
Abstract
Background
Dietary interventions for managing functional bowel disorders are numerous and varied.
Aim
To describe service utilisation patterns and dietary care offered to patients with functional bowel disorders in an outpatient dietetics clinic.
Methods
A retrospective clinical audit of adults (n = 30) with a functional bowel disorder. Patient characteristics, dietary interventions and service-related indicators were extracted from patient records.
Summary
Most patients were female (93%) and aged under 35 years (67%). The wait time to see a dietitian was 4 months and patients were in the service for 20 months. All patients received dietary education, half received artificial nutrition, 40% were recommended supplements, and 30% advised on behavioural modifications. Only one patient was discharged due to the resolution of symptoms following dietetic involvement. This may have been due to the small sample size and focus on symptom resolution rather than a range of outcome measures such as quality of life. Novel interventions for this cohort are warranted.
Introduction
The functional bowel disorders, or disorders of gut-brain interaction, are gastrointestinal disorders related to any combination of motility disturbance, visceral hypersensitivity, altered mucosal and immune function, altered gut microbiota, and altered central nervous system processing (Sperber et al., 2021). They result in significant global healthcare costs and impaired health-related quality of life (Sandler et al., 2002). Irritable bowel syndrome (one type of functional bowel disorder) alone results in 8 to 21 days per year of missed work (Maxion-Bergemann et al., 2006). Further to this, the annual direct costs of ambulatory clinic visits for chronic symptomatic functional bowel disorders in the United States are approximately US$358 million (Ma et al., 2021).
The functional bowel disorders have no identifiable structural or biochemical abnormalities to account for their defining symptoms. Diagnosis relies almost exclusively on symptom patterns, though the Rome IV diagnostic criteria are the most widely accepted standard for such symptom-based diagnoses (Drossman and Hasler, 2016). As such, there have been long-standing difficulties in collecting prevalence data due to varying definitions of the disorder, survey methodologies and the variability of populations studied (Palsson et al., 2020). That said, a recent large-scale multinational study estimated that more than 40% of persons worldwide have a functional bowel disorder, including approximately 40% of Australians (Sperber et al., 2021).
Patients with functional bowel symptoms, such as bloating, abdominal discomfort or pain, and disturbed bowel habits, commonly report that food is a trigger for their symptoms (MacIntosh et al., 2023). Given that food plays such a pivotal role in functional bowel disorders, diet manipulation is considered first-line therapy for many patients. Initially, there is a focus on promotion of healthy diets with adequate fibre and fluid, moving to specific advice regarding types of fibre. Elimination diets are typically reserved for those with persistent symptoms. This is particularly the case given that self-diagnosed food intolerances frequently prompt the elimination of multiple foods; this potentially results in nutritional deficiencies, psychological challenges, disruption to gut microbiota and reduced quality of life (Zingone et al., 2023). Currently available treatment options also include fibre supplementation, probiotics, psychosocial interventions, medications (such as antidepressants), laxatives, antispasmodics, and prokinetics (Singh et al., 2022). In recent years, there has been renewed interest in the role of specific dietary patterns in the treatment of functional bowel disorders, specifically the low-FODMAP diet, fructose or lactose-restricted diets, gluten-free diets and Mediterranean diet (Cenni et al., 2022; Pasta et al., 2024; Rej et al., 2022; Tuck et al., 2020; Wirth et al., 2014). In addition, evidence suggests that gastrointestinal symptoms are a risk factor for disordered eating (Gibson et al., 2021), potentially placing these patients at higher risk of malnutrition and requiring oral nutrition support.
As functional bowel disorders present with a wide range of symptoms, and given the number of treatment options available, managing these conditions in day-to-day practice is complex. Most patients with functional bowel disorders are seen in the outpatient setting, where time constraints and pressures to increase high-throughput efficiency are potential barriers to treating complex, multifactorial diseases (Ma et al., 2021). There is currently little research available describing the dietetic management of functional bowel disorders in a real-world setting; this would help to identify potential therapeutic gaps and areas where the delivery and quality of comprehensive care can be improved (Ma et al., 2021). As such, the aim of this paper is to describe the characteristics of patients with functional bowel disorders attending a Dietetics outpatient service, describe the patterns of service utilisation and dietetic care delivery, and describe the nutrition interventions provided to patients. The current paper provides much needed real-life data on outcomes for patients attending a large gastroenterology service at a time when intervention options for clinicians are numerous and complex.
Methods
We conducted a retrospective audit of all patients presenting to five gastroenterology dietetic outpatient clinics at Mater South Brisbane from 2022 to 2024. The protocol for the current project was reviewed by the Mater Research Human Ethics Committee, which confirmed that the project met the criteria for quality improvement and did not require full review by the Committee (number QACR/MML/108085).
The five gastroenterology clinics include three public and one private service, with each clinic running from 2 to 4 hours once per week. Patients are offered face-to-face, telehealth or telephone consults. All information regarding patient demographics, dietetic intervention and clinical experience was collected from electronic medical records.
The sample for the current study includes all patients with a functional bowel disorder attending an outpatient gastroenterology clinic in a 2 year window between April 2022 and April 2024. Eligible participants were adults (aged >18 years old), with a documented functional bowel disorder who had received an initial consult with a dietitian. Documented functional bowel disorders were considered as a written diagnosis of irritable bowel syndrome, functional gastrointestinal/bowel disorder, functional nausea, functional vomiting, functional dyspepsia, functional abdominal pain, functional bloating, functional constipation and/or functional diarrhoea by a gastroenterologist. Any patients without a documented diagnosis from a gastroenterologist in the patients’ medical file or those yet to be seen by the dietitian were excluded from the study. This was done to remove some of the ambiguity regarding diagnosis of functional bowel disorders that has been documented in the literature (Palsson et al., 2020).
Patient characteristics included as part of data collection were: funding source (public or private); age; height and weight which was used to calculate BMI; type of functional bowel disorder; concurrent medical conditions and the presence of Inflammatory Bowel Disease. Concurrent medical conditions were grouped into systems of interest: gastrointestinal, psychological, Ehlers-Danlos Syndrome, Inflammatory Bowel Disease, Avoidance Restrictive Food Intake Disorder and other.
All dietary interventions were included as part of the data collection and categorised into the following: artificial nutrition, dietary modification, dietary education, mealtime behaviour strategies and supplementation. Artificial nutrition was the provision of nutrition support products either orally or enterally and included both powdered and ready-to-drink formulations. Dietary modification included the increase of fibre (soluble or insoluble), increase fluid consumption, ensuring protein intake met estimated protein requirement, change in food texture and/or manipulation of fermentable oligosaccharides, disaccharides, monosaccharides and polyols (FODMAPs). FODMAP diet advice was provided as per the Monash University Low FODMAP Diet Protocol. Dietary education included advice regarding increasing energy and protein, gluten or lactose free diets, the importance of regular and adequate meals, gastroparesis management, reflux/nausea management and post-inflammatory irritable bowel syndrome management. Mealtime behaviour strategies were focussed on distraction during meal times, relaxation prior to meals and encouraged regular meal times. Supplementation included vitamins or fibre, probiotics and over-the-counter, plant-based remedies to assist with bloating. Fibre supplements included a psyllium supplement or a wheat dextrin supplement available over-the-counter at pharmacies or a partially-hydrolysed guar gum supplement available for online purchase. The intervention patients received, decided by the dietitian, was based on the functional bowel disorder type and predominant symptom causing patient distress.
The clinical experience measures were also included as part of this study. Key variables included: wait time from referral to first appointment (calculated as time from date of referral letter to first appointment), time spent in service, number of appointments, appointment length (calculated from patient appointment start and end times), any hospital admission in the last 3 years, current enteral feeds and the reason listed in the patient file for discharge from the outpatient clinic.
Analyses
All data were analysed descriptively using means with standard deviations or n's and percentages in Stata v16.1 (StataCorp, College Station, TX). Comparisons in treatment types and patient experiences, by type of functional bowel disorder, were made using one-way ANOVAs and chi-square tests. Significance levels were set at p < 0.05. Bias was minimised by including all potential patients within the described timeframe with a written diagnosis and all variables were collected using the same method from patient charts with no assumptions made regarding dietary interventions.
Results
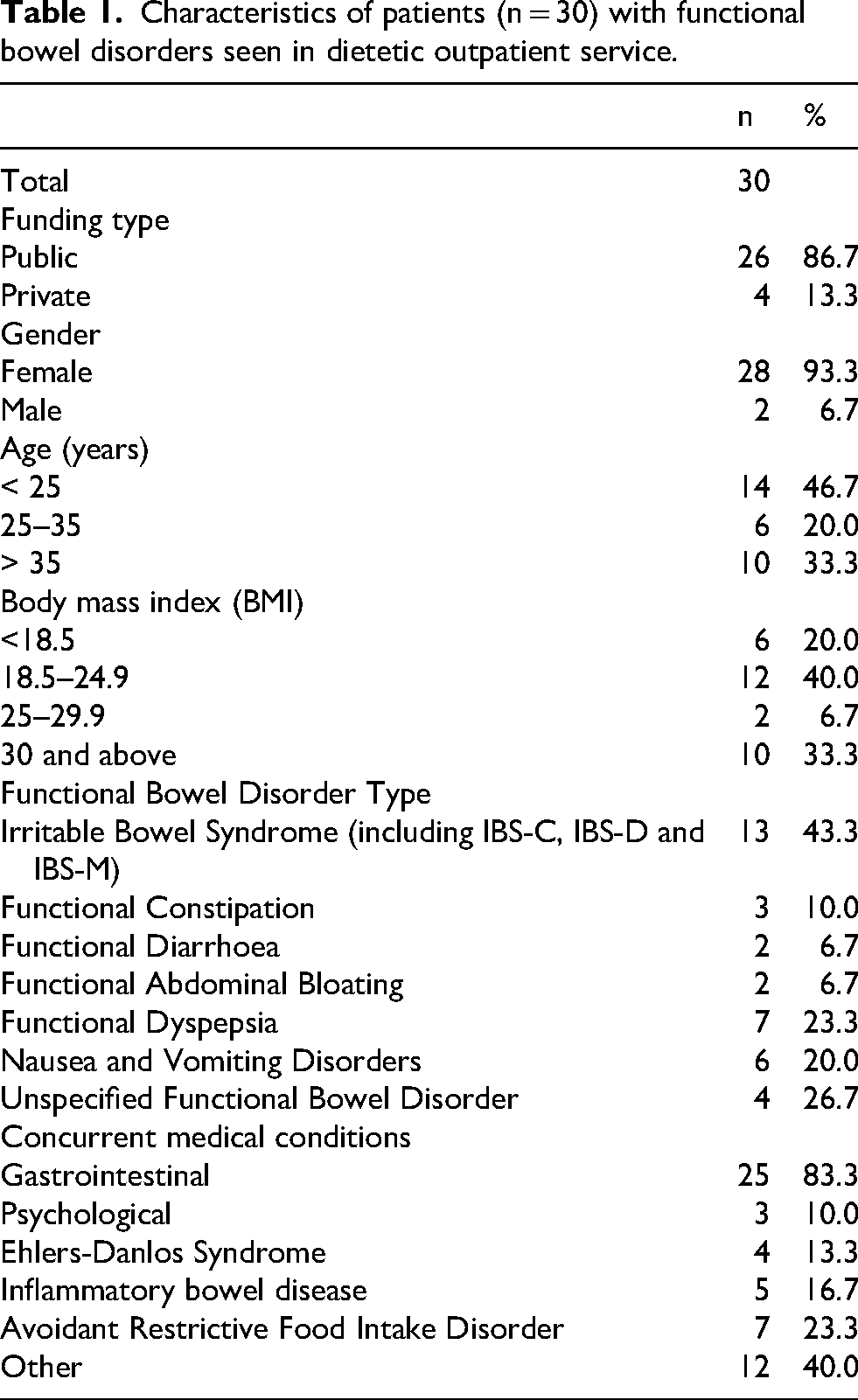
In total, 30 patients met the inclusion criteria for the study (Table 1). Most patients were publicly funded (87%), female (93%) and aged under 35 years (67%). 40% of patients had a BMI in the healthy range and one-third had a BMI of 30 or above. The most common functional bowel disorders within the cohort were irritable bowel syndrome (43%), functional dyspepsia (23%) or an unspecified functional bowel disorder (27%), noting that patients could have more than one. Common concurrent medical conditions included those related to the gastrointestinal system (83%); conditions related to other systems in the body such as respiratory or kidney concerns (40%) or Avoidance Restrictive Food Intake Disorder (23%).
Characteristics of patients (n = 30) with functional bowel disorders seen in dietetic outpatient service.
On average, the wait time to see a dietitian (from referral to initial consult) was 4 months (SD 3.8) (Table 2). Patients were in the service for an average of 20 months (SD 15.4), with an average of 5 appointments (SD 4.8). Patients with functional bowel disorders affecting the upper gastrointestinal tract appeared to be seen more quickly (wait-time 3.7 months) and spend a shorter time in service (17.7 months) compared to patients with other types of functional disorders, but these differences did not reach statistical significance. Two-third (67%) of patients with lower gastrointestinal disorders had been discharged from the service, compared to 43% of patients with upper gastrointestinal disorders and 54% of patients with irritable bowel syndrome. Only one patient was discharged due to resolution of symptoms. All other reasons for discharge were: multiple did not attend (39%), lost to follow up (23%), patient request (23%), and patient not ready for care (8%) (data not shown). Of patients hospitalised in the last three years (n = 7, 23%), all had been seen by the dietitian during their inpatient admission.
Service-related indicators for outpatients with functional bowel disorders (n = 26) a , by type of functional bowel disorder.
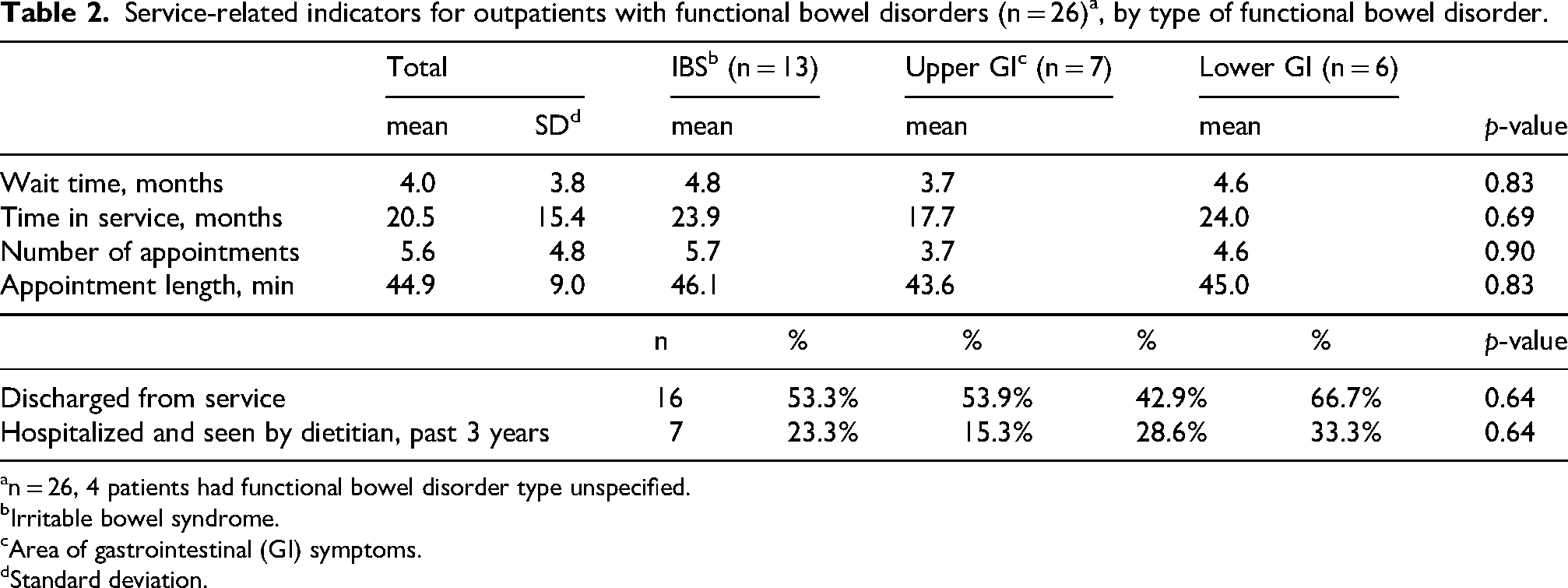
n = 26, 4 patients had functional bowel disorder type unspecified.
Irritable bowel syndrome.
Area of gastrointestinal (GI) symptoms.
Standard deviation.
All patients who were seen by the dietitian were given dietary education and advice for dietary modification relevant to their functional bowel disorder. (Table 3) Half of all patients were provided with artificial nutrition, supplements or pre- and probiotics were commonly recommended to 40% for patients and behavioural modifications were advised for 30% of patients. It appeared that patients with irritable bowel syndrome were most likely to receive advice on supplements or pre- and probiotics (54%) and behavioural strategies (39%) and patients with upper gastrointestinal disorders were more likely to receive artificial nutrition (71%), but the differences in nutrition-related interventions by type of functional bowel disorder did not reach statistical significance in any of the comparisons.
Nutrition-related interventions and patient characteristics for outpatients (n = 30) with functional bowel disorder, by type.
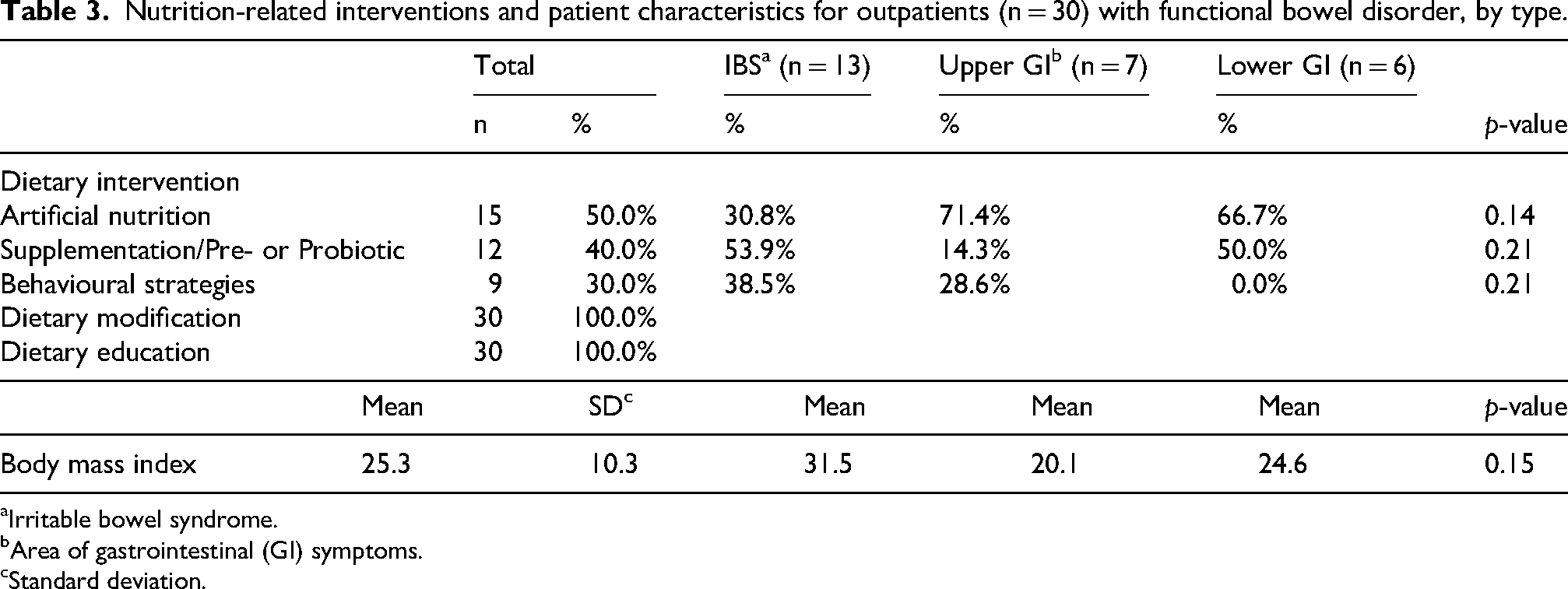
Irritable bowel syndrome.
Area of gastrointestinal (GI) symptoms.
Standard deviation.
Discussion
This study aimed to understand the experiences of patients with functional bowel disorders in a dietetic outpatient clinic. We found that patients reported a broad range of symptoms, and despite the use of both dietary and non-dietary strategies, few patients are discharged from care due to symptom resolution within a 2-year period. The cohort is resource-intense and diet therapies are delivered over significant time in service. Concurrently, this population group has difficulties maintaining nutrition via oral intake alone, particularly those with upper gastrointestinal concerns.
Patients diagnosed with functional disorders, especially those affecting the upper gastrointestinal tract, require intensive interventions over many appointments. As expected, functional dyspepsia was one of the most common subtypes of functional bowel disorders in the service (Talley, 2008). The difficulties in treating this cohort via diet intervention alone have been increasingly understood with emphasis placed on correcting pathophysiology mechanisms contributing to disorders rather than symptom management. Adding to the complexity of this cohort, ARFID was common among those with an upper gastrointestinal disorder. Recent research has highlighted that patients meeting criteria for ARFID present with a significant number of gastrointestinal complaints and these complaints may reinforce continued restrictive eating (Gibson et al., 2021). A correlation exists between weight loss due to restriction, malnutrition, and worsening GI symptoms. Our findings suggest it is important for clinicians to routinely screen for both malnutrition and ARFID to ensure timely referrals to other appropriate support services and avoid the perceived futility of treatment associated with worsening symptoms.
Lower gastrointestinal functional bowel disorders comprised approximately 20% of our patient cohort. Perhaps unsurprisingly, this group had a high percentage of patients being recommended pre- and pro-biotic therapies. Studies have shown altered gut microbiota and possible roles of microbial metabolites such as short-chain fatty acids, secondary bile salts and methane, associated with functional constipation (Wang and Yao, 2021). Given the potential effects of gut microbiota and metabolites on the occurrence and development of functional constipation, there is increasing interest in the use of pre- and pro-biotics.
Patients with irritable bowel syndrome waited nearly 5 months to see a dietitian in the outpatient clinic, with nearly 40% being advised behavioural strategies for symptom management. Interestingly, there has been new research that questions the efficacy of the low FODMAP diet for irritable bowel syndrome, which is one of the most common dietary interventions for patients with irritable bowel syndrome (Bertin et al., 2024). Current research is exploring the benefits of a symptom-modified mediterranean diet in creating a healthier gut microbiome and reduced IBS symptoms (Chen et al., 2024). A recent study comparing a low FODMAP diet to a standard diet in a Mediterranean population found both diets resulted in improvement of symptoms and quality of life at four weeks (Guerreiro et al., 2020). Research also demonstrates a positive impact of a low carbohydrate diet in symptom management. Recently, there has been further discussion of Mast Cell Diseases as they apply to irritable bowel syndrome and the reduced histamine load associated with a low FODMAP diet. (Harris et al., 2024).
Most studies have mainly addressed the short-term effectiveness (up to 4−6 weeks) of the low FODMAP diet. An initial restriction diet for a short period should be followed by a gradual reintroduction of food items containing FODMAPs in order to identify individual FODMAPs that should be restricted in the long term (Whelan et al., 2018). A recent randomised controlled study, including only patients with diarrhoea predominant IBS, evaluated the efficacy and acceptability of short term strict low FODMAP diet and of a long term “modified” FODMAP diet compared with traditional dietary advice, and showed that both, strict and modified low FODMAP diet, are acceptable and lead to significant improvement in symptoms and quality of life (Goyal et al., 2021). There is a significant difference between time spent in studies in the literature and time spent in the dietetic service (38% of patients with IBS spend >24 months), which may account for the differences in patient-reported outcomes. Ultimately, less restrictive dietary interventions may effectively reduce symptoms of irritable bowel syndrome and lead to more positive long-term outcome measures.
A strength of the current study is that it captured clinical practice in the real-world setting. The main limitation of this study was the lack of collection of regular outcome measures outside of symptom resolution. As stated above, functional bowel disorders have significant impact on quality of life which would have ideally been measured during reviews to gain a more nuanced insight into the benefits of different diet therapies. Specifically, dietitians could routinely ask about and record patient wellbeing and distress using tools such as the IBS-QOL Questionnaire (Patrick et al., 1998). The IBS-QOL questionnaire could be given to patients during their initial visit to the clinic and repeated prior to review, after trialling an intervention strategy. Additionally, the study relied on reviewing clinician notes which could be subject to reporter variability and bias. Last, our study population was small and, as such, may not have been sufficient to capture statistically significant differences in the experiences of these different cohorts of patients. Interestingly, only one patient reported resolution of symptoms. It is hypothesised that rates of symptom improvement may be higher if the reason for non-attendance was due to resolution of the presenting complaint. In future studies, there may be value in following up this cohort to explore reasons for non-attendance.
This study contributes to the limited evidence base evaluating dietetic models of care and dietary management strategies for adults with functional bowel disorders, with a particular focus on their impact on service utilisation. The study highlights the lack of meaningful clinical outcomes (e.g., symptom resolution) achieved through current dietary therapies. It would be beneficial to further explore the impacts of greater multidisciplinary team involvement, particularly the benefit of pharmacotherapy, the relationship between upper GI disorders and eating disorders, and the benefit of a variety of diets (such as the Mediterranean diet (Bamidele et al., 2025)), rather than just a low FODMAP diet, in managing functional bowel disorders.
Footnotes
Acknowledgements
The authors acknowledge Monique Terol and Michelle Teo for their assistance with data collection and their early contributions to this project.
Ethical considerations
The Mater Research Human Ethics Committee confirmed that this work meets the criteria for quality improvement and is exempt from full review by the Committee.
Ethical statement
This study was classified as a Quality Assurance activity under NHMRC guidance and was therefore exempt from Human Research Ethics Committee review (QACR/MML/108085).
Consent for publication
n/a.
Author contributions
SM conceived the study, oversaw data collection and drafted the manuscript. JU provided support for all aspects of the study, analysed the data and critically reviewed the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The research data are confidential.