
Abstract
Background
Creatine is a nitrogen-containing conditionally essential nutrient obtained primarily from animal-based foods and has been widely studied for its ergogenic benefits when used in combination with resistance training. However, its independent association with musculoskeletal health markers in the general population remains underexplored.
Objective
To examine the relationship between habitual dietary creatine intake and indicators of muscle mass and strength in a large, nationally representative sample of the U.S. population.
Methods
We analyzed data from 108,403 participants across the NHANES 1999–2023 cycles. Dietary creatine intake was estimated using 24-h dietary recalls. Total lean body mass (excluding bone mineral content) was available for 43,042 individuals, and combined grip strength data were available for 13,612 individuals. Multivariable linear regression models were used to examine associations between creatine intake and musculoskeletal health outcomes, adjusting for dietary, demographic, hormonal, and physical activity-related confounders.
Results
Higher dietary creatine intake was significantly associated with greater total lean body mass and handgrip strength (P < 0.01). Participants in the highest quartile of habitual creatine intake exhibited the most favorable musculoskeletal profiles. Each additional gram of dietary creatine intake was associated with a 2.66 kg increase in lean body mass and a 5.24 kg increase in handgrip strength. Moderate correlations were also observed between creatine intake and other body composition parameters, including bone mineral content and total body fat percentage.
Conclusions
Our study suggests that higher dietary creatine intake is associated with favorable musculoskeletal outcomes, even after adjustment for physical activity, within a cross-sectional framework. These findings point to dietary creatine as a factor of interest in relation to musculoskeletal health, meriting further study. Further longitudinal and mechanistic research is needed to establish causality and better understand the underlying biological pathways.
Introduction
Creatine is a nitrogen-containing organic compound naturally synthesized from the amino acids arginine, glycine, and methionine, and is endogenously produced in the liver, kidneys, pancreas, and brain (Wyss and Kaddurah-Daouk, 2000). It is obtained exogenously almost exclusively from animal-source foods, primarily red meat, poultry, and fish, with negligible amounts present in plant-based foods (Kaviani et al., 2020). As a non-proteinogenic amino acid derivative and conditionally essential nutrient, creatine plays a central role in cellular energy metabolism by maintaining adenosine triphosphate (ATP) availability via the phosphocreatine energy system (Ostojic and Forbes, 2022), particularly in tissues with high and fluctuating energy demands, including skeletal muscle. Approximately 95% of the body's creatine stores are located in skeletal muscle, underscoring its physiological relevance to muscle function and mass maintenance (Kreider and Stout, 2021). Over the past three decades, creatine supplementation has been extensively investigated for its ergogenic and therapeutic effects. Numerous randomized controlled trials and meta-analyses have demonstrated that supplemental creatine, when co-administered with resistance training, can significantly improve muscle strength, lean mass, and physical performance across diverse populations, including athletes, healthy older adults, and clinical cohorts with muscle-wasting conditions (Burke et al., 2023). However, most studies fail to distinguish between the effects of creatine alone and those arising from synergistic interactions with exercise or nutritional supplements. The limited number of studies addressing this topic has often been constrained by small sample sizes, short study durations, heterogeneous dosing regimens, or a narrow focus on athletic or clinical subgroups (Pashayee-Khamene et al., 2024). Despite the robust evidence supporting the use of supplemental creatine, considerably less is known about the role of habitual dietary creatine intake from food sources and its relationship with indices of musculoskeletal health in the general population. Consequently, the extent to which habitual dietary creatine consumption may independently contribute to indicators of muscle function, such as handgrip strength, and body composition, particularly lean soft tissue mass, at the population level remains poorly understood. Handgrip strength is a widely used, non-invasive proxy for overall muscle function and an established predictor of morbidity, disability, and mortality across the lifespan (Vaishya et al., 2024). Likewise, lean mass serves as a critical determinant of metabolic health, physical capability, and quality of life (Wolfe, 2006). Understanding modifiable dietary factors that contribute to the preservation or enhancement of these parameters has become increasingly important in light of the growing public health burden associated with sarcopenia, frailty, and age-related muscle loss. In this context, the primary objective of the present study was to evaluate the relationship between habitual dietary creatine intake and two key indicators of musculoskeletal health (handgrip strength and lean body mass) in a nationally representative sample of U.S. individuals. Using data from the National Health and Nutrition Examination Survey (NHANES), we aimed to determine whether habitual creatine intake is positively associated with muscle strength and mass, independent of major dietary and demographic covariates. These findings may provide valuable insights into the potential contribution of dietary creatine as a modifiable nutritional factor for promoting musculoskeletal health across the general population.
Methods
Study population
This cross-sectional, population-based study utilized data from the NHANES, an ongoing series of biennial surveys designed to evaluate the health and nutritional status of the civilian, non-institutionalized U.S. population. NHANES collects comprehensive data through standardized physical examinations, laboratory tests, and structured interviews addressing dietary habits, lifestyle behaviors, and health conditions. Detailed descriptions of the NHANES methodology have been published elsewhere (Centers for Disease Control and Prevention, 2025). For the present analysis, we compiled and harmonized NHANES data spanning from 1999 to 2023. Participants were eligible for inclusion if they had completed a single in-person 24-h dietary recall and had available data on at least one biomarker of muscle strength or volume (see below), as obtained from the NHANES Examination Data files. All NHANES protocols received ethical approval from the U.S. National Center for Health Statistics Ethics Review Board under the following protocol numbers: #98–12, #2005–06, Continuation of Protocol #2005–06, #2011–17, Continuation of Protocol #2011–17, #2018–01, Continuation of Protocol #2018–01, and #2021–05. Written informed consent was obtained from all participants. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Study outcomes, exposure variables, and covariates
The primary outcome measures included total lean body mass excluding bone mineral content (BMC), assessed using dual-energy X-ray absorptiometry (DXA), and isometric muscle strength, measured via a handgrip dynamometer. Prior research has suggested that lean mass excluding BMC serves as a valid proxy for estimating skeletal muscle mass (Visser et al., 1999). Total lean body mass excluding BMC was analyzed in absolute units rather than normalized to height. This approach was chosen because the primary objective was to evaluate associations between dietary creatine intake and the total amount of metabolically active tissue, which represents the principal physiological reservoir and site of creatine utilization. Height-normalized indices are useful for clinical classification, but absolute lean mass more directly reflects whole-body creatine-relevant tissue burden. Additional whole-body composition parameters analyzed included BMC, lean body mass, fat mass, and percent body fat. The primary exposure variable was total daily dietary creatine intake, measured in grams. For categorical analyses, participants were stratified into quartiles according to their creatine intake levels. Key covariates included dietary intake variables (total energy and protein intake), demographic characteristics (age, sex, race/ethnicity, educational attainment, and family poverty income ratio), circulating sex hormone concentrations (testosterone and estradiol), and indicators of physical activity (daily duration of moderate recreational activity and sedentary behavior).
Data sources and measurements
Whole-body DXA scans were performed as part of the NHANES body composition assessment at the Mobile Examination Center by trained and certified radiologic technologists. Eligible participants included individuals aged 8 to 59 years (NHANES 2011–2018), 8 to 69 years (NHANES 2005–2006), and 8 years and older (NHANES 1999–2004). Exclusion criteria included pregnancy (confirmed via urine test or self-report), self-reported use of radiographic contrast material within the preceding seven days, and self-reported weight exceeding 204 kg or height exceeding 196 cm due to DXA table limitations. Whole-body scans were obtained using Hologic Discovery Model A and Hologic QDR-4500A densitometers (Hologic, Inc., Bedford, MA) equipped with either Hologic software version 8.26:a3* or Apex software version 3.2. Radiation exposure from DXA scanning was minimal (< 20 µSv). Scans from the DXX_G dataset were analyzed using Hologic APEX version 4.0 with the NHANES Body Composition Analysis (BCA) option. Additional details on the DXA examination protocol are available elsewhere (National Center for Health Statistics, 2025). Isometric muscle strength was assessed via a handgrip dynamometer (Model 5401, Takei Digital Grip Strength Dynamometer, Tokyo, Japan) during the NHANES 2011–2014 cycles in participants aged six years and older, as part of the Examination Data component. Trained examiners administered the test following a standardized protocol. Participants were excluded if unable to grip the dynamometer with either hand due to bilateral amputation, paralysis, or absence of thumbs. Those capable of using one hand were still included. Following grip size adjustment and a practice trial to ensure comprehension, participants performed three maximal-effort trials per hand, alternating hands with a 60-s rest between trials. The test was conducted in a standing position unless physical limitations required otherwise. Combined grip strength was defined as the sum of the highest values recorded from each hand (in kilograms) and was not calculated for participants tested with only one hand. Dietary creatine intake was estimated from a single in-person 24-h dietary recall available in each NHANES cycle (1999–2023); multiple-day recalls were not used because several survey rounds provide only one recall assessment. For participants under six years of age, proxy respondents provided dietary information. Intake was calculated based on the average creatine content of food sources, including 0.20 g/kg for dairy products and 3.88 g/kg for meat-based foods, following previously established methods (Todorovic et al., 2022). To estimate creatine intake, creatine-containing foods (e.g., milk and milk products; meat, poultry, and fish) were first identified using eight-digit food codes from the U.S. Department of Agriculture entries in the Individual Foods files. For each participant, the gram weight of every creatine-containing food item (USDA codes 11100000–28522000) was recorded, and the net daily intake of these foods was calculated by aggregating all relevant items. Total daily creatine intake (grams per day) was then determined by applying the average creatine content across all identified creatine-containing food sources to each individual's reported consumption. No exclusions were applied on the basis of reported total energy intake. All participants were retained provided that dietary recall data met NHANES quality-control criteria and were not flagged as incomplete or corrupted. Inspection of the intake distributions indicated that even the highest reported energy intakes (maximum ≈ 15,000 kcal/day) were within physiologically plausible limits and did not reflect obvious data entry errors. Accordingly, extreme dietary patterns, including high creatine intakes, were retained to preserve the full exposure range present in the dataset. Creatine obtained from dietary supplements or pharmacological preparations was not included in the exposure assessment and therefore did not contribute to the estimated total creatine intake. Relevant covariates were extracted from NHANES Demographic and Laboratory Data files.
Statistical analysis
To examine differences in the primary outcomes (total lean mass excluding BMC and handgrip strength) across quartiles of dietary creatine intake, one-way analysis of variance (ANOVA) was conducted, followed by Tukey's post hoc test for pairwise comparisons. Pearson correlation coefficients were calculated to assess associations between dietary creatine intake and both primary and secondary outcomes. Linear regression analyses were employed to evaluate the relationship between creatine intake and study outcomes, beginning with unadjusted models and subsequently incorporating a series of adjusted models: Model 1 (dietary intake), Model 2 (demographic variables), Model 3 (circulating sex hormone levels), and Model 4 (physical activity indicators). All analyses were performed using standard (unweighted) statistical procedures. NHANES sampling weights, strata, and primary sampling units were not incorporated. The analytic approach was selected to examine internal associations between dietary creatine intake and musculoskeletal outcomes rather than to generate nationally representative prevalence estimates. Accordingly, the present results describe within-sample relationships and should not be interpreted as population-level effect estimates for the U.S. population. All statistical tests were two-tailed, with significance defined as P ≤ 0.05. Data analyses were performed using IBM SPSS Statistics for Mac, version 24.0 (IBM Corp., Armonk, NY, USA).
Results
After removing duplicate entries and excluding incomplete or corrupted records (n = 20,406), a total of 108,403 respondents from the cumulative NHANES 1999–2023 cycles provided valid data on dietary creatine intake. Of these, total lean body mass excluding BMC was assessed in 43,042 participants, while combined handgrip strength measurements were available for 13,612 individuals (Figure 1).
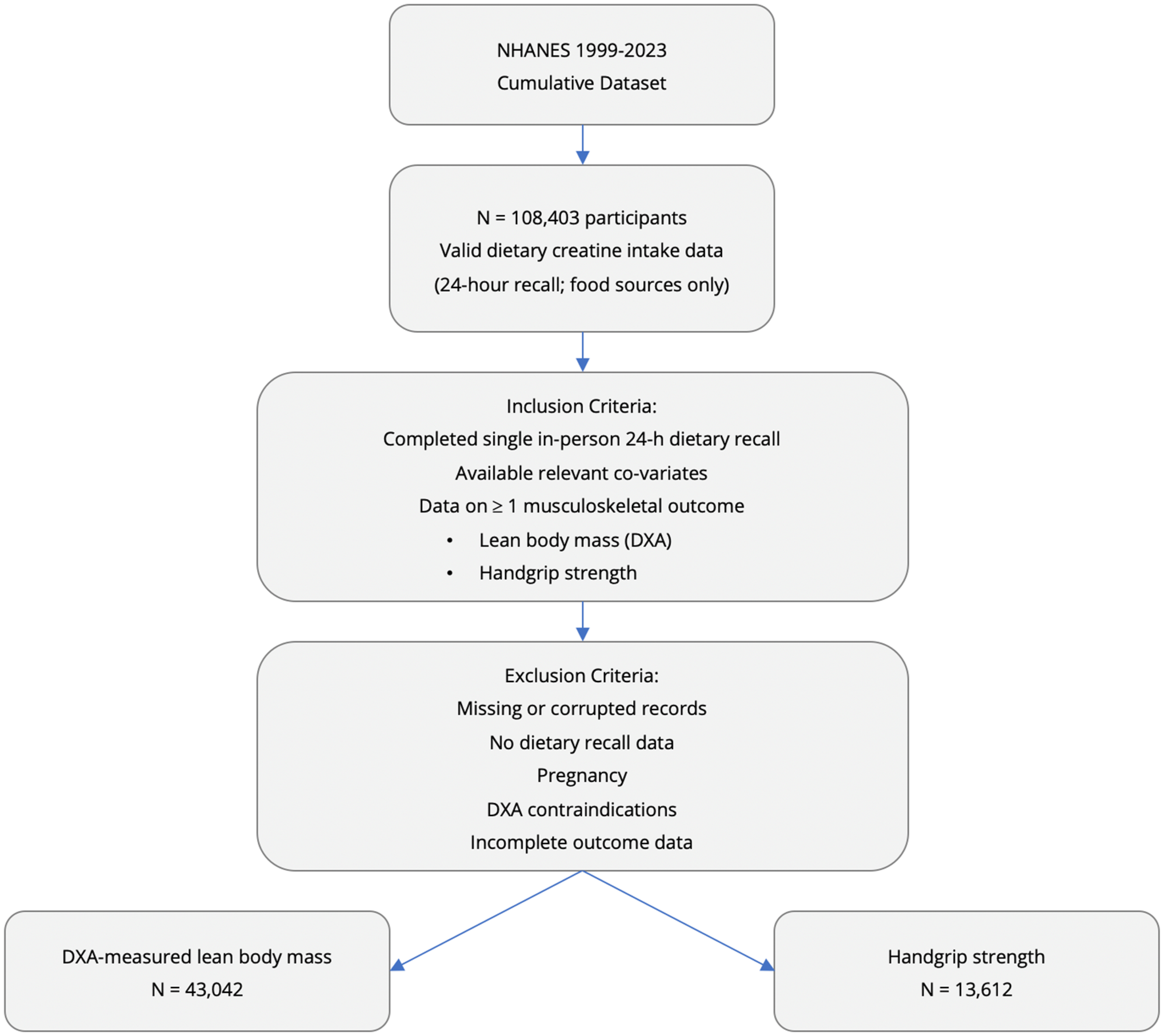
Flowchart illustrating data selection and inclusion criteria.
The characteristics of the study participants are depicted in Table 1.
Characteristics of the study population. Values are mean ± SD.
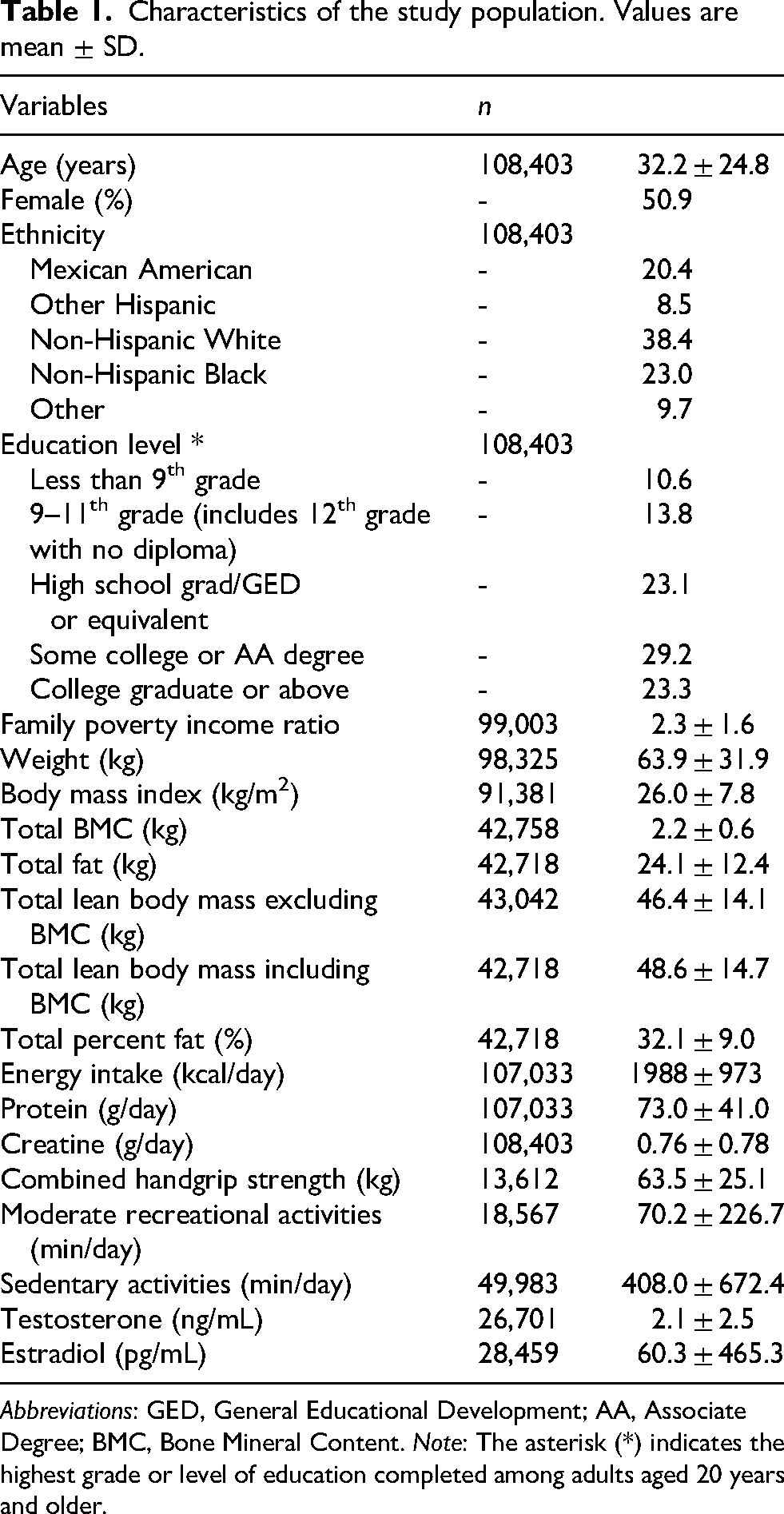
Abbreviations: GED, General Educational Development; AA, Associate Degree; BMC, Bone Mineral Content. Note: The asterisk (*) indicates the highest grade or level of education completed among adults aged 20 years and older.
A comparison of dietary creatine intake across quartiles revealed significant differences in both total lean body mass excluding BMC and handgrip strength among intake categories (P < 0.01) (Figure 2). Specifically, participants in the highest quartile (Q4) exhibited significantly greater total lean body mass and handgrip strength compared to all other quartiles, while values in the third quartile (Q3) were significantly higher than those in the first (Q1) and second (Q2) quartiles. No statistically significant difference was observed between Q1 and Q2 for either outcome.
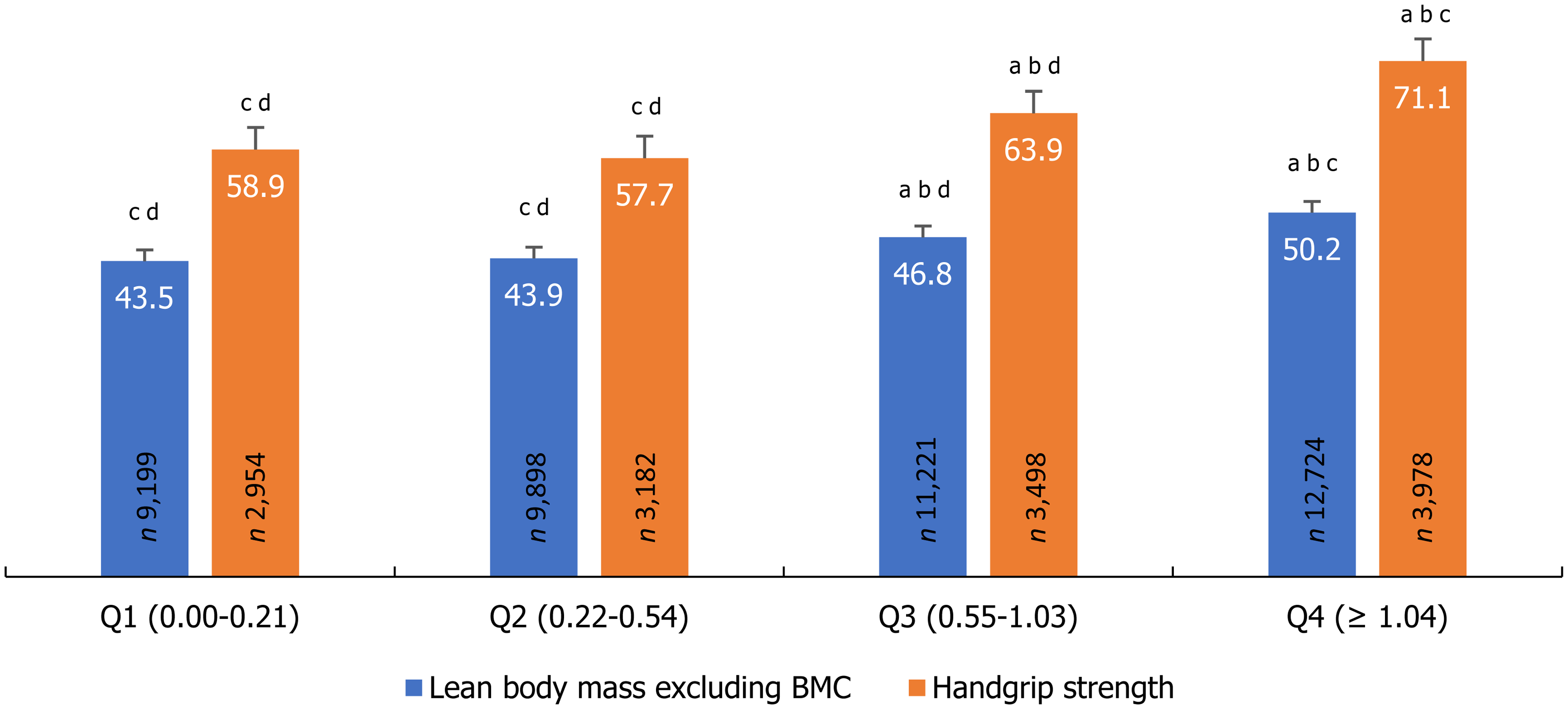
Total lean body mass excluding bone mineral content (BMC, kg; n = 43,042) and handgrip strength (kg; n = 13,612) across quartiles of daily creatine intake (grams per day). Bars represent mean values; error bars indicate standard errors and are shown for descriptive purposes only. Letters indicate a statistically significant difference between quartiles at P ≤ 0.05: a indicates a difference from Q1, b from Q2, c from Q3, and d from Q4; each successive quartile showing significantly higher values than lower quartiles.
Statistically significant correlations were observed between daily dietary creatine intake and both total lean body mass excluding BMC (r = 0.19, P < 0.01), and handgrip strength (r = 0.21, P < 0.01) in the overall sample (Figure 3). Additionally, significant correlations were identified between daily dietary creatine intake and other whole-body composition parameters, including total BMC (r = 0.17, P < 0.01), total lean body mass including BMC (r = 0.19, P < 0.01), and total body fat percentage (r = –0.12, P < 0.01).
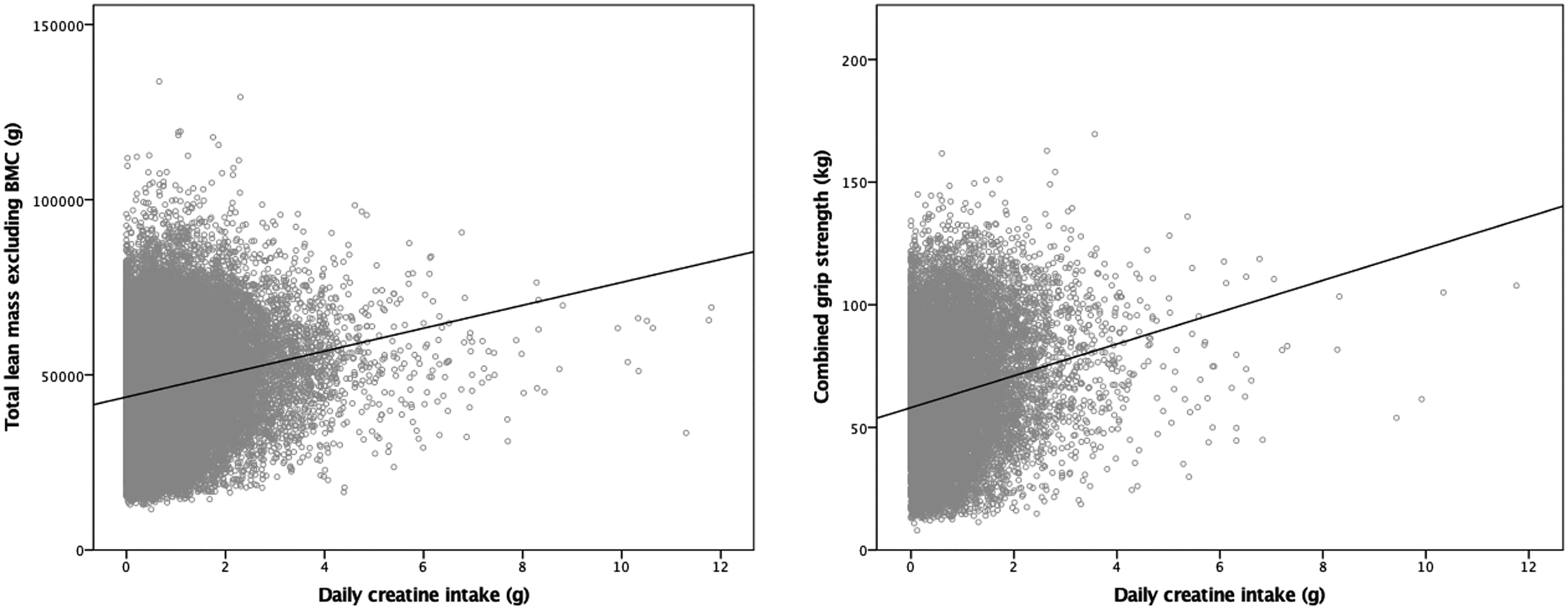
Scatterplot of creatine intake (grams per day) versus total lean body mass excluding bone mineral content (BMC, g; n = 43,042) and handgrip strength (kg; n = 13,612) in the general population. Statistically significant correlations were observed between daily dietary creatine intake and both total lean body mass excluding BMC (r = 0.19, P < 0.01), and handgrip strength (r = 0.21, P < 0.01) in the overall sample.
Crude linear regression analysis indicated a significant positive association between daily dietary creatine intake and total lean body mass excluding BMC (P < 0.01), with each additional gram of creatine intake linked to an estimated increase of 3.2 kg in lean body mass (95% confidence interval [CI]: 3.1–3.4 kg); similarly, each additional gram was associated with a 6.5 kg increase in handgrip strength (95% CI: 6.0–7.0 kg).
In adjusted models, creatine intake remained significantly associated with total lean body mass and handgrip strength after controlling for dietary covariates (Model 1: B = 1.08, ß = 0.06; B = 1.88, ß = 0.06; both P < 0.01), demographics (Model 2: B = 0.69, ß = 0.05; B = 0.78, ß = 0.03; both P < 0.01), sex hormones (Model 3: B = 1.75, ß = 1.03; B = 2.48, ß = 0.09; both P < 0.01), and physical activity (Model 4: B = 2.66, ß = 0.18; B = 5.24, ß = 0.20; both P < 0.01).
Linear regression analyses stratified by gender and age categories yielded consistent results (Table 2 and Table 3), with the exception of the older adult subgroup, in which the association between dietary creatine intake and handgrip strength was attenuated and became non-significant after adjustment for relevant covariates.
Crude and adjusted linear regression analyses stratified by gender.
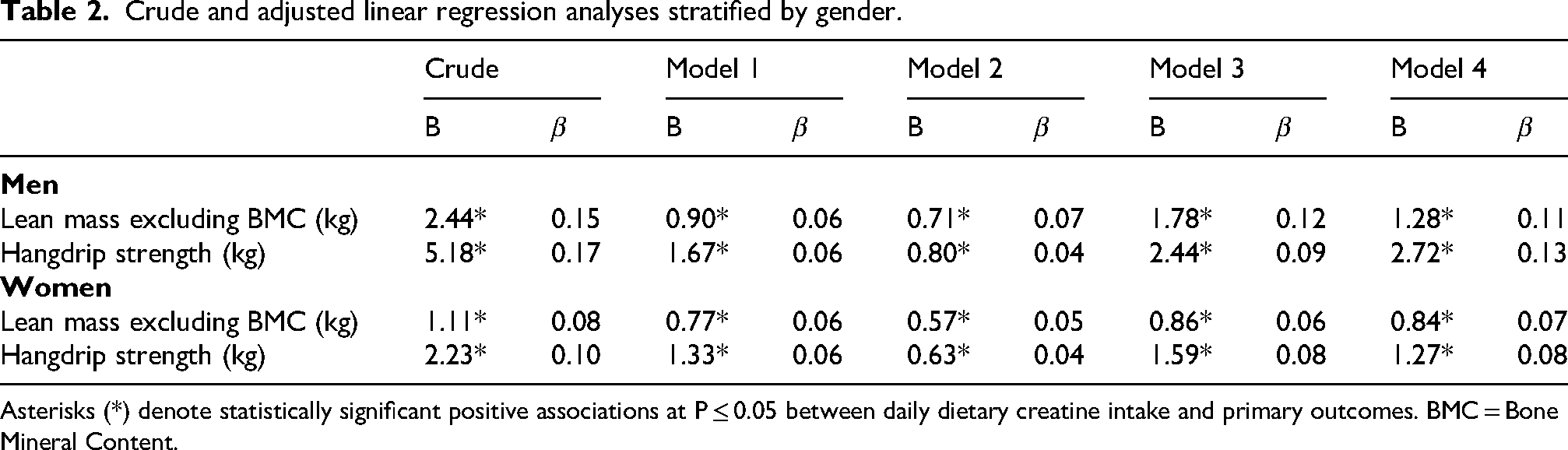
Asterisks (*) denote statistically significant positive associations at P ≤ 0.05 between daily dietary creatine intake and primary outcomes. BMC = Bone Mineral Content.
Crude and adjusted linear regression analyses stratified by age categories.
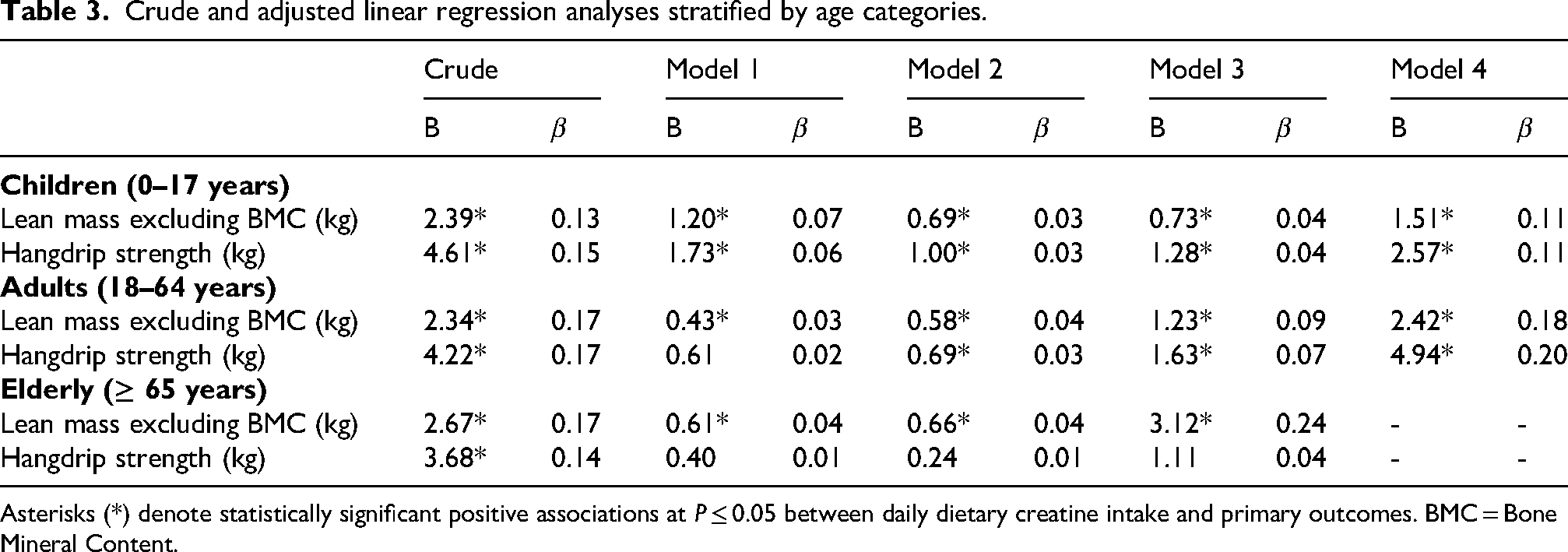
Asterisks (*) denote statistically significant positive associations at P ≤ 0.05 between daily dietary creatine intake and primary outcomes. BMC = Bone Mineral Content.
Discussion
This large-scale epidemiological study provides one of the first comprehensive assessments of the relationship between habitual dietary creatine intake and key markers of musculoskeletal health in a nationally representative and diverse sample of the general population. Our findings demonstrate a consistent and statistically significant positive association between daily dietary creatine intake and both lean body mass (excluding BMC) and muscle strength, as assessed by handgrip dynamometry. Notably, these associations remained robust after adjusting for a wide range of potential confounding factors, including total caloric and protein intake, demographic variables (such as age, sex, and socioeconomic status), circulating sex hormone levels, and physical activity behaviors. The observed relationships suggest that higher habitual consumption of creatine through regular diet, primarily from animal-based foods such as meat and dairy, may contribute to improved muscle mass and function, independent of other nutritional and lifestyle influences. These findings support the potential role of dietary creatine as a modifiable dietary factor with implications for the preservation and promotion of musculoskeletal health across the lifespan.
While numerous studies have demonstrated the efficacy of creatine supplementation in enhancing muscle mass, strength, and physical performance, most have combined creatine with resistance exercise, making it difficult to isolate creatine's independent effects. This co-administration limits understanding of creatine's standalone contribution to musculoskeletal health, particularly in individuals unable or unwilling to engage in structured physical activity. Nonetheless, emerging evidence suggests that creatine supplementation alone may yield modest but meaningful improvements in muscle health indices. Several clinical trials, particularly in older adults and in populations with chronic conditions such as heart disease, rheumatoid arthritis, and those undergoing hemodialysis, have reported significant gains in lean body mass, strength, and functional capacity following creatine supplementation without exercise (Camic et al., 2010; Kuethe et al., 2006; Marini et al., 2020; Stout et al., 2007; Wilkinson et al., 2016). However, other studies have found little to no effect (Backx et al., 2017; Bermon et al., 1998; Hayashi et al., 2014; Lobo et al., 2015; Rawson and Clarkson, 2000; Walter et al., 2002), raising questions about its general applicability as a sole intervention for improving muscle mass or function. A recent systematic review and dose-response meta-analysis concluded that creatine alone may produce a small but statistically significant increase in lean body mass (Pashayee-Khamene et al., 2024). Still, the magnitude of benefit appears smaller in the absence of exercise, and existing studies are constrained by limitations such as small sample sizes, short intervention durations, inconsistent dosing, lack of standardized outcome measures, and insufficient control for confounders like dietary protein and baseline activity. To address these gaps, our cross-sectional study examined the relationship between habitual dietary creatine intake and muscle health indicators using a large, nationally representative dataset, systematically evaluating creatine intake across a wide exposure range while accounting for dietary, hormonal, and physical activity-related confounders to provide a more comprehensive perspective on its potential role in musculoskeletal health.
The present analysis, based on data from over 100,000 individuals across multiple NHANES cycles (1999–2023), provides robust epidemiological evidence supporting a positive association between dietary creatine intake and key indicators of muscle health, including total lean body mass (excluding BMC) and handgrip strength. Among the total sample, lean body mass and strength data were available for substantial subgroups, enhancing the generalizability of the findings. The observed associations were not only statistically significant but also consistent across quartiles of creatine intake, with the highest intake group (Q4) exhibiting significantly greater lean mass and muscle strength compared to lower intake groups. These associations persisted even after adjusting for a wide range of potential confounders, including dietary intake, demographic characteristics, sex hormone levels, and physical activity, suggesting an independent relationship between habitual creatine consumption and muscle status. Furthermore, moderate correlations were observed between creatine intake and additional body composition parameters such as BMC, total lean body mass including BMC, and body fat percentage, reinforcing the relevance of creatine in musculoskeletal physiology and metabolism. Crude regression models showed strong dose-response relationships, wherein each additional gram of daily creatine intake corresponded to an approximate 3.2 kg increase in lean body mass and a 6.5 kg increase in handgrip strength. Although the effect sizes were attenuated after adjustment, the associations remained statistically significant in all models, underscoring the robustness of the findings. These results align with previous interventional studies suggesting potential benefits of creatine supplementation for muscle mass and strength (Kazeminasab et al., 2025; Smith et al., 2025; Zhang et al., 2025). Notably, this study expands upon prior research by evaluating creatine intake from habitual dietary sources, rather than supplements, and in a real-world, population-based setting. Collectively, our findings suggest that higher dietary creatine intake may serve as a modifiable nutritional factor with relevance for muscle preservation and strength maintenance in the general population, including individuals who may not engage in structured physical training. Creatine may positively influence lean body mass and muscle strength even in the absence of exercise through several interconnected mechanisms. One key pathway involves the increase in intramuscular phosphocreatine stores, which enhances ATP resynthesis and supports cellular energy turnover, an essential factor for maintaining muscle integrity even during rest (Casey and Greenhaff, 2000). Additionally, creatine-induced cellular hydration promotes anabolic signaling by increasing intracellular water content, which can activate pathways such as mTOR, stimulating muscle protein synthesis and inhibiting protein breakdown (Marzuca-Nassr et al., 2019). Creatine may also upregulate muscle accretion (a component of lean body mass) by influencing myogenic regulatory factors like MyoD and myogenin while suppressing myostatin, a negative regulator of muscle development (de Carvalho et al., 2023). These molecular effects could enhance satellite cell activity and muscle regeneration (Chilibeck et al., 2017). Furthermore, creatine possesses mild anti-inflammatory and antioxidant properties that may reduce oxidative stress and muscle degradation (Lawler et al., 2002), particularly beneficial in aging populations or those with chronic conditions. The role of creatine in mitochondrial health, by supporting mitochondrial respiration and stabilizing membrane potential, could improve muscle bioenergetics and resilience to fatigue (Barbieri et al., 2016; Ostojic and Rátgéber, 2025), which are often impaired in sarcopenia and other muscle-wasting disorders. There is also evidence suggesting creatine enhances neuromuscular function, potentially improving synaptic efficiency (Bian et al., 2023) and muscle activation (Farshidfar et al., 2017), as reflected in better handgrip strength outcomes, even without physical training. Together, these mechanisms suggest that creatine can act as a low-threshold, non-exercise-based intervention to support muscle mass and function, particularly in populations where exercise is limited or contraindicated. While these effects are generally less pronounced compared to when creatine is combined with resistance training, they still hold clinical relevance. Most evidence to date is derived from cellular, animal, or short-term human studies, and more research is needed to confirm long-term efficacy and optimal dosing in non-exercising populations. Importantly, future studies should aim to dissect the relative contribution of each mechanism (bioenergetic, anabolic, anti-catabolic, neuromuscular, and mitochondrial) to fully understand how creatine exerts its muscle-supporting effects independently of physical activity. As with all cross-sectional analyses, our findings do not establish causality; rather, they identify robust population-level associations that generate biologically grounded hypotheses to be tested in longitudinal and interventional studies.
Although the quartile analysis revealed a generally monotonic increase in both lean body mass and handgrip strength across increasing levels of creatine intake, the pattern was not perfectly linear at the lowest exposure range, with Q2 exhibiting slightly lower mean handgrip strength than Q1. Importantly, this difference was not statistically significant and should be interpreted as random variation rather than evidence of a true inverse effect. Such minor non-monotonic fluctuations are common in large epidemiological datasets, particularly when exposure is derived from a single 24-h dietary recall and categorized into discrete strata. Day-to-day variability in meat consumption, residual confounding by unmeasured factors (e.g., occupation, illness, or transient energy imbalance), and heterogeneity within quartiles may all contribute to local irregularities. The overall dose-response relationship remains positive and robust, as confirmed by the continuous regression models demonstrating a significant linear association between creatine intake and handgrip strength across the full exposure range.
Both crude and adjusted linear regression analyses stratified by age demonstrated a consistent positive association between dietary creatine intake and lean body mass excluding BMC across children, adults, and older adults, and with handgrip strength in children and adults. In contrast, within the older adult subgroup, the association between creatine intake and handgrip strength was attenuated and no longer statistically significant after full adjustment. This pattern does not negate the overall relationship observed in the total sample but rather highlights the complexity of muscle function in later life. Handgrip strength in older adults is strongly influenced by multimorbidity, neuromuscular impairment, medication use, frailty status, and age-related endocrine changes, factors that may overshadow modest nutritional effects in cross-sectional models. Importantly, the persistence of a significant association with lean body mass in older adults suggests that dietary creatine remains linked to structural aspects of muscle, even when functional expression becomes more heterogeneous. The dissociation between mass and strength in aging is well recognized and reflects altered neuromuscular efficiency, motor unit remodeling, and impaired contractile quality. In this context, the null finding for handgrip strength likely reflects biological and methodological noise rather than the absence of a creatine-related signal. Older adults may also exhibit reduced responsiveness to dietary creatine due to impaired muscle uptake, altered mitochondrial function, or anabolic resistance (Chilibeck et al., 2017) and reduced creatine transporter expression (Candow et al., 2025), further dampening observable cross-sectional associations. These findings underscore that nutritional effects on muscle function in late life are more difficult to detect using single-day dietary recalls and simple functional proxies. Rather than undermining the public health relevance of creatine, the age-stratified results emphasize that muscle strength in older adults is shaped by a broader and more dominant set of determinants than in younger populations. Longitudinal and interventional studies with phenotypic stratification, direct measures of intramuscular creatine, and multidimensional functional outcomes will be required to resolve whether dietary creatine can meaningfully modify functional trajectories in aging.
Our study offers a robust analysis of nationally representative data, providing valuable insights into the relationship between dietary creatine intake and markers of muscle mass and strength across the lifespan. However, several methodological limitations should be acknowledged when interpreting these findings. First, the cross-sectional nature of the NHANES data limits the ability to establish causality between dietary creatine intake and measures of muscle mass and strength; associations identified may reflect correlations rather than directional effects. Second, dietary creatine intake was estimated by applying population-average creatine content values to foods reported in a single 24-h dietary recall. This approach entails several important limitations. First, the use of average creatine concentrations does not capture substantial variability arising from food type and preparation. Creatine content differs markedly across animal sources and is sensitive to cooking and processing, as creatine partially degrades with heat exposure (for a detailed review, see Ostojic, 2025). In addition, dietary creatine intake was derived from a single in-person 24-h dietary recall in the harmonized NHANES dataset, as several survey cycles provide only one recall assessment. While this approach is standard in large epidemiological analyses, a single day of intake may not accurately reflect an individual's habitual consumption, particularly for a nutrient such as creatine whose intake is episodic and highly dependent on day-to-day food choices. This reliance on a single recall is therefore subject to random within-person variability and recall bias, which may lead to exposure misclassification. Such error is expected to be largely non-differential with respect to the study outcomes and would tend to attenuate true associations rather than create spurious effects. Nevertheless, the estimated values should be interpreted as approximations of usual dietary creatine exposure at the population level rather than precise individual intake measures. Moreover, the present analysis did not include creatine obtained from dietary supplements or pharmacological sources, which may have led to an underestimation of total creatine exposure in the population. This decision was based on the relatively low prevalence of creatine supplement use in the general population, estimated at approximately 0.9% over a one-week period among U.S. adults (Kaufman et al., 2002). Nonetheless, supplement users may represent a distinct subgroup with different exposure patterns and physiological profiles. Future studies should specifically examine whether habitual creatine supplementation is associated with differential musculoskeletal or clinical outcomes compared with non-consumers. In addition, although NHANES dietary data undergo standardized quality control, single-day recalls may include occasional misreporting, particularly at the extremes of intake. Very high reported creatine values likely reflect rare but biologically feasible patterns of meat or fish consumption, although some degree of reporting error cannot be excluded. We did not impose exclusion thresholds based on energy intake; as such cutoffs are inherently arbitrary and may distort the upper tail of the exposure distribution. Nevertheless, future analyses should incorporate sensitivity testing that excludes implausible reporters to confirm the robustness of these associations. Importantly, although certain laboratory measures were available, circulating and muscle creatine concentrations were not assessed, and creatinine—while measured—is an imprecise proxy for muscle mass and not a reliable indicator of total body creatine stores. As a result, our analyses could not distinguish the relative contributions of endogenous creatine synthesis and exogenous dietary intake to the observed musculoskeletal outcomes. This limitation introduces uncertainty into the causal interpretation of the findings. Future research incorporating direct measures of circulating creatine, stable isotope tracer methodologies, or more specific biomarkers of creatine status is warranted to better elucidate the role of dietary creatine in modulating muscle mass and strength. Third, the availability of key outcome measures (e.g., DXA-derived body composition and handgrip strength) was restricted to specific age groups and NHANES cycles, reducing the analytic sample size and potentially introducing selection bias while limiting comparability across analyses. Additionally, proxy respondents provided dietary data for younger children, which may have introduced measurement error. The use of different DXA software versions and testing protocols across survey cycles may have also introduced variability in body composition estimates. Despite statistical adjustment for several important confounders (including dietary intake, demographics, sex hormones, and physical activity), residual confounding by unmeasured variables cannot be ruled out. An additional methodological limitation is that the analyses did not incorporate NHANES survey weights or complex design variables (strata and primary sampling units). Because NHANES employs a multistage probability sampling framework, unweighted analyses may yield biased population estimates and underestimated standard errors. Consequently, the present findings should be interpreted as describing within-sample associations between dietary creatine intake and musculoskeletal outcomes rather than as population-representative effects for the U.S. population. Future studies should confirm these relationships using fully survey-weighted models. Lastly, the NHANES survey samples only the non-institutionalized U.S. population, limiting the generalizability of results to institutionalized individuals or populations outside the United States.
Conclusion
In this nationally representative cross-sectional study encompassing over 100,000 individuals across 25 years of NHANES data, we found robust and consistent associations between higher dietary creatine intake and greater total lean body mass and handgrip strength, independent of key confounding factors such as exercise. These findings suggest that habitual creatine consumption through the diet may serve as a modifiable nutritional strategy to support musculoskeletal health across diverse populations, including those unable or unwilling to engage in structured exercise. Importantly, the findings are in line with proposed mechanisms of creatine action—such as enhanced bioenergetics, anabolic signaling, and anti-catabolic effects—although their relevance in this context and relative contributions require further investigation. Despite several methodological limitations inherent to the observational design and dietary recall data, this study adds to the growing body of evidence suggesting that creatine may positively influence muscle health outside of exercise contexts. Future longitudinal and interventional research is needed to confirm causality, refine intake recommendations, and clarify mechanistic pathways, ultimately informing public health strategies and clinical guidelines for the prevention of sarcopenia and related conditions.
Footnotes
Acknowledgements
SMO expresses gratitude to VV Nabokov for his transformative works.
Statement of ethics
Ethical approval for the NHANES study was granted by the U.S. National Center for Health Statistics Ethics Review Board (#98–12, #2005–06, Continuation of Protocol #2005–06, #2011–17, Continuation of Protocol #2011–17, #2018-01, Continuation of Protocol #2018-01, and #2021–05)
Author contributions
The authors’ responsibilities were as follows: SMO: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Writing-original draft; Writing-review and editing. DGC: Investigation; Methodology; Writing-review and editing. LR: Data curation; Formal analysis; Investigation; Methodology; Writing-review and editing. JB: Data curation; Investigation; Supervision; Methodology; Writing-review and editing. PA: Data curation; Investigation; Methodology; Supervision; Writing-review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SMO serves as a member of the Scientific Advisory Board on Creatine in Health and Medicine (AlzChem LLC). SMO co-owns patent “Supplements Based on Liquid Creatine” at the European Patent Office (WO2019150323 A1) and patent application “Composition Comprising Creatine for Use in Telomere Lengthening” at the U.S. Patent and Trademark Office (# 18/934,264). SMO has received research funding related to creatine from various public funding agencies and industry partners. SMO is the co-founder of KRE-ALL, a company developing creatine-enriched food products, and the founder of INOVA Nutrition, a biotechnology startup focused on innovative nutraceuticals.DGC has received research grants and performed industry sponsored research involving creatine supplementation, received creatine donation for scientific studies and travel support for presentations involving creatine supplementation at scientific conferences. In addition, DGC serves on the Scientific Advisory Board for Alzchem and Create (companies which manufacture creatine) and the editorial review board for the Journal of the International Society of Sports Nutrition. DGC is also a sports science advisor to the International Society of Sports Nutrition and serves as an expert witness/consultant in legal cases involving creatine supplementation. LR, JB and PA declare no known competing financial interests or personal relationships that could have appeared to influence the authorship of this paper.