
Abstract
Background
Muscle strength is a key determinant of functional capacity and quality of life, influenced by various modifiable factors including nutrition. Emerging evidence suggests a potential link between dietary acid load and musculoskeletal health, but its relationship with muscle strength and performance, especially in young healthy individuals, has not been fully clarified.
Aim
This cross-sectional study aimed to evaluate the relationship between dietary acid load, muscle strength, and physical performance in healthy young women.
Methods
A total of 151 women aged 18–35 years were recruited through convenience sampling from a university campus, excluding those with chronic diseases, physical disabilities, regular exercise habits, or special diets. Handgrip strength was measured using a dynamometer, and functional performance was assessed with a 10-step stair test. A 24-h dietary record was used to calculate the potential renal acid load (PRAL).
Results
Participants had a mean age of 22.5 ± 1.6 years. The average handgrip strength was 25.3 ± 4.8 kg, and the 10-step test times were 5.6 ± 0.9 s. The mean PRAL was 5.0 ± 14.1 mEq/day. There were no significant differences in handgrip strength or 10-step test results across PRAL tertiles (p > 0.05). While no significant correlation was found between PRAL and handgrip strength in the crude model (p = 0.115), a positive association appeared after adjusting for energy intake (p = 0.043). No significant correlation was found between PRAL and 10-step test results (p > 0.05).
Conclusion
A more acidic diet was positively associated with muscle strength, highlighting the potential impact of diet on muscle function.
Introduction
Muscle strength, defined as the maximum voluntary force that muscles can exert on the environment under specific test conditions, is a fundamental component of human physiology (Wang et al., 2024). It plays a crucial role in essential functions such as gait, upper limb movements, and posture maintenance. Consequently, factors that influence muscle strength have substantial implications for health and quality of life.
Multiple factors can negatively affect muscle strength, including aging, low levels of physical activity, inadequate dietary intake—particularly insufficient protein, which is directly linked to muscle protein synthesis—and the presence of metabolic diseases (Bowden Davies et al., 2019; Wolfe, 2006). Aging is strongly associated with sarcopenia and progressive loss of muscle mass and function, whereas physical inactivity accelerates muscle atrophy and impairs metabolic health (Bowden Davies et al., 2019; Larsson et al., 2019). The decline in muscle strength and muscle mass is closely associated with disability, reduced quality of life, and difficulties in performing daily activities (de Carvalho et al., 2019; Wu et al., 2017). Understanding these determinants is vital for developing strategies to preserve muscular function and overall well-being.
Among these factors, nutrition has emerged as a key determinant of musculoskeletal health. Previous studies examined the effects of macro- and micronutrient intake, as well as dietary patterns, on musculoskeletal health (Dominguez et al., 2025). In recent years, dietary acid–base balance has attracted increasing attention in relation to musculoskeletal health, as several studies have suggested that dietary acid load may influence both bone metabolism and muscle function (Applegate et al., 2017; Cao, 2017; Frassetto et al., 2018; Konieczynski et al., 2024). A widely used index in nutritional epidemiology, the potential renal acid load (PRAL), estimates dietary acid load based on protein, calcium, magnesium, phosphorus, and potassium intake (Remer and Manz, 1995). Since PRAL is directly derived from the intake of specific nutrients—particularly the macronutrient protein and the minerals phosphorus, potassium, magnesium, and calcium—examining the distribution of these nutrients across PRAL tertiles helps to better understand how dietary composition contributes to the body's acid–base balance and, consequently, to muscle function.
Dietary sources differ markedly in their acid–base effects. Foods that generally increase the net acid load of the body include animal-based foods such as meat, cheese and eggs, as well as many grain products, largely because of their sulphur-containing amino acids and phosphate content (Storz et al., 2022). In contrast, fruits and vegetables have low PRAL values and promote systemic alkalinity due to their bicarbonate content. Chronic acidosis may impair muscle function by reducing protein synthesis and stimulating proteolysis (Faure et al., 2017; Ho and Abramowitz, 2022).
These mechanisms have also been studied in the context of exercise, since acid–base balance is known to influence not only resting muscle function but also performance during physical activity. It has been hypothesized that an alkaline diet may enhance both aerobic and anaerobic exercise performance by facilitating the clearance of protons and inhibitory electrons produced during exercise. However, studies have yielded conflicting results. For instance, Battazza et al. (2023) found that sodium bicarbonate supplementation did not improve muscle performance, whereas Limmer et al. (2018) reported enhanced sprint performance after an alkaline diet for 4 days (Battazza et al., 2023; Limmer et al., 2018). These divergent findings highlight that dietary acid load may influence muscle performance differently depending on the context, population, and type of exercise tested. Despite these findings, studies specifically investigating the relationship between dietary acid load, muscle strength, and muscle performance are limited. While Mohammadpour et al. (2020) reported that higher dietary acid load was associated with greater muscle strength, Welch et al. (2013) observed a positive association between an alkaline diet and muscle outcomes.
However, existing evidence is limited and inconsistent, and the relationship between dietary acid load, muscle strength, and physical performance in young healthy women has not been clearly established. To address this gap, the present study aimed to evaluate the associations among dietary acid load, muscle strength (assessed by handgrip strength), and physical performance (assessed via a 10-step stair-climb test) in a sample of young healthy women.
Materials and methods
Design and setting
The study protocol complied with the principles of the Declaration of Helsinki. Written informed consent was obtained from all participants before enrollment. This cross-sectional study was conducted on the campus of the University of Health Sciences Turkey in Ankara, Turkey, between May 2022 and May 2024 and included only female students from the Gulhane Faculty of Health Sciences and Gulhane Faculty of Physiotherapy and Rehabilitation. Participants were recruited through convenience sampling among volunteers who responded to faculty-wide announcements. The sampling frame consisted of approximately 2000 undergraduate students enrolled at the University of Health Sciences Turkey. A total of 151 women were included. Inclusion criteria were being a healthy female undergraduate student aged 18–35 years and providing written informed consent. Exclusion criteria were the presence of self-reported, physician-diagnosed chronic diseases (e.g. diabetes, hypertension, thyroid disorders), physical disability, current smoking, engagement in regular exercise—defined as structured physical activity ≥3 times per week for ≥30 min during the past 3 months—or adherence to a special diet (e.g. vegetarian, vegan, ketogenic, low-carbohydrate, or medically prescribed therapeutic diets). All exclusion criteria were assessed by self-report using a structured questionnaire administered before the physical measurements. All data were collected in a controlled laboratory setting within the Department of Nutrition and Dietetics by trained personnel, including a registered dietitian.
This study was conducted exclusively among young adult women to reduce biological variability related to sex and age. Muscle strength, dietary habits, and acid–base metabolism differ markedly between males and females due to hormonal regulation, body composition, and differences in protein and energy metabolism (Nuzzo, 2023; Rein et al., 2024). Including only women helped to avoid the confounding effects of sex hormones such as testosterone and estrogen on muscle protein synthesis (Alexander et al., 2022). Young adults were chosen to minimize the influence of age-related muscle mass decrease (Shimokata et al., 2014). This homogeneous population therefore allowed for a clearer evaluation of the associations between dietary acid load and muscle strength under stable physiological conditions.
Anthropometric measurements
Height, body weight, body composition, waist circumference, and hip circumference were measured for all participants.
Height was measured in the standing position, barefoot, with the head in the Frankfort plane. Body weight and body composition were assessed in the morning using a bioelectrical impedance analyzer (Tanita BC-401, Tokyo, Japan). All anthropometric measurements were performed by a trained dietitian to ensure standardization. Participants were instructed to refrain from eating or drinking for at least 4 h prior to the test and to avoid intense physical activity and alcoholic beverages within the previous 24 h.
Body mass index (BMI) was calculated with the formula [body mass (kg)/(height (m)2)]. According to the World Health Organization classification, participants with a BMI below 18.50 were considered underweight, those with a BMI between 18.50 and 24.99 as normal weight, those with a BMI ≥25.00 as overweight, and those with a BMI ≥30.00 as obese (World Health Organization, 2004).
Waist circumference was measured with a rigid tape at the midpoint between the lowest rib and the iliac crest, while hip circumference was measured at the widest point of the buttocks with the researcher positioned laterally to the participant. The waist-to-hip ratio was then calculated, and values >0.90 in men and >0.85 in women were considered indicative of increased health risk (TÜBER, 2022).
Handgrip strength measurement
Handgrip strength was measured using a Baseline Hand Dynamometer (Baseline, New York, USA). Measurements were performed while the participant was standing, with the shoulder positioned in 15 degrees of abduction, the elbow fully extended, and the dynamometer held without contact with the trunk. Three consecutive measurements were taken for the right and left hands, and the mean values were recorded for analysis (Temur, 2017). Handgrip strength was selected because it is a simple, validated, and widely used proxy for overall muscle strength in epidemiological and clinical studies (Quattrocchi et al., 2024).
10-step stair test
The 10-step stair test was used to evaluate the functional performance of the participants (Lindeman et al., 1998; Nightingale et al., 2014). The test was performed on a standard staircase consisting of 10 steps, each 16 cm in height, located within the university building. Before the measurement, participants were given a brief familiarization trial to ensure safety and understanding of the task. During the task, individuals were instructed to ascend and then descend the staircase as quickly as possible without running and while avoiding falls. Use of the handrails was not permitted. The time taken to ascend and descend was recorded separately in seconds using a stopwatch by the same trained investigator.
Assessment of dietary acid load
A single 24-h dietary record was obtained from each participant to assess dietary intake. Records were collected by a trained dietitian through face-to-face interviews, during which participants were asked to recall all foods and beverages consumed in the previous day.
Dietary intake was assessed using a 24-h dietary record. To estimate portion sizes, participants were assisted by the Food and Nutrition Photo Catalog: Measurements and Quantities (Rakıcıoğlu et al., 2012), a validated Turkish reference atlas widely used in national nutrition surveys to standardize food portion estimation. The dietary data were analyzed using the Nutrition Information Systems Package Program (BEBIS, version 9), which is based on the Turkish National Food Composition Database.
PRAL (mEq/day) was calculated using the equation proposed by Remer and Manz (1995):
PRAL = (0.4888 × protein [g/day]) + (0.0366 × phosphorus [mg/day]) − (0.021 × potassium [mg/day]) − (0.0263 × magnesium [mg/day]) − (0.0130 × calcium [mg/day]). Higher PRAL values indicate a more acidogenic diet.
Statistical analysis
All statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS, version 22.0; IBM Corp., Armonk, NY, USA). Continuous variables are presented as means and standard deviations, and categorical variables are expressed as frequencies (n) and percentages (%). The distribution of continuous variables was assessed for normality using the Kolmogorov–Smirnov test. Depending on the distribution, appropriate parametric or nonparametric tests were applied. Comparisons across tertiles of dietary acid load (PRAL) were conducted using one-way analysis of variance. The chi-square test was applied to evaluate differences in categorical variables. Associations among the dietary acid load (PRAL), hand grip strength, and 10-step stair test results were examined using linear regression analysis with different adjustment models. Two models were designed: a crude model (unadjusted) and Model 1 (adjusted for total energy intake). Energy intake was considered as a covariate because it may influence both dietary acid load and muscle strength. Statistical significance was set at p < 0.05, and 95% confidence intervals (CIs) were reported.
The sample size was calculated using the Raosoft sample size calculator. According to the official student records of the Gulhane Faculty of Health Sciences and Gulhane Faculty of Physiotherapy and Rehabilitation, the source population for this study consisted of approximately 2000 female students aged 18–35 years. Based on this sampling frame, a minimum of 66 participants was required to achieve a 90% confidence level with a 10% margin of error. To enhance the reliability and statistical power of the findings, we aimed to recruit at least 150 participants, and ultimately 151 women were included in the study.
Results
The baseline characteristics of the included participants are presented in Table 1. The mean age was 22.5 ± 1.6 years, the mean body weight was 58.1 ± 10.1 kg, and the mean height was 163.9 ± 5.8 cm. The mean waist circumference was 69.8 ± 7.5 cm, the hip circumference was 96.0 ± 9.7 cm, and the waist/hip ratio was 0.7 ± 0.2. The body fat percentage was 26.6 ± 7.0%, and the body muscle percentage was 69.4 ± 6.5%.
Main characteristics of the participants.
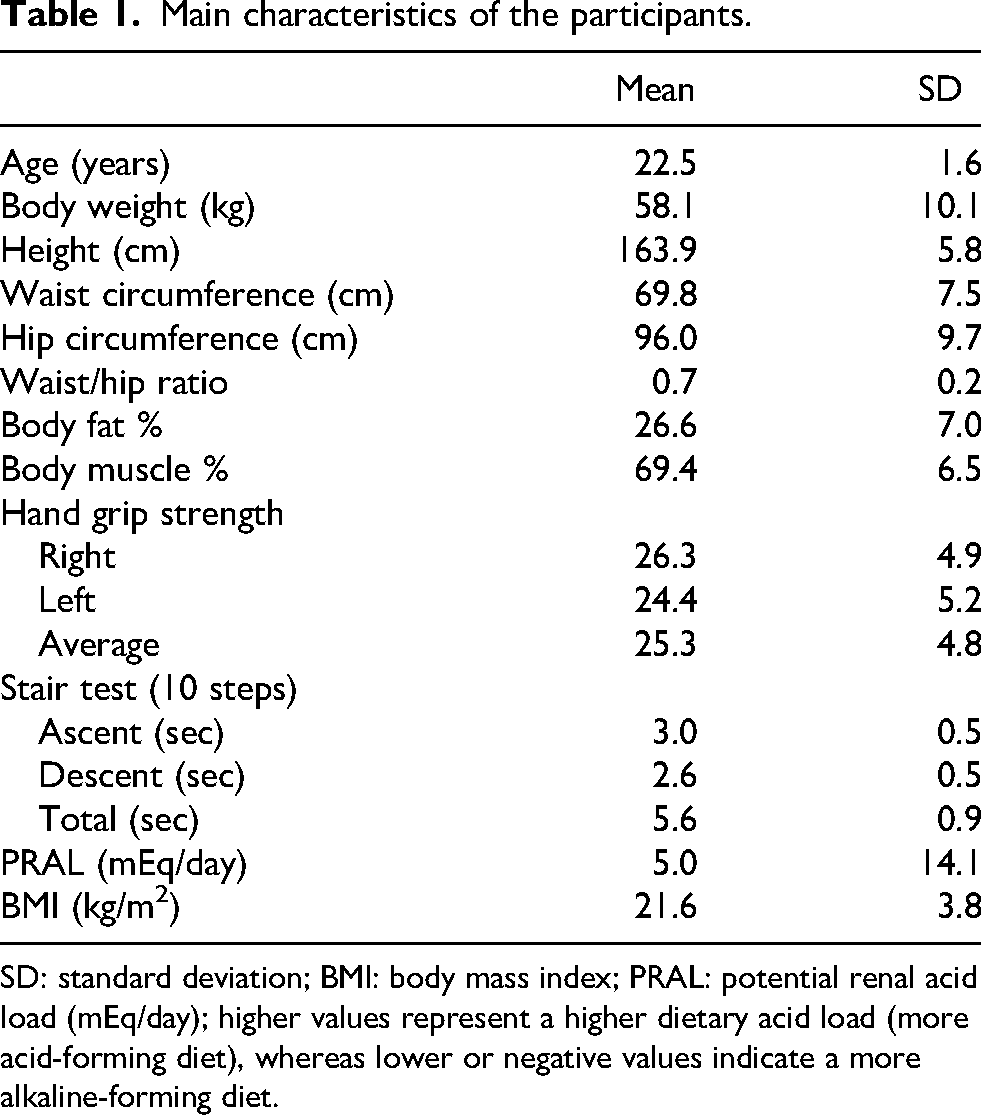
SD: standard deviation; BMI: body mass index; PRAL: potential renal acid load (mEq/day); higher values represent a higher dietary acid load (more acid-forming diet), whereas lower or negative values indicate a more alkaline-forming diet.
The mean handgrip strength was 26.3 ± 4.9 for the right hand and 24.4 ± 5.2 for the left hand, with an overall mean of 25.3 ± 4.8. The mean 10-step stair test times were 3.0 ± 0.5 s for ascending, 2.6 ± 0.5 s for descending, and 5.6 ± 0.9 s in total.
The mean PRAL value of the participants was 5.0 ± 14.1 mEq/day, and the mean BMI was 21.6 ± 3.8 kg/m2. The main characteristics of the participants according to the tertiles of PRAL are presented in Table 2. No significant differences were observed across tertiles for these parameters (p > 0.05). Overall, baseline anthropometric and performance characteristics did not differ significantly across PRAL tertiles.
General characteristics of individuals according to the tertiles of PRAL.
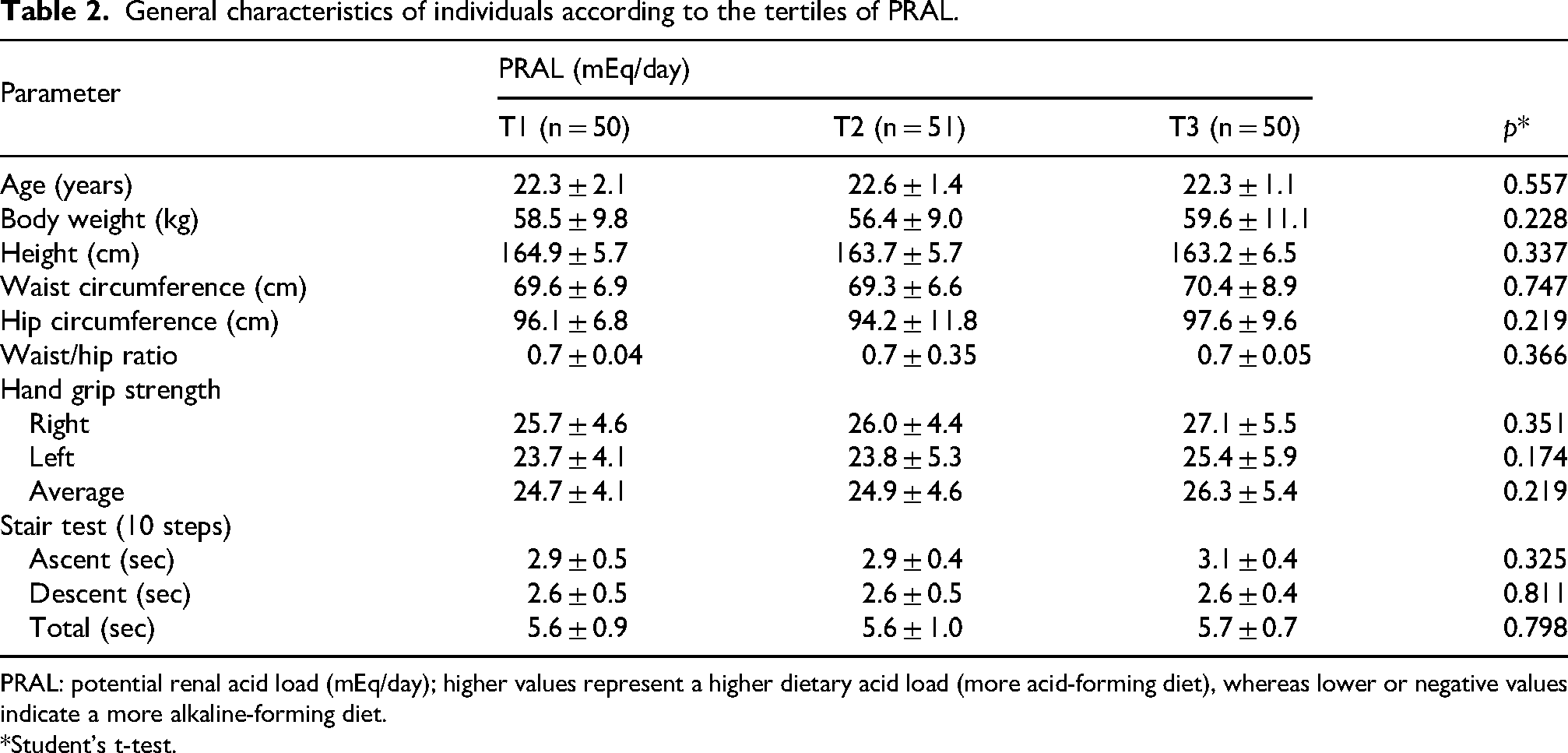
PRAL: potential renal acid load (mEq/day); higher values represent a higher dietary acid load (more acid-forming diet), whereas lower or negative values indicate a more alkaline-forming diet.
*Student's t-test.
The participants’ macro- and micronutrient intakes according to the tertiles of PRAL are shown in Table 3. Total energy, protein, fat, and phosphorus intake were higher in the T3 group compared with T1 and T2 (p = 0.002, p < 0.001, p = 0.003, p < 0.001, respectively). Potassium, magnesium, and fiber intake were significantly greater in T1 than in T2 and T3 (p < 0.001, p = 0.020, and p = 0.019, respectively). There were no significant differences in carbohydrate or calcium intake between the groups (p > 0.05). These findings indicate that higher PRAL values were mainly driven by higher energy, protein, fat, and phosphorus intake, whereas lower PRAL values were characterized by greater potassium, magnesium, and fiber intake.
Macro- and micronutrient intakes of subjects in different PRAL tertiles.
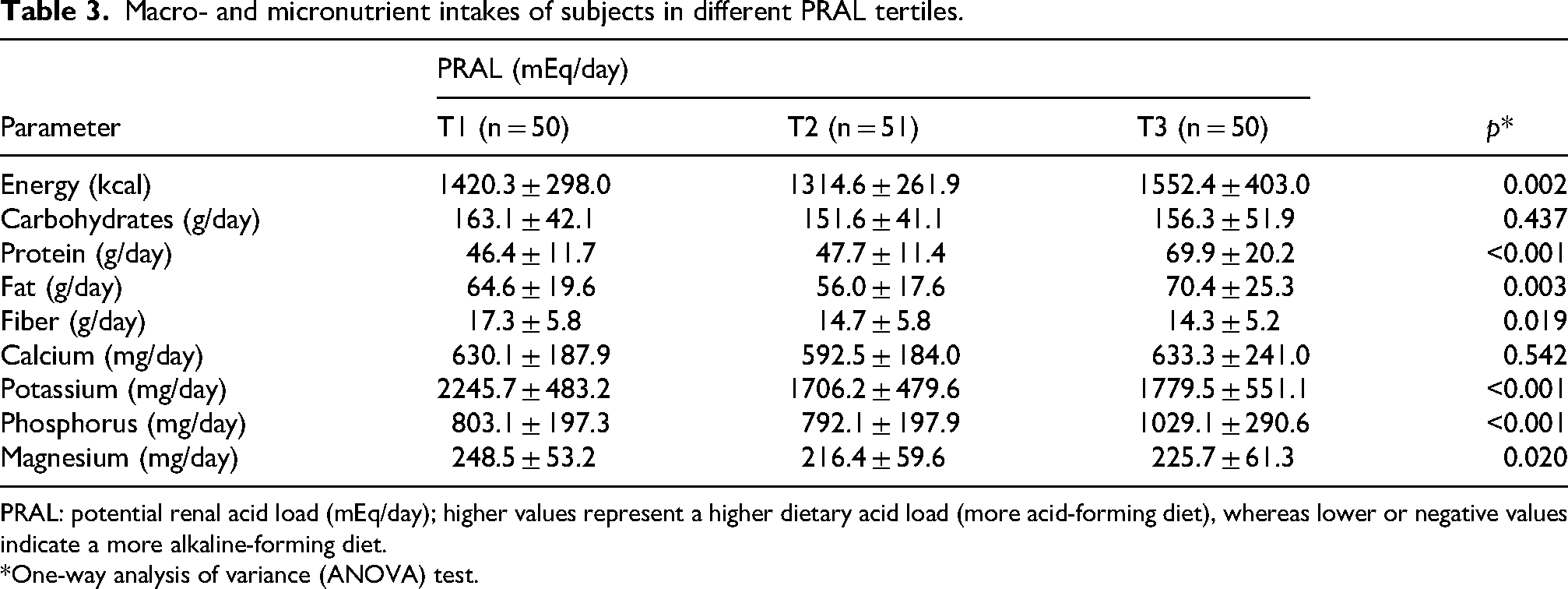
PRAL: potential renal acid load (mEq/day); higher values represent a higher dietary acid load (more acid-forming diet), whereas lower or negative values indicate a more alkaline-forming diet.
*One-way analysis of variance (ANOVA) test.
Correlations between the PRAL, handgrip strength, and 10-step test results are shown in Table 4. Although no significant relationship was observed between PRAL and mean handgrip strength in the crude model (p = 0.115), a significant positive association emerged in Model 1 (p = 0.043). No significant associations were found between the PRAL and the 10-step test results either in the crude model or Model 1 (p = 0.460 and p = 0.516, respectively). Taken together, PRAL was not associated with physical performance but showed a modest positive association with handgrip strength after adjustment for total energy intake.
Correlations among the PRAL, hand grip strength, and 10-step test results.
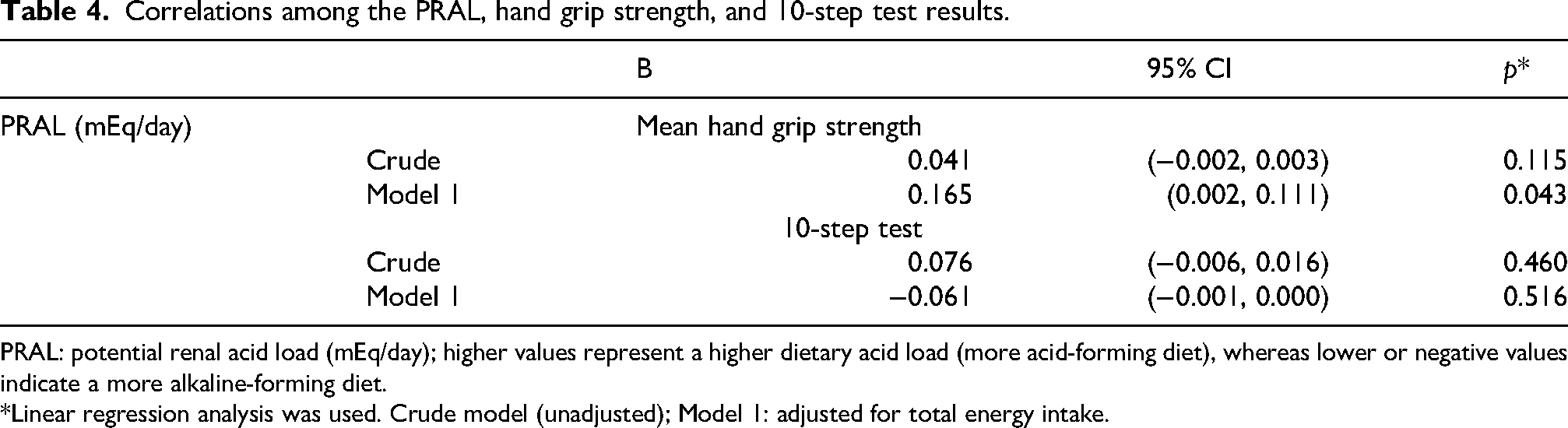
PRAL: potential renal acid load (mEq/day); higher values represent a higher dietary acid load (more acid-forming diet), whereas lower or negative values indicate a more alkaline-forming diet.
*Linear regression analysis was used. Crude model (unadjusted); Model 1: adjusted for total energy intake.
Discussion
In the present study, no significant differences in muscle strength were observed across tertiles of PRAL; however, linear regression analysis revealed a positive association between PRAL and mean handgrip strength in young healthy women. In addition, total energy, protein, fat, and phosphorus intake were highest in the PRAL T3 group, whereas magnesium, potassium, and fiber intake were highest in the PRAL T1 group. These findings suggest that higher PRAL values may reflect increased protein and energy intake, which are known to support muscle protein synthesis and strength, while lower PRAL values may be linked to greater consumption of alkalizing foods such as fruits and vegetables, which benefit metabolic health but may not directly enhance muscle strength in this population.
The dietary acid–base balance is determined by the intake of hydrogen ion-generating foods such as meats, cereals, and dairy products, and base precursor-providing foods such as fruits and vegetables. The PRAL formulation quantifies this effect by considering protein, calcium, magnesium, phosphorus, and potassium intake. In the current study, protein and phosphorus intake were greater in the T3 group, reflecting a more acidogenic dietary pattern, whereas potassium and magnesium intake were greater in the T1 group, reflecting a more alkalogenic pattern. These nutrient distribution trends are consistent with the underlying PRAL concept and may help explain the observed relationship between PRAL and muscle-related outcomes.
When compared with previous research, our results show both similarities and differences. Gholami et al. reported that increasing PRAL was associated with decreased intake of potassium, magnesium, calcium, and carbohydrates (Gholami et al., 2023), whereas Mohammadpour et al. found that PRAL increased with higher protein, carbohydrate, and total fat intake, and lower potassium intake (Mohammadpour et al., 2020). In our sample, protein intake and phosphorus intake were higher in the highest PRAL group (T3), while potassium and magnesium were higher in the lowest PRAL group (T1), which is in partial agreement with these studies. Methodological differences may explain the discrepancies, as we used 24-h dietary records whereas the cited studies used food frequency questionnaires to estimate PRAL, and the study populations differed in age and BMI status. Thus, both the dietary assessment tool and participant characteristics likely contributed to the observed variation across studies.
To the best of our knowledge, the literature on dietary acid load and musculoskeletal outcomes remains inconsistent. Our finding of a positive association between PRAL and handgrip strength is in line with the results of Mohammadpour et al., who also reported a positive relationship between dietary acid load and muscle strength in healthy adults (Mohammadpour et al., 2020). In contrast, Welch et al. observed that more alkaline diets were associated with greater muscle mass indices, and Hayhoe et al. similarly reported a negative association between PRAL and fat-free mass (Hayhoe et al., 2020; Welch et al., 2013). These divergent findings may largely reflect differences in outcome measures.
While our study and that of Mohammadpour et al. assessed muscle strength directly using a handgrip dynamometer, Welch and Hayhoe focused on muscle mass measured via dual-energy X-ray absorptiometry or bioelectrical impedance analysis (Hayhoe et al., 2020; Welch et al., 2013). It is well established that muscle strength and muscle mass, although related, do not always change in parallel. Strength can be maintained despite reductions in muscle mass due to factors such as neuromuscular adaptations and motor unit recruitment (Deschenes et al., 2022; Riviati and Indra, 2023). Therefore, studies that evaluate muscle mass may not yield the same associations as those that measure strength directly, which could explain why dietary acid load appears to be positively related to strength in some studies but negatively related to mass in others.
The role of nutrition, and particularly dietary acid load, in muscle performance has been increasingly emphasized, especially in the context of athletic populations. A low PRAL diet is expected to enhance anaerobic exercise performance by promoting systemic alkalosis, increasing bicarbonate availability, and facilitating the clearance of hydrogen ions during high-intensity exercise. In support of this, Caciano et al. reported that time to exhaustion was 21% longer under a low PRAL diet, and Limmer et al. found improved 400-meter sprint performance after a short alkalizing dietary intervention (Caciano et al., 2015; Limmer et al., 2018). These findings suggest that dietary acid–base balance may act as a natural modulator of exercise performance.
In contrast, our study did not identify a significant association between PRAL and performance on the 10-step stair test. Several factors may account for this discrepancy. First, our participants were healthy but non-athletic young women, in whom anaerobic capacity is typically lower and less responsive to dietary influences compared to trained athletes. Second, unlike previous studies, no dietary intervention specifically targeting acid–base balance was implemented in our study. Third, although practical and easy to administer, the 10-step stair test may not be sufficiently sensitive to detect subtle differences in performance related to dietary acid load. Therefore, our findings suggest that dietary acid load may be more closely related to muscle strength than to short functional performance tasks in this specific population.
This study has several limitations. First, dietary acid load was assessed using a single 24-h dietary record, which may not fully capture habitual dietary intake; multiple-day recalls would provide more reliable estimates. To minimize this limitation, dietary records were collected through face-to-face interviews conducted by trained dietitians, and portion sizes were cross-checked with a validated food photo catalog to improve accuracy. Second, muscle strength was assessed using handgrip dynamometry. Although handgrip dynamometry is not a laboratory-based gold-standard technique such as isokinetic dynamometry, it is a practical and widely accepted method for assessing muscle strength in field studies. Third, muscle performance was evaluated solely with the 10-step stair test, which, although practical, may not fully reflect anaerobic or functional capacity. This limitation was partially addressed by ensuring that the test was administered under standardized conditions by the same investigator, reducing measurement variability. Fourth, the study population consisted of young women from a single faculty, which may limit the generalizability of the findings to other age groups, sexes, or broader populations. However, this homogeneity also reduced confounding by age, sex, and chronic disease, thereby strengthening the internal validity of our results. Another limitation is that the use of hormonal therapies, including oral contraceptives or treatments for conditions such as polycystic ovary syndrome, was not specifically assessed. As hormonal status may influence muscle mass and strength, residual confounding cannot be excluded.
Despite these limitations, the study also has important strengths. All measurements were performed by the same trained investigator using standardized protocols, and the study included a homogeneous sample of healthy young women, reducing confounding effects of age, chronic disease, or sex differences. Moreover, the combined evaluation of dietary intake, muscle strength, and physical performance within the same cohort adds value to the existing literature.
In conclusion, we observed a significant positive association between higher dietary acid load and muscle strength, suggesting that this relationship may be driven more by nutrient composition—particularly higher protein intake—than by acid–base effects alone. Clinically, these findings underscore the importance of diet quality and acid–base balance in musculoskeletal health, even at an early age. They may have implications for nutritional counseling aimed at preventing muscle decline, supporting healthy aging, and informing rehabilitation strategies. While these results should be interpreted with caution, they highlight a potentially modifiable factor that deserves further investigation. Future longitudinal and interventional studies are warranted to confirm these associations and to clarify the mechanisms linking dietary acid–base balance with muscle strength and performance.
Footnotes
Ethical approval and informed consent
This study was approved by the University of Health Sciences, Gulhane Education and Research Hospital Ethics Committee (Approval date/number: 27 June 2022/2022-219).
Consent for publication
All authors have reviewed the content of this manuscript and approve the submission of this manuscript for review. This manuscript has not been published or submitted for publication elsewhere.
Author contributions
KTA: conceived and designed the study, supervised data collection, conducted statistical analysis, interpreted the data, drafted the manuscript, and reviewed the manuscript for intellectual content. SA, BG, ET: assisted in the data collection and contributed to data interpretation, and supported the data acquisition. All authors reviewed and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Türkiye Bilimsel ve Teknolojik Araştırma Kurumu (grant number 1919B012107468).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.