
Abstract
Background
Vitamin D deficiency is prevalent among pediatric patients with sickle cell disease (SCD) and may be associated with acute clinical complications. Despite its potential impact, the effects of this deficiency in this population are not fully understood.
Aims/Objectives
This study aims to review the current literature on vitamin D deficiency in children with SCD, focusing on its clinical and laboratory outcomes, and to explore the potential benefits of vitamin D supplementation.
Methods/Methodology
A systematic review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Searches were performed across five databases—MEDLINE, LILACS, Cochrane, EMBASE, and Scientific Electronic Library Online. From an initial pool of 497 articles, 12 met the inclusion criteria and were included in the final analysis.
Results/Findings
The review identified several clinical and laboratory outcomes associated with vitamin D deficiency in pediatric SCD patients. Vaso-occlusive crises were the most commonly reported clinical outcome, appearing in 25% of the studies. Similarly, hospitalizations were noted in a quarter of the reviewed articles. Laboratory findings most frequently included anemia and hemolysis.
Conclusion
Vitamin D deficiency in pediatric sickle cell patients is linked to worse clinical and laboratory outcomes, including increased crises and hospitalizations. Supplementation may help, but evidence is insufficient; further studies are needed to guide recommendations.
Introduction
The prevalence of vitamin D deficiency in pediatric patients with sickle cell disease (SCD) is high (de Oliveira et al., 2015; Nolan et al., 2015). Studies have demonstrated that this vitamin deficiency in SCD may be associated with acute complications. These include an increased frequency of pain crises, higher hospitalization rates, and damage to target organs such as the lungs, kidneys, and bones (Blake and Lima, 2011; Garadah et al., 2015). Deficiency of this prohormone may contribute to worsened inflammatory patterns in this hemoglobinopathy. This process involves the release of cytokines such as interleukin-6 (IL-8), IL-8, and IL-18 (Adegoke et al., 2017a), which intensify the pathophysiological process of vaso-occlusion (Sundd et al., 2019).
Vitamin D deficiency is also linked to various negative outcomes in other chronic diseases. Hypovitaminosis D may imply a higher risk of oncological diseases such as colon, prostate, and breast cancer (Holick, 2007). Additionally, increased cardiovascular risk for congestive heart disease is described in patients with vitamin D deficiency (de la Guía-Galipienso et al., 2021). Vitamin D deficiency has also been described in autoimmune diseases such as systemic lupus erythematosus and multiple sclerosis (Yang et al., 2013).
Supplementation has proven to be a cost-effective alternative in some pathologies, notably in patients with chronic kidney disease (Kandula et al., 2011). In SCD, vitamin D supplementation appears to be a cost-effective strategy to add to standard therapy for reducing pain events (Abdelhalim et al., 2022). It also appears to increase fetal hemoglobin levels and reduce platelet counts, factors that decrease clinical complications associated with the disease (Dougherty et al., 2015).
To better understand the consequences and repercussions of vitamin D deficiency in pediatric patients with SCD, based on the literature, a systematic review was conducted.
Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (Page et al., 2021). The research question was designed to assess the association between vitamin D status and clinical outcomes in pediatric patients with SCD. Eligibility criteria included observational studies published in English, Portuguese, Spanish, or French up to 30 November 2023. Studies involving patients aged 0 to 21 years were included, consistent with the pediatric age definition proposed by Hardin and Hackell (2017). Studies were excluded if they were reviews, interventional trials, case reports, or if they assessed vitamin D supplementation rather than serum vitamin D levels. Studies including adult populations or individuals with sickle cell trait were also excluded.
A comprehensive literature search was conducted between September and November 2023 using the following databases: MEDLINE (via PubMed), LILACS (via the Virtual Health Library), Cochrane Library, EMBASE, and Scientific Electronic Library Online. Search strategies were adapted for each database using Medical Subject Headings and relevant keywords. The primary search terms included “vitamin D” AND “sickle cell anemia,” combined using Boolean operators.
All retrieved records were consolidated, and duplicate articles were removed. Two authors independently screened titles and abstracts for eligibility, followed by full-text review of potentially relevant studies. Disagreements were resolved through discussion, with the involvement of a third reviewer when necessary. Data were independently extracted by two reviewers using a standardized data extraction form, including study design, population characteristics, sample size, vitamin D assessment methods, and main outcomes. Due to heterogeneity among studies, results were synthesized narratively. The methodological quality and risk of bias of the included studies were assessed using an appropriate tool for observational studies.
Results
Out of 497 initially listed articles, 358 remained after removing duplicates. Following assessment against inclusion and exclusion criteria, 52 articles were selected to address both topics of interest. Of these, 27 were excluded due to involving vitamin D supplementation, and 12 were excluded because they included adult patients, with 1 study including sickle cell trait in the sample, totaling 12 articles for this review (Figure 1).
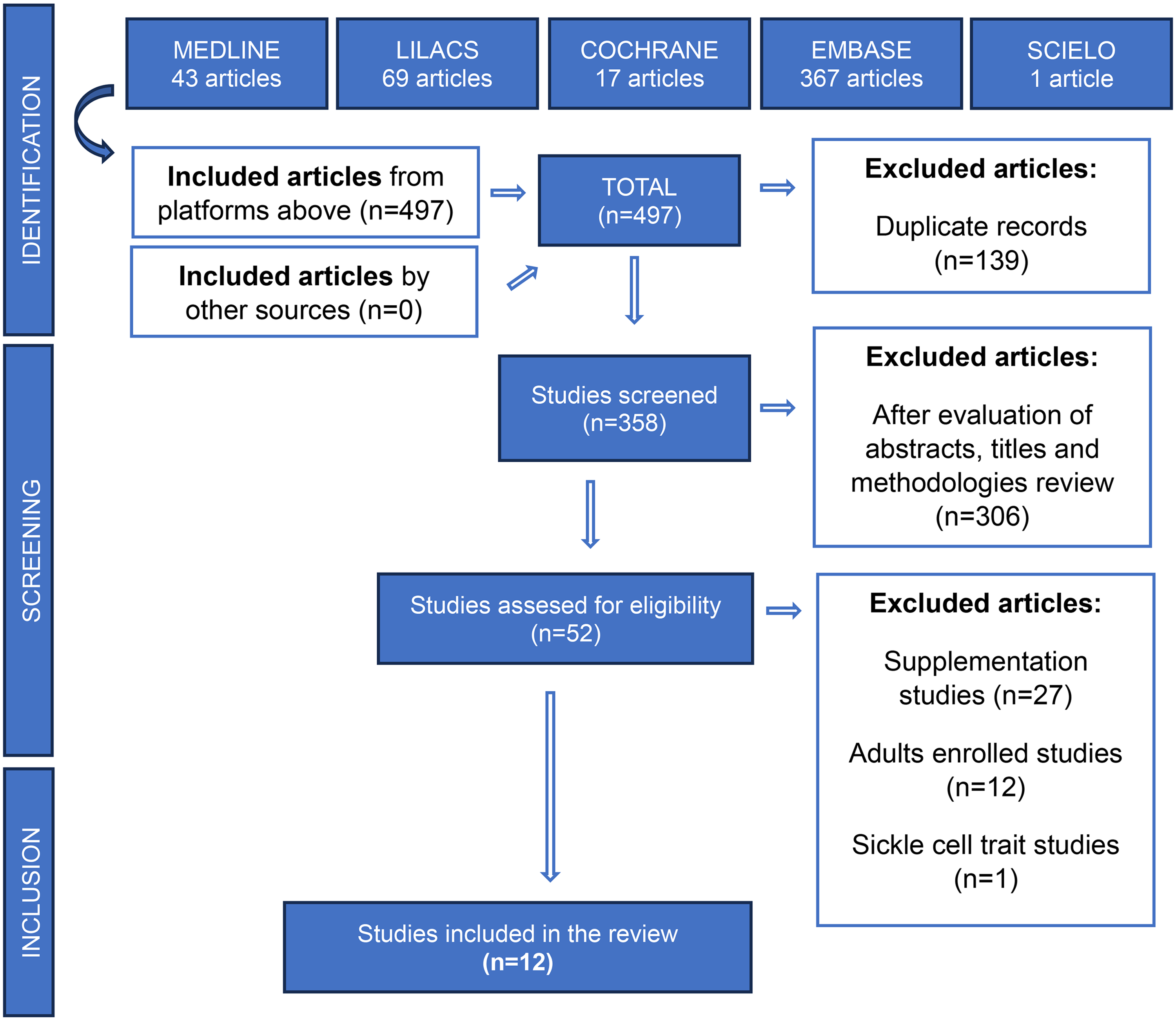
Flowchart of identification, selection, eligibility, and inclusion of studies evaluating the implications of vitamin D deficiency in pediatric patients with sickle cell disease.
The 12 studies found, considering the authorship, year of publication, sample size, and main findings regarding clinical implications of vitamin D deficiency, are listed in Table 1.
Selected studies in the systematic review on the clinical and laboratory implications of vitamin D deficiency in pediatric patients with sickle cell disease are presented in order of publication from the most recent to the oldest.
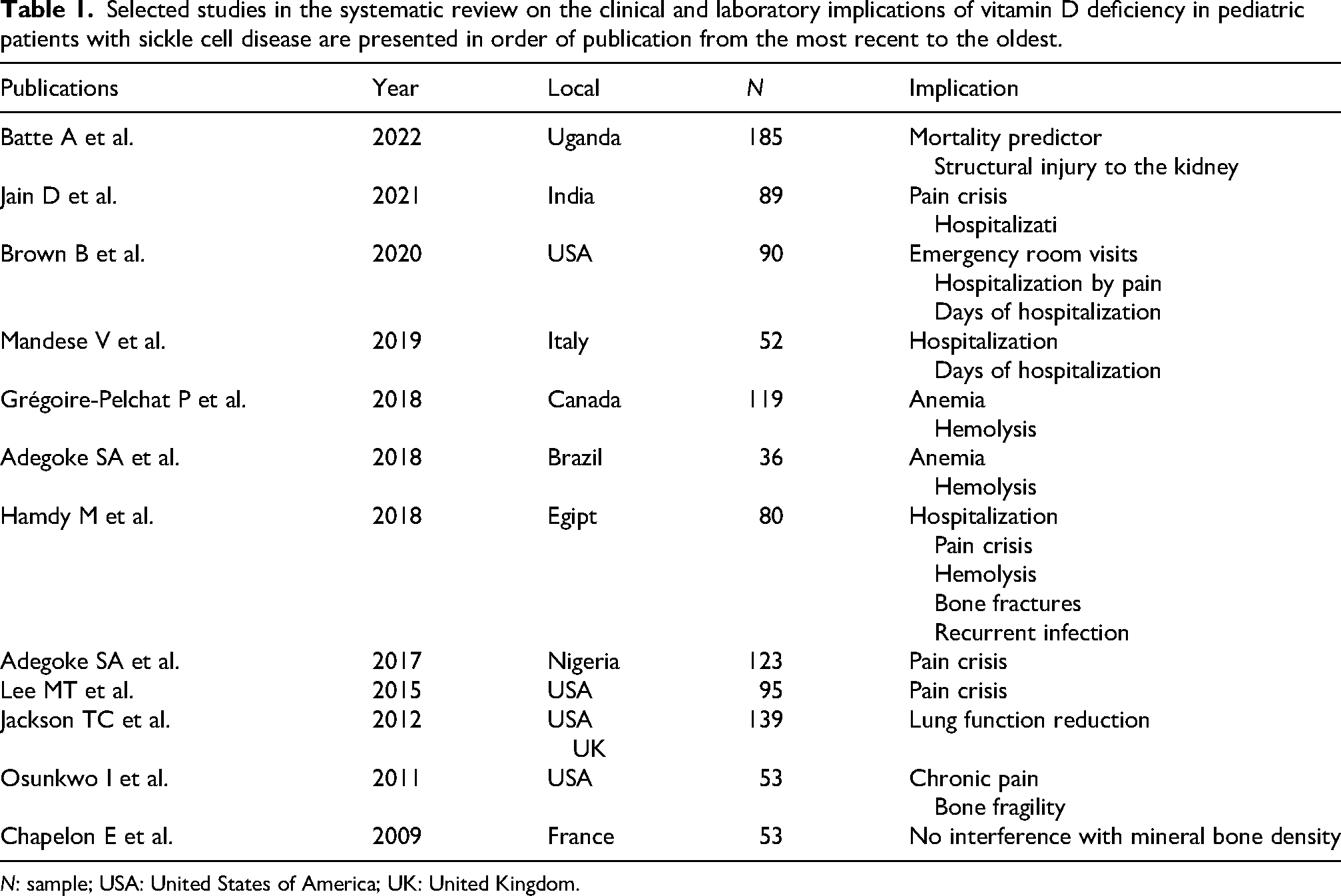
N: sample; USA: United States of America; UK: United Kingdom.
Discussion
Since 2009, several articles have addressed associations of vitamin D deficiency with children and adolescents with SCD across different aspects. The main topics include the manifestation of vaso-occlusive crisis (VOC) or pain crisis, hospitalization frequency and length of hospital stay, organ implications (bone, lung, and kidney), and laboratory findings related to hemolysis, as presented in sequence.
VOC/pain crisis
VOC is the most common acute complication of SCD, resulting in severe pain crises that often require opioid treatment. These crises may affect the limbs, back, abdomen, chest, or other body regions and frequently necessitate hospitalization for adequate management (National Institutes of Health, 2014).
Regarding complaints of painful crises and acute episodes of VOC, four studies confirmed this outcome. Lee et al. (2015) observed a higher association between pain crisis and serum vitamin D status (odds ratio (OR) = 2.7; 95% confidence interval (CI) 1.05–6.94; p = 0.04) in American patients, as 74% of patients with pain had vitamin D deficiency, while 26% had normal values of serum vitamin D assessment (25-OH-D). Serum 25-OH-D was significantly associated with pain (p = 0.012) but not with acute chest syndrome episodes (p = 0.628). In this study, hydroxyurea, sex, race/ethnicity, SCD type, and season were no effect modifiers, but age was a strong confounder in the relationship between vitamin D and pain.
Adegoke et al. (2017b) also demonstrated in a larger Nigerian population the association of vitamin D insufficiency with significant pain episodes in pediatric patients with SCD. In these patients, serum vitamin D levels (OR = 1.2; 95% CI 1.3–1.7; p = 0.04) and fetal hemoglobin (OR = 1.6; 95% CI 1.1–1.4; p = 0.02) were predictors of pain episodes in a binary logistic regression. Similarly, this study did not observe a relationship with acute chest syndrome, hospitalization, transfusion frequency, or avascular bone necrosis, but the vitamin D deficiency group was very small (n = 14), which may have compromised the analysis.
In Egypt Hamdy, Salama, and Maher (2018) analyzed 80 patients and noted a more pronounced association between vitamin D deficiency and VOC episodes over the past year (p = 0.032), but no statistical difference in the degree of the pain crisis.
The fourth study to find a relationship between vitamin D deficiency and pain crises was conducted in India by Jain and Kumar (2021). Data from 89 patients from 2016 to 2018 were collected, and the research noted statistically significant association (p = 0.01; 5.60 ± 3.25 episodes in patients with vitamin D deficiency vs. 2.22 ± 1.64 episodes in patients without vitamin D deficiency) in number of pain episodes in individuals with vitamin D deficiency, but other factors which could affect the development of hypovitaminosis D in this population were not evaluated.
When considering chronic pain, Osunkwo et al. (2011) assessed a 53-patient sample in the United States and found a significant association of chronic pain with lower 25-OH-D levels when compared to those without chronic pain (21.2 ± 8.2 vs. 36 ± 17.5 nmol/l; p = 0.0021). The small sample size and the inclusion of patients with very severe manifestations of SCD were important biases to consider when interpreting the data from this analysis.
As observed, the primary outcome present in almost half of the articles was a painful crisis. It is known that the pathophysiology of SCD involves different inflammatory mechanisms and pathways, with an increase in different cytokines, such as tumor necrosis factor-alpha (TNF-α) and IL-1 (Sundd et al., 2019). These inflammatory mediators, combined with sickle cells, induce endothelial activation, whereby a damaged and stimulated endothelium recruits leukocytes to adhere to the vessel wall. Following a second wave of inflammatory activation signals, neutrophils adhered to the endothelium and eventually captured and adhered to sickle cells, culminating in vaso-occlusion (Manwani and Frenette, 2013). On the other hand, vitamin D plays a crucial immunomodulatory role, and various cells in the body possess vitamin D receptors, such as leukocytes. Vitamin D deficiency increases IL release and TNF-α and interferon-γ expression (Antonucci et al., 2018). Thus, this may strengthen the hypothesis of a relationship between painful crises and vitamin D deficiency.
Hospitalization
Even with disease control and clinical stability achieved through pharmacological treatment, SCD remains a highly complex and severe condition, characterized by acute and chronic complications, limitations in daily activities, and frequent hospitalizations (Odame, 2023).
Similar to the study by Jain and Kumar (2021) conducted in India, which found an association between serum vitamin D levels and hospitalization (p = 0.02; 9.01 ± 5.30 admissions in patients with vitamin D deficiency vs. 5.11 ± 3.01 in those without deficiency), other studies have also investigated the relationship between vitamin D deficiency and the risk of hospital admission. Mandese et al. (2019), in an Italian evaluation of 52 patients, found a higher average hospitalization rate in patients with vitamin D deficiency over the last five years (Spearman R = −0.36; p = 0.009) as well as in the last year of the study (Spearman R = −0.29; p = 0.040). They also observed statistically higher average hospitalization days in the last year among patients with hypovitaminosis D (Spearman R = −0.29; p = 0.034), but the authors only presented the statistical results and not the absolute values of the event numbers for the outcomes assessed. Brown et al. (2020) in the United States also suggested in a sample with 90 patients that lower vitamin D levels were associated with higher hospitalization frequencies due to pain crises (p < 0.01), longer hospital stays (p < 0.001), and more emergency department (ED) visits (p < 0.01), with correlations also statistically significant, being the only study to make this inference. Besides the limitations of a retrospective study, the small sample size limited the evaluation of the hydroxyurea interference in these variables. In turn, Hamdy et al. (2018) found a higher frequency of hospitalizations in the last year when comparing a vitamin D-deficient group to a non-deficient group (p = 0.012). They also observed a higher rate of recurrent infections (p = 0.036), although the sample size was small (n = 36).
Hospitalization was also an outcome in a quarter of the selected articles. This may occur due to VOC, anemia, and hemolysis, as reported by Grégoire-Pelchat et al. (2018) and Adegoke et al. (2018), or due to infection, given the increased recurrence observed by Hamdy et al. (2018). Hospital admission in SCD is negatively correlated with quality of life. Vitamin D supplementation in SCD patients has shown improvement in health-related quality of life and better physical performance in both healthy individuals and those with the hemoglobinopathy in question (Dougherty et al., 2020).
Organ implications
The chronic complications of SCD accumulate over time and affect multiple organ systems. These include significant bone mineral loss and femoral head necrosis, auditory and ocular abnormalities, pulmonary hypertension, gallstone disease secondary to hemolysis-related hyperbilirubinemia, growth impairment and delayed puberty, and glomerular alterations with potential progression to chronic kidney disease, among other long-term manifestations (Piel et al., 2017).
Some studies focused on the manifestation in other organs affected by SCD, both acutely and chronically. In a multicenter study with 139 patients, Jackson et al. (2012) found no clinical association of vitamin D deficiency in SCD concerning asthma, pain crises, acute chest syndrome, or specific spirometry parameters such as forced expiratory volume in one second (FEV1)/forced vital capacity. However, they did find a relationship between predicted FEV1% and 25-OH-D levels, suggesting reduced lung function in this population in a model with a reduced set of covariates (p < 0.20 in full model; β = 0.49; 95% CI 0.08 to 0.90; p = 0.02). This association was also found in a reduced model when using severe vitamin D deficiency as a predictor rather than continuous vitamin D levels (β = −5.59; 95% CI −10.45 to −0.72; p = 0.025). The lack of evaluation of prior vitamin D supplementation, dietary history, and the exclusion of patients using hydroxyurea may have compromised the findings of this study, as they do not represent the reality.
A study in Uganda performed in 2019 with 185 hospitalized patients with VOC reported that vitamin D deficiency associated with hyperparathyroidism was linked to increased mortality risk (Batte et al., 2023). However, the number of deaths as an outcome was limited to affirm conclusions (6 out of 185). The same study found that a marker of structural kidney damage was nine times more likely to present vitamin D deficiency.
Hamdy et al. (2018) also presented a higher frequency of bone fractures in the vitamin D-deficient group (p = 0.034), but the sample size was very limited (n = 8) to be considered reliable. In the same way, Osunkwo et al. (2011) reported an association between bone fragility and lower 25-OH-D levels (23.7 ± 11.5 vs. 36.7 ± 17.7 nmol/l; p = 0.0045). However, Chapelon et al. (2009) in France studied 53 patients and found that low bone mineral density in children and adolescents from 9 to 19 years old was not related to 25-OH-D levels, but the association of vitamin D to clinical or laboratory implications was not the focus of this study.
Target organ damage also contributes to impaired quality of life in patients with SCD, which, when compared with other chronic pediatric conditions, is associated with poorer outcomes (Carrara et al., 2023).
Laboratory findings
In the complex pathophysiology of SCD, intraerythrocytic deoxygenation of HbS in tissues with high oxygen demand promotes the exposure of hydrophobic structures within hemoglobin tetramers (Rees et al., 2010). As a consequence, βS-globin chains interact to shield these hydrophobic regions, initiating HbS polymer formation. Polymerized hemoglobin also contributes to hemolysis, leading to the release of free hemoglobin into the circulation. Hemolysis results in increased reticulocyte counts, elevated indirect bilirubin levels, and more severe anemia.
A Canadian study conducted in Montreal by Grégoire-Pelchat et al. (2018) with 119 patients found no clinical association of vitamin D deficiency in SCD when evaluating event frequency over the two years prior to data collection. However, hemoglobin and reticulocyte counts were lower in patients with hypovitaminosis D (p = 0.002 and 0.008, respectively). The study also observed that age, parathyroid hormone, and hemoglobin levels independently predicted low serum 25-OH-D through multivariable linear regression (β [95% CI]: 0.39 [0.22 to 0.57]; p < 0.001 for hemoglobin). Besides evaluating dietary intake and sun exposure, the cross-sectional nature of the study could not establish whether impaired vitamin D status was the cause or the consequence of the reported associations.
The only publication involving pediatric patients with SCD in South America is from Brazil, conducted by Adegoke et al. (2018) with 36 children aged 4 to 11 years in São Paulo. Hemoglobin and hematocrit were significantly positively correlated to vitamin D levels (r = 0.40, p = 0.017 and r = 0.45, p = 0.006, respectively). Conversely, absolute and percentage reticulocyte counts (r = 0.47, p = 0.007; r = 0.44, p = 0.008), as well as lactate dehydrogenase (LDH) (r = 0.45, p = 0.007), were significantly inversely correlated with 25-OH-D results. However, this analysis did not assess any clinical association between vitamin D deficiency and SCD in Brazilian pediatric patients. It also had a very small sample size from a single center and did not account for other factors associated with anemia in this chronic condition.
Hamdy et al. (2018) found in their study that the vitamin D-deficient group had significantly lower levels of hemoglobin and hematocrit (p = 0.022 and 0.004, respectively). In contrast, levels of aspartate aminotransferase (AST), LDH, as well as total and indirect bilirubin were significantly higher in this group (p = 0.006, 0.001, 0.038, and 0.016, respectively). A weak but statistically significant correlation between serum 25-OH-D levels and biomarkers of hemolysis and red blood cell turnover was found, as patients with vitamin D deficiency exhibited lower hemoglobin and hematocrit levels (r = 0.27, p = 0.019 and r = 0.29, p = 0.011, respectively), along with higher AST, LDH, total and indirect bilirubin levels and reticulocyte count (r = −0.33, p = 0.003; r = −0.27, p = 0.017; r = −0.29, p = 0.01; r = −0.35, p = 0.002; r = −0.31, p = 0.007, respectively). However, the study did not exclude patients who were receiving vitamin D supplementation, which may introduce a potential bias. Among the studies reviewed, this one most clearly emphasizes the clinical and laboratory correlations of vitamin D deficiency in children and adolescents with SCD. Nevertheless, Osunkwo et al. (2011) did not correlate 25-OH-D levels with hemoglobin and reticulocyte count in their analysis.
In addition to these main clinical and laboratory findings and their implications, the social dimension of SCD also plays an important role. Ally et al. (2023) recently evaluated an index that takes into account factors such as education, job prospects, family income, and others, and found that lower social conditions are linked to reduced vitamin D levels. In a multinational study of 985 children with SCD, an inverse relationship between income and ED visits for pain was found. A $10,000 increase in income was linked to a 5% reduction in ED visits (relative risk (RR) 0.95, 95% CI = 0.91 to 1.00, p = 0.05). Additionally, a separate multivariable model showed that income below the federal poverty line was associated with a 31% increase in ED visits for pain (RR 1.31, 95% CI = 1.04 to 1.64, p = 0.02) (Glassberg et al., 2012). These findings reflects that vitamin D deficiency is also associated with socioeconomic deprivation, meaning that the correlations between SCD severity and vitamin D deficiency may largely reflect socioeconomic status.
It should be noted that the great majority of studies in the review addressed vitamin D through categorization between deficiency and sufficiency, with few evaluating the continuous value of serum 25-OH-D levels in relation to other variables. The Endocrine Society Clinical Practice Guideline defined vitamin D deficiency as serum levels below 20 ng/mL, insufficiency as 20–29 ng/mL, and sufficiency as ≥30 ng/mL (Holick et al., 2011). In contrast, the 2016 Global Consensus on Nutritional Rickets proposed lower cutoffs, defining deficiency as <12 ng/mL, insufficiency as 12–20 ng/mL, and sufficiency as >20 ng/mL (Munns et al., 2016). However, the last update from the Endocrine Society Clinical Practice Guideline in 2024 no longer supports its previous definitions of vitamin D sufficiency and insufficiency. This change was made because there was no strong evidence of a threshold that better predicts vitamin D supplementation benefits in the generally healthy population (McCartney et al., 2024). Nevertheless, most studies reported that worse clinical and laboratory outcomes in SCD were associated with vitamin D deficiency, regardless of the reference criteria adopted.
Consideration should be given to studies involving patients from sub-Saharan Africa such as Uganda and Nigeria since they not presented as many clinical findings even with large samples (Adegoke et al., 2017a; Batte et al., 2023). This may be justified by the low prevalence of vitamin D deficiency in this region, as evidenced in a large multicenter international study by Mogire et al. (2022).
As limitations of this review, some studies had very small sample sizes, such as the one conducted with the Brazilian population (de Oliveira et al., 2014). This study also did not assess clinical outcomes in the same way as other studies did. Another limitation of all review studies is publication bias, which may have also influenced the results of this review. Studies with positive or significant findings are more likely to be published, while those with negative or inconclusive results may remain unpublished. Researchers should be encouraged to publish all findings, regardless of the outcome, to provide a more comprehensive and unbiased view of the evidence and associations of vitamin D deficiency with SCD pediatric patients.
Due to several limitations in the data presented across the studies, including small sample sizes and variability in outcome measures, a meta-analysis was not feasible. The studies we reviewed employed different methodologies and outcome measures, making it difficult to aggregate the results in a meaningful way. We acknowledge that, as per the design of the included studies, only non-interventional research was considered, which makes it inherently difficult to establish causal relationships. The cross-sectional design and retrospective collection limited our ability to exclude reverse causation, that is, whether vitamin D deficiency is the cause or consequence.
To address these limitations, we applied strict inclusion and exclusion criteria and conducted independent dual screening of studies. We also used a standardized data extraction form to ensure consistency. Additionally, due to heterogeneity in study designs and outcome measures, a narrative synthesis was performed instead of a meta-analysis, avoiding inappropriate aggregation of results. These measures were implemented to enhance the reliability and transparency of our findings despite the inherent limitations of the available literature.
This review has some strengths, as being the first to emphasize both clinical and laboratory correlations of vitamin D deficiency in pediatric patients with SCD, rather than just assessing prevalence or studying supplementation in adults. Understanding the implications of vitamin D deficiency in these patients can assist in better understanding disease pathophysiology and in developing new therapies or vitamin supplementation recommendations.
Therefore, vitamin D deficiency in pediatric patients with SCD is consistently associated with worse clinical outcomes. These include increased frequency of pain crises, higher hospitalization rates, and target organ damage affecting bones, kidneys, and lungs. Monitoring vitamin D status can help clinicians identify patients at higher risk for severe disease manifestations and guide more comprehensive care strategies. Recognizing these associations highlights the need for careful clinical surveillance and targeted interventions to mitigate complications and improve quality of life in this vulnerable population.
In conclusion, after a systematic review, vitamin D deficiency appears to be associated with worse clinical and laboratory outcomes in pediatric patients with SCD. Increased episodes of vaso-occlusive crises and higher hospitalization rates were observed in several studies. Supplementation could potentially mitigate these outcomes; however, current reviews are not yet robust enough to recommend this therapy. Nevertheless, long-term supplementation appears to reduce disease-related clinical complications.
Footnotes
Acknowledgements
We thank all the professionals and collaborators from the Pediatric Hematology department at Universidade Federal de São Paulo.
Ethical approval and informed consent statements
Not applicable. As a review, this study was exempt from ethical approval by the research ethics committee of the institution where it was conducted.
Author contributions
Thiago de Souza Vilela: Data collection, writing, editing, translation, and final review. Mauro Fisberg: Writing, translation, and final review. Gerson Luis de Moraes Ferrari: Editing, analysis, and final review. Josefina Aparecida Pellegrini Braga: Writing, editing, and final review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data and material availability statement
Not applicable.