
Abstract
Background
Children are particularly vulnerable to the psychological and nutritional consequences of natural disasters such as earthquakes. Understanding the relationship between mental health outcomes and food insecurity is essential for effective post-disaster interventions.
Objectives
This study aimed to assess the prevalence of post-traumatic stress disorder (PTSD), anxiety, and depressive symptoms among children exposed to the 2023 earthquake in Türkiye, and to examine their nutritional status and household food security.
Methods
A multicenter, cross-sectional survey was conducted between March and August 2025 among 782 children aged 6–17 years from twelve earthquake-affected provinces. Participants were recruited using stratified cluster sampling from schools and community health centers. Psychological outcomes were assessed using validated instruments (CPSS, SCARED, CDI). Nutritional status was evaluated using anthropometric measurements, dietary diversity indicators, and standardized food security scales.
Results
Overall, 21.7% of participants met the CPSS cut-off for probable PTSD, with a higher prevalence among girls. Anxiety symptoms were identified in 25.8% and depressive symptoms in 21.4% of children. Nutritional assessment showed that 11.3% were underweight and 18.6% were overweight or obese. Additionally, 40.3% of households experienced food insecurity.
Conclusion
Mental health problems and nutritional vulnerability frequently co-occur among children after earthquake exposure. Integrated interventions addressing both psychological well-being and food security are essential to support recovery in disaster-affected populations.
This is a visual representation of the abstract.
Introduction
Earthquakes are among the most devastating natural disasters and pose substantial threats to children's physical, psychological, and social well-being. Children are particularly vulnerable due to their developmental stage, dependence on caregivers, and limited coping capacities (Tang et al., 2017). Exposure to earthquakes has consistently been associated with a wide range of adverse mental health outcomes, including post-traumatic stress disorder (PTSD), anxiety, and depressive symptoms. Previous studies conducted in earthquake-affected regions have reported PTSD prevalence rates ranging from 10% to 30%, depending on the severity of exposure, displacement, loss of family members, and availability of social support (Ni et al., 2022).
A growing body of literature has documented the psychological consequences of earthquake exposure in pediatric populations. Studies from Türkiye, Nepal, Indonesia, and other disaster-prone regions have demonstrated elevated rates of PTSD, anxiety, and depression among children and adolescents following major seismic events. Both longitudinal and cross-sectional studies indicate that these symptoms may persist for years after the initial trauma and are often associated with functional impairments in academic performance, peer relationships, and daily functioning (Marthoenis et al., 2019; Shrestha and Gopal, 2021). Factors such as female sex, older age, bereavement, and prolonged displacement have been consistently identified as key risk factors for adverse mental health outcomes in post-earthquake contexts (Alataş and Arslan, 2024; Dhoubhadel et al., 2020).
Beyond psychological trauma, earthquakes also disrupt food systems, household livelihoods, and access to adequate nutrition. Damage to infrastructure, population displacement, and interruptions in food supply chains can lead to both acute and chronic food insecurity, particularly among socioeconomically disadvantaged families (Hall et al., 2017). As a result, children in disaster-affected settings are at increased risk of undernutrition, dietary inadequacy, and micronutrient deficiencies. Importantly, malnutrition during childhood has been associated not only with impaired physical growth and cognitive development but also with emotional dysregulation, reduced stress tolerance, and increased vulnerability to mental health disorders (Herrera-Fontana et al., 2020).
Emerging evidence suggests that nutritional status and food insecurity are closely intertwined with children's mental health. Studies have shown that food insecurity is associated with higher rates of depression, anxiety, and stress-related disorders in both children and adolescents (Guldemir and Hizli-Guldemir, 2025; Herrera-Fontana et al., 2020; Köktürk et al., 2025; Liang et al., 2022). This relationship may be explained by both biological mechanisms, such as micronutrient deficiencies and inflammation, and psychosocial mechanisms, including caregiver stress, household instability, and reduced coping capacity. Despite this growing recognition, most post-disaster research has examined mental health outcomes and nutritional status separately, rather than as interconnected dimensions of child well-being (Tsuboyama-Kasaoka et al., 2021).
The 2023 earthquakes in Türkiye, among the most severe seismic disasters in the country's recent history, resulted in widespread destruction, large-scale displacement, and prolonged disruption of education, healthcare, and food systems. Children were exposed not only to traumatic events but also to significant socioeconomic instability and nutritional challenges. These conditions create a unique context in which psychological distress and nutritional vulnerability may coexist and interact.
Despite increasing evidence on the separate effects of disaster exposure and food insecurity on child health, comprehensive multicenter studies that simultaneously assess mental health outcomes, nutritional status, and household food security among earthquake-exposed children in Türkiye remain limited. Moreover, few studies have explored the potential pathways linking food insecurity and mental health outcomes in this population (Majumder et al., 2025; Marthoenis et al., 2019; Shrestha and Gopal, 2021; Silwal et al., 2022; Wahab et al., 2021).
The present study addresses this gap by examining the prevalence of PTSD, anxiety, and depressive symptoms among children and adolescents exposed to the 2023 earthquake in Türkiye, alongside assessments of nutritional status and household food insecurity. By integrating psychological, nutritional, and social dimensions within a single analytical framework, this study aims to provide a more holistic understanding of post-disaster child health and to inform integrated intervention strategies that address both mental health and nutritional needs in disaster-affected populations.
Materials and methods
Study design and setting
Twelve Türkiye provinces affected by the 2023 earthquake were questioned in a multicenter, cross-sectional research from March to August 2025. To measure socioeconomic, environmental, and seismic exposure variance, we picked urban and rural sites. Representative and accessible data were obtained from local schools, community health clinics, and child protection organizations. It assessed nutritional and psychological outcomes in disaster-traumatized children at numerous sites. The study was approved by the Malatya Turgut Ozal University Non-Interventional study Ethics Committee (Approval No: 155/E729416500) and adhered to the Declaration of Helsinki principles. All children consented verbally or in writing to caregiver approval. Professional psychologists assessed participant well-being and directed them to local psychological help during data collection. Research comprised 6–17-year-old earthquake-affected children and adolescents. Living in one of the 12 target provinces and having a caregiver and child assent were qualifying conditions. Schools and hospitals were stratified cluster sampled. We thoroughly examined eligible child homes in each cluster. 782 of 914 invited kids responded, 86.9%. Final sample included 375 boys (47.9%) and 407 girls (52.1%), mean 11.7 years (SD = 3.5). Multivariable analysis and prevalence estimates were powered by sample size.
Data collection procedures
All personnel got a 3-day standardized training on ethics, informed consent, structured interviews, and nutritional and psychological evaluation methods. Children and caregivers were interviewed face-to-face in secure, quiet communal areas. Each session lasted 45–60 min.
Measures
Sociodemographic data [child age, parental education, household income (household income was categorized based on nationally defined poverty thresholds), residence, and earthquake exposure variables] were obtained through caregiver-completed questionnaires administered face-to-face by trained research staff. Nutritional data, including dietary intake and food security measures, were collected through caregiver interviews using standardized questionnaires. Anthropometric measurements were obtained directly from children by trained staff using calibrated equipment. Psychological measures were administered in an interviewer-administered format. For children aged 8 years and older, responses were provided directly by the child. For children aged 6–7 years, items were read aloud and clarified when necessary, with caregiver input permitted only for comprehension support.
Nutritional analysis
WHO growth standards used calibrated height and weight equipment to determine BMI-for-age and height-for-age z-scores. Child weight was underweight, average, or obese. Stunting was specified as height-for-age < −2 SD. FAO-based Food Frequency Questionnaire (FFQ) evaluated cereal, legume, dairy, meat/fish, egg, fruit, vegetable, sugary snack, and sugar-sweetened beverage consumption administered to caregivers. A 24-h dietary recall was also obtained through a caregiver interview. Household food security was assessed using the Food Insecurity Experience Scale (FIES) and the Household Food Insecurity Access Scale (HFIAS), both administered to caregivers (Al-Ghadban, 2012; Ambikapathi et al., 2022)
Psychological assessment
All psychological assessments were administered by trained research staff who were members of the study team. For children aged 6–7 years, instruments were delivered in a structured interviewer-administered format. Items were read aloud and explained in developmentally appropriate language. Caregiver input was incorporated when clarification was necessary. This approach ensured comprehension and minimized response bias. Psychological assessments were conducted by trained psychologists using age-appropriate, validated instruments. Given the developmental limitations of younger children, psychological symptom analyses were restricted to participants aged 8–17 years, consistent with the validated age ranges of the instruments used.
The Child PTSD Symptom Scale (CPSS), validated for children and adolescents aged 8–18 years, was administered only to participants within this age range. Participants aged 6–7 years were not included in PTSD prevalence or regression analyses (Foa et al., 2001; Sapmaz et al., 2016). Using the Screen for Child Anxiety Related Emotional Disorders (SCARED), and depressive symptoms were measured using the Children's Depression Inventory (CDI), both applied in accordance with their validated age ranges (≥7–8 years depending on instrument). Younger children were not included in inferential mental health analyses (HALE III et al., 2005).
Statistical analysis
Descriptive statistics were used to summarize socio-demographic, nutritional, and psychological variables. Categorical data were presented as frequencies and percentages, and continuous variables as means with standard deviations (SD). Prevalence estimates were reported with 95% confidence intervals (CIs). Group differences were tested using chi-square tests for categorical variables and independent-samples t-tests for continuous variables. To identify predictors of PTSD, multivariable logistic regression models were constructed, adjusting for age, sex, bereavement, displacement, and nutritional factors (e.g., dietary diversity, stunting). Results were expressed as adjusted odds ratios (aORs) with 95% CIs. Statistical significance was defined as a two-tailed p-value <0.05. Analyses were conducted using SPSS Statistics, version 29.0 (IBM Corp., Armonk, NY, USA).
Results
The research included 782 children and adolescents, 47.9% boys (n = 375) and 52.1% girls (n = 407). The average age of participants was 11.7 ± 3.5 years, with boys averaging 11.5 ± 3.6 years and girls 11.9 ± 3.4 years. Family death was 12.5% (n = 98) and migration 23.0% (n = 180) during 3 months. Health indicators showed 9.6% (n = 75) of children had chronic difficulties, 3.7% (n = 29) were disabled, and 7.5% (n = 59) were medicated. Depression was 21.4% (n = 167) and anxiety 25.8% (n = 202). Overall, 55.1% of 431 participants reported appropriate social support. 17.2% (134) skipped 20 days, while 84.7% (662) went to school. Online learning was available to 328 (41.9%) (Table 1).
Sociodemographic, health, and psychosocial characteristics of the study population (n = 782).
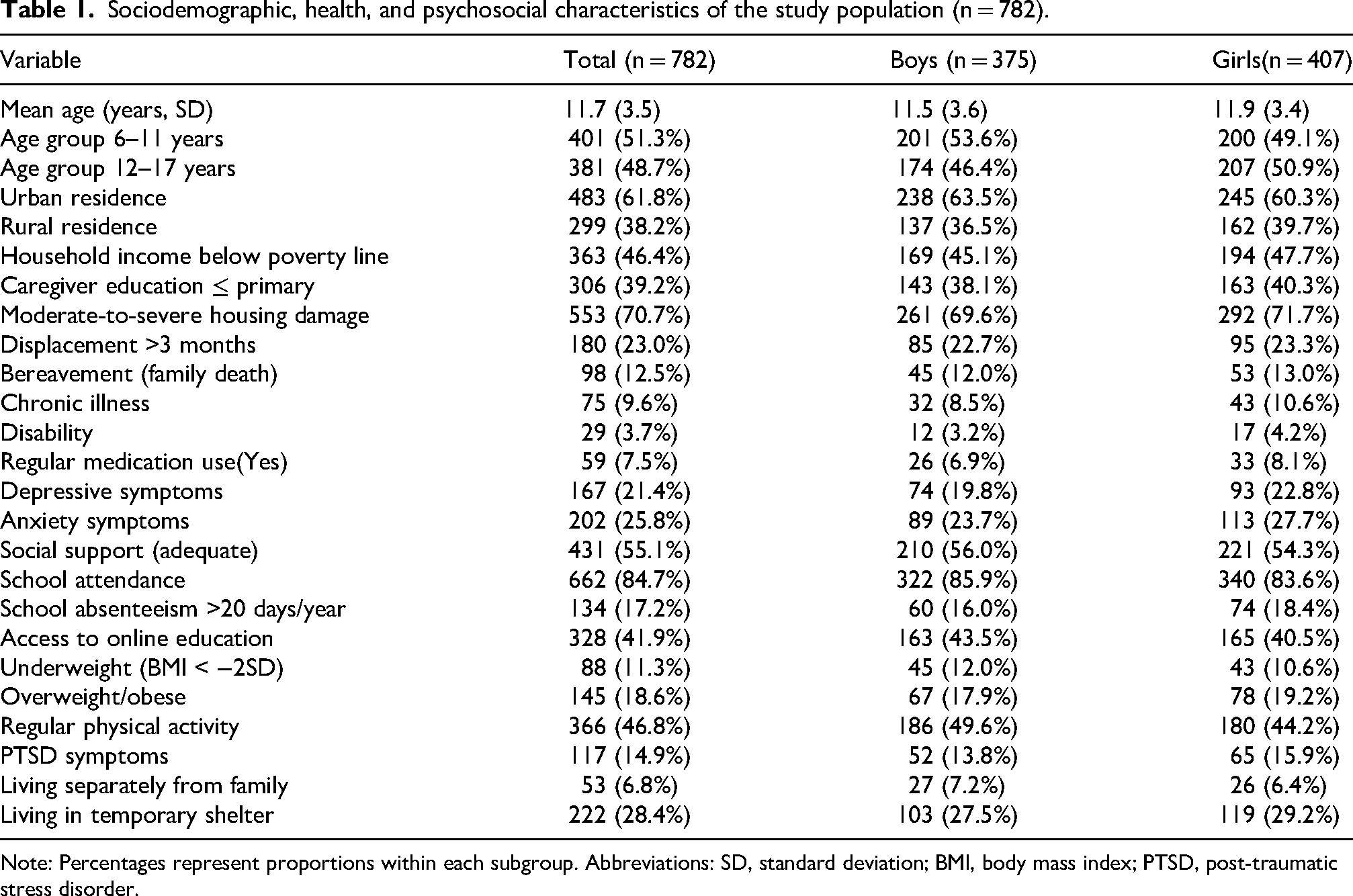
Note: Percentages represent proportions within each subgroup. Abbreviations: SD, standard deviation; BMI, body mass index; PTSD, post-traumatic stress disorder.
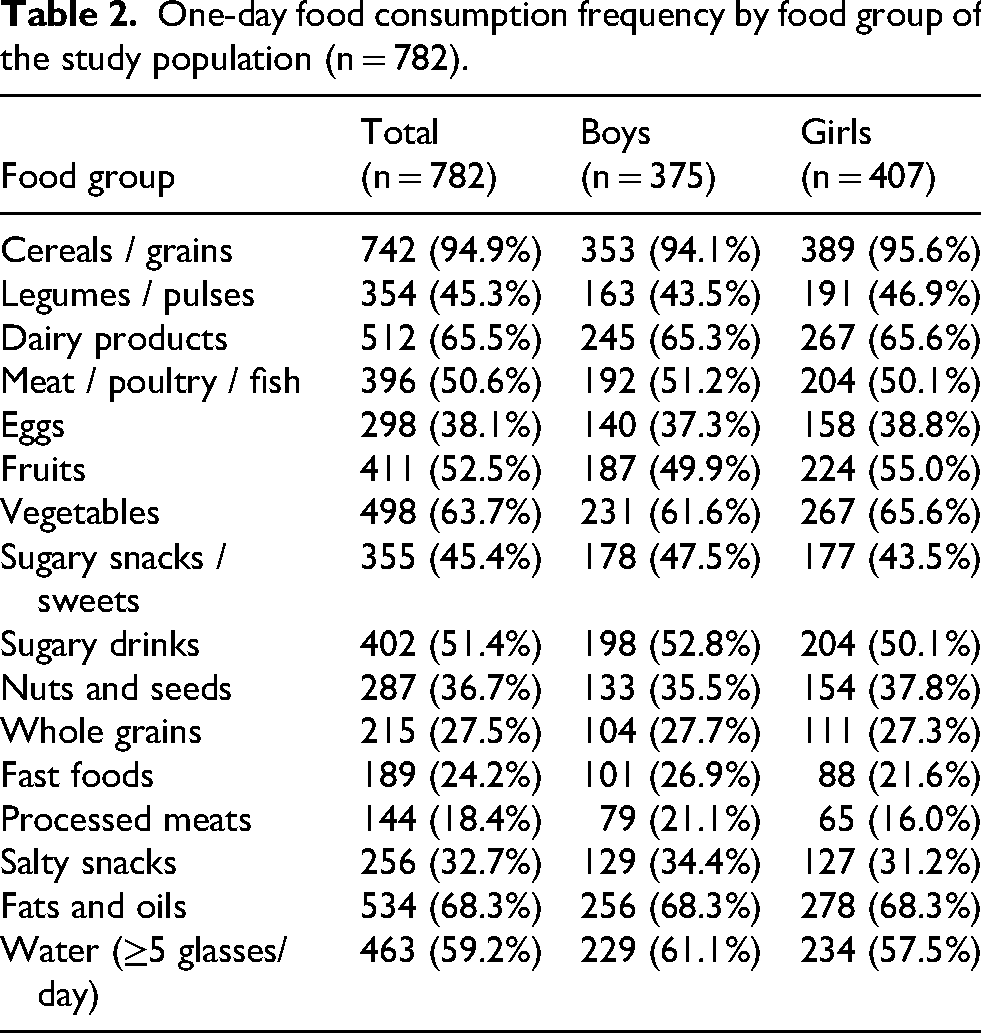
Most children and adolescents ate cereals and grains (94.9%), dairy (65.5%), and vegetables (63.7%) in one day. Half ate meat, poultry, or fish (50.6%), fruits (52.5%), and sugary drinks (51.4%), whereas 45.3% ate legumes. Eggs (38.1%), sweet snacks (45.4%), and nuts and seeds (36.7%) were eaten by one-third. Whole grains (27.5%), fast food (24.2%), and processed meats (18.4%) were less popular. Fats and oils were consumed by 68.3% and salty snacks by 32.7%. Interestingly, 59.2% drank five glasses of water daily (Table 2).
One-day food consumption frequency by food group of the study population (n = 782).
CPSS cut-off for possible PTSD was met by 21.7% of individuals, with girls (24.1%) outnumbering boys (19.2%) (χ2 = 2.16, p = 0.14). While not significantly different, girls reported greater rates of anxiety disorders (18.9% vs. 17.1% boys, χ2 = 1.32, p = 0.25) and depressive symptoms (15.6% vs. 13.1% boys, χ2 = 3.02, p = 0.02). Although not statistically significant, girls had 8.4% and 6.1% higher PTSD with anxiety and sadness (Table 3).
Mental health outcomes by sex of the study population (n = 782).
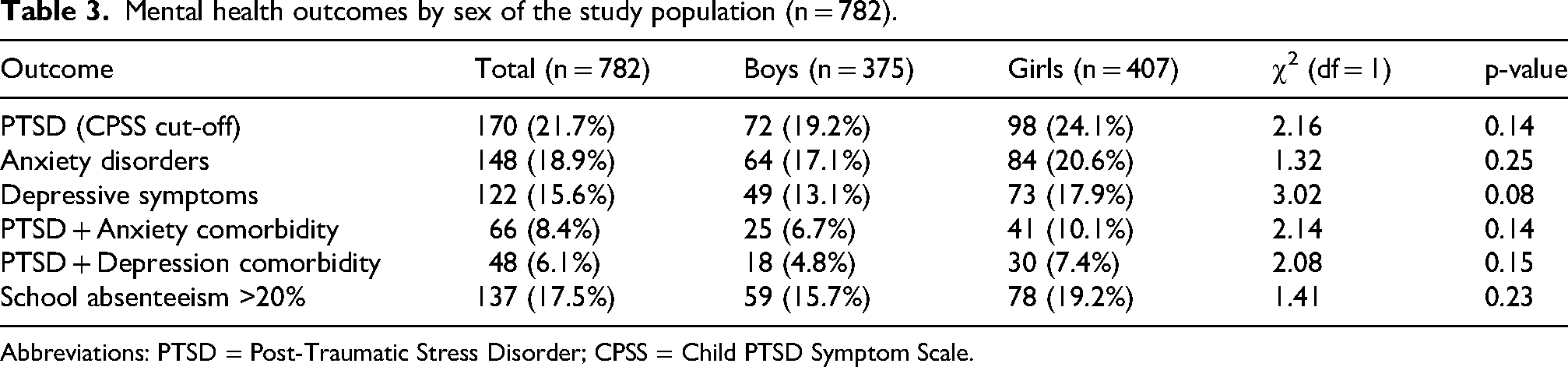
Abbreviations: PTSD = Post-Traumatic Stress Disorder; CPSS = Child PTSD Symptom Scale.
Several sociodemographic and dietary variables independently predicted PTSD in multivariable logistic regression. Girls had greater PTSD rates (aOR = 1.43, 95% CI: 1.02–2.01, p = 0.041). Age strongly predicts PTSD, rising by 8% yr (aOR = 1.08, 95% CI: 1.02–1.14, p < 0.001). Bereavement in the family quadrupled risk (aOR = 2.55, 95% CI: 1.65–3.94, p < 0.001). Three-month displacement was linked with PTSD (aOR = 1.76, 95% CI: 1.20–2.59, p = 0.004). Low dietary diversification and household food poverty were significant predictors (aOR = 1.92, 95% CI: 1.35–2.74, p < 0.001). Anemia did not predict PTSD (aOR = 1.39, 95% CI: 0.74–2.63, p = 0.300) (Table 4).
Multivariable logistic regression predictors of PTSD.
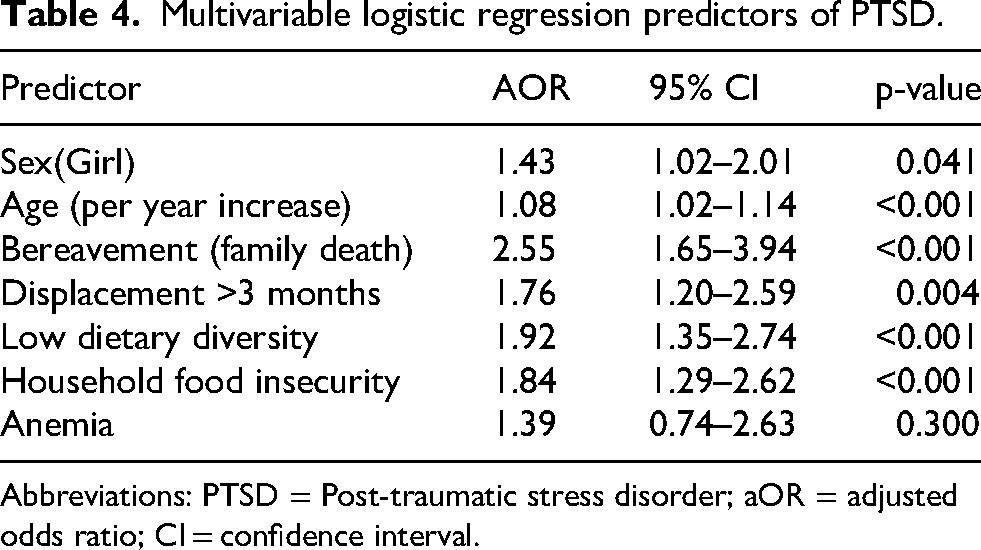
Abbreviations: PTSD = Post-traumatic stress disorder; aOR = adjusted odds ratio; CI = confidence interval.
Food insecurity substantially impacts PTSD (β = 0.61, 95% CI: 0.35–0.88, p < 0.001). PTSD was significantly impacted by food insecurity, but less so after including depressive symptoms (β = 0.38, 95% CI: 0.12–0.64, p = 0.004). Depressive symptoms had a substantial indirect influence (β = 0.23, 95% CI: 0.11–0.39, p < 0.001), accounting for 38% of the link. These data imply that depressive symptoms partly buffer the link between family food insufficiency and PTSD, emphasizing the need to treat comorbid depression in post-disaster mental health (Table 5).
Mediation analysis of the association between household food insecurity and PTSD, with depressive symptoms as a mediator.
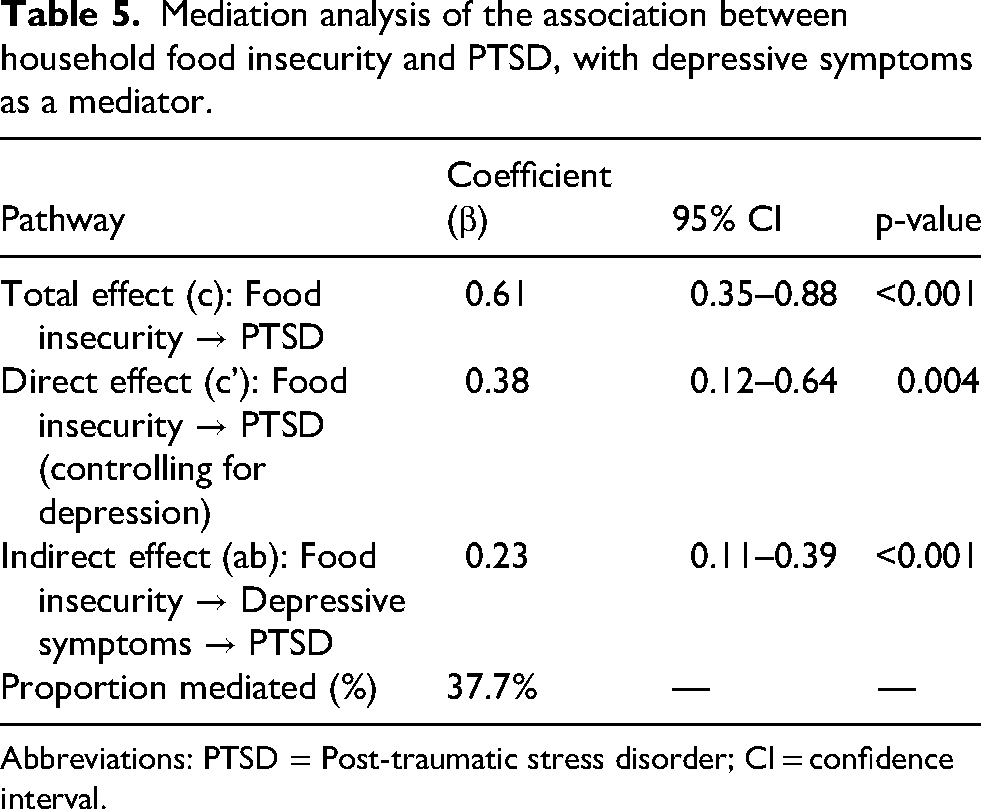
Abbreviations: PTSD = Post-traumatic stress disorder; CI = confidence interval.
Discussion
The 2023 Türkiye earthquakes, with magnitudes of 7.7 and 7.6, caused widespread destruction across multiple provinces, resulting in large-scale displacement, disruption of food systems, and limited access to healthcare and education. These conditions created a complex environment in which children were simultaneously exposed to trauma, socioeconomic instability, and nutritional vulnerability.
Our mediation analysis shows that family food insecurity directly affects PTSD risk in earthquake-traumatized children and adolescents and indirectly affects depressive symptoms. Depressive symptoms explain a large part of the link between material hardship and PTSD. This shows that food insecurity's psychological effects affect trauma susceptibility as well as economic and nutritional stress. Increasing evidence suggests that food insecurity is a social factor of mental health, influencing internalizing illnesses and trauma outcomes directly and via emotional pathways (Akram et al., 2024; Cain et al., 2022; Frongillo et al., 2024). A comprehensive study by Cain et al. (2022) found that food insecurity increases the risk of depression and anxiety in children and parents. A meta-review by Frongillo et al. (2024) found that food insecurity hinders psychological development, cognitive health, and emotional resilience in childhood and adolescence (Frongillo et al., 2024; Cain et al., 2022). The 2025 research points out that mental health issues might decrease food security and vice versa (Baek and Yoon, 2025). Our observed depression mediation matches conceptual theories that increase dietary hardship and psychological anguish.
Child nutrition and catastrophe evidence support our integrated framework. Nutritional disruption in disaster-affected areas increases physical and mental health risks (Adeoya et al., 2022; Agostoni et al., 2023). The scoping study by Adeoya et al. on child nutrition in catastrophe situations underlines how food instability, supply chain disruptions, and limited dietary variety might cause long-term developmental and psychological impairments (Adeoya et al., 2022). Our work bridges disaster nutrition research and trauma epidemiology by integrating mediation analysis in a catastrophe-exposed sample, a relation underexplored in the literature. General population and vulnerable group studies suggest mediation by internalizing symptoms. A recent cohort study in Lebanon revealed that depression and anxiety impacted food insecurity and low quality of life in children (Al-Ghadban, 2012). A meta-analysis of food insecurity and child mental health found substantial links with depression and stress across 19 research, while anxiety was more variable (Ling et al., 2022). Food insecurity was linked to stress and depression in low- and middle-income countries in a worldwide review and study (Alataş and Arslan, 2024; Aydın et al., 2024). Sleep issues mediated the association between food insecurity and mental health outcomes in a moderated mediation design, indicating complicated risk chains. Research on parenting stress shows that parent mental health influences food insecurity and parenting burden (Cain et al., 2022; Vos et al., 2022). These studies show that psychological distress mediates the link between financial hardship and negative psychosocial consequences.
Several convergent mechanisms may explain this mediation mechanistically. First, micronutrient shortages, inflammation, and stress-response dysregulation may be biological processes. Chronic deficiency of B-vitamins, iron, zinc, and omega-3 fatty acids may decrease neurotransmitter synthesis, brain insult resistance, and mood disorder sensitivity (Hilal et al., 2025; Khemraj et al., 2026). Mood instability may precede PTSD, making the person less competent to manage stress (Butler et al., 2024). Second, psychological stress amplification may occur because food insecurity commonly occurs with economic hardship, caregiver stress, and social instability. Depressive symptoms may worsen PTSD symptoms by reducing coping ability, social support, and ruminative thinking. Depressive symptoms amplify trauma in this cascade (Somo, 2024). Depressed people have negative cognitive biases including pessimism, catastrophizing, and low self-efficacy, which may affect trauma processing, extinction learning, and resilience following trauma.
Although higher prevalence rates of PTSD, anxiety, and depressive symptoms were observed among girls, these differences did not reach statistical significance for most outcomes, suggesting that sex-related differences may be influenced by contextual and environmental factors. Even when depression is included, food insecurity has a direct effect. This suggests that anxiety, sleep difficulties, emotion control deficiencies, decreased social functioning, and physiological hyperarousal may potentially contribute (Liao et al., 2025; Wu et al., 2021). Future models should examine parallel and serial mediation pathways, specifically sequences where food insecurity influences sleep difficulties, which lead to depression and PTSD.
We integrate dietary and psychological variables in a trauma-exposed kid population to enhance catastrophe mental health research. Post-disaster mental health studies generally overlook nutrition in favor of exposure variables (loss, displacement, injury). Instead, our research views trauma risk as a multisystem interaction between nutritional deficiency, mental discomfort, and trauma exposure.
Trauma-informed treatment in child health promotes an integrative examination of biological, psychological, and social dimensions. Emerging digital and public health perspectives show that integrative nutritional assistance and psychological treatment may have synergistic advantages (Silwal et al., 2022; Wang and You, 2022). Post-disaster or trauma-exposed child intervention studies often highlight trauma-focused CBT, EMDR, and narrative exposure therapy as frontline treatments for PTSD and internalizing symptoms (Burkhart et al., 2023; Mekuriaw et al., 2025). Nutrition is seldom included in such programs (Mekuriaw et al., 2025). Our data imply that adding nutrition assistance or dietary resilience training to psychological therapies may improve outcomes and minimize symptom persistence.
Strengths and limitations
This study has several notable strengths. It is based on a large, multicenter sample from earthquake-affected regions, which improves the generalizability of the findings. In addition, the combined assessment of anthropometric, dietary, and psychological variables provides a comprehensive view of child health in post-disaster settings. The use of mediation analysis further strengthens the study by allowing examination of potential pathways between food insecurity, depressive symptoms, and PTSD. Adjustment for key covariates also enhances the robustness of the results.
However, some limitations should be acknowledged. The cross-sectional design prevents conclusions about causality. Self- and caregiver-reported data may be affected by recall and social desirability bias. Younger children were not included in inferential psychological analyses, which may limit the generalizability of mental health findings. In addition, unmeasured factors such as family environment and social support may have influenced the results. Mediation analysis also assumes no unmeasured confounding, which may not fully reflect real-world conditions.
Future studies should use longitudinal designs to better understand causal relationships. Interventions combining nutritional and psychological support may help to clarify the observed pathways. Overall, the findings suggest that food insecurity contributes to PTSD both directly and indirectly through depressive symptoms, highlighting the need for integrated post-disaster interventions.
Conclusion
This study highlights the close relationship between food insecurity, nutritional vulnerability, and mental health problems among children exposed to the 2023 Türkiye earthquakes. A substantial proportion of children experienced symptoms of PTSD, anxiety, and depression, alongside notable levels of food insecurity and nutritional imbalance. Importantly, food insecurity was associated with PTSD both directly and indirectly through depressive symptoms, suggesting a complex and interconnected pathway. These findings emphasize that post-disaster child health should be addressed through integrated approaches that consider both psychological and nutritional needs. Interventions focusing solely on mental health may be insufficient if underlying socioeconomic and nutritional challenges are not addressed. Therefore, coordinated strategies combining mental health support, food security interventions, and social protection policies are essential to improve recovery outcomes in disaster-affected children.
Footnotes
Acknowledgements
The author appreciates the time and cooperation of all involved children and caregivers. Thank you to local schools and community health facilities for participant access.
Ethics approval
The study was conducted in accordance with the Declaration of Helsinki and approved by the Non-Interventional Research Ethics Committee of Malatya Turgut Özal University (Approval No: 155/E729416500).
Consent to participate
Written informed consent was obtained from caregivers, and assent was obtained from all participating children prior to enrollment.
Author contributions
N.A. conceived and designed the study, coordinated data collection, performed the statistical analyses, interpreted the results, and drafted the manuscript. The author critically revised the manuscript and approved the final version.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Access to data and materials
Due to ethical and confidentiality concerns regarding children, the present study's datasets are not publicly accessible but are available from the corresponding author on reasonable request.