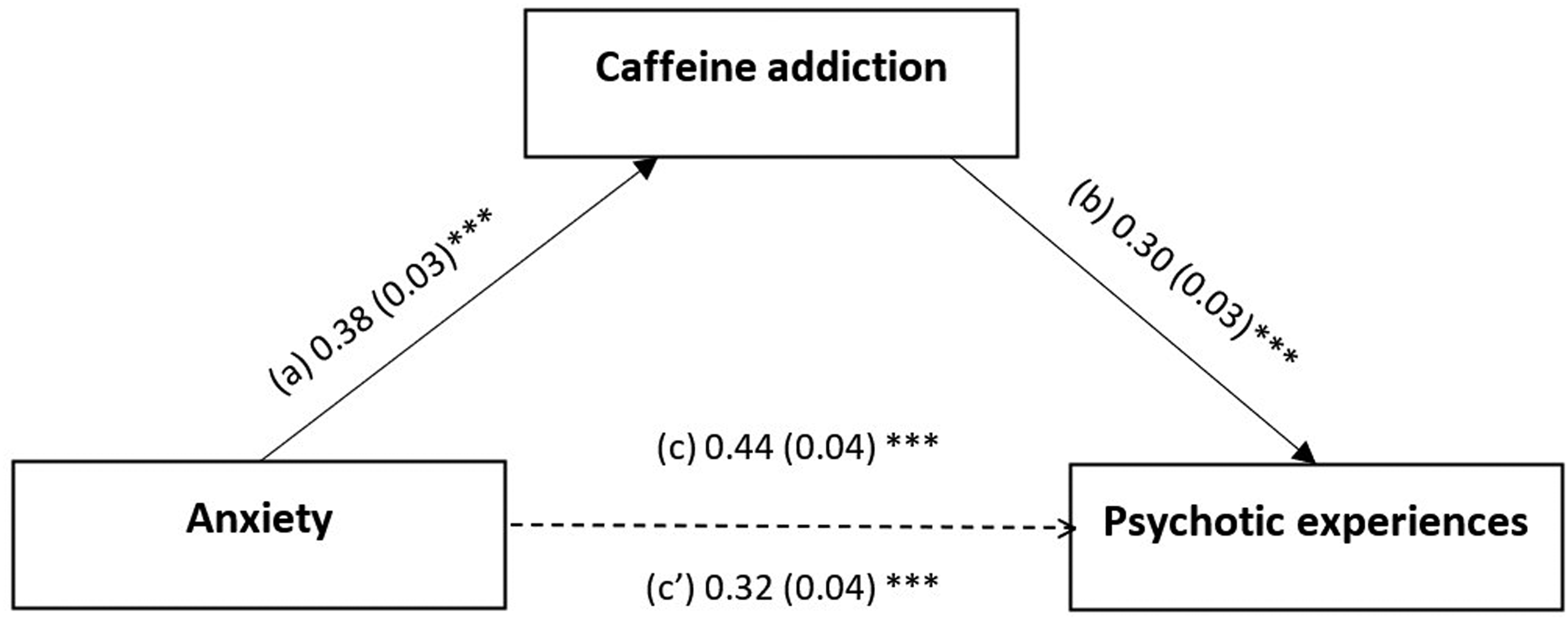
Moderation effect of caffeine addiction symptoms between anxiety and psychotic experiences. (a) Relation between anxiety and caffeine addiction (R2 = 0.146); (b) Relation between caffeine addiction and psychotic experiences (R2 = 0.267); (c) Total effect of anxiety on psychotic experiences (R2 = 0.192); (c’) Direct effect of anxiety on psychotic experiences. Numbers are displayed as regression coefficients (standard error). ***p < 0.001.
Discussion
Through this study, we aimed to contribute to the currently limited number of studies that have examined the relationship between depression symptoms, anxiety symptoms, and PEs in young adults. Findings showed that caffeine addiction symptoms served as a partial mediator in the link between depression symptoms and anxiety symptoms to PEs, indicating the role of caffeine addiction symptoms in increasing proneness to PEs in young people with depression and anxiety symptoms. The direct effect of both depression and anxiety symptoms on PEs concurs with the longitudinal evidence available, indicating that depression and anxiety are each connected with the development of later psychotic symptoms (Freeman et al., 2012; McGrath et al., 2016; Morales-Muñoz et al., 2022; Yamasaki et al., 2018). The presence of a mediation effect indicates that higher depression and higher anxiety scores were associated with increased PEs both directly and indirectly through caffeine addiction symptoms. These findings suggest that depression, anxiety, and caffeine addiction symptoms may jointly contribute to an increased likelihood of PEs.
Individuals with higher depression and higher anxiety scores reported greater caffeine addiction symptoms severity; in turn, greater caffeine addiction symptoms exhibited in turn higher levels of PEs. These findings align with the evidence that depression and anxiety may contribute to increased caffeine intake within the framework of the self-medication theory (López-Cruz et al., 2018; Tenore et al., 2015). Previous research has shown that depression and anxiety can potentially induce excessive caffeine use and abuse (Begdache et al., 2020; Whalen et al., 2008). For example, a repeated cross-sectional study showed that mental distress in young adults was significantly linked to greater caffeine intake (Begdache et al., 2020). Previous research also pointed to a dose–response relationship between consumption of highly caffeinated drinks and depression (Hong and Peltzer, 2017). Researchers from Pakistan found significant positive correlations between caffeine consumption and depression and anxiety scores among university students (Aleem et al., 2024). A study conducted among Turkish adults reported that the risk of caffeine use disorder increased alongside levels of depression and anxiety (Bodur et al., 2024).
Furthermore, mediation analyses results are in agreement with an evolving literature that increasingly recognizes caffeine as one of substances that, when consumed at high doses, can potentially contribute to the onset or exacerbation of psychotic symptoms (Wang et al., 2015a). The existing research supports that caffeine is closely related to not only aggravation of pre-existing psychotic disorders, but also to de novo psychotic symptoms in otherwise healthy individuals (Wang et al., 2015b). In the literature, caffeine-induced psychosis has been reported in people who did not have preexisting psychotic disorders (Hernandez-Huerta et al., 2017a; Mannix et al., 2024). Goiney et al. (2012) presented the case of a previously healthy 29-year-old man who developed a new-onset of psychotic symptoms after increasing his caffeine intake; they also reported seven other similar cases of caffeine-induced psychosis in their systematic review. Of note, although the substance itself can be involved in the development and/or exacerbation of psychotic symptoms by facilitating dopaminergic neurotransmission (Volkow et al., 2015), behavioral aspects of caffeine addiction symptoms, such as emotional and psychological changes, risky behaviors, or isolation may impose substantial psychological stress that contributes to downstream biological manifestations (Fekih- Romdhane et al., 2021a, 2021b, 2023a, 2023b, 2024c). Therefore, our findings should be interpreted with caution, bearing in mind that the observed mediation model might reflect psychological dysregulation rather than caffeine-induced pharmacological effects.
Limitations
The main limitation of this study is its cross-sectional design, which provides evidence for associations but not causality. Based on evidence reporting that caffeine addiction symptoms can cause anxiety (Liu et al., 2024) and depression (Wang et al., 2016), it is likely that relationships between depression symptoms, anxiety symptoms and caffeine addiction symptoms are bidirectional, resulting in a spiraling of negative affect and anxious arousal. Therefore, future longitudinal research is still required to establish the temporal order of the observed correlations. Furthermore, the snowball sampling technique was utilized to collect data, thereby introducing a potential sampling bias, as our participants may not be fully representative of the broader general population of Lebanon. Specifically, this sampling approach may attract a specific subgroup of participants interested in the topic or having access to the Internet, and restrict how broadly we can apply the findings to diverse samples with different characteristics. Moreover, multiple factors that could possibly influence the effects of caffeine (such as caffeine source, body mass index, sleep, lifestyle choices, or external stress triggers [work, family, etc.]) were not taken into consideration in this study. While our SEM approach provides strong model fit and a significant indirect effect, we acknowledge the absence of a formal sensitivity analysis; future studies should incorporate residual correlation sensitivity analyses (e.g., using rho) to examine how robust the mediation effect is in the presence of possible unmeasured confounding. Causal factors contributing to the onset and continuation of PEs include not only depression, anxiety, and caffeine addiction symptoms, but also a range of other factors, including autism spectrum traits, deficits in social cognition, or neurological dysfunctions (such as impaired function of glymphatic system) (Barlattani et al., 2023, 2024a, 2024b). The role of these factors should be considered in future research. Finally, our study relied on self-report measures, which may be subject to reporting biases such as recall bias and social desirability.
Clinical and research implications
Findings suggest that caffeine addiction symptoms may have a mediating role between depression symptoms, anxiety symptoms and PEs. On the basis of the present findings and literature review, more caution should be applied in using caffeine as a supposedly “safe” and “risk-free” substance. Indeed, caffeine is the most commonly accepted, consumed, and unregulated psychoactive drug worldwide. Considering that it has a highly addictive potential, and since its potential mental health risks—including psychosis—are becoming increasingly evident, recognizing and adjusting any patterns of excessive use appear to be a crucial part of prevention. Some researchers have even called for considering excessive caffeine intake “a global public health problem” because of the possible serious and understudied harmful effects on health (Valdivieso-Jiménez, 2022).
The adolescent and adult general population, in particular potentially vulnerable consumers (such as those with a familial risk for psychosis), should be advised to use caffeine in moderation. For instance, information and warnings to the public should be included in caffeinated products. In addition, young people presenting with depression and anxiety symptoms should be carefully assessed for caffeine intake in clinical practice, educated regarding the known health risks associated with this substance, and advised to limit excessive caffeine intake, which can, in turn, help prevent the occurrence of PEs. More research is needed with longitudinal data to confirm our findings and broaden our understanding of this topic. Future interventional studies are warranted to understand the role of treating caffeine addiction symptoms in improving or preventing the occurrence of PEs in young people with depression and anxiety symptoms. Lastly, our study could be replicated using longitudinal designs that allow to better capture causal inferences. Specifically, an integration of diagnosis and prognosis indicators into SEM approaches may enhance the precision and interpretability of causal effect estimates.
Conclusion
The findings from this study suggest that the direct effects of depression and anxiety, combined with the indirect effect of high levels of caffeine addiction symptoms, are likely to increase endorsement of PEs. While these results still need further replication and support using longitudinal and experimental designs, it can be suggested that addictive patterns of caffeine consumption can have profound effects on mental health that should be detected and addressed. In particular, caution should be exercised when people with depression and/or anxiety symptoms increase their use of caffeine, as this might precipitate or exacerbate psychosis in at-risk individuals. Future research is still necessary to improve knowledge on pathways linking depression, anxiety, caffeine addiction symptoms, and psychosis.
Footnotes
Acknowledgments
The authors would like to thank all participants.
Ethical approval
Ethics approval for this study was obtained from the ethics committee of the School of Pharmacy at the Lebanese International University.
Consent for publication
Not applicable.
Informed consent
Written informed consent was obtained from all subjects; the online submission of the soft copy was considered equivalent to receiving written informed consent.
Author contributions
SO, FFR, and SH designed the study; FFR drafted the manuscript; SH carried out the analysis and interpreted the results; FS and MD collected the data; DM, SO, RH, and FH reviewed the paper for intellectual content. All authors reviewed the final manuscript and gave their consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
All data generated or analyzed during this study are not publicly available due to restrictions from the ethics committee, but are available upon a reasonable request from the corresponding author (SH).
Clinical trial number
Not applicable.