
Abstract
To date, findings have denoted that disrupted meal timing and eating during biologically inappropriate hours are associated with an increased risk of adverse cardiometabolic outcomes among shift workers. However, solid evidence remains lacking due to the small number of clinical studies and low methodological quality. This review investigated how an intervention targeting shift workers’ meal timing affects cardiometabolic markers. The MEDLINE, Cochrane Library, Web of Science, Embase, CINAHL Complete, and Scopus were searched using a predefined search strategy. Only randomized controlled trials of adults aged ≥18 under a shift work environment were included. Four trials met the inclusion criteria. Three studies assigned fasting periods during the night shift, ranging between 19:45 and 06:30 h, and one study used 10-h self-selected Time-Restricted Eating (TRE). A 10 h self-selected TRE reported a significantly lower VLDL-C particle size compared with the control group. Four studies reporting fasting insulin levels and homeostatic model assessment of insulin resistance observed a significant change in one trial after an 8.5-h overnight fast. No studies pointed to significant changes in HDL-C. In the postprandial measurement, 10.75 h of night fasting showed significantly lower glucose AUC, non-esterified fatty acids AUC, and 2-h glucose than in the meal- and snack-at-night group. Body weight was slightly lower after a short overnight fast. The scarcity of trials investigating mealtime interventions and cardiometabolic markers among shift workers limits the generalizability of the findings and raises concerns regarding the robustness of the preliminary positive outcomes. Therefore, more trials with larger sample sizes and longer study durations are required, given the limited number of studies.
Keywords
Introduction
The modern work schedule is rapidly evolving into a 24-h society, and people are often engaged in some shift work (Rajaratnam and Arendt, 2001). Shift work is defined as any regularly taken employment outside the “standard working window” from 06:00 to 18:00 h. Shift work involves fixed shifts, such as night work or rotating shifts (Monk and Folkard, 1992). As a workforce, shift workers encompass about 25% of the US population (Lieberman et al., 2020), 20% of the European working population (Paoli and Merllié, 2001), and 1.4 million or 15% of employees in Australia (Australian Bureau of Statistics, 2010). It is known that such work schedules disrupt the biological circadian rhythm and natural sleep–wake cycle, leading to adverse health consequences (Reinganum and Thomas, 2024). For instance, a systematic review and meta-analysis from 12 high-quality studies showed a higher risk of metabolic syndrome (MetS) among medical night shift workers, with a more than twofold increase in the risk of developing MetS compared with day workers (2.17, 95% CI = 1.31–3.60, P = 0.003; I2 = 82%, P < 0.001) (Sooriyaarachchi et al., 2022). Furthermore, recent bibliometric evidence comprising 110 publications identified several important burdens affecting healthcare workers and tactical populations. These include stress and behavioral factors, occupational and mental health challenges, pandemic-related educational disruptions affecting resident training, and psychological sequelae such as depression and anxiety, all of which may contribute to stress accumulation and clinical deterioration (Henchiri et al., 2025). This phenomenon illustrates the multidimensional nature of shiftwork research and acknowledges healthy lifestyle improvement as a key intervention strategy.
Cardiometabolic disorders, including obesity and type 2 diabetes, develop long before the onset of cardiovascular disease (CVD) and may mediate the connection between shift work and CVD (Proper et al., 2016). Several reviews reported that individuals involved in shift work are more likely to be overweight or obese (Sun et al., 2018; Zhang et al., 2020) and have impaired glucose tolerance (Proper et al., 2016). Previous findings further denoted a positive association between shift work and cardiometabolic risk factors, including elevated blood pressure (Yeom et al., 2017), triglyceride (Bayon et al., 2022), uric acid (Dong et al., 2024), and inflammatory markers (Woo et al., 2022). However, in accordance with a review by Proper et al. (2016), solid evidence remains lacking due to the small number of studies and the low methodological quality of previous research, including observational studies.
Further analysis showed that circadian interference correlates with shift work and is considered moderately responsible for the disparity in chronic disease (Antunes et al., 2010). Typically, circadian rhythms occur at central (in the hypothalamus, including the suprachiasmatic nucleus) and peripheral levels, with the environment of clocks within several peripheral tissues exhibiting autonomous daily rhythmicity (Franzago et al., 2023). This system regulates many biochemical and behavioral processes via the day/night cycle (Bass and Takahashi, 2010). Artificial light exposure, such as from electronic devices, interferes with the central clock (Ashbrook et al., 2020). A recent randomized control trial (RCT) indicated that evening blue light exposure divided by three different timings ((i) 7:30–9:00 p.m., (ii) 9:00–10:30 p.m., (iii) 10:30 p.m.–12:00 a.m.) affects sleep quality, motor performance, and cognitive function in participants with intermediate chronotypes. In the same way, night eating, irregular eating patterns, or feeding over resting periods compromise the metabolic homeostasis and lead to higher body mass index (BMI) and disease development (Pickel and Sung, 2020). In shift work environments, irregular and/or poor dietary patterns may contribute to the increased risk of CVD, as shift workers often alter their eating behavior and timing to accommodate shift schedules (Clark et al., 2023). Furthermore, obesity and MetS have been associated with consuming a greater proportion of daily energy intake in the evening and with night eating, both of which are known to affect circadian rhythm and induce changes in human metabolism (Yoshida et al., 2018). Subsequently, evidence has shown that the dietary patterns of night shift workers differ from those of regular day workers, which could also contribute to the rise in metabolic risk abnormalities (Wang et al., 2014).
Meal timing (eating–fasting pattern) is a modifiable lifestyle factor that has the potential to lessen the circadian disruption and promote health in shift workers (Manoogian et al., 2022). Currently, intermittent fasting (IF) is a widely investigated nutritional strategy that involves alternating periods of extreme calorie restriction with periods of normal eating. IF is commonly defined as energy restriction, which encompasses eating and drinking only at regular intervals while consuming very few or no calories (Correia et al., 2020). IF is categorized into four groups: (1) zero-calorie alternate-day fasting, (2) modified alternate-day fasting, (3) the 5:2 diet, and (4) time-restricted eating (TRE) (Patikorn et al., 2021). The proponents of the IF claim that it induces weight loss more rapidly than traditional diets and reduces inflammation and other heart disease risks (Harvard Health Publishing, 2019). A few clinical trials have also observed the cardiometabolic advantage of IF in adults with elevated weight, pre-diabetes, and MetS, including moderate weight loss, improved beta cell function, decreased blood pressure, insulin resistance, oxidative stress, and appetite (Horne et al., 2023; Jamshed et al., 2022). Although associations between night shifts and metabolic dysregulation are well-documented, the implementation of IF strategies among shift workers may require modification compared with daytime workers. In particular, night-shift workers often sleep during the day and remain awake during biologically inappropriate hours, making conventional fasting and feeding schedules difficult to maintain. Consequently, meal-timing interventions for shift workers may need to be tailored to accommodate occupational demands, sleep schedules, and circadian disruption while preserving the intended metabolic benefits of fasting. Existing studies primarily rely on single-point assessments, failing to capture how longitudinal changes in shift schedules influence the evolution of meal timing habits (Oostenbach et al., 2022). Moreover, previous observational studies emphasized that IF practice among shift workers varies with factors such as the timing of calorie intake, dietary patterns, and characteristics of the shift work. Therefore, to the best of our knowledge, no consensus has been reached on the optimal timing of meals to reduce cardiometabolic risk factors among shift workers.
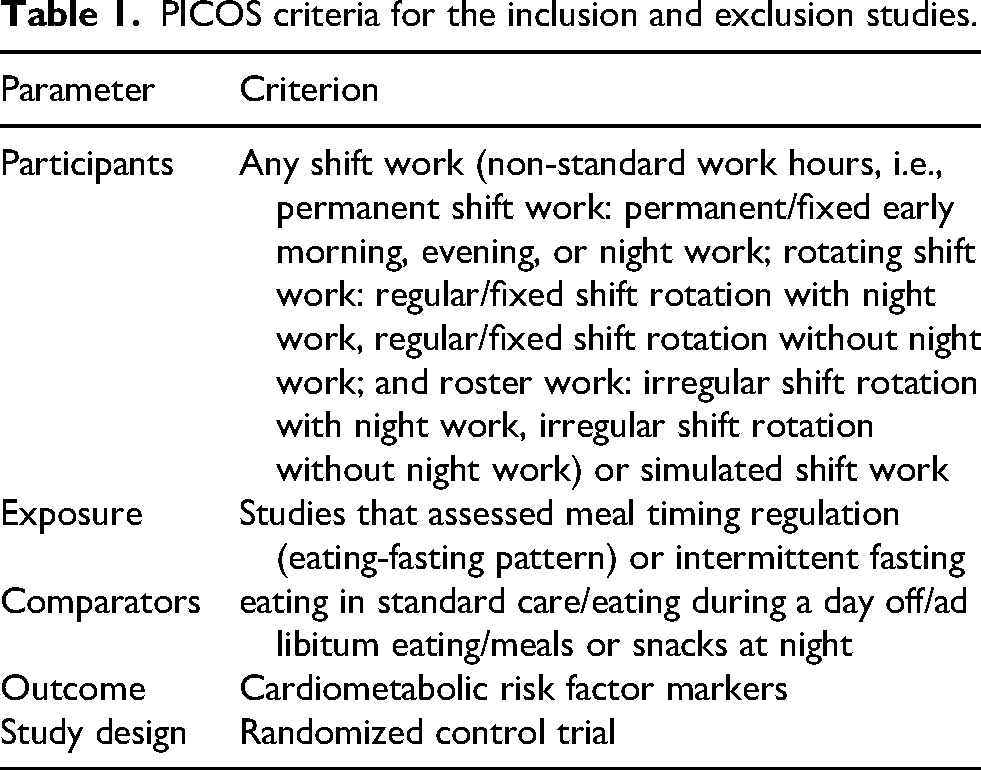
Taken together, the current study aimed to: (1) systematically review the available evidence generated by RCTs of meal timing (eating–fasting pattern), including IF intervention on cardiometabolic risk factors among shift workers according to the guide to PICOS criteria (Table 1), (2) identify the key components of effective intervention, and (3) identify methodological limitations that could be addressed in future research for improving data quality in this area.
PICOS criteria for the inclusion and exclusion studies.
Methods
This review has been reported in adherence to Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) 2020 guidelines (Page et al., 2021) and the protocol was registered in PROSPERO (International Prospective Register of Systematic Reviews; www.crd.york.ac.uk/prospero/index.asp, identifier CRD42024588992). A completed PRISMA 2020 checklist is provided in Supplemental Table 1.
Data sources and search strategy
The systematic literature review was performed in the electronic databases MEDLINE (PubMed), Cochrane Library (Wiley), Web of Science (Clarivate), Embase (Elsevier), and CINAHL Complete (EBSCO) up to September 2024, with no language or time restrictions. An additional citation search was conducted on January 7, 2025. Data from other sources, that is, dissertations, conference abstracts, review articles, book chapters, comments, and unpublished data, were excluded. The complete search strategy for all databases, including keywords and MeSH terms, is provided in Supplemental File 1. All the search results were exported into RIS or EndNote format for screening. Two authors (FW and IEK) independently conducted the study selection.
Selection of studies
Studies were included in the systematic review if they met the following criteria:
RCTs (with parallel or crossover design) examining the effect of meal timing (eating-fasting) regulation or IF (with/without specific meal hours) among shift workers (with current or previous condition of employment) or simulated night shift work. Comparing ad libitum eating/standard care/standard eating/eating during the day off/meal or snack at night. The intervention group is either a meal that the researcher gives during a specific time or a diet guideline with a specific meal time (day or night). Reported an outcome related to cardio-metabolic markers (e.g., fasting measures, postprandial measures, and blood pressure) and anthropometric parameters (e.g., body weight, BMI, and body composition), with or without cardiometabolic abnormalities. RCTs reported any gender, ethnicity, or other demographic status. Participants aged ≥18 years.
The following studies were excluded:
RCTs included subjects with significant organ dysfunction (e.g., hepatic, renal, and CVDs) or on medication for diabetes, hyperlipidemia, or drugs known to alter metabolism. RCTs with pregnant or breastfeeding women. Co-intervention (e.g., drugs, supplements, diet, or physical activity) was not applied in all intervention arms.
All the search results were imported into EndNote 21. Two independent authors (FW, IEK) independently evaluated the early records screening according to the criteria. At the initial screening stage, the title and abstract were consistent with the inclusion criteria and listed as the search results benchmark. Later, the same two authors reviewed the full texts independently and discussed discrepancies. Any disagreements between the two authors were resolved through discussion with the third author (AJN) until consensus was reached.
Data extraction
For the included studies, two reviewers (FW and IEK) independently extracted data using a pilot-tested standardized data extraction form developed in Microsoft Excel. Extracted information included the first author, year of publication, country of origin, study design (parallel or crossover RCT, including washout duration), sample size, age, study duration, occupation, research setting, provision of food, inclusion criteria, and outcomes. In addition, characteristics of the intervention in the included studies were reported, including: type of intervention and control group, meal-time regulation and meal conditions, physical activity, sleep conditions, and methods to ensure dietary compliance. Any disagreements were resolved via consensus with the third author (AJN).
Outcomes
Primary outcomes data were collected for cardiometabolic markers, including: fasting measures (glucose, insulin, triglyceride (TAG), total cholesterol, HDL-C, LDL-C, HDL-C: LDL-C, VLDL-C particle size, Homeostatic Model Assessment of Insulin Resistance (HOMA-IR), Non-Esterified Fatty Acids (NEFA)), postprandial measures (glucose AUC, 2-h glucose, NEFA AUC, and TAG AUC), systolic/diastolic blood pressure, and percent of HbA1c. Meanwhile, secondary outcome data were collected on weight, BMI, body fat percentage, daily caloric intake, and daily activity energy expenditure.
Risk of bias assessment
Two authors independently assessed the Risk of bias (FW, IEK) using RoB 2.0 according to the methods described in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins et al., 2011). The following domains will be considered: selection bias (random-sequence generation and allocation concealment), performance bias (blinding of participants and personnel), detection bias (blinding of outcome and assessment), attrition bias (incomplete outcome data), reporting bias (selective reporting), and other bias (carryover effect in crossover RCTs and potential conflict of interest). A judgment about the risk of bias can be “Low,” “High” risk bias, or “Some concerns” (JPT et al., 2024). Any disagreements were resolved via consensus, or a third reviewer if consensus could not be reached.
Results
Search results
The PRISMA diagram of the selection process is provided in Figure 1. A total of 2396 articles were initially obtained from database searches in September 2024, and after removing 200 duplicates, title and abstract screening excluded 2177 studies. Of the remaining 19 full-text articles, 16 were not retrieved (nine studies did not use meal time or IF as the primary intervention, and seven reported different outcomes). Subsequently, one article authored by Centofanti et al. (2025) obtained from citation searching in January 2025 was included. Therefore, four clinical trials were recognized to be qualified for inclusion in this review.
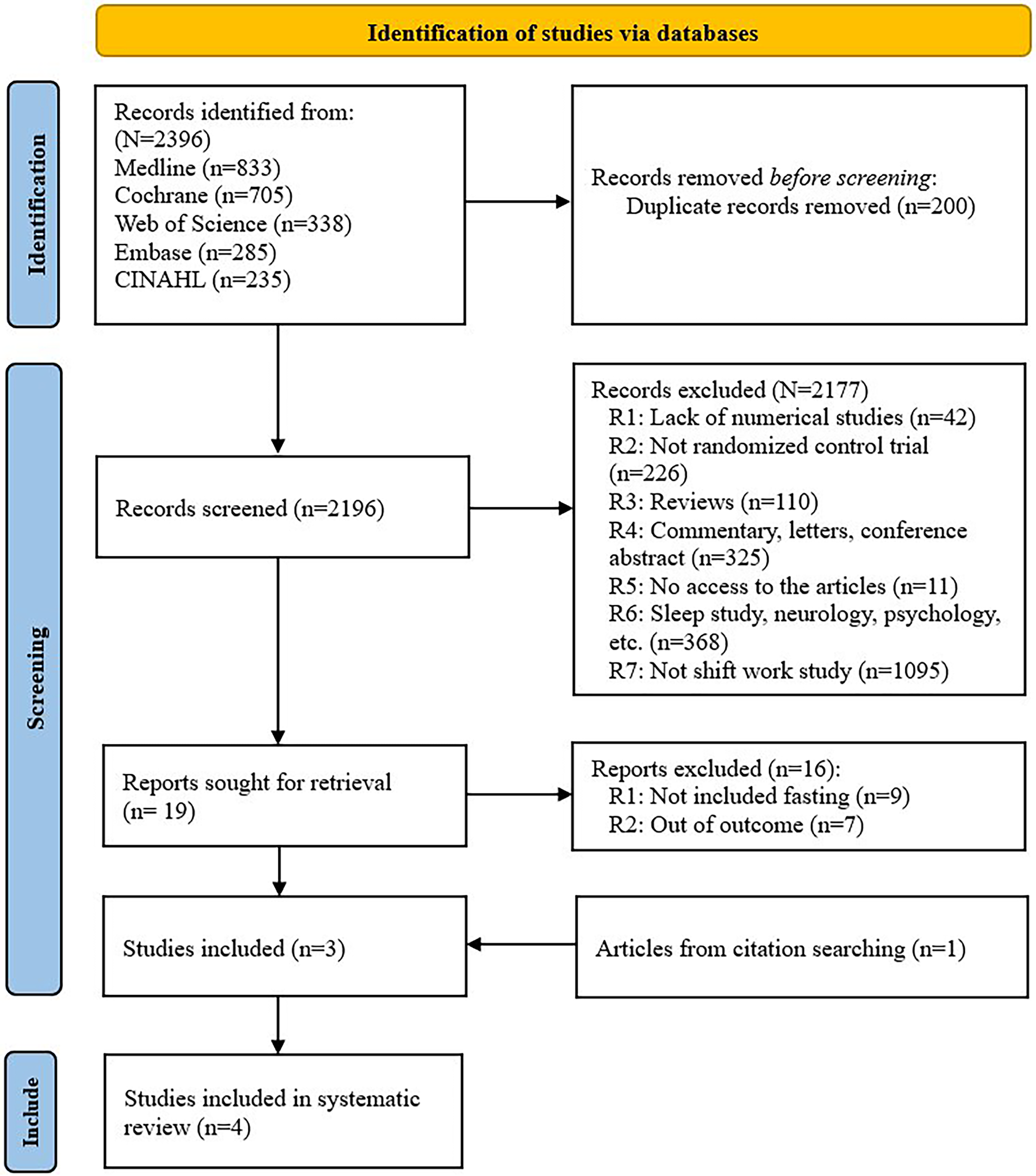
Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) 2020 flow diagram of the studies included.
Characteristic of included studies
Table 2 sums up the main characteristics of the four included trials. The selected studies were published between 2021 and 2025 and were conducted in three countries: Australia (Centofanti et al., 2025; Leung et al., 2021), the United States (Manoogian et al., 2022), and Brazil (Teixeira et al., 2023). Two studies performed an RCT using a crossover study design with at least six days (Teixeira et al., 2023) and two weeks (Leung et al., 2021) washout periods, comparing two and three conditions, respectively. Meanwhile, the two remaining studies carried out an RCT using a parallel design, comparing three groups (Centofanti et al., 2025). The trial size ranged from 10 to 137 participants. A total of 221 participants were included, with an age range of 18–50 years. The total study duration ranged from 7 days to 12 weeks. Two studies provided isocaloric meals (Centofanti et al., 2025; Teixeira et al., 2023), one study gave nutritional counseling and instructed the participants to follow the Mediterranean diet (Manoogian et al., 2022), and one study asked participants to change their mealtime only, and not the types of food and beverages consumed (Leung et al., 2021). Firefighters, police officers, night-shift workers (not specified), and non-shift workers were selected and divided into free-living conditions (three studies) and a laboratory setting (one study). All trials included healthy subjects, with one study dealing with participants who had abdominal obesity (Leung et al., 2021) and one with/without cardiometabolic risk at baseline. Cardiometabolic markers were measured in all trials, with two studies reporting body weight, one BMI, two sleeping quality, and one dietary pattern.
Study characteristics of the included RCTs.
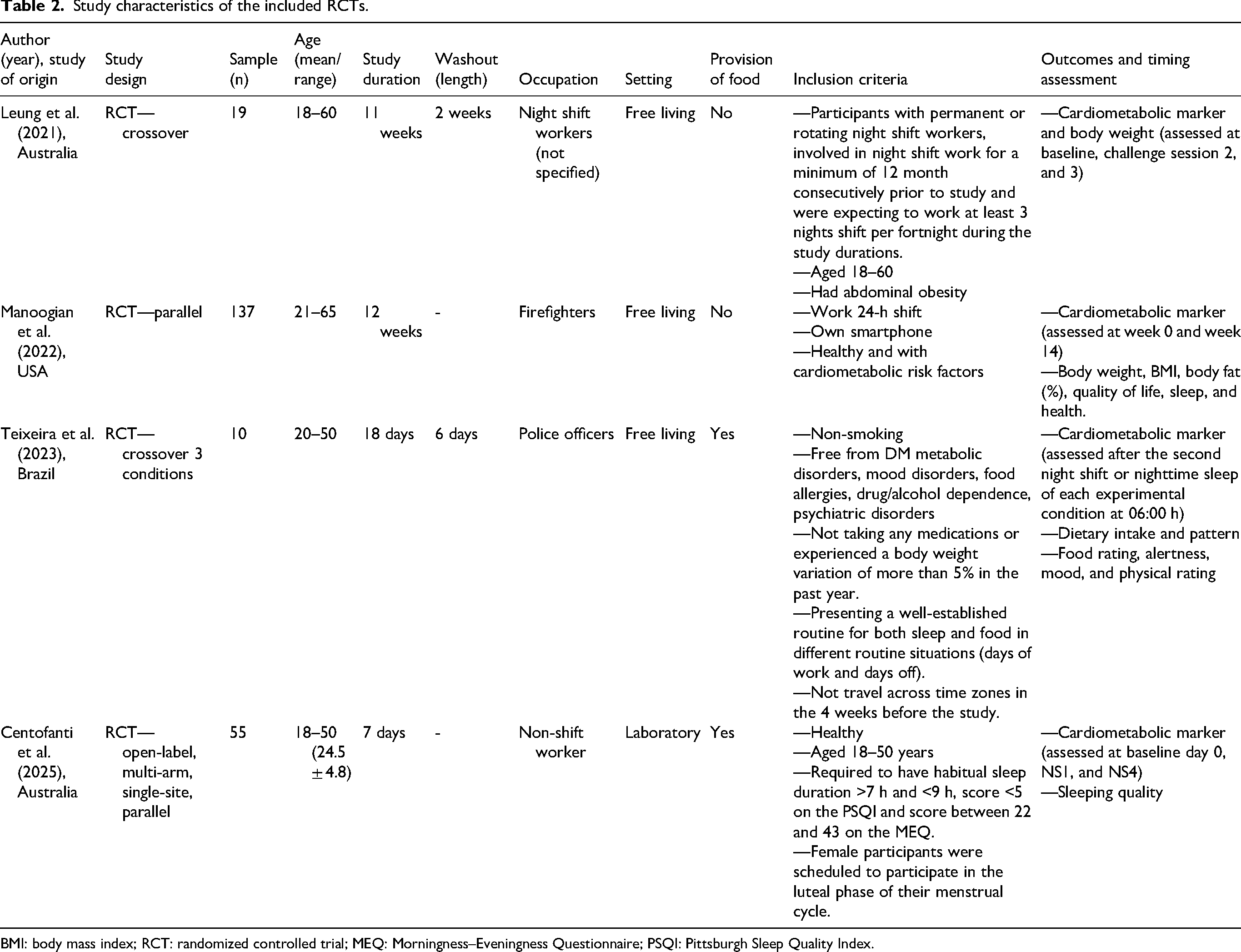
BMI: body mass index; RCT: randomized controlled trial; MEQ: Morningness–Eveningness Questionnaire; PSQI: Pittsburgh Sleep Quality Index.
Intervention characteristic
An overview of the main characteristics of mealtime or IF interventions during shiftwork is detailed in Table 3. The duration of the intervention group ranged from two days to eight weeks. Three studies specifically assigned fasting periods during the night shift, ranging from 19:45 to 06:30 h (5–10.75 h) (Centofanti et al., 2025; Leung et al., 2021; Teixeira et al., 2023), while one study did not specify the time (self-selected 10 h TRE) (Manoogian et al., 2022). Participants in two studies received isocaloric meals during the intervention period, comprising diets of 40–55% carbohydrate, 15–17% protein, 30–33% fat (Centofanti et al., 2025; Teixeira et al., 2023), and one study included 23 g of fiber (Centofanti et al., 2025). The Estimated Energy Requirement (EER) distribution was reported in two studies (participants in one study received 100% EER before 22:00 h (Teixeira et al., 2023), and the other received 30% EER at 06:30 h for breakfast, 10% and 20% EER at 09:30 and 17:00 h, respectively, for snack, and 40% EER at 19:00 h for dinner (Centofanti et al., 2025)). As for participants with no food prescription, one study received strategies on how to redistribute the mealtimes and avoid changes in their usual dietary habit (Leung et al., 2021) and one obtained nutrition counseling to follow a Mediterranean diet (Manoogian et al., 2022) with general consumption goals of 60% carbohydrate (whole grain, fruits, vegetables, beans, and legumes), 15% protein (fish and seafood at least twice a week, yogurt, cheese, poultry, and eggs), and 25% fat (olive oil, canola oils, tree nuts, peanuts, avocado, and seeds). Two studies (Manoogian et al., 2022; Teixeira et al., 2023) allowed their participants to consume caffeine (one study allowed ad libitum outside the eating window for sugar-free caffeine, and one allowed them to drink coffee once a day at breakfast), and one study did not permit (water and caffeine-free tea were allowed ad libitum) (Centofanti et al., 2025). Participants in three trials were instructed to maintain their usual daily activities and sleeping habits (Leung et al., 2021; Manoogian et al., 2022; Teixeira et al., 2023), while one study was conducted in a laboratory area (Centofanti et al., 2025).
Characteristics of the interventions of the included studies.
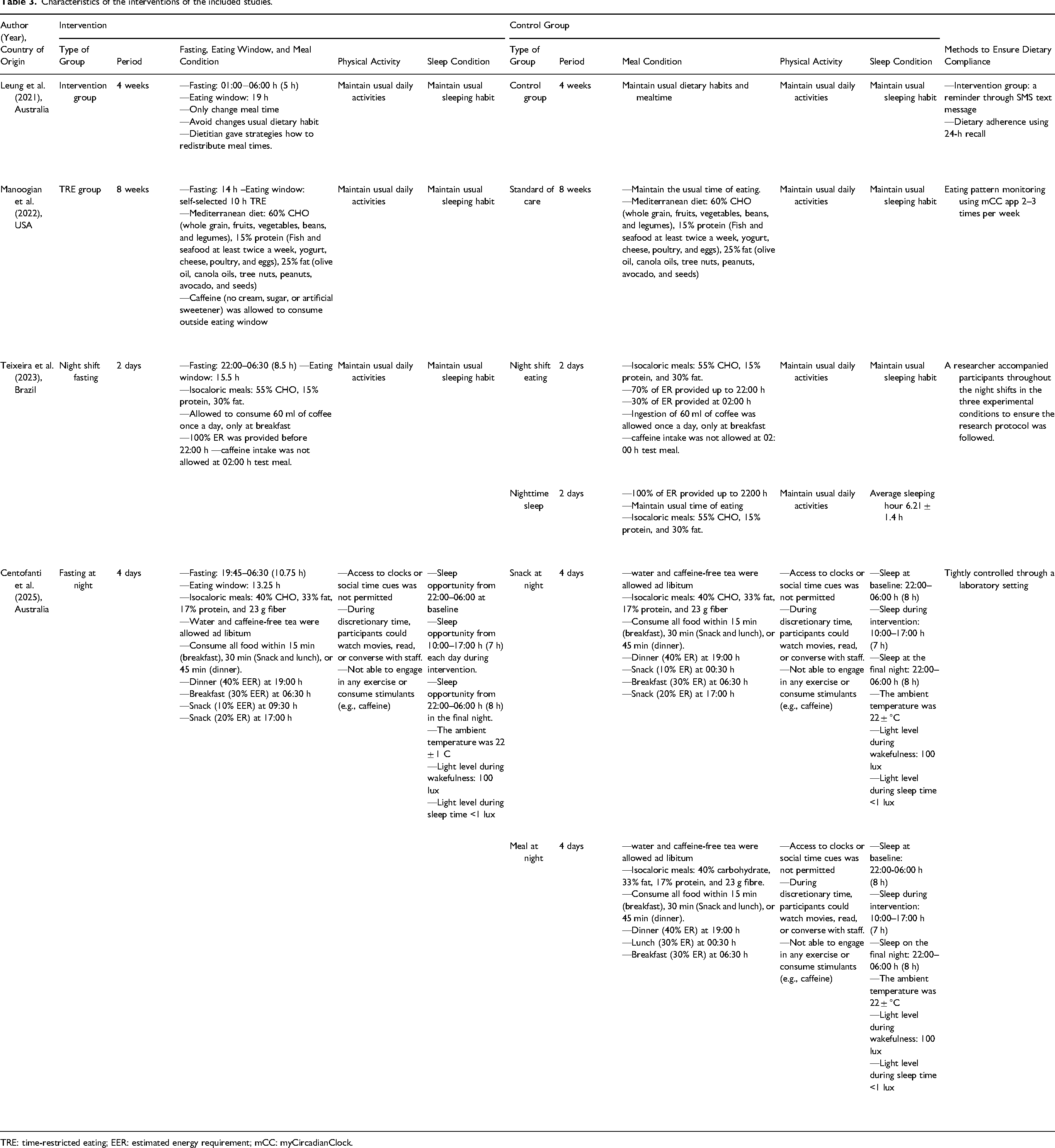
TRE: time-restricted eating; EER: estimated energy requirement; mCC: myCircadianClock.
In the control group, two studies assigned participants to maintain their usual dietary habits and/or mealtime with the same nutrition counseling as the intervention group (Leung et al., 2021; Manoogian et al., 2022). Meanwhile, two studies compared the intervention group with night-shift eating (Teixeira et al., 2023) and one with night-time snacks, using the same isocaloric meals (Centofanti et al., 2025). The night shift eating mealtime varied, ranging from 00:30 h to 02:00 h, with 30% ER. One study with a snack-at-night group asked participants to eat a snack with 10% EER at 00:30 h (Centofanti et al., 2025), and another study allowed participants to sleep at night, with an average sleep duration of 6.21 ± 1.4 h (Teixeira et al., 2023). Three studies maintained their control groups’ daily activities and sleeping behavior (Leung et al., 2021; Manoogian et al., 2022; Teixeira et al., 2023). Methods to ensure dietary compliance among participants were diverse. A study reminded the intervention group via SMS text message not to consume any meals or drinks during the designated time and asked them to record their eating patterns using a 24-h food recall (Leung et al., 2021). The other group was monitored using the myCircadianClock (mCC) app 2–3 times per week (Manoogian et al., 2022). A researcher in one study controlled participants who received prescribed meals to ensure the research protocol was followed (Teixeira et al., 2023).
Results of the RCTs
Table 4 summarizes the overall outcome reported by the four included trials, illustrating several significant differences between intervention and control groups. The four studies reported results for 10 fasting markers, five postprandial measures, five anthropometric parameters, and three other outcome measures.
Overview of Intervention-Group Outcomes Compared to Control-Group Outcomes
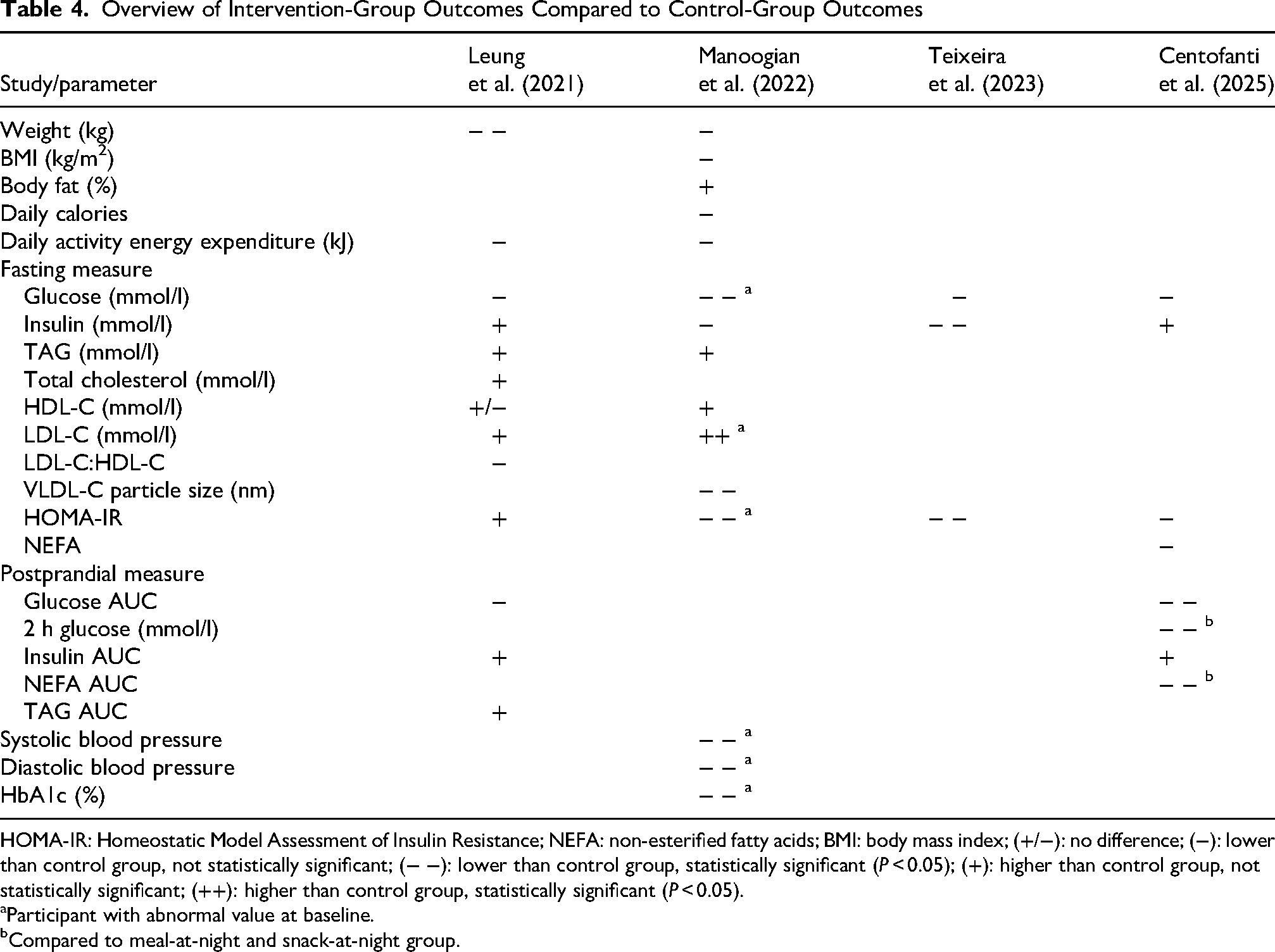
HOMA-IR: Homeostatic Model Assessment of Insulin Resistance; NEFA: non-esterified fatty acids; BMI: body mass index; (+/−): no difference; (−): lower than control group, not statistically significant; (− −): lower than control group, statistically significant (P < 0.05); (+): higher than control group, not statistically significant; (++): higher than control group, statistically significant (P < 0.05).
Participant with abnormal value at baseline.
Compared to meal-at-night and snack-at-night group.
In the fasting measures, of the four studies measuring fasting glucose, meal timing, and fasting duration did not significantly alter fasting glucose levels compared to the control group across all participants. However, Manoogian et al. reported lower fasting glucose in the intervention group only among participants with abnormal baseline values. Four studies observing fasting insulin reported a significant change in one trial. Morning insulin was significantly lower after 8.5 h of night-shift fasting (P < 0.001), compared with the night-shift eating and nighttime sleep group, which combined isocaloric meals (15.5 h eating window). In the lipid outcome, TAG, HDL-C, and LDL-C changes were measured in three studies, yet none showed statistically significant differences compared with the control group. Only one study by Leung et al. reported homogeneous HDL-C results in both the intervention and control groups. The total cholesterol and LDL-C:HDL-C were observed among night shift workers by Leung et al.; however, no notable changes were reported after the intervention. VLDL-C particle size was measured in one study by Manoogian et al. (2022), and was significantly lower in the intervention group than in the control group. A similar result found no substantial alteration of the NEFA marker in the Centofanti et al. study after designated night fasting compared to the snack- and meal-at-night group. According to Teixeira et al.'s study, HOMA-IR was significantly lower in the 8.5 h night shift fasting group than in the night shift eating and nighttime sleep groups. In addition, a 10-h self-selected TRE by Manoogian et al. study indicated a lower value among participants with abnormal HOMA-IR at baseline. Meanwhile, two other studies declared no significance (Centofanti et al., 2025; Leung et al., 2021).
In the postprandial measurement, one out of two studies showed significantly lower glucose AUC, while insulin AUC showed no significant changes. Meanwhile, 2-h glucose and NEFA AUC were reported by Centofanti et al., indicating a notable alleviation in the simulated fasting-at-night group compared with the meal- and snack-at-night groups. Furthermore, short 5-h overnight fasting did not significantly affect TAG AUC in one study. Lastly, systolic and diastolic blood pressure and percent HbA1c were measured in one study and showed a significant increase at the end of the intervention among participants with baseline abnormalities.
As secondary outcomes, anthropometric parameters were measured in two studies, and weight change was observed in both, but only one reported a significant change after intervention. In the study by Leung et al. (2021) where 19 participants had a small 5-h overnight fast for four weeks, the mean (± SD) body weight at the end of the trial was slightly lower compared to the end of the control (MD: −0.9 kg; 95% CI: −1.3 to −0.4; P < 0.001). Meanwhile, in the study by Manoogian et al., a self-selected 10-h eating window (14-h fasting) for 8 weeks did not significantly change body weight compared with the control group. Unfortunately, BMI, body fat, and daily calories observed by Manoogian et al. reported no significant decrease between the intervention and control groups. Moreover, two studies that observed daily activity energy expenditure showed no significant difference after the intervention.
Risk of bias and quality assessment
The risk of bias assessment is shown in Figure 2. All studies were judged to have a low risk of selection bias, performance bias, and attrition bias since the method of blinding was not appropriate in this trial. One study was judged with some concern, and one is at high risk of bias due to missing outcome data. Moreover, half of the studies were judged to have some concern due to the selection of the reported results. Overall, four RCTs were rated high RoB in ≥1 domain.
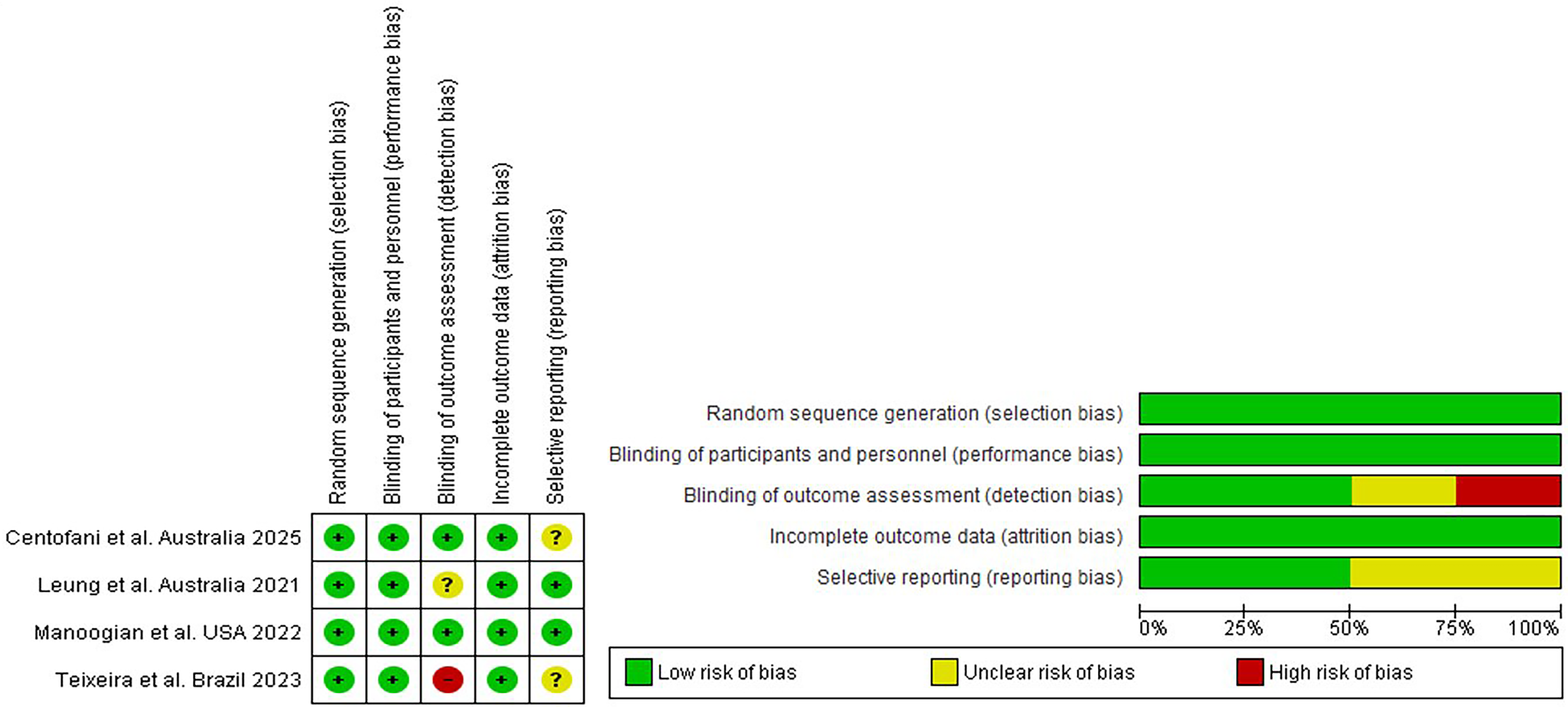
Risk of bias graph and summary of included studies.
Discussion
Despite a growing body of studies, the current review found only four trials reported cardiometabolic markers among designated participants. However, since studies assigned different fasting and eating window durations (ranging from 5–14 h fasting or 10–19 h eating window and 7 days up to 12 weeks of study duration), included participants with different occupation backgrounds, different settings, and observed diverse outcome measures, it is impossible to generalize these findings.
Nonetheless, the current review provides a first glimpse of the emerging evidence on the effects of meal timing (eating-fasting pattern) or IF on cardiometabolic markers among shift workers and has key implications for future research. Firstly, the fasting measurement found that 8.5 h of overnight fasting among police officers with night-shift work significantly improved fasting markers, with lower insulin and HOMA-IR. Similar improvement was also reported by Manoogian et al. (2022) among 10 night-shift firefighters with abnormal glucose, HOMA-IR, and HbA1c at baseline who were assigned a 10-h self-selected TRE, but not among all participants. This finding can support the limitation of previous observational studies, indicating impaired insulin sensitivity and glucose tolerance among people with night shift work and nighttime eating (Bayon et al., 2022; Lee et al., 2022; Manodpitipong et al., 2017; Molzof et al., 2022; Rizza et al., 2021; Sadeghniiat-Haghighi et al., 2022; Tawfik et al., 2025). Nevertheless, the strength of this evidence is limited by the short duration of the trials, even though isocaloric meals were prescribed in the study of Teixeira et al. (2023). Another potential issue of these results was the small sample size in Teixeria et al.'s (2023) study (n = 10). A smaller sample size may yield insufficient power to detect a difference between groups, leading to a type II error (Nayak, 2010). Therefore, the findings of Teixeira et al. should be interpreted cautiously, as the small sample size may have limited statistical power and increased the likelihood of imprecise effect estimates. However, remains limited within shift worker literature. Furthermore, due to the small sample size, the study by Teixeira et al. (2023) failed to report the withdrawal of participants, which yielded a high risk of bias in assessing missing outcome data in one study. Of note, both Manoogian et al. (2022) and Teixeira et al. (2023) conducted their interventions among tactical populations, namely firefighters and police officers. These occupations are characterized by irregular work schedules, high occupational stress, demanding physical requirements, and frequent circadian disruption, all of which may influence metabolic regulation and cardiometabolic risk. Consequently, the physiological responses to meal-timing interventions observed in these populations may not be directly generalizable to other shift-working populations. Future studies should investigate whether the cardiometabolic effects of meal-timing interventions differ across occupational groups with varying physical and metabolic demands. Moreover, irregular shift schedules, sleep restriction, and high occupational stress may alter circadian regulation, hormonal responses, substrate utilization, and appetite control. Consequently, tactical populations may respond differently to meal timing and dietary pattern interventions than civilians, highlighting the importance of tailored nutritional approaches in this group. In addition to occupational and physiological considerations, the social context of eating may also influence the implementation and effectiveness of meal-timing interventions among tactical populations. Firefighters and police officers frequently work within close-knit teams where shared meals contribute to social interaction, team cohesion, and workplace culture. These group-based eating practices may facilitate adherence to dietary interventions through peer support and collective participation. Conversely, shift workers in other occupational settings may have fewer opportunities for communal eating and may be required to implement meal-timing interventions independently. Therefore, the social environment surrounding food consumption should be considered when interpreting the feasibility and potential generalizability of meal-timing interventions across different shift-working populations.
Secondly, the study by Manoogian et al. denoted that 10-h self-selected TRE notably decreased the VLDL-C particle size of night shift firefighters compared to the control group. The clinical significance of the observed reduction in VLDL-C particle size remains uncertain. Because only one included study reported this outcome, and particle size changes may not directly translate into overall cardiometabolic benefit or harm. Therefore, further studies are needed to clarify the implications of meal-timing interventions on lipoprotein particle characteristics among shift workers. Likewise, the same study reported a higher LDL-C among participants with abnormal baseline values (n = 24). However, the overall effect of dyslipidemia should be interpreted with caution and requires further investigation, as participants with abnormal values were included at baseline in this study. The subgroup of participants with abnormal baseline lipid values was small (approximately n = 24 within a total sample of 137), which substantially limits the robustness of these findings. In such small subgroups, regression to the mean represents a major methodological concern, as individuals with extreme baseline lipid values are statistically more likely to demonstrate improvement over time independent of the intervention effect. Consequently, these results should be interpreted as exploratory and hypothesis-generating rather than definitive, and the overall impact of TRE on dyslipidemia in shift-working populations remains uncertain. Larger trials with adequate power, stratified randomization based on baseline lipid status, and prespecified subgroup analyses are required to clarify whether the 10-h self-selected TRE exerts clinically meaningful lipid-modifying effects beyond statistical regression.
Thirdly, in terms of postprandial measurements, one study reported notable reductions in glucose AUC, NEFA AUC, and 2-h glucose in the fasting group compared to the snack or meal at night group (Centofanti et al., 2025) following simulated night shift work. Similar to a controlled study by Grant et al. (2016, 2017), the finding indicated a significant increase in the glucose AUC response to breakfast in the eating-at-night group compared with the not-eating-at-night group. It is broadly known that studies in day workers versus simulated shift work conditions have demonstrated elevated postprandial glucose (Al-Naimi et al., 2004; Bonham et al., 2019; Keithellakpam et al., 2019; Morris et al., 2015; Roestamadji et al., 2019; Sharma et al., 2017). Meanwhile, a non-randomized controlled study by Naimi et al. found that NEFA levels were not affected by shift work (Al-Naimi et al., 2004). Even though the current finding may support previous observational studies, the robustness of the present evidence is limited because the study was conducted in a controlled laboratory setting, which may be difficult to generalize to real-life contexts. To be more specific, the significant results of Centofanti et al.'s study might be affected by restricted light exposure during wakefulness and sleep, which could influence postprandial measurements (Her et al., 2024; Li et al., 2025). A 2024 review of artificial light at night reports that higher outdoor night-time light exposure is associated with higher fasting and 2-hour postprandial glucose and HbA1c in a dose-dependent manner in population studies, although light levels are estimated rather than measured at the eye and are typically higher than 100 lux in the brightest environments (Baek et al., 2024). Moreover, a large cohort study on personal light exposure patterns shows that greater light at night and circadian-disrupting light patterns predict a higher incidence of type 2 diabetes, suggesting that chronic exposure to brighter evening/night light can worsen overall glucose homeostasis, including postprandial measures (Windred et al., 2024). Consequently, the light level that is controlled in the laboratory setting may affect the results. Therefore, future clinical trials in a free-living setting must be conducted to investigate changes in glucose AUC, 2-h postprandial glucose, and NEFA AUC, comparing the night-fasting and the meal-or-snack-at-night groups.
Fourthly, a short overnight fast for 4 weeks in the Leung et al. (2021) study promoted a slightly lower weight in the fasting group after intervention. Conversely, no studies reported a notable effect of meal time on BMI, body fat, daily caloric intake, or daily energy expenditure from activity among shift workers. To date, an increasing body of evidence has suggested an association between shift work and several adverse health effects, including MetS and overweight (Bonham et al., 2019; Łagowska et al., 2024; Q Liu et al., 2018a; W Liu et al., 2018b; Wang et al., 2014, 2018; Zhang et al., 2020). Hence, the recent evidence warrants further investigation into the effects of meal timing on weight management among shift workers. However, critical to the pilot nature of this study with a small sample size (n = 19), further investigation with a larger sample size and a longer study period is necessary to verify the effect of 5-h fasting at night on weight changes, BMI, and daily calories. Of note, since this study included shift workers with abdominal obesity, slight changes in body weight were most likely affected among subjects with abnormal values at baseline, yet the study did not investigate changes in weight among abdominal participants alone. Therefore, a designated study assessing different participant characteristics, for example, healthy versus abdominal obesity, is needed, including changes in body composition, to ensure a broader perspective on body weight management among fasting shift workers.
Subsequently, self-selected 10-h TRE significantly lowered systolic and diastolic blood pressure among firefighters with abnormal baseline rates, but not among all participants, according to Manoogian et al. (2022). In this study, the involvement of Mediterranean diet intervention appeared to be significantly lower in hypertension, in line with the past research, which pointed out that intakes of olive oil, vegetables, and fruit significantly improve both systolic and diastolic blood pressure among the adult population (Ahmed et al., 2020; De Pergola and D’Alessandro, 2018; Magriplis et al., 2020; Psaltopoulou et al., 2004). However, the Mediterranean diet did not significantly lower blood pressure in the overall population, possibly due to shortcomings in adherence. At baseline in both groups, only 35% of food descriptors represented these Mediterranean diet components, even though there was an increase in percentage at 6 weeks (38% for SOC and 42% for TRE) (Manoogian et al., 2022). A possible explanation is that sleep hygiene plays a concurrent role in blood pressure regulation and cardiometabolic health, particularly among shift workers (Direksunthorn, 2025). Short or irregular sleep has been shown to increase sympathetic nervous system activity, impair endothelial function, and disrupt nocturnal blood pressure dipping, all of which contribute to elevated systolic and diastolic blood pressure (Makarem et al., 2021). Consequently, improvements in blood pressure observed among participants with abnormal baseline values may partly reflect concurrent changes in sleep behavior rather than isolated effects of meal timing or diet composition alone. These observations underscore the importance of integrating sleep hygiene as a core component of lifestyle-based interventions, as addressing sleep insufficiency may enhance the responsiveness to nutritional strategies and yield more consistent cardiometabolic benefits across the entire study population. Furthermore, recent research indicates that sleep extension strategies can improve physical performance and cognitive alertness, which may synergize with meal timing, partially attenuating the typical circadian performance decline and establishing sleep extension as an effective, non-pharmacological strategy for optimizing performance capabilities (Bouzouraa et al., 2025). However, although sleep extension and sleep hygiene interventions may improve cardiometabolic health, their application in shift-working populations requires careful consideration. Many traditional sleep hygiene recommendations were developed for individuals with conventional daytime schedules and may be difficult to implement among night-shift workers. Therefore, sleep interventions for shift workers may need to be tailored to accommodate daytime sleep, rotating schedules, and circadian disruption, consistent with emerging shift worker-specific sleep hygiene recommendations (Shriane et al., 2023).
Lastly, another crucial factor that no studies have assessed is participants’ chronotype. Chronotype dictates the individual's internal circadian phase, which in turn determines metabolic readiness for nutrient processing, independent of external clock time (Almoosawi et al., 2019). Studies indicate that evening chronotypes (E-types) and morning chronotypes (M-types) exhibit differential metabolic responses to the exact meal timing; for instance, E-types are more prone to circadian misalignment and glucose intolerance when forced to adopt early eating schedules that conflict with their biological rhythms (Lotti et al., 2022; Ren et al., 2021). Furthermore, ignoring chronotype introduces statistical bias in intervention data, as E-types may adapt more readily to night-shift eating patterns than M-types, thereby diluting the observed efficacy of fasting or timing protocols when groups are aggregated. Consequently, interventions that fail to personalize meal timing relative to an individual's internal clock, rather than wall-clock time, risk misinterpreting the effectiveness of meal timing strategies and exacerbating metabolic risks for the vulnerable subgroup.
Here, our review was comprehensive, including trials with no date-of-publication or language restrictions. Likewise, the current study included those with abdominal obesity and subjects with cardiometabolic risk factors. These studies, however, were too diverse to be accommodated in a meta-analysis, and thus far, similar trials remain lacking. Furthermore, some concerns and a high risk of bias from some domains should be noted for prospective studies. The use of methodological control strategies in current trials is advancing, aiming to produce stronger evidence to reduce cardiometabolic risk factors among shift workers for the future.
As for the future directions, the current evidence regarding mealtime interventions and cardiometabolic health among shift workers remains limited by the small number of clinical trials, modest sample sizes, short intervention durations, and heterogeneity in intervention protocols and outcome assessments. Future research should prioritize adequately powered randomized controlled trials with longer follow-up periods to determine the sustainability of cardiometabolic benefits associated with meal-timing interventions.
In addition, future studies should recruit a broader range of shift-working populations beyond healthcare workers, firefighters, and police officers to improve the generalizability of findings. Given the unique occupational and circadian challenges faced by shift workers, further investigation is needed to identify optimal eating windows, fasting durations, and intervention strategies that are both physiologically effective and operationally feasible. Researchers should also consider social, behavioral, and workplace factors that may influence adherence to meal-timing interventions.
Finally, greater standardization of cardiometabolic outcome measures and assessment protocols would facilitate comparison across studies and strengthen the evidence base. Future trials should evaluate both short-term and long-term outcomes, including glycemic control, lipid metabolism, body composition, sleep-related outcomes, and markers of cardiovascular risk, to provide a more comprehensive understanding of the health effects of meal-timing interventions among shift workers. studies.
Conclusion
Based on current knowledge, we have reported the first systematic review of RCTs, to our knowledge, focused on meal timing regulation or IF intervention and cardiometabolic risk factors among shift workers. The current review shows that only four trials report results for the idea in question, which limits the generalizability of the findings and raises concerns about the robustness of the preliminary positive outcomes. Optimizing shift work arrangements with fasting during specific nighttime hours can help unavoidable shift workers implement better meal timing schedules that are less detrimental to cardiometabolic health risks, thereby minimizing sickness, work absence, and improving work- and leisure-time productivity. However, a more detailed analysis of the specific effects of different participants’ characteristics, for example, healthy/overweight/obese, those with abnormal cardiometabolic risk, or those with certain diseases, is not possible due to the small number of studies and the heterogeneity of intervention settings and outcome measures. Therefore, further studies that examine the effects of IF on broader characteristics, occupational background, and sample size are required among shift workers.
Supplemental Material
sj-docx-1-nah-10.1177_02601060261464874 - Supplemental material for Cardiometabolic status among shift workers under meal time regulation: A systematic review of randomized controlled trials
Supplemental material, sj-docx-1-nah-10.1177_02601060261464874 for Cardiometabolic status among shift workers under meal time regulation: A systematic review of randomized controlled trials by Fatqiatul Wulandari, Imas E Khoiriyah, Anisa J Naim, Anita N Walker, Dominikus R Atmaka, Ime A Khuang and Qing Feng in Nutrition and Health
Supplemental Material
sj-docx-2-nah-10.1177_02601060261464874 - Supplemental material for Cardiometabolic status among shift workers under meal time regulation: A systematic review of randomized controlled trials
Supplemental material, sj-docx-2-nah-10.1177_02601060261464874 for Cardiometabolic status among shift workers under meal time regulation: A systematic review of randomized controlled trials by Fatqiatul Wulandari, Imas E Khoiriyah, Anisa J Naim, Anita N Walker, Dominikus R Atmaka, Ime A Khuang and Qing Feng in Nutrition and Health
Footnotes
Acknowledgments
The authors gratefully thank the Chinese Scholarship Council (CSC), which fully supports the academic journey of FW in China.
Registration
PROSPERO registration No. CRD42024588992.
Ethical approval
Ethics approval was not required for this systematic review.
Consent for publication
All authors agreed to the publication of this manuscript.
Authors’ contributions
F.W., I.E.K., A.J.N., and Q.F.: conceptualization and designing the project. F.W., I.E.K., and A.J.N: data collection, screening, extraction, and quality assessment. F.W. and I.E.K.: data interpretation, analysis, and critical review. F.W.: writing the manuscript. F.W., I.E.K, A.J.N., A.N.W., D.R.A., I.A.K., and Q.F.: editing and finalizing the submitted manuscript.
Funding
This study did not receive a specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
All data can be found in the main manuscript and supplementary materials.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.