
Abstract
Background and aims
Computed tomography (CT)-derived measures of low muscle quantity and quality may indicate reduced physiologic reserve, but their prognostic value after isolated coronary artery bypass grafting (CABG) is uncertain. We conducted a PRISMA-guided systematic review and conservative meta-analysis of adjusted estimates to examine associations between preoperative CT-derived low muscle status and outcomes after isolated CABG.
Methods
We searched PubMed, Embase, Web of Science, Cochrane CENTRAL, and ClinicalTrials.gov from inception to December 23, 2025. Cohort studies of adults undergoing isolated CABG were eligible if they assessed preoperative low muscle status using CT (dual-energy X-ray absorptiometry eligible) and reported mortality and/or postoperative complications. Overlapping cohorts were excluded. Adjusted hazard ratios (HRs) were pooled using random-effects meta-analysis (restricted maximum likelihood) with the Hartung–Knapp–Sidik–Jonkman adjustment.
Results
Four independent cohorts (n = 3931) met inclusion criteria and used CT-based definitions spanning lumbar and thoracic muscle quantity/quality measures. Three cohorts (n = 3452) contributed adjusted estimates for long-term mortality. Across studies, the direction of association was unfavorable, but quantitative synthesis was exploratory and highly uncertain (pooled HR 2.71, 95% confidence interval 0.38–19.40; I2 = 92.3%; approximate 95% prediction interval 0.47–15.6). Secondary outcomes were too heterogeneous for pooling and were summarized narratively.
Conclusions
Preoperative CT-derived low muscle status may serve as a pragmatic vulnerability flag in isolated CABG when CT is already available, but current pooled evidence for long-term mortality remains exploratory, highly heterogeneous, and statistically imprecise. Standardized measurement, more comparable adjustment strategies, and harmonized outcome reporting are needed before broader clinical translation.
This is a visual representation of the abstract.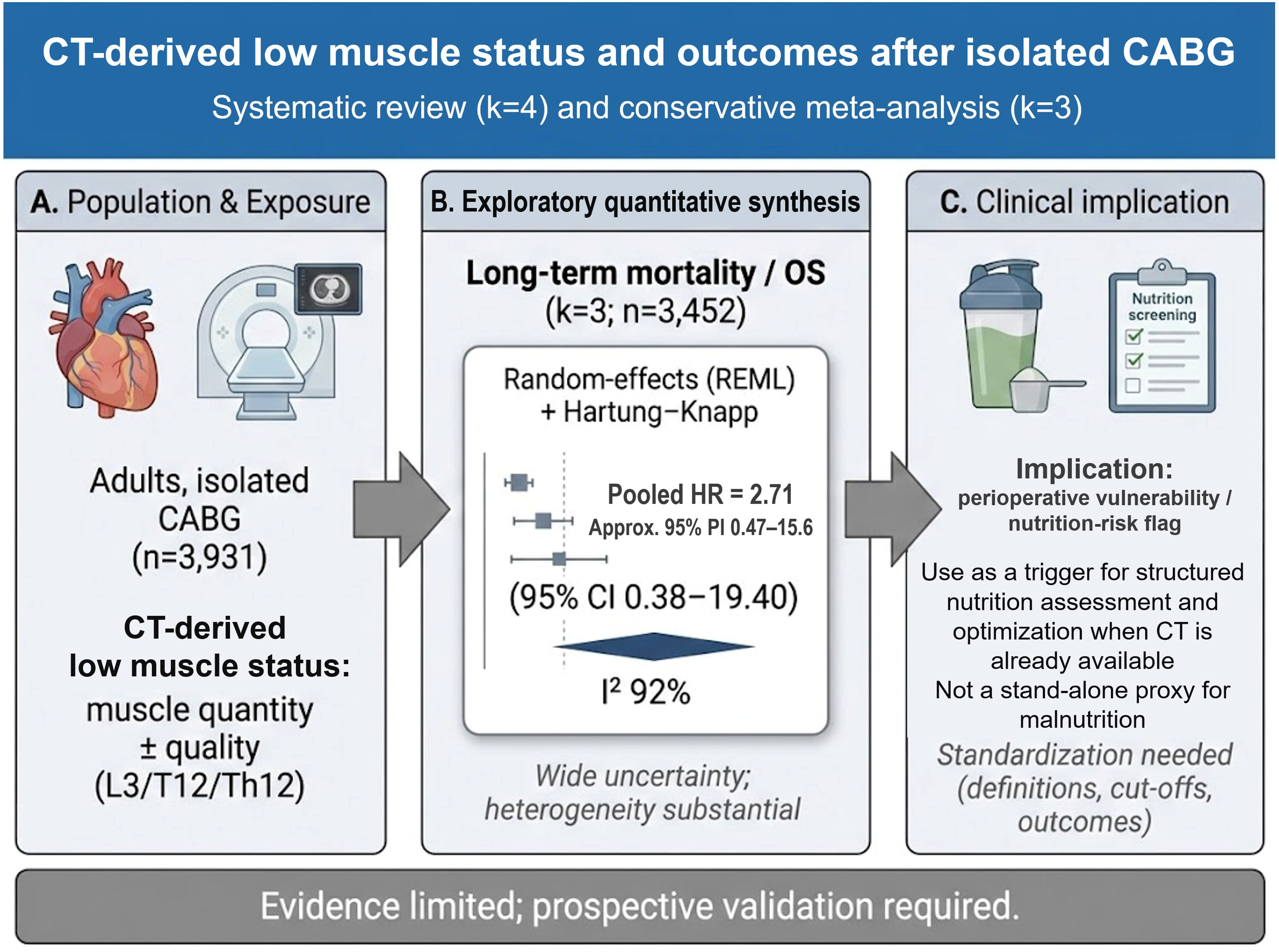
Keywords
Introduction
Coronary artery disease remains a leading contributor to global morbidity and mortality, and coronary artery bypass grafting (CABG) continues to play a central role in revascularization—particularly for complex multivessel disease—alongside percutaneous strategies. Contemporary myocardial revascularization guidelines emphasize CABG as a durable option in selected anatomical and clinical settings, yet outcomes remain strongly influenced by baseline vulnerability and physiologic reserve rather than procedural factors alone (Lawton et al., 2022; Neumann et al., 2019; Roth et al., 2020).
Risk stratification for cardiac surgery is well established through models such as the Society of Thoracic Surgeons (STS) risk models and EuroSCORE II, which support benchmarking and clinical decision-making (Nashef et al., 2012; Shahian et al., 2018). However, these models were not designed to directly quantify nutrition-related phenotypes or body composition, and may underrepresent elements of physiologic reserve that are potentially modifiable in the preoperative period (Nashef et al., 2012; Shahian et al., 2018). The incremental prognostic information offered by geriatric vulnerability measures (e.g., frailty) beyond traditional surgical risk scores further underscores this gap in capturing reserve-related risk (Afilalo et al., 2012; Shahian et al., 2018).
Sarcopenia is a progressive skeletal muscle disorder that is consistently linked to frailty, disability, and mortality across clinical populations. In the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), low muscle strength is the primary determinant, with low muscle quantity/quality used to confirm the diagnosis and physical performance used for severity staging (Cruz-Jentoft et al., 2019). In routine surgical practice—especially in retrospective cardiac surgery cohorts—strength and performance metrics are rarely available. As a result, imaging-derived measures of muscle quantity (e.g., skeletal muscle index, SMI; psoas muscle index, PMI) and muscle quality (e.g., radiodensity or myosteatosis proxies) are commonly operationalized as pragmatic computed tomography (CT)-derived low muscle phenotypes to identify higher-risk patients (Aubrey et al., 2014; Chen et al., 2020; Cruz-Jentoft et al., 2019; Goodpaster et al., 2000; Mourtzakis et al., 2008; Paris et al., 2020).
This approach may also be interpreted within a Clinical Nutrition framework, provided that CT-derived low muscle status is not treated as synonymous with malnutrition. The Global Leadership Initiative on Malnutrition (GLIM) criteria recognize reduced muscle mass as a phenotypic criterion for malnutrition diagnosis, reinforcing the intersection between body composition and nutrition-related risk (Cederholm et al., 2019). In parallel, the European Society for Clinical Nutrition and Metabolism (ESPEN) guidance for surgical patients emphasizes early identification of nutrition risk and targeted perioperative interventions to reduce complications and support recovery (Weimann et al., 2021). Thus, when CT imaging is already available as part of the preoperative workup, opportunistic muscle assessment may offer an objective, scalable method to enrich perioperative nutrition risk stratification and to prioritize patients for structured nutrition assessment and prehabilitation pathways (Cederholm et al., 2019; Grant et al., 2024; Paris et al., 2020; Weimann et al., 2021).
In isolated CABG populations, several cohort studies have reported associations between preoperative CT-derived low muscle mass or myosteatosis proxies and adverse outcomes, including long-term mortality and postoperative complications (Krombholz-Reindl et al., 2024; Lee et al., 2024; Okamura et al., 2020; Shen et al., 2023). However, the evidence base remains small and methodologically heterogeneous: anatomical landmarks vary (lumbar vs. thoracic), muscle constructs differ (quantity vs. quality), cut-offs are derived using different strategies, and postoperative outcomes are not uniformly harmonized. These features create a practical tension: the clinical question is actionable for perioperative nutrition care, but quantitative synthesis must be conservative and transparent to avoid overinterpretation when the number of independent cohorts is limited.
Therefore, we conducted a PRISMA-guided systematic review and a conservative random-effects meta-analysis of adjusted estimates to evaluate the association between preoperative CT-derived low muscle status and clinical outcomes after adult isolated CABG (Page et al., 2021), and we interpret the findings in the context of perioperative nutrition risk stratification and the need for standardized measurement and reporting (Roth et al., 2020).
Methods
Reporting standard and protocol
This systematic review and meta-analysis was conducted and reported in accordance with the PRISMA 2020 statement (Page et al., 2021). An a priori protocol was developed to guide the review process (search strategy, eligibility criteria, study selection procedures, data extraction plan, and statistical approach) and was applied consistently throughout. The protocol was not prospectively registered.
Data sources and search strategy
We searched PubMed, Embase, Web of Science Core Collection, Cochrane CENTRAL, and ClinicalTrials.gov from inception to the final search dates. The PubMed search was conducted on December 17, 2025 and restricted to human and English-language records using database filters. Searches in Embase, Web of Science, CENTRAL, and ClinicalTrials.gov were conducted on December 23, 2025. Search strategies combined controlled vocabulary (e.g., MeSH/Emtree were supported by the interface) and free-text terms for: (1) the population (isolated CABG/coronary artery bypass/coronary revascularization) and (2) imaging-derived muscle constructs (e.g., sarcopenia/low skeletal muscle mass, SMI, PMI, radiodensity, myosteatosis, muscle attenuation; CT/dual-energy X-ray absorptiometry (DXA)). Full electronic search strategies for each database, including the exact syntax and limits as executed, are provided in the Supplemental materials.
Language restrictions differed by database as implemented in each search interface and are documented in the search record: PubMed applied an English-language filter; Web of Science applied an English-language restriction; no language restriction was applied in Embase, CENTRAL, or ClinicalTrials.gov. To maintain a reproducible, database-driven identification process, we did not perform backward reference-list screening or forward citation tracking.
Eligibility criteria
We included original cohort studies of adults (≥18 years) undergoing isolated CABG that: (i) assessed preoperative sarcopenia or low skeletal muscle status using CT- or DXA-derived measures (e.g., SMI/PMI or radiodensity-based metrics), and (ii) reported at least one clinically relevant outcome, including mortality and/or postoperative complications.
We excluded studies that: (i) did not involve isolated CABG populations (e.g., mixed cardiac surgery without separable CABG subgroup), (ii) did not quantify preoperative muscle status, (iii) did not report eligible outcomes, (iv) were not original research (e.g., reviews, editorials), or (v) represented overlapping cohorts such that independence could not be ensured.
Study selection and handling of duplicates/overlapping cohorts
All identified records were imported into Rayyan for de-duplication and screening (Ouzzani et al., 2016). After de-duplication, 988 unique records underwent title/abstract screening, and 45 records were retrieved for full-text assessment. After full-text assessment, nine articles met eligibility criteria prior to assessment of cohort overlap; five were subsequently excluded due to duplicate/overlapping cohorts, leaving four independent cohort studies for inclusion. Reasons for exclusion were recorded at each stage (Figure 1).
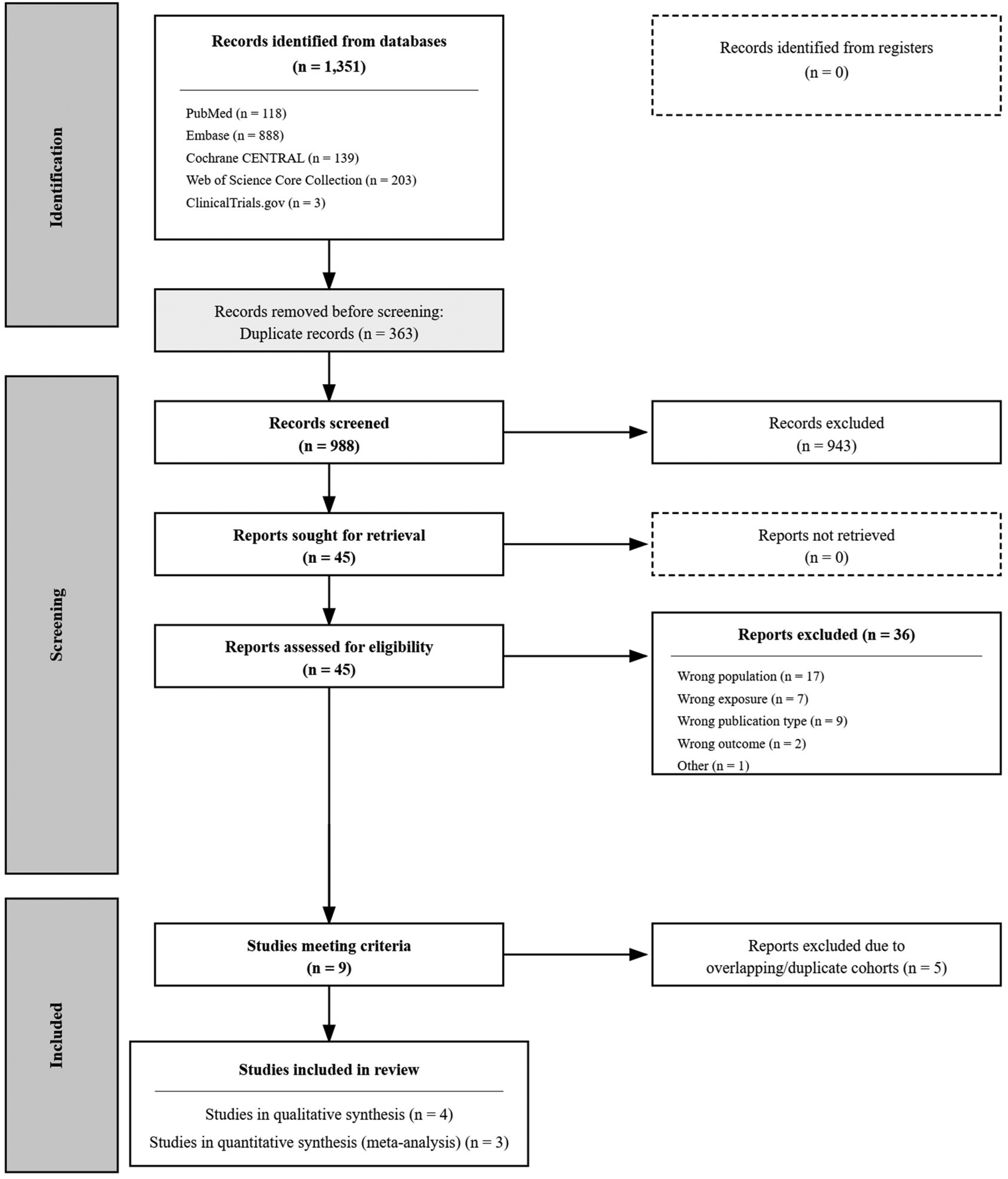
PRISMA flow diagram. Flow diagram summarizing study identification, screening, eligibility, and inclusion, including removal of overlapping cohorts.
Two reviewers independently screened titles/abstracts and full texts using prespecified criteria. Disagreements were resolved by discussion and consensus; when consensus could not be reached, a third reviewer adjudicated.
To ensure cohort independence, we assessed potential overlap using study center(s), enrollment years, inclusion/exclusion criteria, sample size, and reported baseline characteristics. When multiple publications appeared to derive from the same underlying cohort, we retained the single most informative report for the relevant outcome(s) (typically the report with the clearest exposure definition, the most complete multivariable adjustment, and/or the most complete follow-up) and excluded overlapping reports from quantitative synthesis.
Data extraction
A standardized extraction form was developed a priori and piloted to ensure consistent capture of key variables. Two reviewers extracted: study characteristics (design, setting, enrollment years, sample size), patient characteristics, imaging modality and timing, exposure definitions (anatomical level, muscle metric(s), normalization, cut-off rationale, thresholds), outcome definitions and ascertainment, and effect estimates (including covariate-adjusted models). Extracted data were cross-checked against source articles; discrepancies were resolved by consensus with third-reviewer adjudication as needed.
For time-to-event outcomes, we prioritized adjusted hazard ratios (HRs) with the corresponding 95% confidence intervals (CIs) from the most fully adjusted model that remained clinically interpretable and not overspecified. For non-time-to-event outcomes, we extracted adjusted effect estimates as reported (e.g., odds ratios (ORs) for complications). When reporting formats were incompatible or effect estimates were not extractable with uncertainty (e.g., absence of HRs and CIs), studies were retained for qualitative synthesis only. To improve transparency regarding comparability of adjustment, covariates included in the selected adjusted models are summarized in Supplemental S6.
Exposure terminology
For terminological precision, we preferentially use “CT-derived low muscle status” to describe radiologically defined low muscle quantity and/or quality proxies. We retained study-specific terminology when summarizing the original reports, including instances in which the source articles used the term “sarcopenia.” Because functional assessments required by consensus diagnostic frameworks were not available in the included CABG cohorts, this review does not treat CT findings alone as a clinical diagnosis of sarcopenia (Cruz-Jentoft et al., 2019). We discuss these imaging phenotypes within a perioperative nutrition-risk context because low muscle status may contribute to physiologic vulnerability, but we do not equate CT-defined low muscle status with malnutrition per se (Cederholm et al., 2019).
Outcomes
The primary quantitative outcome was long-term all-cause mortality/overall survival, summarized as an adjusted HR. Secondary outcomes included postoperative complications and composite cardiovascular end points (e.g., major adverse cardiac and cerebrovascular events (MACCE)/MACCE-like outcomes), as defined in each study. Outcomes were meta-analyzed only when definitions, follow-up structure, and reporting formats were sufficiently comparable.
Risk of bias assessment
Risk of bias of included observational cohort studies was assessed using the Newcastle–Ottawa Scale, which evaluates study quality across selection, comparability, and outcome domains (Wells et al., 2014). Risk-of-bias judgments were used to inform interpretation rather than to exclude studies based solely on score.
Statistical analysis
When ≥2 studies reported comparable adjusted time-to-event estimates for long-term mortality/overall survival, we pooled log-transformed HRs using a random-effects model. Effect estimates for ratio measures (HRs and ORs) were pooled on the natural logarithmic scale, with the corresponding standard errors derived from reported CIs. Between-study variance (τ2) was estimated using restricted maximum likelihood (REML). Given the small number of studies and expected clinical heterogeneity (anatomical level, muscle quantity vs. quality proxies, and cut-off derivation), we used the Hartung–Knapp–Sidik–Jonkman (HKSJ) adjustment when constructing CIs (Hartung and Knapp, 2001; IntHout et al., 2014; Rover et al., 2015). Heterogeneity was summarized using I2 and τ2. Formal assessment of small-study effects/publication bias was not performed because the number of studies was insufficient for meaningful inference.
Prespecified sensitivity analyses included leave-one-out analyses and substitution of alternative adjusted estimates within a study when available. Meta-analysis was not performed for outcomes with incompatible definitions or reporting formats. Analyses were performed in R using the metafor package (Viechtbauer, 2010).
Results
Study selection
Across databases, 1351 records were identified. After deduplication, 988 unique records underwent title/abstract screening, yielding 45 records for full-text assessment. Nine reports met eligibility criteria after full-text review; after assessment of cohort overlap, five were excluded due to duplicate/overlapping cohorts, leaving four independent cohort studies for qualitative synthesis (Figure 1).
Study and exposure characteristics
The four included studies (total n = 3931) (Krombholz-Reindl et al., 2024; Lee et al., 2024; Okamura et al., 2020; Shen et al., 2023) were single-center retrospective cohorts from South Korea, Japan, Austria, and China, enrolling adults undergoing isolated CABG with preoperative CT-based assessment of muscle status (Table 1). Exposure definitions were heterogeneous (Table 2), spanning muscle quantity indices (L3 SMI, L3 PMI, T12 SMI) and a muscle quality proxy (T12 Hounsfield unit average calculation (HUAC)). In this review, the term “CT-derived low muscle status” was used as a pragmatic umbrella label for these heterogeneous CT-defined low-muscle phenotypes, spanning both quantity-based measures (L3 SMI, L3 PMI, T12 SMI) and a radiodensity-related quality proxy (T12 HUAC). This integration was intended to support cautious synthesis across a sparse evidence base, while recognizing that these measures are not anatomically or biologically identical. The prevalence of CT-derived low muscle status ranged from 13.0% to 32.9% (Table 2). The CT-to-surgery interval was explicitly defined in two studies (≤3 months and ≤1 month), whereas two studies described CT as part of routine/standard preoperative workup without specifying a maximum interval (Table 1).
Characteristics of included cohort studies of CT-derived low muscle status in adults undergoing isolated CABG.
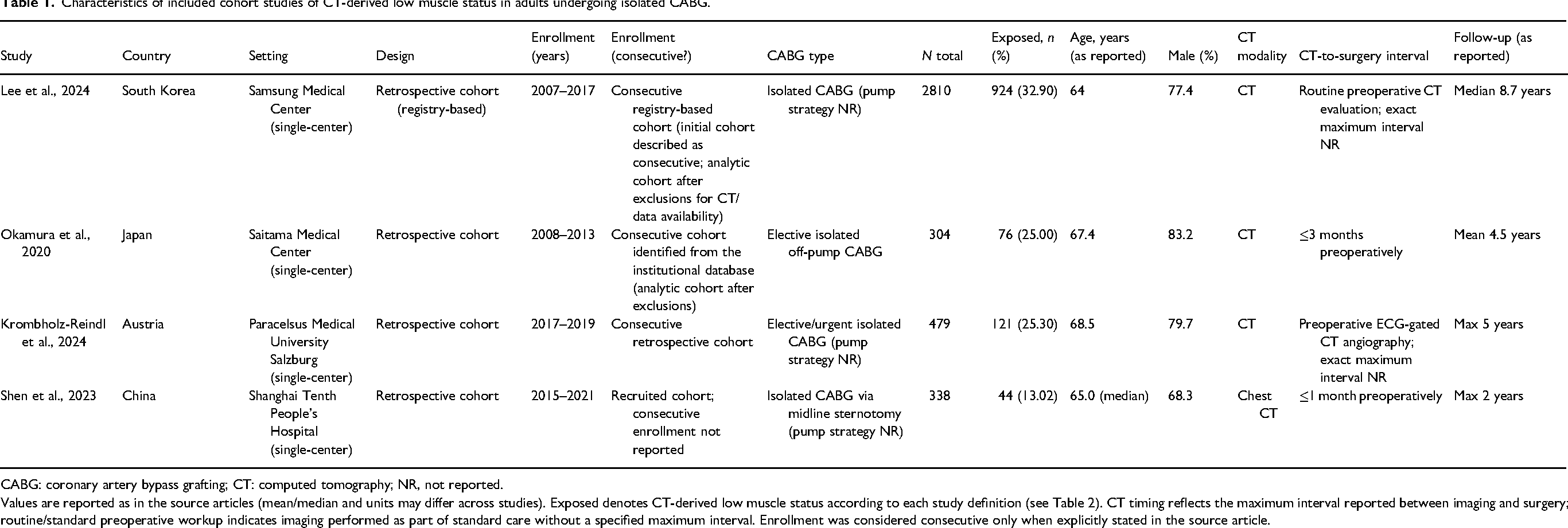
CABG: coronary artery bypass grafting; CT: computed tomography; NR, not reported.
Values are reported as in the source articles (mean/median and units may differ across studies). Exposed denotes CT-derived low muscle status according to each study definition (see Table 2). CT timing reflects the maximum interval reported between imaging and surgery; routine/standard preoperative workup indicates imaging performed as part of standard care without a specified maximum interval. Enrollment was considered consecutive only when explicitly stated in the source article.
Definitions of CT-derived low muscle status across included studies (anatomical level, construct, cut-off derivation, and prevalence).
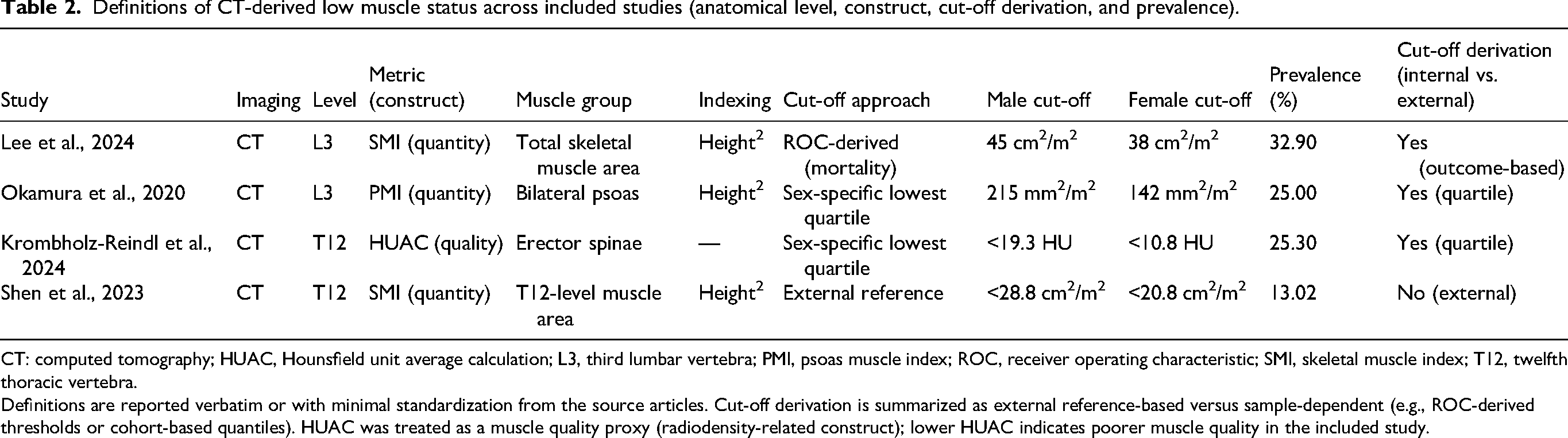
CT: computed tomography; HUAC, Hounsfield unit average calculation; L3, third lumbar vertebra; PMI, psoas muscle index; ROC, receiver operating characteristic; SMI, skeletal muscle index; T12, twelfth thoracic vertebra.
Definitions are reported verbatim or with minimal standardization from the source articles. Cut-off derivation is summarized as external reference-based versus sample-dependent (e.g., ROC-derived thresholds or cohort-based quantiles). HUAC was treated as a muscle quality proxy (radiodensity-related construct); lower HUAC indicates poorer muscle quality in the included study.
Primary outcome: long-term all-cause mortality/overall survival
Three studies (Lee et al., 2024; Okamura et al., 2020; Shen et al., 2023; Table 3) reported adjusted time-to-event associations for long-term mortality/overall survival that were sufficiently comparable for pooling (k = 3; total n = 3452; Table 3). In a random-effects meta-analysis (REML with HKSJ adjustment), CT-derived low muscle status was compatible with higher long-term mortality, but the pooled estimate was imprecise (pooled HR 2.71, 95% CI 0.38–19.40; I2 = 92.3%; Figure 2 and Table 3). Substantial between-study heterogeneity was observed (τ2 = 0.58 on the log scale), consistent with differences in anatomical level (lumbar vs. thoracic), construct (quantity vs. quality proxies), and cut-off derivation strategy (Table 2). The approximate 95% prediction interval ranged from HR 0.47 to 15.6, underscoring that the true effect in a future study could vary widely. Given the marked heterogeneity in anatomical level, construct (quantity vs. quality), and cut-off derivation, this pooled HR should be interpreted as an exploratory, signal-generating summary of direction and uncertainty under a conservative random-effects framework, not as a single transportable effect size. Leave-one-out analyses suggested that heterogeneity was largely driven by Lee et al. (2024): omitting this study yielded a pooled HR of 4.46 (95% CI 2.72–7.30) with I2 = 0% and τ2 = 0, whereas omission of the other studies retained substantial heterogeneity (Supplemental S3).
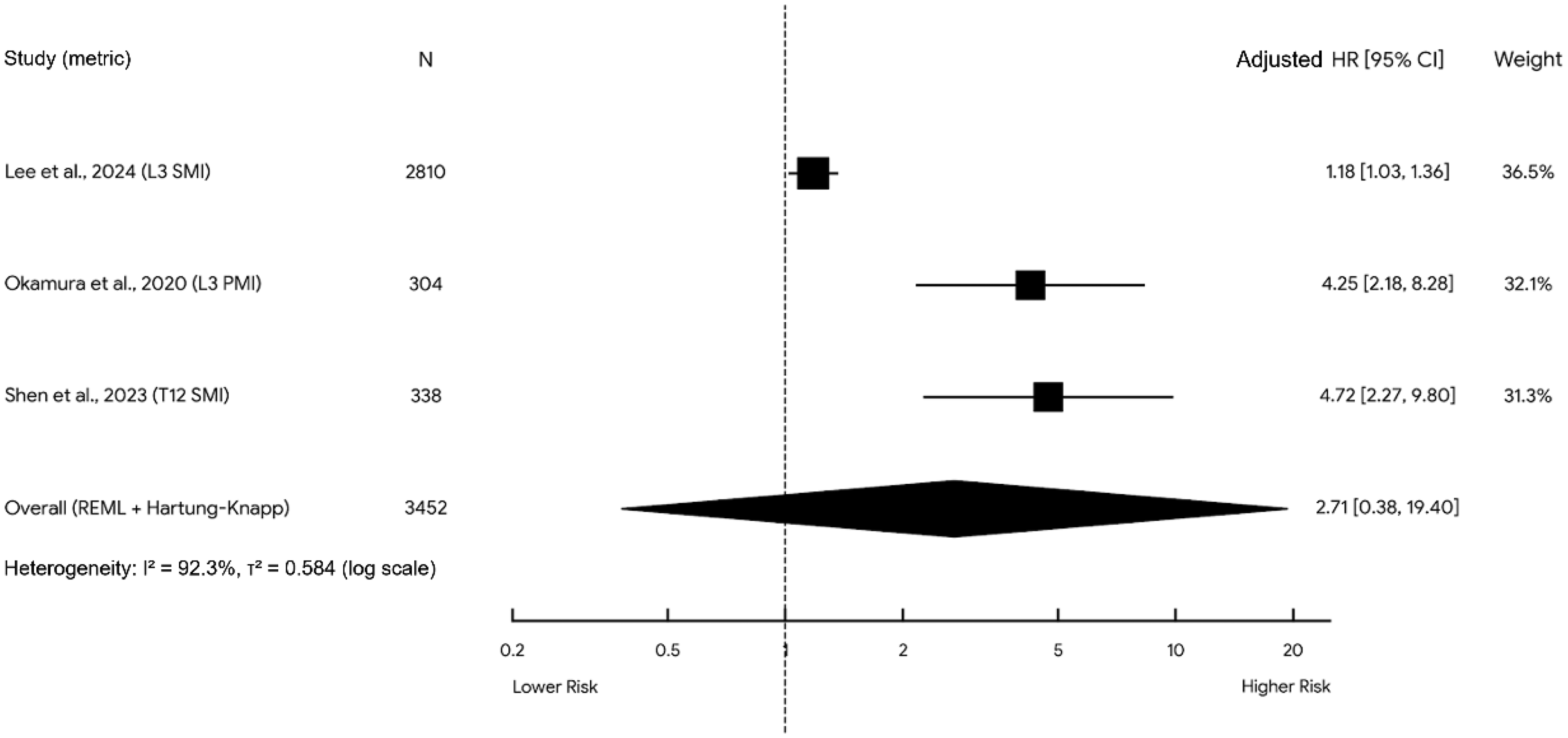
Association between CT-derived low muscle status and long-term mortality after isolated CABG. Random-effects meta-analysis of adjusted hazard ratios (REML). Given the small number of studies (k = 3), confidence intervals were calculated using the Hartung–Knapp adjustment. CT-derived low muscle status was directionally associated with higher long-term mortality, but the pooled estimate should be interpreted as exploratory because heterogeneity was substantial (HR 2.71, 95% CI 0.38–19.40; I2 = 92.3%; τ2 = 0.58 on the log scale; approximate 95% prediction interval HR 0.47–15.6). Squares represent study-specific estimates (size proportional to random-effects weight), and the diamond denotes the pooled effect. CABG: coronary artery bypass grafting; CI: confidence interval; HR: hazard ratio; HKSJ: Hartung–Knapp–Sidik–Jonkman; PMI: psoas muscle index; SMI: skeletal muscle index; CT: computed tomography; REML: restricted maximum likelihood.
Summary of associations between CT-derived low muscle status and clinical outcomes after isolated CABG.
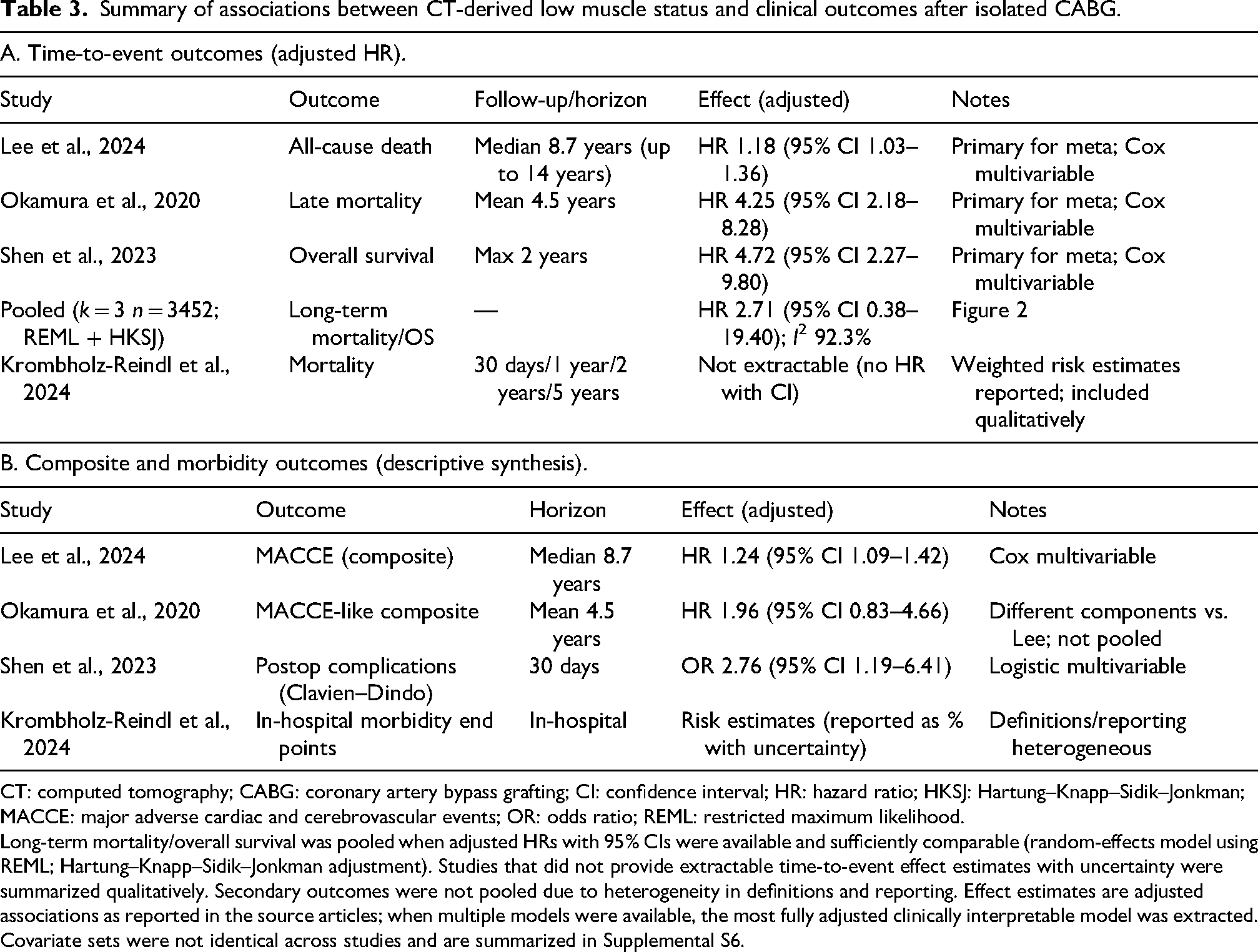
CT: computed tomography; CABG: coronary artery bypass grafting; CI: confidence interval; HR: hazard ratio; HKSJ: Hartung–Knapp–Sidik–Jonkman; MACCE: major adverse cardiac and cerebrovascular events; OR: odds ratio; REML: restricted maximum likelihood.
Long-term mortality/overall survival was pooled when adjusted HRs with 95% CIs were available and sufficiently comparable (random-effects model using REML; Hartung–Knapp–Sidik–Jonkman adjustment). Studies that did not provide extractable time-to-event effect estimates with uncertainty were summarized qualitatively. Secondary outcomes were not pooled due to heterogeneity in definitions and reporting. Effect estimates are adjusted associations as reported in the source articles; when multiple models were available, the most fully adjusted clinically interpretable model was extracted. Covariate sets were not identical across studies and are summarized in Supplemental S6.
Across the three mortality cohorts, all adjusted HRs were greater than 1.0, but the effect magnitude varied substantially, from a modest association in the largest L3 SMI cohort to larger estimates in the smaller L3 PMI and T12 SMI cohorts. Secondary outcomes also showed an unfavorable pattern, although end-point definitions and follow-up structures were not sufficiently aligned for pooling. This consistency in direction, despite marked variation in measurement site, construct, and threshold derivation, supports cautious narrative interpretation rather than overreliance on a single pooled value.
A fourth cohort (Krombholz-Reindl, 2024; Krombholz-Reindl et al., 2024) reported mortality as weighted event rates at multiple fixed horizons (30 days, 1 year, 2 years, and 5 years) but did not provide extractable time-to-event effect estimates with CIs; therefore, it was retained for qualitative synthesis only (Table 3).
Secondary outcomes
Secondary outcomes were variably defined and inconsistently reported, precluding quantitative synthesis. Composite cardiovascular end points (MACCE/MACCE-like outcomes) were reported in two studies with different component definitions and follow-up structures; these were summarized descriptively (Table 3). One study reported a higher postoperative complication burden (Clavien–Dindo grade ≥II) among patients with thoracic sarcopenia (adjusted OR 2.76, 95% CI 1.19–6.41; Table 3).
Discussion
Principal findings
In this PRISMA-guided systematic review restricted to adults undergoing isolated CABG, preoperative CT-derived low muscle status was directionally associated with worse postoperative prognosis across independent cohorts (Krombholz-Reindl et al., 2024; Lee et al., 2024; Okamura et al., 2020; Shen et al., 2023). In the conservative meta-analysis of adjusted survival estimates, the pooled association was directionally consistent with higher long-term mortality, but statistical uncertainty was substantial and between-study heterogeneity was high. The approximate 95% prediction interval ranged from HR 0.47 to 15.6, underscoring that the true effect in a future study could vary widely. Accordingly, the pooled HR is best interpreted as exploratory and hypothesis-generating, summarizing direction and uncertainty across sparse and heterogeneous cohorts rather than providing a single transportable effect size. Secondary outcomes, including postoperative complications and MACCE/MACCE-like end points, were also directionally unfavorable in patients with low muscle status, but could not be pooled because outcome definitions, follow-up structures, and reporting formats were not aligned across studies (Krombholz-Reindl et al., 2024; Lee et al., 2024; Okamura et al., 2020; Shen et al., 2023). This synthesis should therefore be understood as a pragmatic integration of related but nonequivalent CT-derived low-muscle phenotypes, rather than as evidence that L3 SMI, L3 PMI, T12 SMI, and HUAC represent interchangeable constructs. Taken together, current evidence supports cautious narrative interpretation and the need for standardized measurement and harmonized outcome reporting before more definitive quantitative inference is possible.
Contribution of the present review
This review contributes to the literature in several ways. First, by restricting inclusion to isolated CABG and explicitly removing overlapping cohorts, we synthesized evidence from independent datasets and reduced the risk of double-counting, which can otherwise inflate apparent precision in small evidence bases. Second, we integrated studies capturing both muscle quantity (e.g., SMI/PMI) and muscle quality proxies (radiodensity/myosteatosis-related measures), consistent with contemporary CT-based body composition assessment where “quality” may add prognostic information beyond area-based indices (Goodpaster et al., 2000; Mourtzakis et al., 2008); radiodensity/attenuation is a recognized muscle-quality phenotype with established biological and technical determinants (Aubrey et al., 2014; Engelke et al., 2018). Third, we prespecified and implemented a conservative synthesis strategy tailored to few studies and expected heterogeneity: pooling only clinically comparable adjusted time-to-event estimates, performing analyses on the log scale, using REML for τ2 estimation, and applying the HKSJ adjustment to avoid false precision (Hartung and Knapp, 2001; IntHout et al., 2014; Jackson et al., 2017; Rover et al., 2015; Viechtbauer, 2010). Consistent with this approach, we deliberately did not pool secondary outcomes when definitions and reporting were incompatible, prioritizing interpretability over nominal statistical “significance.” Finally, we framed the evidence in a perioperative nutrition risk stratification perspective aligned with clinical nutrition readership and existing perioperative nutrition guidance (Cederholm et al., 2019; Weimann et al., 2021) (including ESPEN perioperative/surgical nutrition guidance) (Weimann et al., 2017, 2021).
Terminology and interpretability in a nutrition framework
EWGSOP2 emphasizes muscle strength as the primary criterion for sarcopenia, with muscle quantity/quality supporting confirmation and physical performance indicating severity (Cruz-Jentoft et al., 2019). In parallel, Asian Working Group for Sarcopenia (AWGS) provides region-specific consensus operationalization for Asian populations, which is relevant given that several included cohorts were conducted in Asia (Chen et al., 2020). In CABG cohorts—predominantly retrospective—functional assessments are rarely available; consequently, exposures are operationalized using radiologic indices of low muscle quantity and/or poor quality. CT-derived low muscle status should not be interpreted as synonymous with either consensus-diagnosed sarcopenia or malnutrition. Rather, it represents one component of physiologic reserve/vulnerability that may reflect the combined influence of nutrition-related factors, frailty, chronic disease burden, inflammatory burden, and reduced physical activity. In a perioperative CABG pathway, its most appropriate role is therefore as a pragmatic risk flag that can trigger structured nutrition assessment and optimization when CT is already available, not as a stand-alone diagnostic substitute.
Biological plausibility and links to outcomes
The observed associations are biologically plausible. Low muscle quantity may reflect diminished protein reserve and reduced capacity to buffer the catabolic stress of major surgery, potentially affecting ventilatory function, mobility, wound healing, and immune competence. In addition, anabolic resistance—described in aging and wasting states—may limit the effectiveness of perioperative nutritional intake in the absence of structured assessment and individualized planning (Breen and Phillips, 2011; Cuthbertson et al., 2005). Muscle quality metrics such as radiodensity/myosteatosis-related proxies may capture intramuscular lipid infiltration and metabolic dysregulation not fully reflected by muscle area, plausibly linking to inflammation, insulin resistance, and impaired recovery trajectories (Aubrey et al., 2014; Goodpaster et al., 2000). These constructs may be particularly relevant in cardiac surgery populations where body mass index (BMI) can obscure risk, including sarcopenic obesity phenotypes in which excess adiposity coexists with low muscle reserves and adverse metabolic profiles (Donini et al., 2022; Prado et al., 2008, 2012).
Clinical implications: Perioperative nutrition risk stratification
From a clinical nutrition perspective, the practical question is whether CT-derived low muscle status can support triage and optimization rather than simply label risk. Perioperative nutrition guidance emphasizes early identification of patients at nutrition risk and targeted interventions around major surgery (Weimann et al., 2017, 2021). Our findings support a cautious and pragmatic inference: when CT-derived low muscle status is identified in an isolated CABG patient, it may serve as an adjunctive risk flag that could prompt structured nutrition assessment and optimization, rather than as an established decision-making tool; given the observational nature of the evidence, the association should be interpreted as prognostic rather than causal.
A cautious clinical application framework could be:
Opportunistic identification of low muscle status on available CT (using locally feasible quantity and/or quality indices). Confirmatory assessment using established frameworks (including GLIM where feasible) and clinical context (Cederholm et al., 2019). Targeted optimization aligned with perioperative nutrition guidance (individualized protein/energy planning, and where appropriate, short preoperative multimodal support) (Weimann et al., 2017, 2021).
Scalability remains a practical barrier; however, automated CT-based body composition pipelines using neural networks have been demonstrated on routinely acquired clinical CT, supporting the feasibility of opportunistic muscle assessment at scale in real-world workflows (Paris et al., 2020; Weston et al., 2019). Longitudinal opportunistic CT biomarkers have also been linked to subsequent cardiovascular events in other settings, suggesting a trajectory-based direction that warrants evaluation in CABG cohorts (Graffy et al., 2021).
Finally, CT-derived muscle measures should be considered complementary to—rather than a replacement for—established cardiac surgery risk models. A reasonable next step for the field is to test incremental value beyond contemporary risk models (e.g., STS, EuroSCORE II), and to determine whether adding an objective body composition phenotype improves calibration or discrimination for longer-term outcomes (Nashef et al., 2012; Shahian et al., 2018); similar “incremental value beyond traditional risk scores” has been demonstrated for frailty measures in cardiac surgery (Afilalo et al., 2012).
Explaining heterogeneity: Measurement level, construct, and cut-off derivation
Substantial heterogeneity in pooled survival estimates is expected and likely reflects real differences across cohorts. Key sources include anatomical level (lumbar vs. thoracic), construct (quantity vs. quality), CT acquisition and segmentation parameters, and cut-off derivation. Lumbar (L3) muscle quantification is widely used as a reference approach for CT-based body composition, and correlates strongly with whole-body fat-free mass, yet thoracic measurements may be more practical in cardiac surgery settings where chest CT is commonly available (Mourtzakis et al., 2008; Nemec et al., 2017); across vertebral levels, agreement and variability have been described for T4/T12 versus L3 measurements (Arayne et al., 2023; Derstine et al., 2018). In addition, psoas-only indices may not be equivalent to whole-slice skeletal muscle assessment, introducing construct heterogeneity (Pigneur et al., 2023; Rollins et al., 2020). Vertebral-level cut-offs across the thoracolumbar region have also been described, underscoring that thresholds may vary materially by level even within the same individual (Derstine et al., 2018).
Cut-off derivation strategy is particularly important for transportability. Sample-dependent thresholds (e.g., cohort quantiles) and outcome-derived cut-offs may improve within-cohort discrimination but can reduce generalizability across settings and populations. Notably, Lee et al. derived sex-specific SMI cut-offs using receiver operating characteristic analysis for all-cause mortality—an explicitly outcome-derived approach that may overfit within-cohort risk separation and complicate external application (Lee et al., 2024). Population- and ethnicity-specific reference values can further influence classification, especially in Asian cohorts where baseline body composition differs from Western reference samples (Chen et al., 2020; Hamaguchi et al., 2016). These considerations support the need for external validation (or prespecified reference-based thresholds) before CT-derived thresholds are used for routine CABG risk stratification.
Reporting and research roadmap
To move from signal detection to clinical adoption, future CABG studies should report CT-derived muscle assessment in a standardized and reproducible manner. At a minimum, reports should specify: (i) CT timing relative to surgery and acquisition context (routine preoperative workup vs. symptom-driven imaging); (ii) anatomical level and muscle group(s) analyzed; (iii) segmentation approach and software (including quality control procedures); (iv) the construct measured (quantity and/or quality), units, and normalization method; and (v) the rationale for cut-off selection, with preference for prespecified or externally validated thresholds rather than purely sample-dependent or outcome-derived cut-offs (Derstine et al., 2018; Hamaguchi et al., 2016; Mourtzakis et al., 2008); for multilevel CT muscle assessment, reporting should also clarify level selection and comparability across vertebral levels (Arayne et al., 2023; Derstine et al., 2018).
Equally important, outcomes should be harmonized with clear time windows and definitions (e.g., standardized complication definitions and consistent follow-up for survival end points), enabling future pooling without forcing clinically incompatible end points into a single synthesis. Where feasible, incorporation of simple functional measures (e.g., grip strength or gait speed) would help bridge imaging-derived traits with consensus sarcopenia definitions and improve clinical interpretability (Chen et al., 2020; Cruz-Jentoft et al., 2019).
Beyond descriptive prognostic associations, prospective multicenter cohorts should evaluate whether CT-derived low muscle status provides incremental prognostic information beyond established cardiac surgery risk models and whether nutrition-focused optimization and multimodal prehabilitation targeted to this phenotype can improve postoperative outcomes (Weimann et al., 2017, 2021). Future prospective CABG cohorts could evaluate how CT-derived muscle phenotypes integrate with structured nutrition assessment frameworks (including GLIM where feasible) and whether combined approaches improve longer-term risk stratification.
Strengths and limitations
Strengths of this review include a prespecified multidatabase search, strict eligibility restricted to isolated CABG, and explicit handling of overlapping cohorts to ensure independent evidence. We also adopted conservative synthesis methods appropriate for a few studies and expected heterogeneity, prioritizing uncertainty quantification over spurious precision (Hartung and Knapp, 2001; IntHout et al., 2014; Jackson et al., 2017; Rover et al., 2015).
Limitations largely reflect the underlying evidence base. Only four independent cohorts met strict criteria, and only three contributed comparable adjusted survival estimates, limiting precision and precluding metaregression. Exposure definitions (including anatomical level, construct, and cohort-specific or outcome-derived cut-offs) and reporting of secondary outcomes were heterogeneous, which likely contributed to the substantial heterogeneity and imprecision and prevented pooled analyses for complications and composite end points. An additional limitation is the conceptual and anatomical heterogeneity of the pooled exposures. The primary meta-analysis combined measures obtained at different vertebral levels (L3 and T12) and across different constructs (SMI, PMI, and a radiodensity-related quality proxy). Although all were intended to capture low muscle status, they are related but not biologically or statistically identical markers, and pooling across them may obscure level-specific or construct-specific associations. With only three studies in the primary meta-analysis, informative subgroup analyses by vertebral level, construct, or cut-off strategy were not feasible. Residual confounding remains possible in observational cohorts. The transparency of statistical reporting varied among the included studies; for example, some cohorts did not explicitly report all covariates retained in their final adjusted models (as detailed in Supplemental Table S6), which limits our ability to perfectly assess the comparability of confounding adjustment across studies. Although our multidatabase and trial registry searches were designed to maximize retrieval, language restrictions were applied in some databases, we did not systematically perform backward or forward citation tracking, and additional eligible reports may have been missed. The protocol was not prospectively registered.
Conclusions
Current evidence linking CT-derived low muscle status with postoperative risk after isolated CABG remains highly uncertain, exploratory, and hypothesis-generating, given the very limited number of independent cohorts, substantial heterogeneity, and wide confidence and prediction intervals. Across included studies, the direction of association was generally unfavorable, but the pooled survival estimate should not be interpreted as definitive or directly transportable. At present, CT-derived low muscle status is best viewed as an adjunctive perioperative vulnerability/risk flag, rather than an established decision-making tool, and may support further structured nutrition assessment when opportunistic CT data are already available.
Supplemental Material
sj-docx-1-nah-10.1177_02601060261461906 - Supplemental material for Computed tomography-derived low muscle status and clinical outcomes after isolated coronary artery bypass grafting: A systematic review and meta-analysis with implications for perioperative nutrition risk stratification
Supplemental material, sj-docx-1-nah-10.1177_02601060261461906 for Computed tomography-derived low muscle status and clinical outcomes after isolated coronary artery bypass grafting: A systematic review and meta-analysis with implications for perioperative nutrition risk stratification by Ziqiang Zhou, Tingting Sun, Jiangang Zhao, Yanjun Wang and Wenbo Wu in Nutrition and Health
Footnotes
Acknowledgments
The authors acknowledge the use of artificial intelligence-assisted tools (ChatGPT) for language editing and grammatical refinement during manuscript preparation. The authors take full responsibility for the content, interpretation, and integrity of the work.
Ethical considerations
Ethical approval was not required for this systematic review/meta-analysis because it included only previously published data.
Author contributions
Z.Z. conceived the study, designed the protocol, performed the literature search, conducted the statistical analysis, and drafted the original manuscript. T.S. contributed to the study design from a perioperative care perspective, assisted in clinical heterogeneity assessment, and critically revised the manuscript for intellectual content. J.Z. and Y.W. performed data acquisition, study selection, and quality assessment. W.W. contributed to data curation and assisted with software implementation. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.