
Abstract
Background
Body dysmorphic disorder (BDD) is a psychiatric condition that is not widely recognized, despite being prevalent worldwide. It involves obsessions related to one's physical appearance, and there is no appropriate screening tool for it in Turkey.
Aim
The aim is to adapt the Body Dysmorphic Disorder Screener (BDDS-5) for use in a Turkish cultural context, enabling the practical assessment of BDD.
Methods
This methodological study collected data between January and April 2025. The sample consisted of 405 young adults aged 19–29. Confirmatory factor analysis (CFA) was performed and examined using factor structure fit indices. Internal consistency was assessed using Cronbach's α coefficient, and the Eating Disorder Examination Questionnaire-13 (EDE-Q-13) was employed to evaluate convergent validity.
Results
According to the CFA results, the single-factor structure of the Turkish version of the BDDS-5 has been confirmed, and Cronbach's α has been determined as 0.88. A weak to moderate correlation was found between the EDE-Q-13 total score, the subfactors “shape and weight over-evaluation” and “body dissatisfaction,” and the BDDS-5 total score.
Conclusion
The BDDS-5 is a valid and reliable measurement tool that can be used to screen BDD in young adults. To the best of our knowledge, this is the first study in Turkey to adapt the BDDS-5 into Turkish, and the scale can serve as a valid and reliable guide for healthcare professionals and academic research.
Introduction
Body dysmorphic disorder (BDD) is a psychiatric disorder characterized by excessive and persistent preoccupation with defects in physical appearance that are nonexistent or minimal (Phillips and Susser, 2023). The BDD shares many similarities with obsessive-compulsive disorder (OCD) and is therefore classified under “OCD-related disorders” in the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5), a categorization that is maintained in the updated Diagnostic and Statistical Manual of Mental Disorders, 5th edition, text revision (DSM-5-TR) (APA, 2013, 2022). In BDD, there is excessive preoccupation with perceived appearance flaws, and although these perceived defects may appear insignificant to others, they constitute a significant source of distress for individuals with BDD (Jassi and Krebs, 2023). The BDD, which typically emerges during adolescence, is characterized by repetitive behaviors such as spending long hours preoccupied with perceived appearance flaws, a persistent urge to check mirrors, and attempts to correct perceived defects through cosmetic procedures (Hardardottir et al., 2019; Rück et al., 2024). This condition leads to significant distress as well as psychosocial impairment in individuals with BDD, resulting in important functional impairments such as leaving work, discontinuing education, and social avoidance (Trichas et al., 2025).
The BDD may occur across all populations, and its prevalence varies depending on the setting (Rück et al., 2024). The prevalence is reported to be approximately 1.9% in the general adult population, 2.2% among adolescents, and 3.3% among university students (Veale et al., 2016). Although BDD is more common in clinical settings and among young people, it is most frequently observed in the 18–24 age group, and its prevalence decreases with age (Gazzarrini and Perugi, 2017; Phillips and Susser, 2023). It has been suggested that this may be linked to the impact of unrealistic beauty and aesthetic standards portrayed in the media on young people (Alonazi et al., 2017; Marron et al., 2020). Some studies have reported that the prevalence of BDD is higher in women than in men (Rajabi et al., 2022; Veale et al., 2016). Haider et al. (2023) reported a higher prevalence of BDD symptoms among female students in Pakistan and found a significant positive association between BDD symptoms and depressive symptomatology. On the other hand, Hameed et al. (2025) reported that there was no significant difference in the prevalence of BDD between genders among medical students in Pakistan. Similarly, Haider et al. (2025) found that the prevalence of BDD among Chinese students did not differ by gender. Overall, there are still some gaps in our understanding of gender-specific differences in the prevalence of BDD (Trichas et al., 2025).
In order to establish a clear understanding of BDD for both healthcare professionals and patients, it is necessary to distinguish the concept of BDD from “perceived appearance flaws” and body dissatisfaction (Rück et al., 2024). Body dissatisfaction refers to the negative attitudes or feelings of dissatisfaction an individual exhibits toward their physical appearance, body measurements, body shape, and their body in general (Howard et al., 2017). On the other hand, perceived appearance flaws are associated with an individual's excessively negative evaluation of a specific physical trait. While not every perceived flaw increases body dissatisfaction, an increase in the importance attributed to perceived flaws can lead to a worsening of body dissatisfaction (Cash, 2004; Veale, 2004). In such cases, the excessive importance attributed to perceived flaws, the emergence of repetitive behaviors, and increased preoccupation may develop into BDD symptoms in some individuals (APA, 2013). Body dissatisfaction also differs from BDD in various ways. Compared to BDD, body dissatisfaction is more prevalent, tends to increase during adolescence, is generally transient, and may be influenced by social and cultural factors (Singh and Gadiraju, 2020). In a cross-cultural study, 74.3% of American students reported body dissatisfaction, while only 4% were diagnosed with BDD (Bohne et al., 2002). In BDD, there are appearance-related obsessions, repetitive and compulsive behaviors, and clinically significant distress (APA, 2022). The similarities between BDD and OCD, along with its diagnostic classification in the DSM-5-TR, indicate that this condition represents a more comprehensive psychopathological condition compared to general body dissatisfaction (APA, 2022; Rück et al., 2024). In short, body dissatisfaction is a nonclinical and common condition, whereas BDD is a clinical disorder characterized by obsessions and significant impairments in functioning. Given this theoretical distinction between body dissatisfaction and BDD, the reliable assessment of BDD symptoms in individuals belonging to high-risk groups, such as college students, is becoming increasingly important.
Eating disorders that share similarities with BDD in terms of clinical symptoms—such as excessive concern about physical appearance and body dissatisfaction—are also more common among young adults (Kollei et al., 2013; Potterton et al., 2020). A link between BDD and eating disorders has been reported, and BDD is considered to have a high potential to trigger eating disorders (Milligan and Middleman, 2022; Phillips and Susser, 2023). The presence of eating disorders negatively affects the quality of life of individuals with BDD (Rück et al., 2024). One study found that individuals with early-onset BDD (before the age of 18) are more likely to experience a lifetime eating disorder (anorexia nervosa or bulimia nervosa) than individuals with late-onset BDD (Bjornsson et al., 2013). The similarities between BDD and eating disorders make the diagnosis of BDD more difficult, especially in individuals who have concerns about body weight and exhibit certain abnormal eating behaviors (Dingemans et al., 2012). Early diagnosis of BDD is of great importance, as it can reduce the likelihood of development or persistence of eating disorders. For this reason, the regular use of a reliable screening tool for BDD is strongly recommended (Van Rood et al., 2023). However, the fact that BDD is a psychiatric disorder makes it difficult to diagnose. In some cases, individuals may hide their concerns out of fear that healthcare providers will view them negatively or underestimate them, which can lead to underdiagnosis of BDD (Al Shuhayb et al., 2023).
In the assessment of BDD, numerous screening tools have been developed and used, such as the Dysmorphic Concern Questionnaire (DCQ) and the Body Image Disturbance Questionnaire (Cash et al., 2004; Mancuso et al., 2010; Summers et al., 2022). In Turkey, clinical interviews, the Turkish Version of the Yale-Brown Obsessive-Compulsive Scale Modified for Body Dysmorphic Disorder, and the Body Dysmorphic Symptoms Scale (BDSS) have been used in studies for the assessment of BDD (Kaymak et al., 2009; Şeker et al., 2024; Uzun et al., 2003). Although these screening tools are clinically applicable, they do not fully align with DSM-5 criteria. To address this gap, Schieber et al. (2015) and Möllmann et al. (2017) developed DSM-5-aligned screening tools that include additional questions to assess eating disorders. However, it has been reported that the addition of these eating disorder-related questions makes the tools difficult to understand, unnecessarily lengthy, and tedious for individuals without eating disorders. In response to the need for a practical and easy-to-understand screening tool for a wide audience, Van Rood et al. (2023) developed the Body Dysmorphic Disorder Screener (BDDS-5). In Turkey, there is a recognized need for a screening instrument for BDD that is practical, easy to administer, and consistent with DSM-5 diagnostic criteria. Accordingly, the present study aimed to adapt the BDDS-5 to Turkish culture in a sample of young adults.
Methods
Study design
This study adapted the BDDS-5 to Turkish culture following the best practice framework for scale development and the guidance for researchers (Boateng et al., 2018). It employed a cross-sectional methodological design.
Settings and participants
The sample for this study consists of individuals aged 19–29 who are enrolled in faculties and colleges at Niğde Ömer Halisdemir University and who volunteered to participate. The study employed a convenience sampling method. Since a sample size of 300 or more is considered appropriate for factor analysis (Tabachnick and Fidell, 2019), the goal was to reach at least 300 individuals, and a total of 405 young adults were included. Individuals diagnosed with a condition that could negatively affect mental health, those with a serious chronic illness that could impact their nutritional status, individuals under 19 or over 29 years of age, and those who voluntarily declined to participate were excluded. The questionnaire was administered face-to-face to university students by trained research team members to ensure a consistent understanding of the items. The study did not include any clinical interviews or diagnostic confirmation, as its aim was to assess the validity and reliability of the screening tool in a nonclinical population. All researchers were trained in the standardized administration of the questionnaire, and no leading questions that could influence responses were asked during its administration.
Data collection
Research data were collected using a questionnaire between January and April 2025. The questionnaire form created by the researchers consisted of a sociodemographic information form, the Turkish version of the BDDS-5, and the Turkish version of the Eating Disorder Examination Questionnaire-13 (EDE-Q-13).
Sociodemographic information form
The form created by the researchers includes questions regarding the participants’ age, gender, education level, department, and income level. In addition, self-reported data on height (cm) and body weight (kg) were also collected from participants, which were used for calculating body mass index (BMI). The BMI values were then classified according to World Health Organization criteria as follows: <18.5 kg/m2 as underweight, 18.50–24.99 kg/m2 as normal weight, 25.0–29.99 kg/m2 as overweight, and ≥30.00 kg/m2 as obese (WHO, 2020).
Body dysmorphic disorder screener
Body dysmorphic disorder screener is a simple screening tool developed by Van Rood et al. (2023) based on the current version of the DSM-5 to facilitate the early identification of individuals with BDD and refer them to appropriate care. It consists of 12 items over two factors (BDD, eating disorder), with binary response options (true or false). The screening tool uses clear and simple language and can be safely administered to all individuals aged 8 and older. In the scoring of the scale, 1 point is assigned to each correct answer in Sections A, B, and C, and 1 point is assigned to each incorrect answer in Section D. The total score on the scale ranges from 0 to 12. The Cronbach's alpha coefficient for the original scale has been reported as 0.87 (Van Rood et al., 2023).
Eating Disorder Examination Questionnaire-13
Eating Disorder Examination Questionnaire-13, consisting of 28 items, was developed by Fairburn and Beglin (1994) to assess eating disorder psychopathology. The shortened version was developed by Lev-Ari et al. (2021). In this study, the Turkish version of the EDE-Q-13, validated and reliability-tested by Esin and Ayyıldız (2022), was used. The Cronbach's alpha of the original scale was reported as 0.89. The EDE-Q-13 consists of 13 items and five subfactors (eating restraint, shape and weight over-evaluation, body dissatisfaction, bingeing, purging). Items 1–3, items 4–5, items 6–7, items 8–10, and items 11–13 belong to the eating restraint, shape and weight overevaluation, body dissatisfaction, bingeing, and purging subfactors, respectively. The scale is scored on a 7-point Likert scale based on responses referring to the previous 28 days (0 days = 0 points, 1–5 days = 1 point, 6–12 days = 2 points, 13–15 days = 3 points, 16–22 days = 4 points, 23–27 days = 5 points, every day = 6 points). Subfactor scores are calculated by summing the item scores within each subfactor and dividing by the number of items in that subfactor. The total EDE-Q-13 score is calculated by summing all subfactor scores and dividing the sum by 5. Higher scores indicate greater eating-related psychopathology. In the current study, EDE-Q-13 was selected to assess the convergent validity of the BDDS-5 for the following reasons: (1) BDD and eating disorders overlap clinically, (2) BDD and eating disorders are frequently observed together, and (3) they both involve concerns related to body image (Samad et al., 2021).
Translation and adaptation of the scale
During the adaptation process of the scale, permission to use the scale was first obtained from Van Rood et al. via email (2023). Subsequently, the scale was translated from English into Turkish by expert translators proficient in both languages. The original scale and its Turkish translations were reviewed by a team of experts in the field of Nutrition and Dietetics (11 people), and the necessary corrections were made in a common translation format to finalize the scale. The Turkish form was then translated into English using the back-translation method (Wild et al., 2005).
After the scale adaptation process was completed, a pilot study was conducted using a questionnaire form via face-to-face interviews with 30 students studying at Niğde Ömer Halisdemir University to assess the comprehensibility of the items. The data obtained from the pilot study were not included in the final analysis.
Statistical analyses
R Studio Team (2021) software and SPSS 25.0 (IBM Corp, 2017) software package were used for the statistical analyses of the study data. Before conducting confirmatory factor analysis (CFA), descriptives and normality of the data were assessed with mean, standard deviation, skewness, and kurtosis values for univariate statistics and Henze–Zirkler value for multivariate statistics. CFA was performed using R (version 4.4.1), with the lavaan package (version 0.6–19). The model was estimated using maximum likelihood (ML) method, as it is considered robust to moderate violations of normality in large sample sizes (Yuan and Bentler, 2007). Model identification was achieved by fixing latent variable variances to one (std.lv = TRUE). Modification indices were examined to identify potential localized areas of misfit. No additional post hoc modifications were applied.
To test whether the hypothesized factor structure is confirmed by the adapted scale, a number of fit indices are used in the literature (Kyndt and Onghena, 2014; Schumacker and Lomax, 2022). In the current study, the chi-square (χ2) goodness-of-fit index (GFI), the adjusted GFI (AGFI), GFI, comparative fit index (CFI), Tucker–Lewis Index (TLI), root mean square residual (SRMR), and root mean square error of approximation (RMSEA) were used as fit indices. Acceptable cutoff points for fit indices have been presented in previous studies (Kyndt and Onghena, 2014; Schumacker and Lomax, 2022).
The internal consistency of the adapted scale was assessed using Cronbach's α reliability coefficient and composite reliability (CR), with a cutoff value of 0.6 and 0.7 (Nunnally and Bernstein, 1994), respectively, while the relationship between the item and its corresponding factor was assessed using the item-scale correlation value, with a cutoff value of 0.5 (Hajjar, 2018).
Convergent validity was examined at two complementary levels. First, convergent validity at the measurement-model level was evaluated using average variance extracted, which indicated that the latent constructs accounted for a substantial proportion of variance in their indicators with a threshold of 0.50 (Henseler et al., 2015). Second, external convergent validity was assessed using EDE-Q-13. The Spearman correlation coefficients between the composite scores of the two scales and the EDE-Q-13 subfactor scores were calculated, and the strength of the relationship between the scales was evaluated according to the cutoff values presented in the literature (Akoglu, 2018). In all statistical analyses, the significance level was set at p < 0.05.
Ethical considerations
Permission was first obtained from the scale authors to adapt the BDDS-5 to Turkish culture, followed by obtaining Ethics Committee Approval from Niğde Ömer Halisdemir University (Date: 03.12.2024, decision no: 2024/20-35). Prior to participation, all participants received comprehensive information about the study's objectives and procedures. Written informed consent was obtained from all participants, and participation was entirely voluntary. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Results
Sociodemographic characteristics of the participants
Data on the sociodemographic characteristics of the young adults who participated in the study are presented in Table 1. The mean age of young adults was 21.33 ± 1.88 years, and women constituted 61.2% of the sample. Of the participants, 82.0% held a bachelor's degree, and 50.6% were studying at health-related departments. Additionally, 48.6% of participants reported having a middle-income level. The mean BMI was 22.95 ± 4.33 kg/m2. According to BMI classification, 67.7% of participants were classified as normal weight, and 15.8% were classified as overweight. The mean values of BDDS-5 and EDE-Q-13 total scores were 3.13 ± 2.21 and 1.26 ± 1.19, respectively. The Kaiser–Meyer–Olkin measure of sampling adequacy was 0.892, and Bartlett's test of sphericity was significant (χ2 = 2039.99, p < 0.0001).
Participants’ sociodemographic characteristics (n = 405).
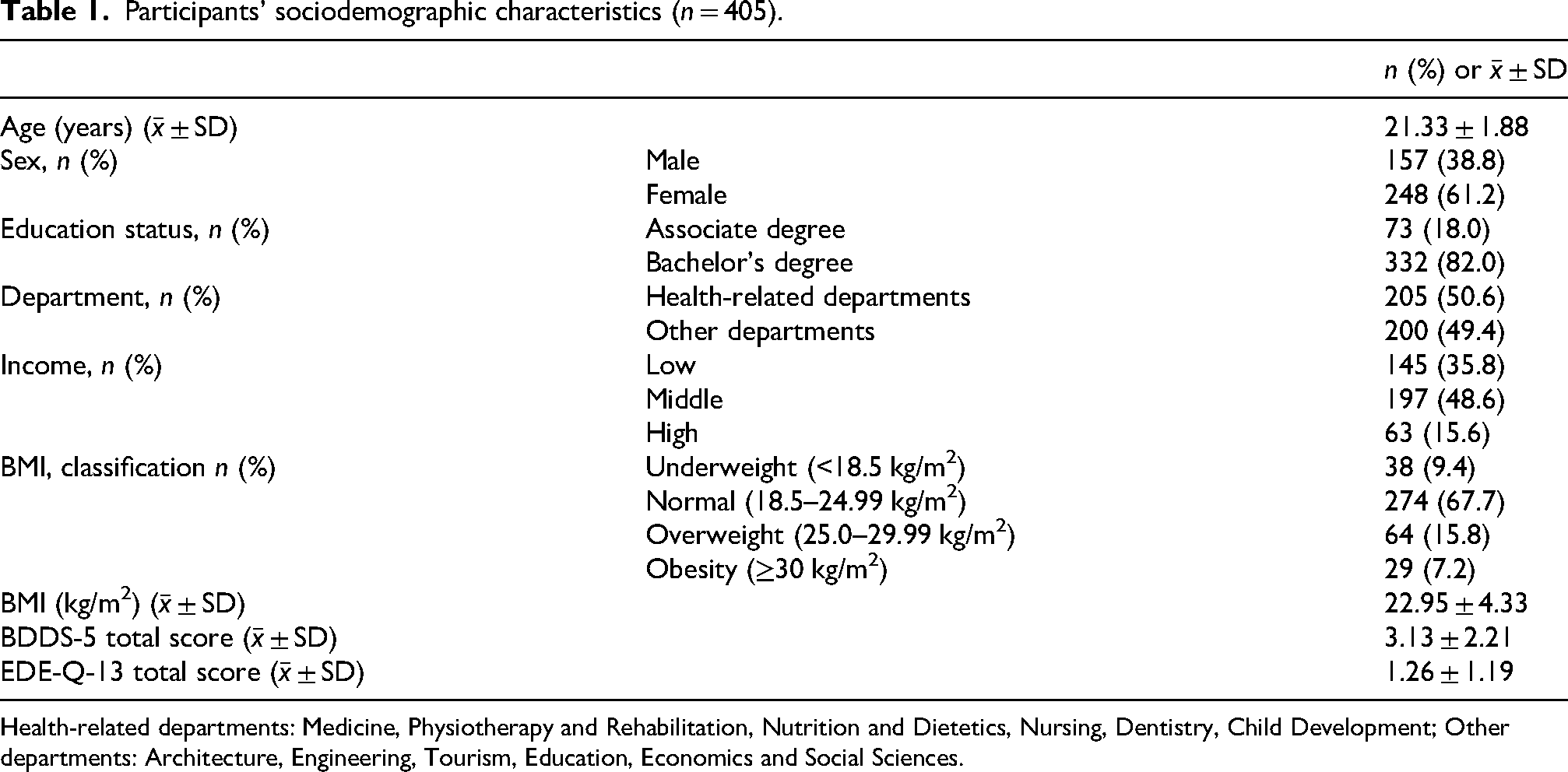
Health-related departments: Medicine, Physiotherapy and Rehabilitation, Nutrition and Dietetics, Nursing, Dentistry, Child Development; Other departments: Architecture, Engineering, Tourism, Education, Economics and Social Sciences.
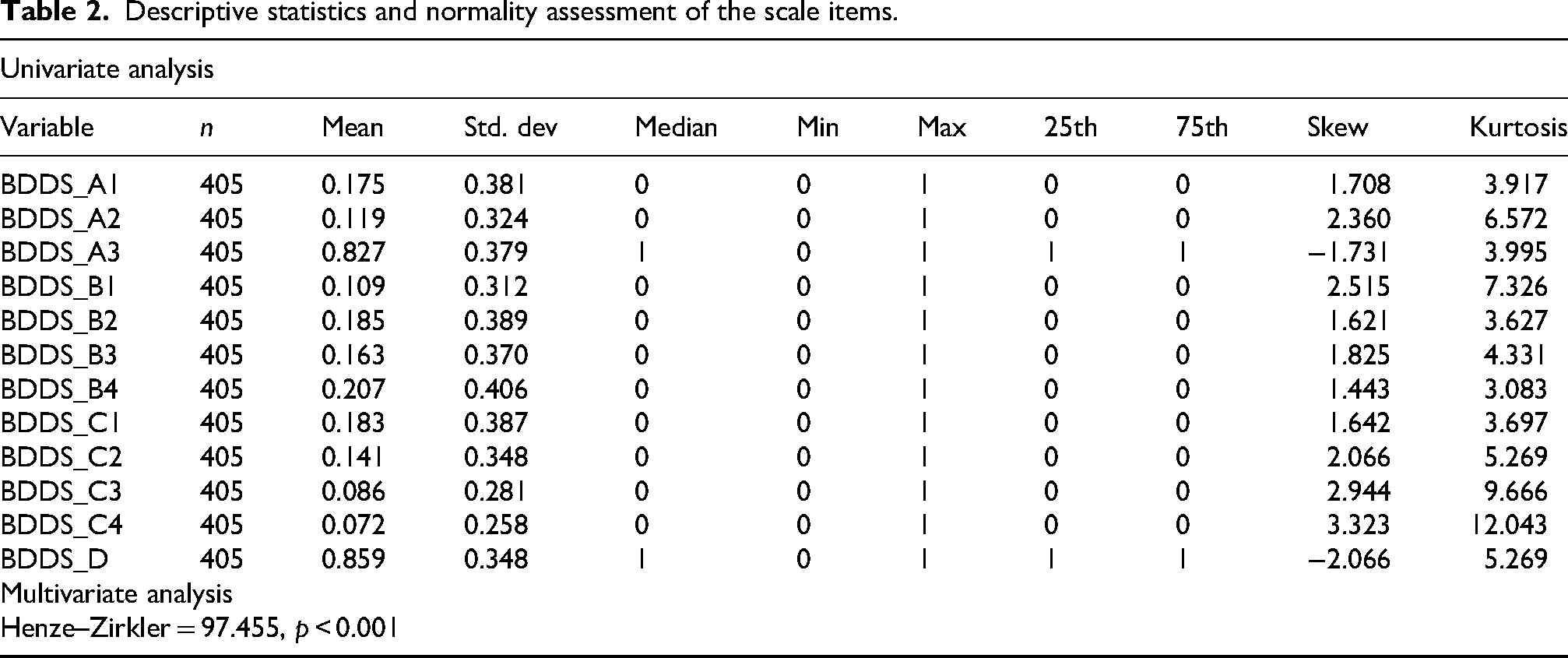
Descriptive statistics and normality assessment of the scale items.
Preliminary analysis
The descriptive statistics and normality indices (skewness and kurtosis) of the scale items are presented in Table 2. The dataset consisted of 405 participants with no missing data. Scale items were scored dichotomously (0 = absent, 1 = present). Descriptive statistics demonstrated variation in item endorsement rates (mean range = 0.07–0.86). Expectedly, for binary variables, skewness and kurtosis values exceeded traditional thresholds for normality (skewness range = |1.4|–|3.3|; kurtosis range = |3.1|–|12.0|).
Multivariate normality was evaluated using the Henze–Zirkler test, which revealed a statistically significant deviation from multivariate normality (p < 0.001). Nevertheless, given the categorical design of the indicators and the relatively large sample size (N = 405), the ML approach was deemed a robust alternative to address normality assumptions.
Confirmatory factor analysis
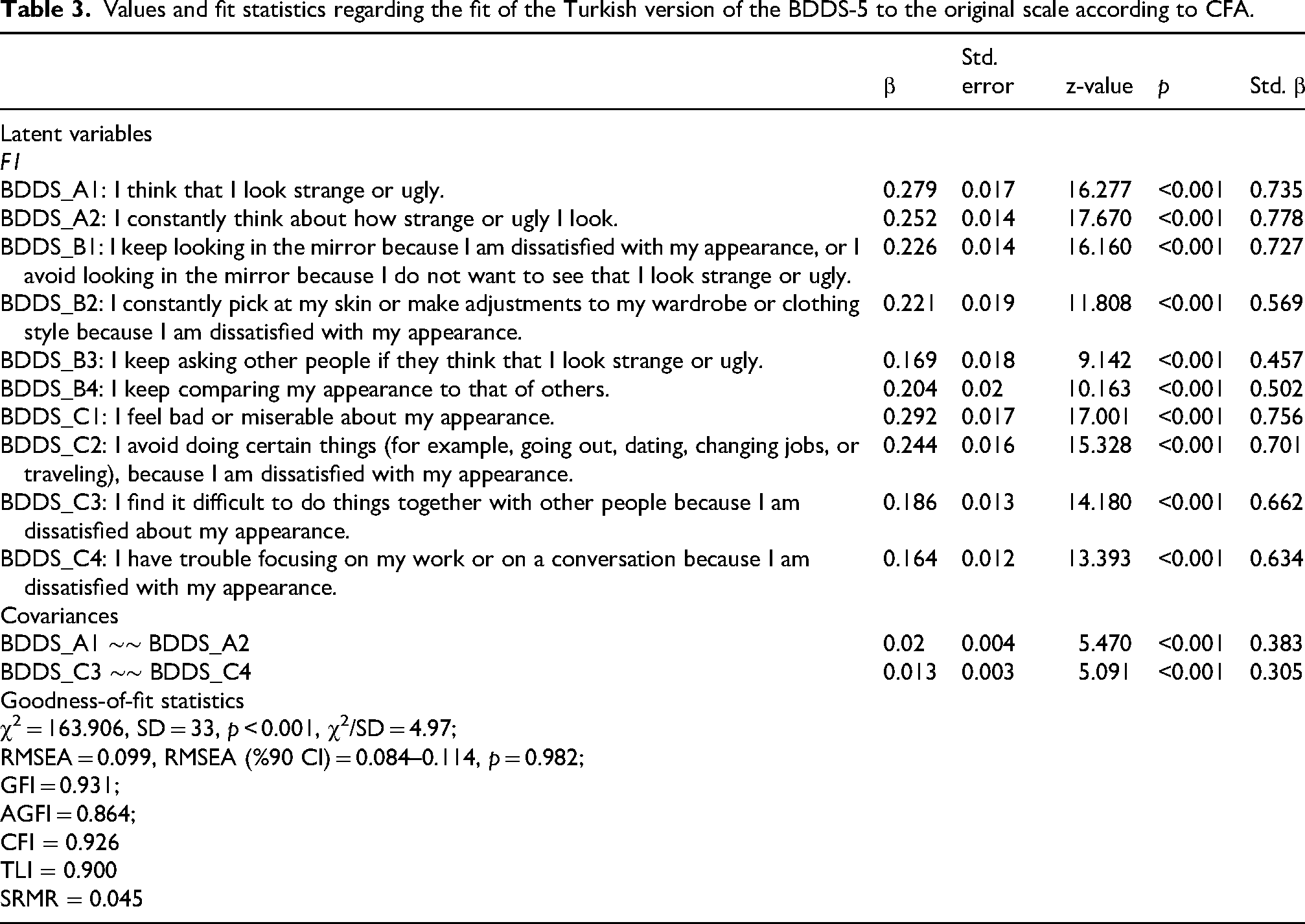
Confirmatory factor analysis was performed to test whether the structure presented in the original scale could be achieved with the adapted scale. The questions BDDS_A3 and BDDS_D have not been added to the model, taking into account the structure established on the reference scale. Modification indices were estimated since the first draft of the model showed poor fit according to the indicators. Suggested modification indices indicated the presence of significant residual covariances between the items BDDS_A1 and BDDS_A2 (MI = 52) and the BDDS_C3 and BDDS_C4 (MI = 38.5). Taking into account the similarity of expressions in the relevant items, the scale structure was reanalyzed by defining the correlations between the residuals. The revised model showed acceptable fit (χ2/df = 4.97, RMSEA = 0.10, GFI = 0.93, AGFI = 0.86, CFI = 0.92, TLI = 0.90, SRMR = 0.045) with statistically significant standardized factor loadings ranging between 0.50 and 0.78 (p < 0.001), meeting the recommended minimum threshold of 0.50 for scale adaptation research (Figure 1 and Table 3).
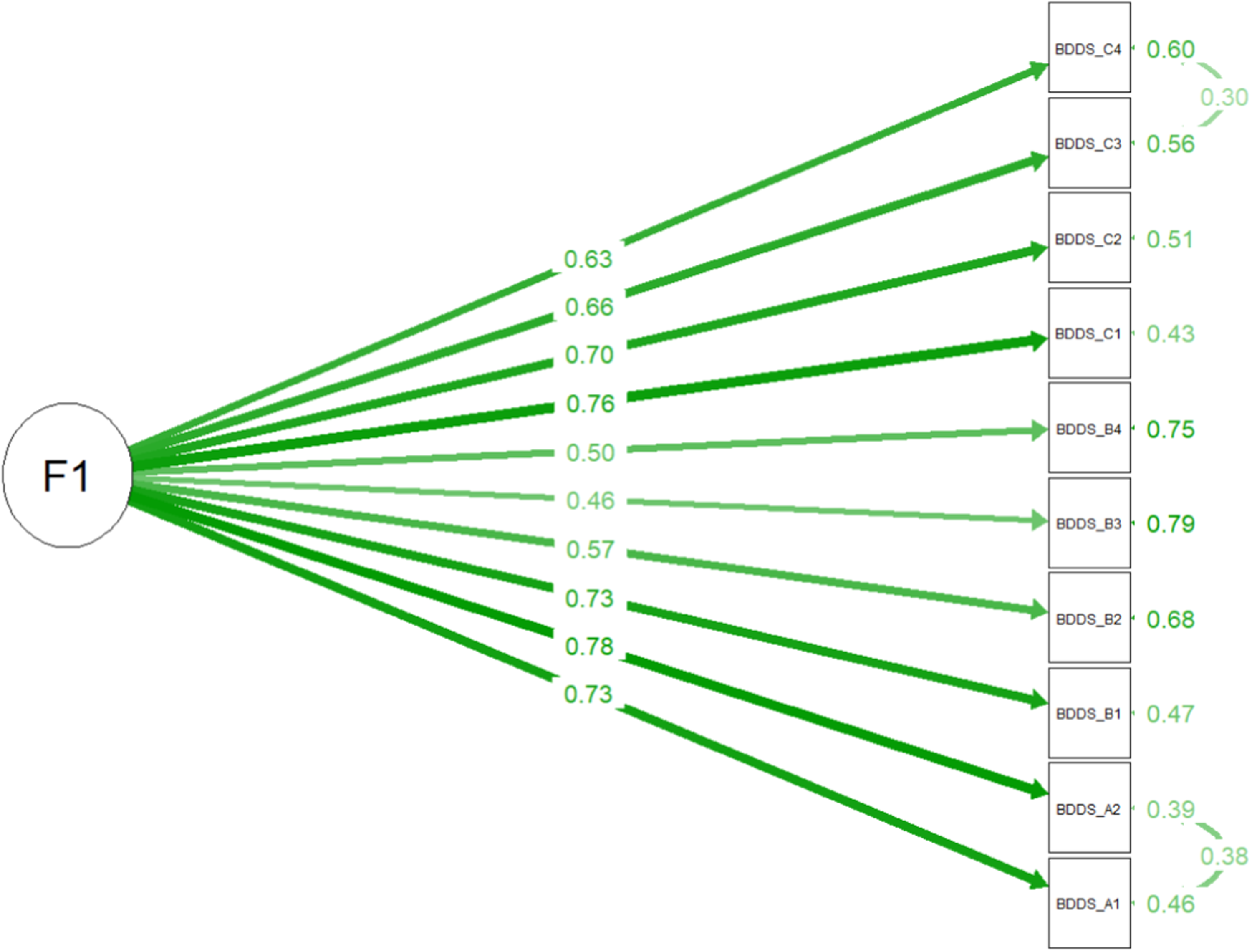
Confirmatory factor analysis (CFA) of the Turkish version of the Body Dysmorphic Disorder Screener (BDDS-5).
Values and fit statistics regarding the fit of the Turkish version of the BDDS-5 to the original scale according to CFA.
Reliability and convergent validity
The item analysis, internal consistency (Cronbach α and CR) and internal convergent validity of the Turkish version of the BDDS-5 are presented in Table 4. According to item-factor correlation values, only BDDS_B3 (r = 0.442) and BDDS_B4 (r = 0.49) showed slightly lower correlations below the acceptable thresholds. Given their theoretical relevance and contribution to content validity, the items were retained in the scale.
Item statistics and measurement model quality indicators.
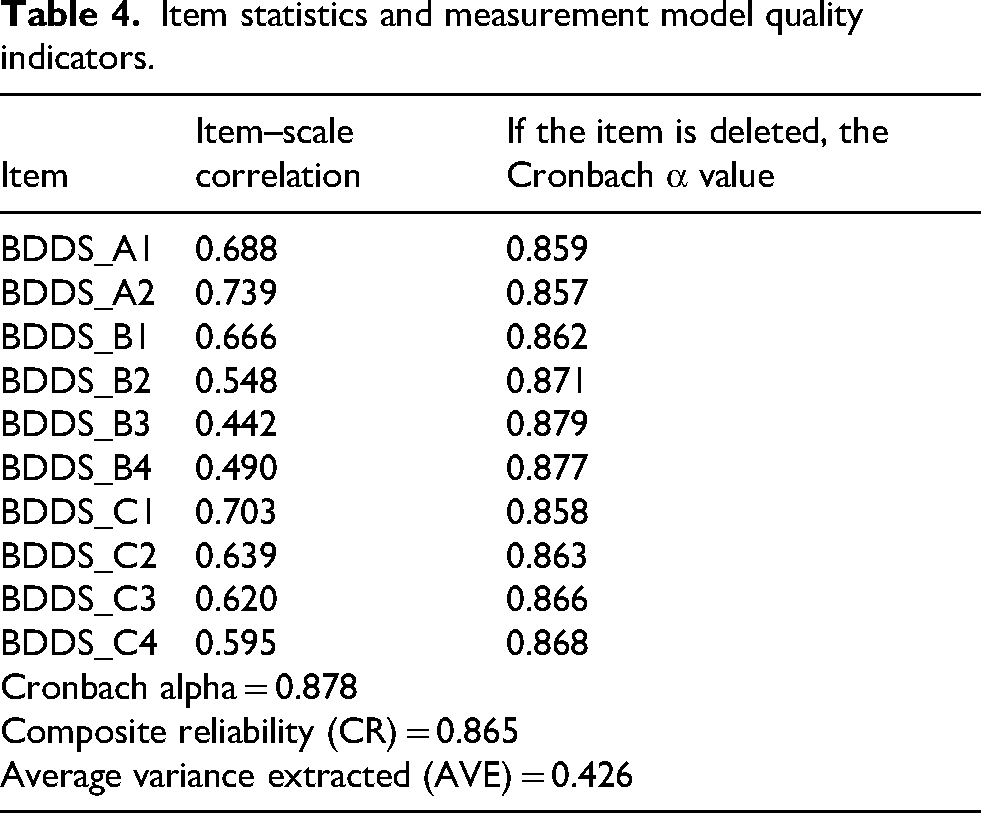
The Cronbach's α and CR values of the adapted scale were found to be 0.88 and 0.87, respectively, indicating high reliability and high internal consistency.
Average variance extracted value, standing for internal convergent validity of the scale, on the other hand, was 0.426, which is slightly below the conventional 0.50 criterion. However, as CR exceeded .60, convergent validity was considered as acceptable (Fornell and Larcker, 1981).
Correlations related to the external convergent validity of the BDDS-5 are presented in Table 5. Accordingly, there is a moderate-weak correlation between the total score of the scale and the total score of the EDE-Q-13. Similarly, there is a moderate-weak correlation between the EDE-Q-13 scale's subfactors of “shape and weight over-evaluation” and “body dissatisfaction” and the BDDS-5 composite score. However, the other subfactors of the EDE-Q-13 scale (eating restraint, bingeing, and purging) showed weak correlations with the BDDS-5 composite score.
Correlations between BDDS-5 and EDE-Q-13 subfactors and total scores.
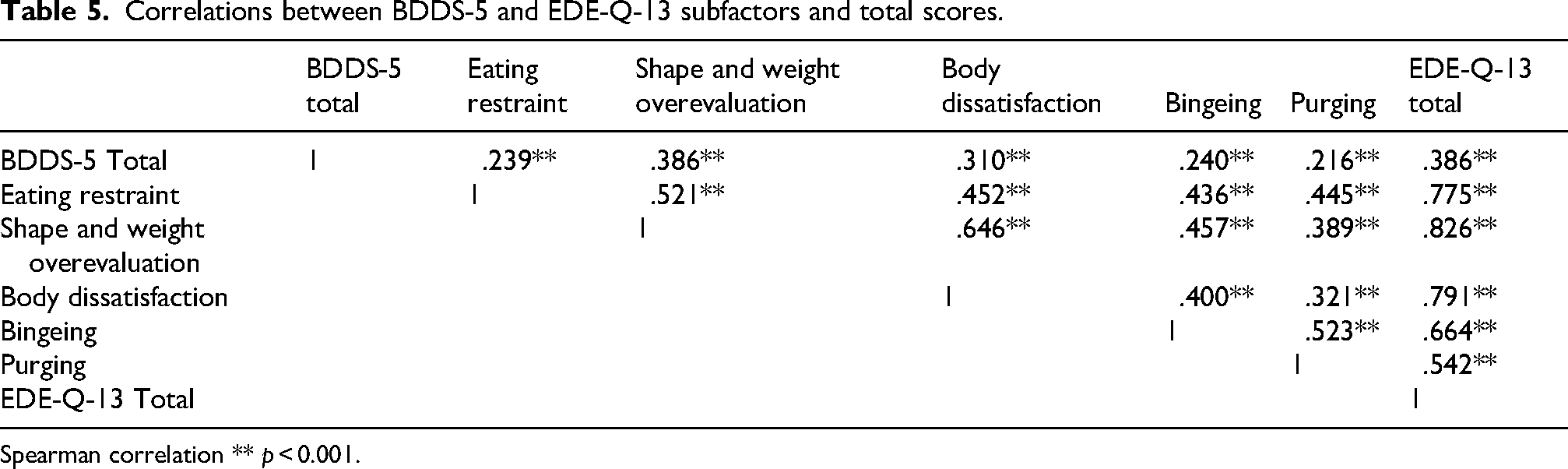
Spearman correlation ** p < 0.001.
Discussion
In this study, it was aimed to adapt the BDDS-5 scale—developed by Van Rood et al. (2023) in accordance with the DSM-5 criteria—into Turkish for use with a sample of young adults. To the best of our knowledge, this is the first methodological study to examine the validity and reliability of the BDDS-5. Body dysmorphic disorder typically has its onset in adolescence or early adulthood, with approximately two-thirds of individuals developing the disorder before the age of 18. It has been reported that the prevalence and the severity of BDD increase significantly during adolescence (Krebs et al., 2025). Therefore, the present study was conducted with young adults (university students), who are considered to be at high risk of developing BDD.
A high level of body image-related anxiety among university students, together with exposure to changes in environmental and lifestyle habits, increases the risk of BDD in this group (Veale et al., 2016). The prevalence of BDD in university students has been reported to vary by gender, with higher rates observed among women than their men counterparts (Shaffi Ahamed et al., 2016). Some studies examining the prevalence of BDD in young adults have used the Body Dysmorphic Disorder Questionnaire (Bartsch, 2007; Liao et al., 2010), while other studies have used the DCQ (Saab et al., 2024) and the Body Dysmorphic Disorder Assessment Scale (Cansever et al., 2003). Since discrepancies in results across different studies may originate from the variety of screening tools employed, standardizing assessment using a shorter and easier-to-administer tool—such as the BDDS-5, which meets DSM-5 criteria—could enable more accurate identification of BDD risk and support clinical practice.
The original BDDS-5 includes an additional section (Section S) that assesses eating disorders. When section S is included, the scale comprises two factors: BDD and eating disorder. The items in section S (S3, S4, and S5) are classified under the eating disorder factor. Since excluding items that assess eating disorders from the original scale did not negatively affect BDD screening results for the majority of participants (92%), it has been reported that Section S could be removed. In fact, removal of questions related to eating disorders from the BDDS-5 could facilitate its use and lead its wider adoption among the general population (Van Rood et al., 2023). For this reason, the items in Section S were not included in our study, and a single-factor structure was obtained.
In the original survey instrument, the authors suggested that the factor structure should be validated through CFA in future studies and even stated that item D could be removed depending on the population studied (Van Rood et al., 2023). In our study, based on the CFA results, a single-factor structure was identified. Similar to the original study, items A3 and D were excluded from the factor structure due to their low factor loadings. According to goodness-of-fit indices, GFI and AGFI values (0.931 and 0.864, respectively) indicated acceptable fit, while CFI, TLI, and SRMR values (0.926, 0.900, and 0.045, respectively) demonstrated good fit. In order to test the fit of the structure, we chose to use SRMR instead of the RMSEA for the one-factor model with 10 items. Previous research by Shi et al. (2019) suggests that SRMR provides more accurate assessments of close model fit and more reliable confidence intervals under various conditions, including models with a small number of observed variables and minor misfit. Their study further indicated that RMSEA shows an advantage over SRMR only in very specific scenarios, such as when fitting a one-factor model to a nearly identical two-factor model with highly correlated factors. When considering the fact that our model is accurately defined as a single-factor structure consisting of 10 items and does not yield results similar to a two-factor model, the SRMR is considered a more reliable fit index. Additionally, SRMR is less sensitive to sample size compared to RMSEA, making it a robust choice for our analysis. In the original scale, internal consistency assessed with Cronbach's alpha was reported as 0.87, while in the present study, it was 0.88, indicating a sufficient level of reliability (Field, 2024).
The BDD symptoms may be associated with psychopathologies that closely affect eating behavior (Aflakseir et al., 2021; Grant et al., 2017), and it has been reported that approximately one-third of individuals with BDD have a comorbid eating disorder diagnosis (Laughter et al., 2023). In a study examining the prevalence of BDD by eating disorder status, the incidence of BDD was found to be higher in individuals exhibiting eating disorder symptoms (Trott et al., 2021). Rabe-Jablonska and Sobow (2000) reported that one-quarter of individuals exhibited BDD symptoms 6 months prior to receiving a diagnosis of anorexia nervosa. Our study also demonstrated a moderate-to-weak relationship between BDD and eating disorders. All these findings support the possibility of a relationship between BDD and eating disorders. It is recommended that individuals who test positive in the BDD screening be clinically evaluated for eating disorders (Van Rood et al., 2023).
Impaired body image perception in individuals with BDD may lead to an increased anxiety related to weight gain. This may cause them to restrict their food intake and lose their appetite (Nascimento et al., 2012). A systematic review found that individuals with BDD and eating disorders exhibited similar levels of body dissatisfaction (Phillipou et al., 2019). In our study, the EDE-Q-13 subfactors, “shape and weight over-evaluation” and “body dissatisfaction,” were found to be moderately to weakly associated with BDD, while a weak relationship was observed with the “eating restraint” subfactor. These results suggest that high levels of body dissatisfaction and shape and weight overevaluation in BDD may negatively affect eating behavior and be associated with eating disorders. More research is needed to raise awareness about BDD and identify environments where BDD risk is high (Veale et al., 2016).
Strength and limitations
The use of the convenience sampling method in the study, where the majority of the sample consisted of women and individuals of normal body weight, may constitute a limitation in terms of sample diversity. Additionally, the fact that no test–retest was performed in the study and that the screening tool was not supported by a clinical evaluation are considered other limitations. Although BDD is closely related to obsessive-compulsive symptoms and body dissatisfaction, the limited assessment of the convergent validity of the BDDS-5 with only EDE-Q-13 is another limitation of the study. It is recommended that future studies conduct additional validity analyses using measurement tools related to obsessive-compulsive symptoms and body dissatisfaction. Nevertheless, the simplicity of the scale, which can be answered with a binary “yes” or “no” response, is the study's most salient strength. This scale can be utilized by individuals aged 8 and above who possess the capacity to read and write, and who can discern BDD without the aid of eating disorder screening questions. Furthermore, the first-time validation of BDDS-5 in a different culture, along with the assessment of its convergent validity, demonstrates the strength of this study in this regard.
Conclusions
This study found that the Turkish version of the BDDS-5 is a valid and reliable measurement tool that can be used for screening BDD in young adults. The use of the scale will contribute to healthcare professionals working in these fields as well as to academic studies. From a social perspective, the use of the BDDS-5 to identify BDD will guide the development of programs aimed at improving the quality of life for young people. Furthermore, early detection of BDD can help reduce/prevent eating disorders and suicide attempts, which are increasingly common among young adults. Although research on BDD has gained momentum, larger studies involving different populations are needed to understand the underlying causes.
Footnotes
Acknowledgments
The authors would like to thank all the young adults who participated in the study.
Ethical approval and informed consent statements
Permission has been obtained from the Ethics Committee of Niğde Ömer Halisdemir University (Date: 03/12/2024, decision no: 2024/20-35). The study was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all the individual participants included in the study.
Consent for publication
All authors reviewed the manuscript and gave their consent for the publication of the manuscript in Nutrition and Health.
Authors’ contributions
Ceren Şarahman Kahraman contributed to conceptualization, methodology, investigation, writing – original draft, and writing – review and editing; Cansu Memiç İnan contributed to conceptualization, methodology, and writing – review and editing; Özlem Çetiner contributed to validation and formal analysis; Emir Artma contributed to data curation; Meltem Soylu contributed to supervision. All authors approved the manuscript in its current form.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The data used and analyzed during the study are available from the corresponding author upon reasonable request.